
Abstract
Close to 75% of hip and non-hip fractures occur among seniors age 65 years and older. Notably, the primary risk factor for a hip fracture is a fall, and over 90% of all fractures occur after a fall. Thus, critical for the understanding and prevention of fractures at later age is their close relationship with muscle weakness and falling. In fact, antiresorptive treatment alone may not reduce fractures among individuals 80 years and older in the presence of nonskeletal risk factors for fractures despite an improvement in bone metabolism. This article will review the epidemiology of falls, and their importance in regard to fracture risk. Finally, fall prevention strategies and how these translate into fracture reduction are evaluated based on data from randomized controlled trials.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Thirty percent of those 65 years or older and 40–50% of those 80 years or older report having had a fall over the past year [1, 2]. Serious injuries occur with 10–15% of falls, resulting in fractures in 5% and hip fracture in 1–2% [3]. As an independent determinant of functional decline [4], falls lead to 40% of all nursing home admissions [5]. The primary risk factor for a hip fracture is a fall, and over 90% of all fractures occur after a fall [6]. Recurrent fallers may have close to fourfold increased odds of sustaining a fall-related fracture compared to individuals with a single fall [7]. As the number of seniors 65 years of age and older is predicted to increase from 25–40% by 2030 [8–12], the number of fall-related fractures will increase substantially. Notably, even today 75% of fractures occur among seniors age 65 years and older [13], and by 2050 the worldwide incidence in hip fractures is expected to increase by 240% among women and 310% among men [14]. Thus, therapeutic interventions that are effective in fall prevention are urgently needed.
Fall Definition and Inclusion of Fall Risk in Fracture Risk Prediction
Buchner et al. [15] created a useful fall definition for the common data base of the FICSIT (Frailty and Injuries: Cooperative Studies of Intervention Techniques) trials. Falls were defined as “unintentionally coming to rest on the ground, floor, or other lower level.” Coming to rest against furniture or a wall was not counted as a fall [15]. Challenging for their assessment is that falls tend to be forgotten if not associated with significant injury [16], requiring short periods of follow-up. Thus, high-quality fall assessment in older persons requires a prospective ascertainment of falls and their circumstances, ideally in short periods of time (< 3 months) [16].
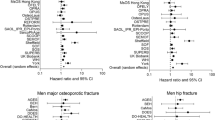
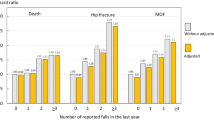
Fall reports may be performed by postcards, phone calls, or diary/calendar, although the usefulness and comprehensiveness of different ascertainment methods have not been compared directly. Notably, fall assessment has not been standardized across randomized controlled trials (RCTs) or large epidemiologic data sets [17], which prevented falls to be included in the World Health Organization FRAX tool (http://www.shef.ac.uk/FRAX/) that estimates the probability of a major osteoporotic fracture in the next 10 years [17]. Based on one Australian cohort study (Dubbo study), the Garvan nomogram has been developed as an alternative fracture prediction tool that includes falling as a risk factor of fracture (www.fractureriskcalculator.com). In a comparative assessment, however, the predictive accuracy of the two tools showed similar performance in postmenopausal women [18]. One explanation for a similar predictive accuracy between FRAX and the Garvan nomogram may be the relatively long time interval of fall assessment in the Garvan nomogram (fall recall in the last 12 months), which may lead to the underreporting of falls not associated with significant injury [16]. Notably, however, there was a suggestion that the Garvan nomogram had greater fracture predictive accuracy among men compared with FRAX [18, 19].
Fall Mechanics and Risk of Fracture
Mechanistically, the circumstances [20] and the direction [21] of a fall determine the type of fracture, whereas bone density and factors that attenuate a fall (eg, better strength or better padding) critically determine whether a fracture will take place when the faller lands on a certain bone [22]. Moreover, falling may affect bone density through increased immobility from self-restriction of activities [23]. It is well known that falls may lead to psychological trauma known as fear of falling [24]. After their first fall, about 30% of persons develop fear of falling [23] resulting in self-restriction of activities [23], and decreased quality of life. In support of the concept that falling is a key determinant of fracture risk, antiresorptive treatment alone may not reduce fractures among individuals 80 years and older in the presence of nonskeletal risk factors for fractures despite an improvement in bone metabolism [25].
