
Objective
To assess racial/ethnic differences in multiple diabetes self-care behaviors.
Design
Cross-sectional study.
Participants
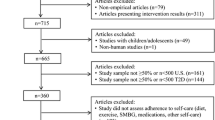
21,459 participants with diabetes in the 2003 Behavioral Risk Factor Surveillance survey.
Measurements
The study assessed self-care behaviors including physical activity, fruits/vegetables consumption, glucose testing, and foot examination, as well as a composite of the 4 self-care behaviors across racial/ethnic groups. Multiple logistic regression was used to assess the independent association between race/ethnicity, the composite variable, and each self-care behavior controlling for covariates. STATA was used for statistical analysis.
Results
Overall, 6% engaged in all 4 self-care behaviors, with a range of 5% in non-insulin users to 8% in insulin users. Blacks were less likely to exercise (OR 0.63, 95% CI 0.51, 0.79), while Hispanics and “others” were not significantly different from whites. Hispanics (OR 0.64, 95% CI 0.49, 0.82) and others (OR 0.69, 95% CI 0.49, 0.96) were less likely to do home glucose testing, while blacks were not significantly different from whites. Blacks (OR 1.42, 95% CI 1.12, 1.80) were more likely to do home foot examinations, while Hispanics and others were not significantly different from whites. Blacks (OR 0.56, 95% CI 0.36, 0.87) were less likely to engage in all 4 behaviors, while Hispanics and others were not significantly different from whites. There were no significant racial/ethnic differences in fruit and vegetable consumption.
Conclusions
Few patients engage in multiple self-care behaviors at recommended levels, and there are significant racial/ethnic differences in physical activity, dietary, and foot care behaviors among adults with diabetes.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
INTRODUCTION
Diabetes is a chronic debilitating condition that is associated with significant morbidity, mortality, and increased health care costs.1 Blacks and Hispanics have higher prevalence of diabetes, are disproportionately burdened with the complications and disability from diabetes, and are less likely to attain national targets for metabolic control.1,2 Effective diabetes self-management is essential to achieve optimal glycemic control and decrease the morbidity and mortality associated with diabetes. Studies have shown that people equipped with self-management skills have increased knowledge, improved self-management of blood glucose, improved dietary habits, and better glycemic control.3
Prior studies have examined the association between race/ethnicity and diabetes self-care behaviors.4–6 Although these studies yielded important findings, they all used data prior to 2003, they did not examine multiple self-care behaviors, and most did not adequately control for relevant confounding variables. Two studies used data from 1988 to 1994 National Health and Nutrition Examination surveys,4,5 while the other study used data from the 2001 Behavioral Risk Factor Surveillance survey (BRFSS).6 One study did not look at physical activity or diet,4 another did not look at home blood glucose monitoring or foot care,5 while the third study6 did not control for important confounders like access to care, BMI, insulin use, and diabetes education. The current study complements and improves on these prior studies by examining racial/ethnic differences in diabetes self-care across multiple behaviors, using a more recent nationally representative sample, and controlling for important confounding variables.
This study used the 2003 BRFSS to answer the following questions: (1) Are there racial/ethnic differences in multiple self-care behaviors like physical activity, fruits and vegetables consumption, home blood glucose testing, and home foot examination among adults with diabetes? (2) Is race/ethnicity an independent correlate of optimal self-care behavior after controlling for covariates? Based on a review of existing literature, we hypothesized that there would be significant racial/ethnic differences in multiple diabetes self-care behaviors after controlling for relevant confounders. We further hypothesized that blacks and Hispanics would be less likely to meet national guidelines for physical activity, fruits and vegetables consumption, home blood glucose testing, and home foot examination after controlling for relevant confounding variables.
RESEARCH DESIGN AND METHODS
Study Setting and Sample
We analyzed data from the 2003 BRFSS.7 The BRFSS is a state-based, random-digit-dialing telephone survey of the United States population sponsored by the Center for Disease Control. The BRFSS uses a complex sampling design involving stratification, clustering, and multistage sampling to yield nationally representative estimates. Details about the methodology of the 2003 BRFSS are available.8
Demographic and Socioeconomic Characteristics
We created 4 age categories: 18–34, 35–49, 50–64, and 65+ years. We combined race and ethnicity to create 4 racial/ethnic groups: non-Hispanic whites (whites), non-Hispanic blacks (blacks), Hispanics, and non-Hispanic other (other). Four categories of levels of education—<high school graduate, high school graduate, <college graduate, and college graduate—and 4 income categories—<$25,000, <$50,000, <$75,000, and $75,000+—were created. We defined marital status as married and not married, employment status as employed and unemployed, and insurance status as insured and uninsured. We defined access to care as visit to a health care provider within the previous 12 months and perceived health status as excellent/very good/good versus fair/poor. We defined BMI as the ratio of body weight in kilograms to height in meters squared and created 3 categories: <25.0, 25.0–29.9, and 30.0+. A person was deemed on insulin if they reported using insulin for treatment of diabetes.
