
Abstract
Summary
This retrospective analysis of hip fracture patients with and without muscle atrophy/weakness (MAW) revealed that those with MAW had significantly higher healthcare utilization and costs compared with hip fracture patients without MAW.
Purpose
Examine the demographics, clinical characteristics, and healthcare resource utilization and costs of hip fracture patients with and without MAW.
Methods
Using a large US claims database, individuals who were newly hospitalized for hip fracture between 1 Jan 2006 and 30 September 2009 were identified. Patients aged 50–64 years with commercial insurance (Commercial) or 65+ years with Medicare supplemental insurance (Medicare) were included. The first hospitalization for hip fracture was defined as the index stay. Patients were categorized into three cohorts: patients with medical claims associated with MAW over the 12 months before the index stay (pre-MAW), patients whose first MAW claim occurred during or over the 12 months after the index stay (post-MAW), and patients without any MAW claim (no-MAW). Multivariate regressions were performed to assess the association between MAW and healthcare costs over the 12-month post-index period, as well as the probability of re-hospitalization.
Results
There were 26,122 Medicare (pre-MAW, 839; post-MAW, 2,761; no-MAW, 22,522) and 5,100 Commercial (pre-MAW, 132; post-MAW, 394; no-MAW, 4,574) hip fracture patients included in this study. Controlling for cross-cohort differences, both the pre-MAW and post-MAW cohorts had significantly higher total healthcare costs (Medicare, $7,308 and $18,753 higher; Commercial, $18,679 and $25,495 higher) than the no-MAW cohort (all p < 0.05) over the 12-month post-index period. The post-MAW cohort in both populations was also more likely to have any all-cause or fracture-related re-hospitalization during the 12-month post-index period.
Conclusions
Among US patients with hip fractures, those with MAW had higher healthcare utilization and costs than patients without MAW.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
As one of the most serious consequences of falls in the elderly population [1], hip fractures can lead to substantial mobility limitations, morbidity, loss of independence, and mortality [2–4]. The lifetime risk of hip fracture is 17.5 % for women and 6 % for men [5], while the annual number of hospitalizations due to hip fracture is approximately 300,000 [6]. The lifetime cost of treating hip fractures in the United States has been estimated to be $20 billion [3]. Research has shown that 18 % of women and 32 % of men die within the first year of hip fracture [2].
Treatment for hip fracture varies according to the patient health profile and injury type [7]. Hip fractures are treated nonsurgically if the fracture is considered sufficiently stable or if the patient is too ill to undergo surgery; otherwise, patients usually receive internal fixation, partial hip replacement (hemiarthroplasty), or total hip replacement (total hip arthroplasty) [7, 8]. To return to community living after hospitalization for acute treatment, patients typically require multidisciplinary rehabilitation [8]. Patients with hip fractures may require post-acute rehabilitation services provided through home healthcare programs, skilled nursing facilities (SNF), inpatient rehabilitation facilities, or some combination of these resources [8].
One consequence of hip fractures is that the associated reduction in mobility may result in muscle atrophy/weakness (MAW). For example, research has shown that, in the absence of any voluntary contractions, muscle strength can decrease by as much as 5 % per day [9]. Such deficits in muscle strength have been associated with poor recovery in mobility [10] and poor physical functioning [11] among post hip fracture patients. Muscle atrophy has also been found to persist for up to 2 years after hip arthroplasty [12].
Although previous research conducted among hip fracture patients has shown that individuals with MAW have poorer physical functioning [10, 11], no previous attempt has been made to quantify the differences in resource use or costs between hip fracture patients with and without MAW. The purpose of this study was to examine the differences in patient characteristics, treatment patterns, healthcare resource use, and costs among individuals hospitalized for hip fracture who had no diagnosis of MAW and those who had a diagnosis of MAW before or after their hip fracture. We hypothesize that patients with MAW would have significantly higher healthcare utilization and costs when compared with hip fracture patients without MAW.