Further, consistent with the understanding that factors unrelated to bone are at play in fracture epidemiology, the circumstances of different fractures are strikingly different. Hip fractures tend to occur in less active individuals falling indoors from a standing height with little forward momentum, and they tend to fall sideways or straight down on their hip [22]. Conversely, other nonvertebral fractures (eg, distal forearm or humerus fractures) tend to occur among more active older individuals who are more likely to be outdoors and have a greater forward momentum when they fall [26].
Supporting the notion of bone not to be seen in isolation, fracture risk due to falling is increased among individuals with osteoarthritis of the weight-bearing joints despite having increased bone density compared with controls [27]. One prospective study found that prevalent knee pain due to osteoarthritis increased the risk of falling by 26% and the risk of hip fracture twofold [28]. A most recent study applied a biomechanical risk measure, the factor-of-risk, for the prediction of hip fracture risk [29]: it is the ratio of force on the hip in a fall to femoral strength, and 1 standard deviation increase in peak factor-of-risk was associated with a 1.88-fold increased risk of hip fracture in men and a 1.23-fold increased risk of hip fracture in women. Notably, examining the components of factor-of-risk, fall force, and soft tissue thickness were predictive of hip fracture risk independent of femoral strength estimated from bone mineral density [29].
Risk Factors for Falls
Falls are a hallmark of age and becoming frail, and falls are often heralded by the onset of gait instability, visual impairment or its correction by multifocal glasses, drug treatment with antidepressants, anticonvulsants/barbiturates, or benzodiazepines, weakness, cognitive impairment, vitamin D deficiency, poor mental health, home hazards, or often a combination of several risk factors [30, 31]. The seemingly inseparable relationship of falls to worsening health status and the complexity of factors involved in falling has led to pessimism on the part of physicians when faced with falling, especially recurrent falling. However, there is a growing body of literature that should encourage the standardized assessment of falls and application of fall prevention strategies for fracture prevention.
Fall Prevention Strategies
Fall prevention by risk factor reduction has been tested in several approaches. Multifactorial approaches, such as medical and occupational therapy assessment or adjustment in medications, behavioral instructions and exercise programs, as demonstrated in the PROFET (Prevention of Falls in the Elderly Trial) [32] and FICSIT trials [33], as well as single intervention strategies, such as Tai Chi balance training [34] and exercise [33] reduced falls by 25–50%. Multifactorial approaches may be especially useful in high-risk populations for falls, such as older individuals in care institutions [35]. Significant limitations of multifactorial interventions and exercise programs are their cost, high implementation time, and limited long-term adherence. The latter may explain the lack of data regarding fracture prevention with these interventions.
Notably, however, exercise as a strategy of fall prevention may be applied at a smaller expense when the program is instructed but unsupervised. Such a home exercise program reduced falls in a randomized trial by Campbell et al. [36] among community-dwelling elderly women age 80 years and older. Consistently, a simple unsupervised exercise home program, instructed during acute care after hip fracture repair, reduced falls significantly by 25% over 12-month follow-up among 173 senior hip fracture patients with a mean age of 84 years [37•]. Although not powered for a fracture end point, there was a suggestion that the unsupervised home exercise program contributed to reduction in repeat fractures among acute hip fracture patients (relative fracture rate difference was −56% for the exercise home program vs control; 95% CI, −82%, +9%; P = 0.08) [37•].
Tai Chi has been successful in reducing falls among healthy older individuals [34, 38], and physically inactive community-dwelling older individuals [39], whereas frail older individuals [40] and fallers [38] may not benefit as much. Furthermore, Tai Chi may not improve bone density [41], and fracture prevention has not been explored as an end point with Tai Chi intervention programs.
