
Abstract
Summary
The aim of the present study was to identify patient factors associated with higher costs in hip fracture patients. The mean costs of a prospectively observed sample of 402 patients were 8853 €. The ASA score, Charlson comorbidity index, and fracture location were associated with increased costs.
Purpose
Fractures of the proximal end of the femur (hip fractures) are of increasing incidence due to demographic changes. Relevant co-morbidities often present in these patients cause high complication rates and prolonged hospital stays, thus leading to high costs of acute care. The aim of this study was to perform a precise cost analysis of the actual hospital costs of hip fractures and to identify patient factors associated with increased costs.
Methods
The basis of this analysis was a prospectively observed single-center trial, which included 402 patients with fractures of the proximal end of the femur. All potential cost factors were recorded as accurately as possible for each of the 402 patients individually, and statistical analysis was performed to identify associations between pre-existing patient factors and acute care costs.
Results
The mean total acute care costs per patient were 8853 ± 5676 € with ward costs (5828 ± 4294 €) and costs for surgical treatment (1972 ± 956 €) representing the major cost factors. The ASA score, Charlson comorbidity index, and fracture location were identified as influencing the costs of acute care for hip fracture treatment.
Conclusion
Hip fractures are associated with high acute care costs. This study underlines the necessity of sophisticated risk-adjusted payment models based on specific patient factors. Economic aspects should be an integral part of future hip fracture research due to limited health care resources.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Hip fractures are typical osteoporotic fractures in elderly patients. The increased life expectancy and increased activity levels of elderly people have led to an increased incidence of fractures at the proximal end of the femur [1–3]. The incidence of these fractures in Germany has increased to 439 per 100,000 people per year [4]. Many of the patients with hip fractures have pre-existing impaired mobility and relevant co-morbidities leading to prolonged hospital stays, significant complications, and mortality rates. Therefore, the acute care needed for these patients is associated with high costs.
Hip fracture treatment accounts for more than 50% of total costs of osteoporotic fractures. These fractures are therefore the most expensive osteoporosis-related fractures [5–7]. The annual total hospital costs were the highest for osteoporotic fractures ($5.1 billion per year), followed by myocardial infarction, stroke, and breast cancer [8].
As a result, hip fractures represent a serious global health issue [1]. In the conflict between financial challenges due to limited resources and high health care costs due to demographic changes, an understanding of detailed direct costs is very important. However, detailed data on direct costs of acute care resulting from hip fractures and their distribution within acute care, as well as the evaluation of the effect of patient factors, are limited.
Some authors previously calculated the costs of hip fracture treatment, and results vary widely [9]. For example, Sahota et al. estimated costs of £9.429 (10.896 €) in their analysis of 100 care home residents in the UK [10].
The aim of this study was to perform a detailed cost analysis of actual hospital costs of hip fractures as accurately as possible for each patient included in a prospective single-center observational study. Subsequently, we wanted to correlate patient characteristics with the calculated hospitalization costs.
Patients and methods
The basis of this cost analysis is a prospectively observed single-center trial; the results of which have been published before [11]. In total, 402 patients with fractures of the proximal end of the femur admitted to our level 1 trauma department between April 1, 2009 and September 30, 2011 were included in the study. The study was conducted in the University Hospital of Gießen and Marburg, Marburg, Germany. Patients who sustained multiple trauma (ISS >16) as well patients <60 years old and patients with malignancy-associated fractures were excluded from the study. All patients were treated surgically with either internal fixation or hip arthroplasty. The aim of the underlying single-center trial was a detailed assessment of the acute care phase as well as the identification of independent factors related to HrQoL and functional outcomes in geriatric hip fracture patients. Approval by the local ethics committee was obtained for this study (AZ 175/08).
Patient characteristics
Demographic data, e.g., age, gender, co-morbidities (Charlson comorbidity index [12]; dichotomized using the categories less than 4 and greater than or equal to 4), American Society of Anesthesiologist (ASA) score [13], pre-fracture anticoagulation with phenprocoumon, and fracture type (non-displaced femoral neck fracture, displaced femoral neck fracture, stable trochanteric fracture, unstable trochanteric fracture, and subtrochanteric fracture), among other factors, were documented. Depression was evaluated using the short form of the Geriatric Depression Scale (GDS) [14]. Patients with a GDS >4 were classified as at risk for depression to achieve high sensitivity in the depression screening [15]. Cognitive impairment was assessed using the Mini Mental Status Examination (MMSE) [16]. According to the current German guidelines for dementia, the results of the MMSE were divided into no or mild cognitive impairment (MMSE 20–30) and moderate to severe cognitive impairment (MMSE <20) [17].