Methods
Data for this study came from the Thomson Reuters Marketscan® Commercial Claims and Encounter (Commercial) Database and the Medicare Supplemental Insurance (Medicare) Databases. These retrospective claims databases are fully compliant with the Health Insurance Portability and Accountability Act privacy requirements and capture person-specific healthcare use, expenditures, and enrollment across inpatient, outpatient, and prescription drug services. The Commercial database includes large employers, health plans, government organizations, and public organizations and covers approximately 100 payers and more than 500 million claims records. The Medicare database contains information on Medicare beneficiaries who are age 65 years or older and who have employer-sponsored supplemental insurance. The databases link paid claims and encounter data to detailed patient information across sites and types of providers over time. Data records examined for this study spanned the time period from 1 January 2005 through 30 September 2010.
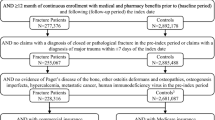
For inclusion in this study, a patient was required to have an inpatient stay with an accompanying diagnosis of hip fracture between 1 January 2006 and 30 September 2009, with the admission date of the first such inpatient stay denoted as the index date. Patients who received a prior diagnosis of a hip fracture over the time period from 1 year through 7 days before the index date were excluded from the analysis. Patients in the Commercial database were required to be 50–64 years old at the index date, while those in the Medicare database were required to be at least 65 years old as of the index date. Finally, patients were required to have continuous insurance coverage over the time period from 1 year before the index date (the pre-period) through 1 year after the discharge of index hospital stay (the post-period).
Individuals in the Commercial and Medicare databases were analyzed separately. This separation was due to differences among the elderly and non-elderly hip fracture populations, as well as differences between the Commercial and Medicare insurance. Each of these two populations was then subdivided into three distinct cohorts: those with no diagnosis of MAW (no-MAW) from the pre-period to the post-period, those diagnosed with MAW before the index date (pre-MAW), and those diagnosed with MAW during or after the index hospital stay (post-MAW). Table 1 provides the ICD-9 codes and description for codes used to identify both hip fractures and MAW.
The analysis compared patient characteristics, healthcare resource use, and costs of the no-MAW, pre-MAW, and post-MAW cohorts. The patient characteristics included age, sex, region of residence, type of insurance coverage, and comorbid conditions (i.e., osteoarthritis, osteoporosis, rheumatoid arthritis). Overall general health was approximated using the modified Charlson Comorbidity Index (CCI) [13] which measures 23 different categories of comorbidities and creates a score that is used to predict costs. The patterns of treatment associated with the index hospitalization included length and cost of inpatient stay and discharge status (e.g., home, SNF). Resource use variables included hospitalizations, physician office visits, outpatient hospital visits, emergency room (ER) visits, and the use of a SNF, an inpatient rehabilitation facility, home health care, physical therapy, or occupational therapy. Costs were calculated as total direct medical costs and subdivided into inpatient, outpatient, and pharmacy costs. All costs were adjusted to 2011 US dollars using the medical care component of the Consumer Price Index [14].
Unadjusted differences between groups were compared with chi-square statistics used for categorical variables (e.g., gender, region of residence, health plan type, comorbidities, discharge status of index stay, and proportion with resource use), Student’s t tests for age, and non-parametric Wilcoxon rank-sum tests for other continuous variables (e.g., CCI, length of index hospital stay, healthcare resource utilization including total hospital days, number of physician office visits, outpatient hospital visits, ER visits, and healthcare costs in the pre- and post-periods).
Multivariate generalized linear regression models with log-link and gamma distribution were used to assess the association between MAW and health care costs, controlling for age, gender, region of residence, health plan type, comorbid medical conditions, CCI, pre-period resource use (any hospitalization, ER, or outpatient hospital visit), and discharge status from the index hospitalization. To better interpret results derived from the generalized linear models, the marginal difference in healthcare costs for pre-MAW and post-MAW cohorts when compared with the no-MAW cohort were estimated by computing the expected instantaneous change of mean healthcare costs as a function of a change in the MAW cohort variables while keeping all the other covariates constant [15].
When 10 % or more of the populations have zero costs, two-part models were performed to estimate the adjusted differences on healthcare costs associated with MAW [16]. In the first part, the probability of utilizing the service of interest is estimated while the second part estimates costs among those who utilized the service. The adjusted difference on healthcare costs between the pre-MAW or post-MAW cohort and the no-MAW cohort were calculated the same way as in the generalized linear regression model, and a 95 % confidence interval (CI) was estimated using the 2.5 and 97.5 percentile of the 1,000 estimated marginal difference estimates by bootstrapping the two-part model with 1,000 iterations [17].