As an extension of exercise, programs that support dual tasking may be valuable for fall prevention. Earlier studies suggested that fall risk is increased in seniors unable to walk while talking (stop walking when talking [42, 43]). Thus, dual tasking assessments may best identify those at the greatest risk of falling and programs that improve dual tasking may be useful in fall prevention at a higher age. This concept was tested in a recently published trial which showed that a music-based multitask exercise program improved gait and balance and reduced fall risk significantly by 39% in community-dwelling seniors [44•].
Fall Prevention Strategies with Evidence for Fracture Reduction
Two interventions among older individuals resulted in both fall and fracture reduction. One is cataract surgery with limited evidence from one trial. A total of 306 women over 70 years of age, with cataract, were randomized to expedited (~ 4 weeks) or routine (12 months wait) surgery. Over a 12-month follow-up, the rate of falling was reduced by 34% in the expedited group (rate ratio, 0.66; 95% CI, 0.45–0.96) accompanied by a significantly lower number of persons with a new fracture (P = 0.04) [45].
With evidence from several double-blind RCTs (12 RCTs for fractures and 8 RCTs for falls) summarized in two 2009 meta-analyses, supplementation with vitamin D should reduce the risk of falls [46] and nonvertebral fractures, including those at the hip [47], by about 20%. Notably, however, for both end points, this benefit was dose-dependent and only observed at an adherence-adjusted dose greater than 480 IU per day for fractures [47], and a treatment dose of at least 700 IU per day for falls [46].
Muscle weakness is an important risk factor for falls and is a prominent feature of the clinical syndrome of vitamin D deficiency [48]. Thus, muscle weakness due to vitamin D deficiency may plausibly mediate fracture risk through an increased susceptibility to falls. The vitamin D receptor is expressed in human muscle tissue [49, 50•], and vitamin D bound to its nuclear receptor in muscle tissue may lead to de novo protein synthesis [51, 52], followed by a relative increase in the diameter and number of fast type II muscle fibers [52]. Notably, fast type II muscle fibers decline with age relative to slow type I muscle fibers resulting in an increased propensity to fall [53].
The Institute of Medicine (IOM) did a thorough review on the effect of vitamin D on fall prevention in 2010 [54••]. However, their synopsis—that the evidence of vitamin D on fall prevention is inconsistent—is in contrast to the 2011 assessment of the Agency for Healthcare Research and Quality for the US Preventive Services Task Force [55••], the 2010 American Geriatric Society/British Geriatric Society Clinical Practice Guideline [56], and the 2010 assessment by the International Osteoporosis Foundation (IOF) [57••], all three of which identified vitamin D as an effective intervention to prevent falling in older adults reviewing the same evidence. Notably, the main inconsistency raised by the IOM is based on four studies that cannot be considered reliable indicators of true treatment efficacy, as those studies used low-dose vitamin D [58], had less than 50% adherence [59], had a low-quality fall assessment [60], or used one large bolus dose of vitamin D among seniors in unstable health [61]. Further, including these four studies in a pooled analysis of a total of 12 blinded and open-design trials evaluated by the IOM, there was a significant benefit overall (odds ratio [OR], 0.89; 95% CI, 0.80–0.99), most pronounced in 6 of 12 studies that fulfilled the criteria for a high-quality fall ascertainment (OR, 0.79; 95% CI, 0.65–0.96) [54••]. As falling is a challenging end point to assess as discussed above [62], the latter analysis by the IOM restricted to the six trials with high-quality fall assessment may best reflect true treatment efficacy with a 21% fall reduction. Further, these finding support the 2009 meta-analysis of eight double-blind RCTs with a high-quality fall ascertainment, also showing a significant benefit with a 19% fall reduction based on the relative risk of individual trials that gave a higher dose of vitamin D [46].