Cost analysis
All potential cost factors were prospectively recorded as accurately as possible for each of the 402 patients individually. Afterward, the actual costs for each cost factor were retrospectively calculated with help of the controlling division in our financial department.
Total costs were divided into major cost components. These components were calculated individually, then summarized by subcomponent to total costs per patient. Ward costs were recorded separately for intensive care and for normal acute ward care. Calculation of ward costs included hotel costs, costs for personnel (nursing staff and doctors), medication (every single tablet was separately documented), and for high-consumption items. Theater costs were accurately calculated with respect to the following: costs for the personnel (surgeons, surgical nursing staff, anesthesiologists, and anesthesiology nursing staff), sterile materials, maintenance, and amortization costs. The costs of implants were calculated using the costs of all components, and in the case of concomitant fractures, further implants were also included in the overall cost calculation. Further costs for physiotherapy were calculated as well (frequency and time of physiotherapy, one or two therapists necessary). All examinations including laboratory examinations (every single laboratory value), microbiology, virology, blood bank, and radiologic examinations (including additional fees for holiday or night examination) were recorded and their costs were calculated. Every additional cost relevant to special events or treatment was also included (e.g., consultation of other specialists and dialysis). In the current analysis, standardization was used for the costs of treatment in the emergency department; for nursing services, hotel costs, and miscellaneous costs on the ICU and acute ward; and for the medical treatment on ICU and acute ward. Other variables were calculated individually on patient level on the basis of actual resource use.
Statistics
The data were collected in a Filemaker® database (FileMaker Inc., Santa Clara, CA, USA). Double entry with a plausibility check was performed to monitor data quality. Predictive Analysis Software version 22.0 (SPSS Inc., Chicago, IL, USA) was used for explorative data analysis. The data are presented as the means and standard deviations (SDs) from the mean. The Shapiro-Wilk test was used to test for normal distribution. Accordingly, means were compared using the Mann-Whitney test or the Kruskal-Wallis test. A p value of <0.05 was considered to be significant. The cost of acute care of hip fracture treatment and some of its potential predictors were analyzed in a multivariate analysis. A generalized linear model with a log-link and gamma errors was used as recommended in previous research for health care cost data [18, 19].
Results
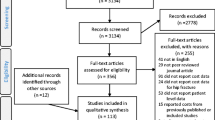
During the investigation period, a total of 539 hip fracture patients were treated in our department. Of the 477 patients who met the inclusion criteria, 75 patients declined to participate; 402 patients were included in the study. The mean age of patients included was 81 ± 8 years. In total, 73% (n = 293) of the patients were female. The mean pre-operative ASA score was 2.9 ± 0.6, and the mean Charlson comorbidity index at admission was 2.4 ± 2.3. The mean length of hospital stay was 14 ± 6 days. Fracture localization is shown in Table 1.
The mean total acute care costs per patient were 8853 ± 5676 €. The total costs were subdivided into ward costs (5828 ± 4294 €), costs for surgical treatment (1972 ± 956 €), laboratory investigations (390 ± 440 €), blood bank (234 ± 353 €), physiotherapy (262 ± 224 €), radiological examinations (120 ± 179 €), and other costs (47 ± 123 €) (Table 2).
Further analysis of the effect of pre-existing conditions and clinical course variables on total acute care costs was conducted (Table 3). We observed no significant differences between different groups based on age and patient gender.
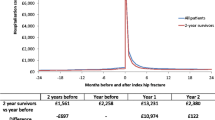
Femoral neck fractures caused higher average costs than trochanteric and subtrochanteric fractures (9351 vs. 8475 vs. 7578 €, respectively) without significant differences (p = 0.651). However, an evaluation of more detailed categorizations of the fracture types (Fig. 1) showed that the severity of the fracture is significantly associated with total acute care costs. Thus, dislocated fractures of the femoral neck (garden III–IV) and instable trochanteric fractures (A2 or A3 according to the AO classification) were associated with significantly higher costs.

Total acute care costs according to fracture type
A significant difference was found between the ASA score categories with costs continuously rising with higher ASA scores (p = 0.007). Patients with a Charlson comorbidity index less than 4 had average costs of 8353 €, compared with 10,383 € for patients with Charlson comorbidity indices greater than or equal to 4 (p = 0.047). Cognitive impairment (Mini Mental State Examination <20) did not have a significant effect on total costs (MMSE ≤20 8248 € vs. MMSE >20 9176 €; p = 0.616). The length of hospital stay was shorter for patients with an MMSE ≤20 (12 vs. 15 days; p < 0.001).