In addition, the impact of MAW on any all-cause or fracture-related hospitalization in the post-period was examined via logistic regressions controlling for cross-cohort differences in age, gender, region of residence, health plan type, CCI, comorbidities, discharge status from the index hospitalization, and pre-period healthcare utilization (any hospitalization, ER, or outpatient hospital visit). Odds ratio as well as the 95 % CI were reported. All analyses were performed using SAS version 9.1, and P values < 0.05 were considered, a priori, to be statistically significant.
Results
This study included 5,100 patients aged 50–64 years in the Commercial population and 26,122 patients aged 65 years and above in the Medicare population (Table 2). Of these individuals, 2.6 % of the Commercial population was diagnosed with MAW before their hip fracture (pre-MAW) and 7.7 % were diagnosed with MAW during or after their hip fracture (post-MAW). MAW was found to be more prevalent in the Medicare population, with 3.2 % of individuals in the pre-MAW and 10.7 % in the post-MAW cohorts, respectively. In the Medicare population, pre- and post-MAW cohorts were significantly older and more likely to reside in the South. Patients in the Commercial population were most commonly insured via a preferred provider organization, while those in the Medicare population most commonly had comprehensive insurance. In both the Commercial and Medicare populations, the pre- and post-MAW cohorts had significantly higher CCI scores and a significantly longer stay for the index hip fracture hospitalization. Furthermore, the pre- and post-MAW cohorts in the Medicare population and the post-MAW cohort in the Commercial population had significantly higher costs for their index hospitalization. In the Commercial population, patients in all cohorts were most frequently discharged to home followed by SNF. In contrast, patients in the Medicare population had different distribution of discharge status based upon MAW status. Specifically, patients in the no-MAW cohort were most frequently discharged to home, while those with pre- or post-MAW were most commonly discharged to a SNF, followed by home and a short-term hospital.
Table 3 summarizes the healthcare utilization over the 12-month pre- and post-periods. For both insurance populations (Commercial and Medicare), patients in the MAW (pre- or post-) cohorts had significantly more total hospital days and outpatient hospital visits in both the pre- and post-periods. In addition, patients in the pre-MAW and post-MAW cohorts were more likely to have used a SNF, to have had a home health visit, or to have had occupational therapy in the post-period relative to the no-MAW patients. Over 60 % of the Commercial patients used physical therapy, 23–45 % had a SNF stay, and 12–19 % had an inpatient rehabilitation stay over the 12-month post-period. In comparison, 62–83 % of the Medicare patients stayed at a SNF, 22–37 % had a physical therapy visit, and only 2–3 % had an inpatient rehabilitation stay.
The unadjusted healthcare costs in the pre- and post-periods for each cohort were summarized in Figs. 1 and 2. Both the pre-MAW and post-MAW cohorts generally had higher costs than the no-MAW patients. In the Commercial population, pre-MAW and post-MAW patients had significantly higher total costs ($96,387 and $35,079 versus $ 24,564; both p < 0.05) than those in the no-MAW cohort in the pre-period with the largest share of costs contributed by inpatient setting; patients in the pre-MAW cohort ($91,643) and post-MAW cohort ($69,202) had higher total costs compared with no-MAW cohort ($39,296; both p < 0.05) in the post-period. In general, costs increased in the 12-month post-hip fracture index hospital stay compared with the 12 months prior among those in the Commercial population, although total costs remained the same for those in the pre-MAW cohort ($91,634 versus $96,387, p = 0.728 [data not shown]). For patients in the Medicare population, pre- and post-MAW cohorts had significantly higher pre- and post-period total costs, with the largest share of costs being outpatient costs. Total costs increased for all three cohorts in the Medicare population when comparing the pre-period to the post-period, with the biggest cost increase in the post-MAW cohort ($16,397 versus $48,589).