The IOM raised several issues with the 2009 meta-analysis [54••], which were addressed by the authors in a 2011 rebuttal [63•]. In the re-analysis suggested by the IOM, the authors confirmed their earlier finding of a dose-response association: there was a significant reduction in the odds of falling based on all eight trials (OR, 0.73 [0.62, 0.87]); however, this benefit was driven by trials that tested high-dose vitamin D (700–1000 IU vitamin D per day), which reduced the odds of falling by 34% (OR, 0.66 [0.53, 0.82]), whereas low-dose vitamin D did not reduce the odds of falling (OR, 1.14 [0.69, 1.87]) [63•]. Notably, a dose-response relationship between vitamin D and fall and fracture reduction is supported by epidemiologic data showing a significant positive trend between serum 25(OH)D concentrations and hip bone density [64] and lower extremity strength [65, 66].
Finally, it is important to note that vitamin D may address several components of the fall-fracture construct, including strength [67], balance [68], lower extremity function [65, 66], falling [69, 70], bone density [64, 71], the risk of hip and nonvertebral fractures [72], and the risk of nursing home admission [73]. In a most recent trial that tested 2000 IU of vitamin D per day to the current standard of care of 800 IU of vitamin D per day in a double-blind RCT of 173 acute hip fracture patients, the higher dose of vitamin D did not reduce the rate of falls superior to 800 IU of vitamin D [37•]. However, the higher dose compared with 800 IU of vitamin D reduced the rate of hospital readmission significantly by 39%, which was driven by a significant 60% reduction of fall-related injuries, primarily refracture [37•].
Conclusions
Fall risk reduction is a significant component of fracture prevention at older age and the public health impact of falls is significant. Falls can be reduced by several interventions, with vitamin D offering efficacy established in several RCTs extending to fracture reduction in some of the same trials. To study falls and the fall-fracture risk profile from different interventions and cohort studies better, fall definition and ascertainment need to be standardized.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Tinetti ME. Risk factors for falls among elderly persons living in the community. N Engl J Med. 1988;319:1701–7.
Campbell AJ, Reinken J, Allan BC, Martinez GS. Falls in old age: a study of frequency and related clinical factors. Age Ageing. 1981;10(4):264–70.
Fatalities and injuries from falls among older adults—United States, 1993–2003 and 2001–2005. MMWR Morb Mortal Wkly Rep. 2006;55(45):1221–4.
Tinetti ME, Williams CS. The effect of falls and fall injuries on functioning in community-dwelling older persons. J Gerontol A Biol Sci Med Sci. 1998;53(2):M112–9.
Tinetti ME, Williams CS. Falls, injuries due to falls, and the risk of admission to a nursing home. N Engl J Med. 1997;337(18):1279–84.
Cummings SR, Nevitt MC, Browner WS, Stone K, Fox KM, Ensrud KE, et al. Risk factors for hip fracture in white women. Study of osteoporotic fractures research group. N Engl J Med. 1995;332(12):767–73.
Pluijm SM, Smit JH, Tromp EA, Stel VS, Deeg DJ, Bouter LM, et al. A risk profile for identifying community-dwelling elderly with a high risk of recurrent falling: results of a 3-year prospective study. Osteoporos Int. 2006;17(3):417–25. Epub 2006 Jan 17.
EC. European economy: Special Report n° 1/2006. European Commission, Directorate-General for Economic and Financial Affairs. http://urbact.eu/fileadmin/corporate/pdf/news/Focus/Impact_public_finance_DGEco_EN.pdf
Eberstadt N., H. G. Europe’s coming demographic challenge: unlocking the value of health. American Enterprise Institute for Public Policy Research. 2007.
Europe Co. Recent demographic developments in Europe 2005 (2006) European population Committee of the Council of Europe: Strasbourg.
Eurostat. First demographic estimates for 2005: statistics in focus. http://eppeurostateceuropaeu/cache/ITY_OFFPUB/KS-NK-06-001/EN/KS-NK-06-001-ENPDF. 2006.
Lee RD. Global population aging and its economic consequences. Washington, DC: AEI Press, 2007. 2007.
Melton 3rd LJ, Crowson CS, O’Fallon WM. Fracture incidence in Olmsted County, Minnesota: comparison of urban with rural rates and changes in urban rates over time. Osteoporos Int. 1999;9(1):29–37.