Additionally, depression at admission (Geriatric Depression Scale >4) did not significantly increase acute care costs. Patients who were on phenprocoumon at admission had similar hospitalization costs compared with those who were not (8775 vs. 8867 €; p = 0.061).
Multivariate analysis showed that fracture type (unstable trochanteric fracture (A2, A3)), ASA score (ASA 3–5), and Charlson comorbidity index (cutoff 4) are independent significant predictors of high acute care costs, whereas MMSE ≤20 showed to be associated with lower acute care costs (Table 4).
Discussion
In this study, we aimed to determine hospital costs for the acute care of hip fractures and to find patient factors that influence these costs. The total costs were comparable to previous studies, and ward costs were the main cost factor present in this study. We found higher costs for patients with higher ASA scores and higher Charlson comorbidity indices as well as for patients with displaced femoral neck and unstable trochanteric fractures compared with other fracture types.
For the first time, in this study, costs for acute care treatment were analyzed in that detail. Previously, data for actual costs in Germany were completely lacking. The average of 8853 € per patient was slightly lower compared with the figures of $13,805 (12,855 €) and £9429 (10,896 €) calculated previously in other countries [10, 20]. We are aware that the comparison of the total costs across countries might be misleading. However, both these studies and our data suggested that ward costs accounted for the biggest proportion of total hospitalization costs [21, 22]. Therefore, care models that include rapid recovery, thus reducing the length of hospital stay, might reduce hip fracture costs.
The significance of early mobilization and return to previous mobility for hip fracture patients is well known. When taking this into consideration, it is remarkable that only 3% of total costs were spent on physiotherapy (Table 2). We concluded that efforts regarding patient mobilization must be increased. Ortho-geriatric treatment models might be cost-effective due to reducing hospitalization costs and indirect costs of hip fractures [23]. Economic aspects should be an integral part of future hip fracture research due to limited health care resources.
In addition to total treatment costs, it seemed to be crucial to identify patient factors that predict these costs as this knowledge could advance the discussion on appropriate reimbursement in different payment models worldwide. Although it was not significant, we found treatment for men compared with women was nearly 800 € more expensive (Table 3). This is in line with previous studies [20, 24]. A potential explanation is that men who experience hip fractures usually have a poor health status, potentially leading to complicated or prolonged hospital stays. Consistent with this hypothesis, Leal et al. found higher male mortality when compared with females [25].
The additional impact of co-morbidities on hospitalization costs was assessed in the present study. Nikkel et al. showed in their analysis of 32,440 hip fractures that only 4.9% of the patients had no co-morbidities. Co-morbidities were directly related to hospitalization costs and lengths of stay in hip fracture treatment [20]. In our analysis, co-morbidities were summarized using the Charlson comorbidity index. The Charlson comorbidity index has been shown to correlate with the in-hospital 30- and 90-day mortality rates after hip fracture treatment [26–28], suggesting that the CCI adequately summarizes patients’ health status. Johnson et al. recently found that the Charlson comorbidity index is associated with prolonged length of stay and increased hospital costs following surgical treatment for hip fractures [29]. Additionally, Leal et al. found that increased Charlson comorbidity index was associated with higher hospitalization costs [25]. Consistent with these findings in our sample, the Charlson comorbidity index did significantly increase acute hospital care costs (Table 3). Chen et al. also found that hip fracture patients with comorbidities incurred higher hospitalization costs [30]. Their study showed that dementia added the largest amount to total costs. In contrast to those findings, in our sample, patients with cognitive impairment had lower hospitalization costs. This might be because many of the cognitively impaired patients were discharged sooner and sent back to their prior environment to prevent further confusion and because these patients often did not have the potential for rehabilitation, resulting in shorter lengths of hospital stay. Another method to summarize the patients’ overall health status is the ASA score. Earlier studies have shown that an increased ASA score is associated with increased hospital costs [24, 31]. Garcia et al. found that an increase of one point in the ASA classification system led to extra costs of $9300 [24]. However, as hospital costs were only estimated as indirect means of lengths of stay in this study, this finding should be regarded with caution. We also found a continuous increase in acute care costs with increased ASA score (Table 3).