Unadjusted healthcare costs over the 12-month pre-period

Unadjusted healthcare costs over the 12-month post-period
The impact of MAW on direct healthcare costs controlling for cross-cohort differences is presented in Fig. 3. Among the Commercial patients, those in the pre- and post-MAW cohorts had significantly higher marginal total costs than the no-MAW patients (cost difference, $18,679 pre-MAW and $25,496 post-MAW; both p < 0.05). Similar to results from the Commercial patients, the Medicare patients in the pre- and post-MAW cohorts had significantly higher total marginal costs than the no-MAW patients ($7,308 pre-MAW, $18,753 post-MAW; p < 0.05). However, most of these cost differences were from the outpatient costs ($5,783 pre-MAW, $13,301 post-MAW; both p < 0.05).

Marginal difference in healthcare costs in 1 year post-hip fracture surgery
Table 4 presents factors associated with re-hospitalization in the year after the initial hospitalization for hip fracture. In general, a diagnosis of MAW was associated with a significantly higher likelihood of being hospitalized. Specifically, the likelihood of being hospitalized for any cause for Commercial patients in the post-MAW cohort was 1.76 (95 % CI, 1.42–2.20) times as high as that for no-MAW patients, and the likelihood increased to 1.93 (95 % CI, 1.46–2.54) times for a fracture-related hospitalization. Similarly, Medicare patients in the post-MAW cohort were found to be 1.75 (95 % CI, 1.61–1.90) times to be hospitalized for any cause and 1.72 (95 % CI, 1.52–1.96) times for a fracture-related hospitalization compared with those with no-MAW. Patients in the Commercial pre-MAW cohort were 1.60 (95 % CI, 1.11–2.31) times to be hospitalized for any cause, while those in the Medicare cohort were 1.32 (95 % CI, 1.05–1.66) times to have a fracture-related hospitalization, compared with those with no-MAW. A higher CCI (2 and above) and a discharge to SNF were both predictors of hospitalization in the post-period. Pre-period hospitalization, ER, or outpatient hospital visits were also significantly associated with a higher likelihood of hospitalization in the post-period, except for fracture-related hospitalization in the Commercial population.
Discussion
Age-related MAW “has been indicated as a reliable marker of frailty and poor prognosis among the oldest individuals” [18]. Among hip fracture patients, in particular, the presence of MAW is associated with poor recovery in mobility [10] and poor physical functioning [11]. Previous research has shown that elderly patients tend to decline physiologically and functionally following hip fracture surgery [19] and that these declines include MAW [20]. However, no previous research has compared the healthcare resource use, costs, or risk of re-hospitalization among hip fracture patients with and without MAW. This study adds to the body of literature on the impact of MAW on healthcare utilization and costs.
The majority of the hip fracture patients in this study were found in the Medicare (65 years and older) population. This finding is consistent with US-wide survey data, which have shown the rate of total hip replacement to be twice as high in inpatients age 65 years and over (33.8 per 10,000 population) relative to their counterparts ages 45–64 years (12.3 per 10,000 population) [21], as well as with a recent study of patients with osteoporotic hip fracture reporting that 90 % of these patients were 65 years or older [22]. Additionally, patients with MAW in our Medicare population were significantly older than those without MAW; this finding is consistent with previous reports that declines in muscle mass and strength are more likely to occur with advancing age, due to age-related metabolic and physiologic changes [23, 24].
Across both populations and all cohorts, the hip fracture patients in this study were more likely to be female than male. This is consistent with findings from previous research which found the rate of hip fracture to be nearly twice as high among women as among men [25, 26] and women generally having higher rates of musculoskeletal disorders [27, 28] and osteoporosis [29] relative to men. The pre-MAW Commercial patients in this study had significantly greater odds of being female relative to their no-MAW counterparts. Future study may need to explore what caused such distribution and whether additional screening for MAW is needed among the under age 65 years women who have hip fracture.
Hip fracture patients with MAW in this study were more likely to be from the Southern region of the United States and less likely to be from the Western states. These findings are in agreement with numerous nationwide health statistics showing the South to have poorer health and the West to have better health [30]. In addition, national statistics have indicated that the highest number of total hip replacements is in the South, while the lowest is in the West [21].