Gullberg B, Johnell O, Kanis JA. World-wide projections for hip fracture. Osteoporos Int. 1997;7(5):407–13.
Buchner DM, Hornbrook MC, Kutner NG, Tinetti ME, Ory MG, Mulrow CD, et al. Development of the common data base for the FICSIT trials. J Am Geriatr Soc. 1993;41(3):297–308.
Cummings SR, Nevitt MC, Kidd S. Forgetting falls. The limited accuracy of recall of falls in the elderly. J Am Geriatr Soc. 1988;36(7):613–6.
Kanis JA, Borgstrom F, De Laet C, Johansson H, Johnell O, Jonsson B, et al. Assessment of fracture risk. Osteoporos Int. 2005;16(6):581–9. Epub 2004 Dec 23.
Sandhu SK, Nguyen ND, Center JR, Pocock NA, Eisman JA, Nguyen TV. Prognosis of fracture: evaluation of predictive accuracy of the FRAX algorithm and Garvan nomogram. Osteoporos Int.21(5):863–71.
van den Bergh JP, van Geel TA, Lems WF, Geusens PP. Assessment of individual fracture risk: FRAX and beyond. Curr Osteoporos Rep. 2010;8(3):131–7.
Cummings SR, Nevitt MC. Non-skeletal determinants of fractures: the potential importance of the mechanics of falls. Study of osteoporotic fractures research group. Osteoporos Int. 1994;4 Suppl 1:67–70.
Nguyen ND, Frost SA, Center JR, Eisman JA, Nguyen TV. Development of a nomogram for individualizing hip fracture risk in men and women. Osteoporos Int. 2007;17:17.
Nevitt MC, Cummings SR. Type of fall and risk of hip and wrist fractures: the study of osteoporotic fractures. The study of osteoporotic fractures research group. J Am Geriatr Soc. 1993;41(11):1226–34.
Vellas BJ, Wayne SJ, Romero LJ, Baumgartner RN, Garry PJ. Fear of falling and restriction of mobility in elderly fallers. Age Ageing. 1997;26(3):189–93.
Arfken CL, Lach HW, Birge SJ, Miller JP. The prevalence and correlates of fear of falling in elderly persons living in the community. Am J Public Health. 1994;84(4):565–70.
McClung MR, Geusens P, Miller PD, Zippel H, Bensen WG, Roux C, et al. Effect of risedronate on the risk of hip fracture in elderly women. Hip intervention program study group. N Engl J Med. 2001;344(5):333–40.
Graafmans WC, Ooms ME, Hofstee HM, Bezemer PD, Bouter LM, Lips P. Falls in the elderly: a prospective study of risk factors and risk profiles. Am J Epidemiol. 1996;143(11):1129–36.
Arden NK, Nevitt MC, Lane NE, Gore LR, Hochberg MC, Scott JC, et al. Osteoarthritis and risk of falls, rates of bone loss, and osteoporotic fractures. Study of osteoporotic fractures research group. Arthritis Rheum. 1999;42(7):1378–85.
Arden NK, Crozier S, Smith H, Anderson F, Edwards C, Raphael H, et al. Knee pain, knee osteoarthritis, and the risk of fracture. Arthritis Rheum. 2006;55(4):610–5.
Dufour AB, Roberts B, Broe KE, Kiel DP, Bouxsein ML, Hannan MT. The factor-of-risk biomechanical approach predicts hip fracture in men and women: the Framingham Study. Osteoporos Int. 2011.
Tinetti ME, Inouye SK, Gill TM, Doucette JT. Shared risk factors for falls, incontinence, and functional dependence. Unifying the approach to geriatric syndromes. Jama. 1995;273(17):1348–53.
Mowe M, Haug E, Bohmer T. Low serum calcidiol concentration in older adults with reduced muscular function. J Am Geriatr Soc. 1999;47(2):220–6.
Close J, Ellis M, Hooper R, Glucksman E, Jackson S, Swift C. Prevention of falls in the elderly trial (PROFET): a randomized controlled trial. Lancet. 1999;353:93–7.