In the present study, femoral neck fractures were associated with insignificantly higher costs compared with trochanteric fractures (Table 3). In a more detailed analysis, displaced femoral neck fractures that were treated with hemi-arthroplasty were the most expensive factures (Fig. 1). This observation could potentially be explained by the higher costs of implants and the longer operation time required for arthroplasty. Consistent with these findings, Nikkel et al. found that arthroplasty was shown to be associated with higher costs compared to internal fixation [20]. In addition, unstable trochanteric fractures were also associated with higher costs, which might be a result of a longer surgery time and difficulties in the post-surgical period. Overall, displaced femoral neck fractures and unstable trochanteric fractures were associated with significantly higher costs compared with non-displaced femoral neck fractures, stable trochanteric fractures, and subtrochanteric fractures, indicating that the severity of the fracture somehow predicts subsequent hospitalization costs.
Strengths and limitations
The fact that an accurately conducted prospective observational study was the basis of this analysis is one of the major strengths of this study. Furthermore, this analysis represents the result of an extremely detailed analysis of the actual costs of care for every individual patient. Another strength is the relatively large size of the sample evaluated. However, there are also several limitations. First, the results of this patient sample and the resulting costs of inpatient care reflect only the reality of a single level 1 university trauma center in Germany. Further studies are warranted to obtain similar results in other settings and countries. Second, a cost analysis, regardless of how detailed and accurate it is, contains some assumptions. For example, it is not possible to exactly determine the duration of doctor-patient contact during the acute ward phase. Another drawback of this study is that it only includes primary hospitalization costs. Other studies have shown that relevant costs following hip fractures also occur in the period after discharge [25].
Conclusion
In summary, the results of this study suggest that the ASA score, Charlson comorbidity index, and fracture location do influence the costs of acute care in hip fracture treatment. Reimbursement models worldwide are increasingly transitioning to fixed reimbursement depending on the main diagnosis (e.g., German Diagnosis Related Groups (DRGs)) or expected costs (e.g., bundled payment). This study underlines the necessity for sophisticated risk-adjusted payment models based on specific patient factors. To reduce the socio-economic burden, fracture prevention programs and cost-effective treatment models are necessary.
References
Marks R (2010) Hip fracture epidemiological trends, outcomes, and risk factors, 1970-2009. Int J Gen Med 3:1–17
Icks A, Haastert B, Wildner M, Becker C, Meyer G (2008) Trend of hip fracture incidence in Germany 1995-2004: a population-based study. Osteoporos Int 19:1139–1145
White SM, Griffiths R (2011) Projected incidence of proximal femoral fracture in England: a report from the NHS Hip Fracture Anaesthesia Network (HIPFAN). Injury 42:1230–1233
Kanis JA, Odén A, McCloskey EV, Johansson H, Wahl DA, Cooper C, Life IWGoEaQo (2012) A systematic review of hip fracture incidence and probability of fracture worldwide. Osteoporos Int 23:2239–2256
Dolan P, Torgerson DJ (1998) The cost of treating osteoporotic fractures in the United Kingdom female population. Osteoporos Int 8:611–617
Burge R, Dawson-Hughes B, Solomon DH, Wong JB, King A, Tosteson A (2007) Incidence and economic burden of osteoporosis-related fractures in the United States, 2005-2025. J Bone Miner Res 22:465–475
Ström O, Borgström F, Kanis JA, Compston J, Cooper C, McCloskey EV, Jönsson B (2011) Osteoporosis: burden, health care provision and opportunities in the EU: a report prepared in collaboration with the International Osteoporosis Foundation (IOF) and the European Federation of Pharmaceutical Industry Associations (EFPIA). Arch Osteoporos 6:59–155
Singer A, Exuzides A, Spangler L, O’Malley C, Colby C, Johnston K, Agodoa I, Baker J, Kagan R (2015) Burden of illness for osteoporotic fractures compared with other serious diseases among postmenopausal women in the United States. Mayo Clin Proc 90:53–62
Braithwaite RS, Col NF, Wong JB (2003) Estimating hip fracture morbidity, mortality and costs. J Am Geriatr Soc 51:364–370
Sahota O, Morgan N, Moran CG (2012) The direct cost of acute hip fracture care in care home residents in the UK. Osteoporos Int 23:917–920
Buecking B, Struewer J, Waldermann A, Horstmann K, Schubert N, Balzer-Geldsetzer M, Dodel R, Bohl K, Ruchholtz S, Bliemel C (2014) What determines health-related quality of life in hip fracture patients at the end of acute care?—a prospective observational study. Osteoporos Int 25:475–484
Charlson ME, Pompei P, Ales KL, MacKenzie CR (1987) A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 40:373–383
Anaestesiologists ASo (2015) American Society of Anesthesiologists. ASA physical status classification system. Accessed Accessed: 18 February 2015
Sheikh JI, Yesavage, J.A. (1986) Geriatric Depression Scale (GDS). Recent evidence and development of a shorter version. In (Ed.) TLB (ed) Clinical gerontology: a guide to assessment and intervention. The Haworth Press, NY, pp 165–173.