Among both the Commercial and Medicare populations, those with MAW were generally in poorer health, compared with those with no-MAW. Specifically, patients in the pre-MAW and post-MAW cohorts had higher CCI and a greater likelihood of pre-period hospitalization relative to patients in the no-MAW cohort. These findings support recent research among older adults showing an association between frailty and chronic disease [31]. In addition, previous research has found that “individuals with chronic diseases often live a sedentary lifestyle, which leads to physical de-conditioning” [32]. All patients in the pre-MAW cohort as well as Medicare patients in the post-MAW cohort were more likely to have osteoarthritis or osteoporosis. Previous research has likewise indicated that older patients with osteoarthritis are at high risk for age-related MAW [12, 18] and for bone fracture [33]. Future studies may need to examine the impact of comorbidities on patients with MAW after hip fracture.
The hip fracture patients with MAW in this study used more healthcare resources relative to their counterparts without MAW. Specifically, among both the Commercial and Medicare populations, patients with MAW had longer hospital stays, more physician office visits, and more outpatient hospital and ER visits, as well as more use of SNFs, occupational therapy, and inpatient rehabilitation services. These results support earlier research showing deficits in muscle strength to be associated with higher rates of functional limitation and worse outcomes among all older individuals [34, 35]. Additionally, findings from this study are consistent with previous studies which have found muscle weakness to be associated with longer lengths of hospital stay and more post-operative complications among surgical patients [36, 37]. In particular, the results of our study support previous investigations linking loss of muscle strength to poorer recovery after surgery for hip fracture [10]. These findings suggest that paying attention to MAW among patients with hip fracture may help the post-surgical recovery.
Previous estimates, based on national survey data, of the cost of an initial hospitalization for hip fracture have ranged from $9,200 to $12,100 [38, 39], while costs in the year after hip fracture have ranged from $13,585 to $29,800 [38, 40, 41]. Among the Medicare patients in our present study, costs of index hospitalization ranged from $19,299 to $21,056, while unadjusted costs in the 1 year post-fracture ranged from $28,653 to $48,589. These results appear to be roughly consistent with inflation adjustment of previous estimates. Patients in the Commercial population experienced higher costs than those in the Medicare population, a finding which is consistent with the fact that Medicare and Commercial insurances have different rate of reimbursement.
No previous study has compared the costs of hip fracture patients with and without MAW. Patients with MAW in this study had not only higher pre- and post-period healthcare resource use, but also higher costs, including higher inpatient, outpatient, some pharmacy, and total costs, and these higher costs were seen in both the pre- and post-periods. In both the insurance populations, the index hospital stay medical costs were the highest for patients diagnosed with MAW during or after their index hospitalization. The timing of MAW diagnosis also had an impact on healthcare costs: Pre-MAW patients had similar total costs (cost difference < $7,300) in both the pre- and post-periods, but post-MAW patients had higher post-period than pre-period costs (cost difference > $31,000). These findings suggest that programs designed to mitigate or prevent MAW during or after the inpatient stays for hip fracture might significantly reduce the overall costs of hip fracture. Further studies are needed to determine what kinds of interventions will be most cost-effective in preventing MAW among elderly patients recuperating from hip fracture.
Limitations
The results of this study should be interpreted in the context of the following limitations. First, the use of diagnostic codes is not as rigorous as formal diagnostic assessments for identifying study subjects and such codes may not be applied uniformly across providers. Second, the analysis focused exclusively on patients with medical and prescription benefit coverage who did not have prior hip fracture and also survived from their hip fracture for at least 1 year, thus this limitation may affect the generalizability of the findings. Third, the use of medical claims data precludes the assessment of quality-of-life outcomes or indirect costs. Fourth, unobservable confounders might have biased the estimates. Finally, the findings from this analysis can be interpreted as association and not causation due to its study design.
Conclusions
This analysis of patients with hip fractures showed that those with MAW had a greater burden of illness, higher resource use, and higher costs as compared with the patients without MAW. Patients with MAW diagnosed during or after the index hip fracture hospitalization had the greatest cost increase from the pre-period to the post-period. In addition, hip fracture patients who had MAW, more comorbidities, or greater disability based on discharge status after the initial hospitalization had significantly higher odds of being re-hospitalized within 1 year. The results of this study suggest that the mitigation of MAW among elderly patients may significantly lessen the humanistic and economic burden associated with fractures of the hip.