Province MA, Hadley EC, Hornbrook MC, Lipsitz LA, Miller JP, Mulrow CD, et al. The effects of exercise on falls in elderly patients. A preplanned meta-analysis of the FICSIT Trials. Frailty and Injuries: Cooperative Studies of Intervention Techniques. Jama. 1995;273(17):1341–7.
Wolf SL, Barnhart HX, Kutner NG, McNeely E, Coogler C, Xu T. Reducing frailty and falls in older persons: an investigation of Tai Chi and computerized balance training. Atlanta FICSIT Group. Frailty and Injuries: Cooperative Studies of Intervention Techniques. J Am Geriatr Soc. 1996;44(5):489–97.
Oliver D, Connelly JB, Victor CR, Shaw FE, Whitehead A, Genc Y, et al. Strategies to prevent falls and fractures in hospitals and care homes and effect of cognitive impairment: systematic review and meta-analyses. Bmj. 2007;334(7584):82. Epub 2006 Dec 8.
Campbell AJ, Robertson MC, Gardner MM, Norton RN, Tilyard MW, Buchner DM. Randomised controlled trial of a general practice programme of home based exercise to prevent falls in elderly women. Bmj. 1997;315(7115):1065–9.
• Bischoff-Ferrari HA, Dawson-Hughes B, Platz A, Orav EJ, Stahelin HB, Willett WC, et al. Effect of high-dosage cholecalciferol and extended physiotherapy on complications after hip fracture: a randomized controlled trial. Arch Intern Med. 2010;170(9):813–20. The trial tests a simple home exercise program in acute hip fracture patients instructed during acute care compared to standard physiotherapy. The trial also tested 2000 IU vitamin D compared to 800 IU vitamin D per day in a 2x2 factorial design. The higher vitamin D dose resulted in a 39% reduction in hospital re-admission, which was driven by a 60% reduction in fall-related injury. The higher dose of vitamin D did not reduce falls superior to 800 IU vitamin D.
Voukelatos A, Cumming RG, Lord SR, Rissel C. A randomized, controlled trial of tai chi for the prevention of falls: the Central Sydney tai chi trial. J Am Geriatr Soc. 2007;55(8):1185–91.
Li F, Harmer P, Fisher KJ, McAuley E, Chaumeton N, Eckstrom E, et al. Tai Chi and fall reductions in older adults: a randomized controlled trial. J Gerontol A Biol Sci Med Sci. 2005;60(2):187–94.
Wolf SL, Sattin RW, Kutner M, O’Grady M, Greenspan AI, Gregor RJ. Intense tai chi exercise training and fall occurrences in older, transitionally frail adults: a randomized, controlled trial. J Am Geriatr Soc. 2003;51(12):1693–701.
Lee MS, Pittler MH, Shin BC, Ernst E. Tai chi for osteoporosis: a systematic review. Osteoporos Int. 2007;23:23.
Lundin-Olsson L, Nyberg L, Gustafson Y. Stops walking when talking as a predictor of falls in elderly people. Lancet. 1997;349(9052):617.
de Hoon EW, Allum JH, Carpenter MG, Salis C, Bloem BR, Conzelmann M, et al. Quantitative assessment of the stops walking while talking test in the elderly. Arch Phys Med Rehabil. 2003;84(6):838–42.
• Trombetti A, Hars M, Herrmann FR, Kressig RW, Ferrari S, Rizzoli R. Effect of music-based multitask training on gait, balance, and fall risk in elderly people: a randomized controlled trial. Arch Intern Med. 2011;171(6):525–33. Trombetti et al. test a new concept of dual tasking as a music-based coordination. Training in seniors at risk of falling and show a significant benefit on fall reduction in a controlled study design.
Harwood RH, Foss AJ, Osborn F, Gregson RM, Zaman A, Masud T. Falls and health status in elderly women following first eye cataract surgery: a randomised controlled trial. Br J Ophthalmol. 2005;89(1):53–9.