Almeida OP, Almeida SA (1999) Short versions of the geriatric depression scale: a study of their validity for the diagnosis of a major depressive episode according to ICD-10 and DSM-IV. Int J Geriatr Psychiatry 14:858–865
Folstein MF, Folstein SE, McHugh PR (1975) “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 12:189–198
(AWMF) AWMF (2009) S3-guideline “dementia”, long version. Accessed 5 October 2015
Dunn G, Mirandola M, Amaddeo F, Tansella M (2003) Describing, explaining or predicting mental health care costs: a guide to regression models. Methodological review. Br J Psychiatry 183:398–404
Rolfson O, Ström O, Kärrholm J, Malchau H, Garellick G (2012) Costs related to hip disease in patients eligible for total hip arthroplasty. J Arthroplast 27:1261–1266
Nikkel LE, Fox EJ, Black KP, Davis C, Andersen L, Hollenbeak CS (2012) Impact of comorbidities on hospitalization costs following hip fracture. J Bone Joint Surg Am 94:9–17
Wong MK, Arjandas CLK, Lim SL, Lo NN (2002) Osteoporotic hip fractures in Singapore—costs and patient’s outcome. Ann Acad Med Singap 31:3–7
Lawrence TM, White CT, Wenn R, Moran CG (2005) The current hospital costs of treating hip fractures. Injury 36:88–91 discussion 92
Kammerlander C, Roth T, Friedman SM, Suhm N, Luger TJ, Kammerlander-Knauer U, Krappinger D, Blauth M (2010) Ortho-geriatric service—a literature review comparing different models. Osteoporos Int 21:S637–S646
Garcia AE, Bonnaig JV, Yoneda ZT, Richards JE, Ehrenfeld JM, Obremskey WT, Jahangir AA, Sethi MK (2012) Patient variables which may predict length of stay and hospital costs in elderly patients with hip fracture. J Orthop Trauma 26:620–623
Leal J, Gray AM, Prieto-Alhambra D, Arden NK, Cooper C, Javaid MK, Judge A, group Rs (2015) Impact of hip fracture on hospital care costs: a population-based study. Osteoporos Int
Kirkland LL, Kashiwagi DT, Burton MC, Cha S, Varkey P (2011) The Charlson comorbidity index score as a predictor of 30-day mortality after hip fracture surgery. Am J Med Qual 26:461–467
Souza RC, Pinheiro RS, Coeli CM, Camargo KR Jr (2008) The Charlson comorbidity index (CCI) for adjustment of hip fracture mortality in the elderly: analysis of the importance of recording secondary diagnoses. Cad Saude Publica 24:315–322
Neuhaus V, King J, Hageman MG, Ring DC (2013) Charlson comorbidity indices and in-hospital deaths in patients with hip fractures. Clin Orthop Relat Res 471:1712–1719
Johnson DJ, Greenberg SE, Sathiyakumar V, Thakore R, Ehrenfeld JM, Obremskey WT, Sethi MK (2015) Relationship between the Charlson comorbidity index and cost of treating hip fractures: implications for bundled payment. J Orthop Traumatol 16:209–213
Chen LT, Lee JA, Chua BS, Howe TS (2007) Hip fractures in the elderly: the impact of comorbid illnesses on hospitalisation costs. Ann Acad Med Singap 36:784–787
Thakore RV, Lee YM, Sathiyakumar V, Obremskey WT, Sethi MK (2014) Geriatric hip fractures and inpatient services: predicting hospital charges using the ASA score. Curr Gerontol Geriatr Res 2014:923717
Acknowledgments
The authors want to thank Gerhard Bodenbender for his valuable contribution to the acquisition of data. We also wish to acknowledge Monika Balzer-Geldsetzer and Richard Dodel for their assistance in planning the study design.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None.
Electronic supplementary material
ESM 1
(DOCX 21 kb)
Rights and permissions
About this article

Cite this article
Aigner, R., Meier Fedeler, T., Eschbach, D. et al. Patient factors associated with increased acute care costs of hip fractures: a detailed analysis of 402 patients. Arch Osteoporos 11, 38 (2016). https://doi.org/10.1007/s11657-016-0291-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11657-016-0291-2