References
Bischoff-Ferrari HA (2011) The role of falls in fracture prediction. Curr Osteoporos Rep 9(3):116–121
Bass E, French DD, Bradham DD, Rubenstein LZ (2007) Risk-adjusted mortality rates of elderly veterans with hip fractures. Ann Epidemiol 17(7):514–519
Braithwaite RS, Col NF, Wong JB (2003) Estimating hip fracture morbidity, mortality and costs. J Am Geriatr Soc 51(3):364–370
Hopley C, Stengel D, Ekkernkamp A, Wich M (2010) Primary total hip arthroplasty versus hemiarthroplasty for displaced intracapsular hip fractures in older patients: systematic review. BMJ 340:c2332–c2332, jun11 1
Cooper C, Campion G, Melton LJ 3rd (1992) Hip fractures in the elderly: a world-wide projection. Osteoporos Int 2(6):285–289
National Center for Health Statistics (US) (2010) “Health, United States, 2009; with special feature on medical technology,” National Center for Health Statistics (US), Hyattsville (MD) Jan
American Academy of Orthopaedic Surgeons, “Hip fractures,” aaos.org, [Online]. Available: http://orthoinfo.aaos.org/topic.cfm?topic=A00392Apr 2009
Butler M, Forte M, Kane R et al (2009) “Treatment of common hip fractures. Rockville (MD): Agency for Healthcare Research and Quality (US)”, Evidence reports/technology assessments vol. no. 184, Aug
Creditor MC (1993) Hazards of hospitalization of the elderly. Ann Intern Med 118(3):219–223
Visser M, Harris TB, Fox KM, Hawkes W, Hebel JR, Yahiro JY, Michael R, Zimmerman SI, Magaziner J (2000) Change in muscle mass and muscle strength after a hip fracture: relationship to mobility recovery. J Gerontol A Biol Sci Med Sci 55(8):M434–M440
Bhave A, Marker DR, Seyler TM, Ulrich SD, Plate JF, Mont MA (2007) Functional problems and treatment solutions after total hip arthroplasty. J Arthroplasty 22(6 Suppl 2):116–124
Rasch A, Byström AH, Dalén N, Martinez-Carranza N, Berg HE (2009) Persisting muscle atrophy two years after replacement of the hip. J Bone Joint Surg Br 91(5):583–588
Charlson ME, Charlson RE, Peterson JC, Marinopoulos SS, Briggs WM, Hollenberg JP (2008) The Charlson comorbidity index is adapted to predict costs of chronic disease in primary care patients. J Clin Epidemiol 61(12):1234–1240
The Bureau of Labor Statistics, “Databases, tables & calculators by subject: inflation and prices”
Greene W H (2002) Econometric analysis, 5th ed. Upper Saddle River, NJ, Prentice Hall
Afifi AA, Kotlerman JB, Ettner SL, Cowan M (2007) Methods for improving regression analysis for skewed continuous or counted responses. Annu Rev Public Health 28(1):95–111
Efron B, Tibshirani R (1993) An introduction to the bootstrap. Boca Raton, FL, CRC Press
Landi F, Liperoti R, Fusco D, Mastropaolo S, Quattrociocchi D, Proia A, Russo A, Bernabei R, Onder G (2012) Prevalence and risk factors of sarcopenia among nursing home older residents. J Gerontol A Biol Sci Med Sci 67(1):48–55
Wehren LE, Hawkes WG, Hebel JR, Orwig DL, Magaziner J (2005) Bone mineral density, soft tissue body composition, strength, and functioning after hip fracture. J Gerontol A Biol Sci Med Sci 60(1):80–84
Fox KM, Magaziner J, Hawkes WG, Yu-Yahiro J, Hebel JR, Zimmerman SI, Holder L, Michael R (2000) Loss of bone density and lean body mass after hip fracture. Osteoporos Int 11(1):31–35
Centers for Disease Control and Prevention (2010) “National Hospital Discharge Survey: 2006 annual summary,” Vital and Health Statistics Number 168, Dec
Pasoto S G, Yoshihara L A K, Maeda L C, Bernik M M S, Lotufo P A, Bonfa E, Pereira R M R (2011) “Osteoporotic hip fractures in non-elderly patients: relevance of associated co-morbidities,” Rheumatol. Int: Sep
Heuberger RA (2011) The frailty syndrome: a comprehensive review. J Nutr Gerontol Geriatr 30(4):315–368