Bischoff-Ferrari HA, Dawson-Hughes B, Staehelin HB, Orav JE, Stuck AE, Theiler R, et al. Fall prevention with supplemental and active forms of vitamin D: a meta-analysis of randomised controlled trials. BMJ. 2009;339(1):339:b3692.
Bischoff-Ferrari HA, Willett WC, Wong JB, Stuck AE, Staehelin HB, Orav EJ, et al. Prevention of nonvertebral fractures with oral vitamin D and dose dependency: a meta-analysis of randomized controlled trials. Arch Intern Med. 2009;169(6):551–61.
Schott GD, Wills MR. Muscle weakness in osteomalacia. Lancet. 1976;1(7960):626–9.
Bischoff-Ferrari HA, Borchers M, Gudat F, Durmuller U, Stahelin HB, Dick W. Vitamin D receptor expression in human muscle tissue decreases with age. J Bone Miner Res. 2004;19(2):265–9.
• Ceglia L, da Silva Morais M, Park LK, Morris E, Harris SS, Bischoff-Ferrari HA, et al. Multi-step immunofluorescent analysis of vitamin D receptor loci and myosin heavy chain isoforms in human skeletal muscle. J Mol Histol. 2010;41(2–3):137–42. Ceglia et al. confirm earlier findings of the presence of the vitamin D receptor in muscle tissue.
Boland R. Role of vitamin D in skeletal muscle function. Endocrine Reviews. 1986;7:434–47.
Sorensen OH, Lund B, Saltin B, Andersen RB, Hjorth L, Melsen F, et al. Myopathy in bone loss of ageing: improvement by treatment with 1 alpha-hydroxycholecalciferol and calcium. Clin Sci (Colch). 1979;56(2):157–61.
von Haehling S, Morley JE, Anker SD. An overview of sarcopenia: facts and numbers on prevalence and clinical impact. J Cachex Sarcopenia Muscle.1(2):129–33.
•• Institute of Medicine. Dietary Reference Ranges for Calcium and Vitamin D. http://wwwiomedu/Reports/2010/Dietary-Reference-Intakes-for-Calcium-and-Vitamin-D/Report-Briefaspx. 2010. The IOM released new recommendations on vitamin D suggesting 600 IU vitamin D in all adults up to age 70 and 800 IU vitamin D per day in seniors age 70 years and older. These recommendations are primarily based on bone health.
•• Michael YL, Whitlock EP, Lin JS, Fu R, O’Connor EA, Gold R. Primary care-relevant interventions to prevent falling in older adults: a systematic evidence review for the US. Preventive services task force. Ann Intern Med. 2011;153(12):815–25. The preventive task forced reviewed all evidence from clinical trials and concluded that vitamin D is an effective strategy in fall prevention.
American Geriatric Society/British Geriatric Society Guidelines on Fall Prevention in older Persons. http://wwwamericangeriatricsorg/files/documents/health_care_pros/FallsSummaryGuidepdf. 2010.
•• Dawson-Hughes B, Mithal A, Bonjour JP, Boonen S, Burckhardt P, Fuleihan GE, et al. IOF position statement: vitamin D recommendations for older adults. Osteoporos Int. 2010;21(7):1151–4. The IOF released a position statement of vitamin D in May 2010 and recomments vitamin D supplementation at a dose of 800–1000 IU per day in all adults age 60 years and older to reduce their risk of falls and fracture. The 25(OH)D threshold for optimal fall and fracture prevention, as defined by the IOF, is 75 nmol/l (30 ng/ml).
Graafmans WC, Ooms ME, Hofstee HM, Bezemer PD, Bouter LM, Lips P. Falls in the elderly: a prospective study of risk factors and risk profiles. Am J Epidemiol. 1996;143(11):1129–36.
Grant AM, Avenell A, Campbell MK, McDonald AM, MacLennan GS, McPherson GC, et al. Oral vitamin D3 and calcium for secondary prevention of low-trauma fractures in elderly people (Randomised Evaluation of Calcium Or vitamin D, RECORD): a randomised placebo-controlled trial. Lancet. 2005;365(9471):1621–8.