Topinková E (2008) Aging, disability and frailty. Ann Nutr Metab 52 Suppl 1:6–11
Brauer CA, Coca-Perraillon M, Cutler DM, Rosen AB (2009) Incidence and mortality of hip fractures in the United States. JAMA 302(14):1573–1579
Abrahamsen B, van Staa T, Ariely R, Olson M, Cooper C (2009) Excess mortality following hip fracture: a systematic epidemiological review. Osteoporos Int 20(10):1633–1650
Bhattacharya A, Leigh JP (2011) Musculoskeletal disorder cots and medical claim filing in the US retail trade sector. Ind Heal 49:517–522
Wijnhoven HAH, de Vet HCW, Picavet HSJ (2006) Prevalence of musculoskeletal disorders is systematically higher in women than in men. Clin J Pain 22(8):717–724
Burroughs K, Walker K (2012) “Hip fractures in adults,” UpToDate, no. Topic 226, Version 12.0
Milken Institute, “An unhealthy America: the economic burden of chronic disease.” Santa Monica, CA, Milken Institute 2012
Weiss CO (2011) Frailty and chronic diseases in older adults. Clin Geriatr Med 27(1):39–52
Pang MY (2010) Whole body vibration therapy in fracture prevention among adults with chronic disease. World J Orthop 1(1):20–25
Dennison E M, Compston J E, Flahive J, Siris E S, Gehlbach S H, Adachi J D, Boonen S, Chapurlat R, Díez-Pérez A, Anderson Jr F A, Hooven F H, Lacroix A Z, Lindsay R, Netelenbos J C, Pfeilschifter J, Rossini M, Roux C, Saag K G, Sambrook P, Silverman S, Watts N B, Greenspan S L , Premaor M, Cooper C (2012) “Effect of co-morbidities on fracture risk: findings from the Global Longitudinal Study of Osteoporosis in Women (GLOW)”. Bone: Mar
Marzetti E, Leeuwenburgh C (2006) Skeletal muscle apoptosis, sarcopenia and frailty at old age. Exp Gerontol 41(12):1234–1238
Woods JL, Iuliano-Burns S, King SJ, Strauss BJ, Walker KZ (2011) Poor physical function in elderly women in low-level aged care is related to muscle strength rather than to measures of sarcopenia. Clin Interv Aging 6:67–76
Mahalakshmi VN, Ananthakrishnan N, Kate V, Sahai A, Trakroo M (2004) Handgrip strength and endurance as a predictor of postoperative morbidity in surgical patients: can it serve as a simple bedside test? Int Surg 89(2):115–121
Sultan P, Hamilton MA, Ackland GL (2012) Preoperative muscle weakness as defined by handgrip strength and postoperative outcomes: a systematic review. BMC Anesthesiol 12:1
Chrischilles E, Shireman T, Wallace R (1994) Costs and health effects of osteoporotic fractures. Bone 15(4):377–386
Tosteson AN, Rosenthal DI, Melton LJ 3rd, Weinstein MC (1990) Cost effectiveness of screening perimenopausal white women for osteoporosis: bone densitometry and hormone replacement therapy. Ann Intern Med 113(8):594–603
U. S. C. O. of T (1993) Assessment, hip fracture outcomes in people age 50 and over: mortality, service use, expenditures, and long-term functional impairment. The Office
Cummings SR, Rubin SM, Black D (1990) “The future of hip fractures in the United States. Numbers, costs, and potential effects of postmenopausal estrogen,”. Clin Orthop Relat Res 252:163–166
Acknowledgments
The authors would like to thank HealthMetrics Outcomes Research for their writing assistance.
Conflicts of interest
Dr. Zhao was employed by Eli Lilly and Company when this study was carried out. During Dr. Zhao’s employment with Eli Lilly and Company, she owned stock in the company. United BioSource was compensated by Eli Lilly and Company for its work on the project.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Zhao, Y., Chen, SY., Lee, YC. et al. Clinical and economic characteristics of hip fracture patients with and without muscle atrophy/weakness in the United States. Arch Osteoporos 8, 127 (2013). https://doi.org/10.1007/s11657-013-0127-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11657-013-0127-2