Trivedi DP, Doll R, Khaw KT. Effect of four monthly oral vitamin D3 (cholecalciferol) supplementation on fractures and mortality in men and women living in the community: randomised double blind controlled trial. BMJ. 2003;326(7387):469.
Latham NK, Anderson CS, Lee A, Bennett DA, Moseley A, Cameron ID. A randomized, controlled trial of quadriceps resistance exercise and vitamin D in frail older people: the Frailty Interventions Trial in Elderly Subjects (FITNESS). J Am Geriatr Soc. 2003;51(3):291–9.
Cummings SR, Nevitt MC, Kidd S. Forgetting falls. J Am Geriatr Soc. 1988;36(7):613–6.
• Bischoff-Ferrari HA, Willett WC, Orav EJ, Kiel DP, Dawson-Hughes B. Re: Fall prevention with Vitamin D. Clarifications needed. http://wwwbmjcom/content/339/bmjb3692/reply. 2011. The authors confirm a dose-response association between vitamin D supplementation and fall reduction.
Bischoff-Ferrari HA, Dietrich T, Orav EJ, Dawson-Hughes B. Positive association between 25-hydroxy vitamin d levels and bone mineral density: a population-based study of younger and older adults. Am J Med. 2004;116(9):634–9.
Bischoff-Ferrari HA, Dietrich T, Orav EJ, Hu FB, Zhang Y, Karlson EW, et al. Higher 25-hydroxyvitamin D concentrations are associated with better lower-extremity function in both active and inactive persons aged > =60 y. Am J Clin Nutr. 2004;80(3):752–8.
Wicherts IS, van Schoor NM, Boeke AJ, Visser M, Deeg DJ, Smit J, et al. Vitamin D status predicts physical performance and its decline in older persons. J Clin Endocrinol Metab. 2007;6:6.
Bischoff HA, Stahelin HB, Dick W, Akos R, Knecht M, Salis C, et al. Effects of vitamin D and calcium supplementation on falls: a randomized controlled trial. J Bone Miner Res. 2003;18(2):343–51.
Pfeifer M, Begerow B, Minne HW, Abrams C, Nachtigall D, Hansen C. Effects of a short-term vitamin D and calcium supplementation on body sway and secondary hyperparathyroidism in elderly women. J Bone Miner Res. 2000;15(6):1113–8.
Broe KE, Chen TC, Weinberg J, Bischoff-Ferrari HA, Holick MF, Kiel DP. A higher dose of vitamin d reduces the risk of falls in nursing home residents: a randomized, multiple-dose study. J Am Geriatr Soc. 2007;55(2):234–9.
Bischoff-Ferrari HA, Orav EJ, Dawson-Hughes B. Effect of cholecalciferol plus calcium on falling in ambulatory older men and women: a 3-year randomized controlled trial. Arch Intern Med. 2006;166(4):424–30.
Dawson-Hughes B, Harris SS, Krall EA, Dallal GE. Effect of calcium and vitamin D supplementation on bone density in men and women 65 years of age or older. N Engl J Med. 1997;337(10):670–6.
Bischoff-Ferrari HA, Willett WC, Wong JB, Giovannucci E, Dietrich T, Dawson-Hughes B. Fracture prevention with vitamin D supplementation: a meta-analysis of randomized controlled trials. Jama. 2005;293(18):2257–64.
Visser M, Deeg DJ, Puts MT, Seidell JC, Lips P. Low serum concentrations of 25-hydroxyvitamin D in older persons and the risk of nursing home admission. Am J Clin Nutr. 2006;84(3):616–22. quiz 71–2.
Disclosure
Conflicts of interest: H.A. Bischoff-Ferrari: has been a consultant for Novartis, Amgen, DSM, MSD, and Nestlé; and has received grant support from Nestlé, DSM, and MSD.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bischoff-Ferrari, H.A. The Role of Falls in Fracture Prediction. Curr Osteoporos Rep 9, 116–121 (2011). https://doi.org/10.1007/s11914-011-0059-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11914-011-0059-y