Diagnosis of Diabetes and Diabetes Education
The diagnosis of diabetes was based on self-report. Diabetes education was based on the question “have you ever taken a course or class in how to manage your diabetes yourself?” Subjects were deemed to have received diabetes education if they responded “yes” to this question.
Diabetes Self-Care Behaviors
Respondents were asked several questions about diabetes self-care behaviors.
Physical Activity
This was computed by BRFSS based on questions about type, duration, and intensity of physical activity. Two categories of physical activity were created: meeting physical activity recommendations (defined as 30 or more minutes per day for 5 or more days per week of moderate activity or 20 or more minutes per day on 3 or more days of vigorous activity) and not meeting physical activity recommendations.
Fruits and Vegetables Consumption
This was assessed by asking respondents about their daily consumption of fruits and vegetables. Based on national guidelines, the consumption of fruits and vegetables was categorized as intake of <5 servings per days versus intake of 5 or more servings per day.
Home Blood Glucose Testing
To assess home blood glucose testing behavior, respondents were asked “about how often do you check your blood for glucose or sugar? Include times when checked by a family member or friend, but do not include times when checked by a health professional.” Clinical guidelines for diabetes9–11 recommend home blood glucose testing 1–3 times daily for all patients on insulin. The optimal testing frequency for patients with type 2 diabetes on oral agents is not known.9 Guideline recommendations for patients with type 2 diabetes on oral agents vary from at least twice daily10 to twice weekly.11 A dichotomous variable for frequency of testing was created—1 or more times per day versus less than once per day. Because of variation in recommended testing frequency for patients not on insulin, we stratified home blood glucose testing frequency by insulin use.
Home Foot Examination
Foot care behavior was assessed by asking respondents “about how often do you check your feet for any sores or irritations? Include times when checked by a family member or friend, but do not include times when checked by a health professional.” Current American Diabetes Association guidelines recommend daily home foot examination for patients with diabetes.9 A dichotomous variable for frequency of foot examination was created—1 or more times per day versus less than once per day.
Composite of Self-Care Behaviors
Based on the dichotomous variables for physical activity, consumption of fruits and vegetables, frequency of home blood glucose testing, and frequency of home foot examinations, a composite variable was created to assess how many respondents engaged in the 4 self-care behaviors measured. This composite variable was categorized as follows: engaged in at least 1 self-care behavior, engaged in at least 2 self-care behaviors, engaged in at least 3 self-care behaviors, and engaged in all 4 self-care behaviors. To account for variation in recommended home glucose testing frequency between patients on insulin and those not on insulin, we stratified frequency of engaging in all 4 self-care behaviors by insulin use.
Statistical Analyses
STATA version 8.012 was used for statistical analyses. We performed 3 types of analyses. First, we compared demographic characteristics of patients with diabetes by race/ethnicity. Second, we compared attendance of diabetes education classes and diabetes self-care behaviors by race/ethnicity using χ 2 statistics. We also computed the frequency of home blood glucose testing and frequency of engaging in all 4 self-care behaviors across racial/ethnic groups stratified by insulin use. Third, we ran separate multiple logistic regression models to assess the independent association between race/ethnicity and each self-care behavior, as well as the composite self-care variables. For each model, we used the dichotomous variable for each behavior or composite variable as the independent variable; race/ethnicity as the primary dependent variable; and age, sex, education, income, marital status, employment, insurance status, access to care, health status, BMI, attendance of diabetes education classes, and insulin use as covariates. We used insulin use as a surrogate for disease severity. We included all variables in the adjusted models because they were significantly different across racial/ethnic groups and were conceptually related to the outcomes of interest.
RESULTS
The 2003 BRFSS sample included 264,684 adults. Of this number, 21,459 (8.1%) had diabetes. Among adults with diabetes, 15,495 were white, 2,738 were black, 1,431 were Hispanic, and 1,795 belonged to other ethnic groups. Sixty-five percent of the sample were white, 51% were women, 37% were 65 years or older, 20% had less than high school education, and 46% had household incomes <$25,000. Sixty percent were married; 37% were employed; 50% reported that their health was excellent, very good, or good; 89% were insured; 93% had access to care; 48% had BMI ≥30; and 26% were on insulin. Table 1 compares the demographic characteristics of adults with diabetes by race/ethnicity. There were significant racial/ethnic differences by age, sex, education, income, marital status, employment, perceived health status, insurance, access to care, BMI, and insulin use.
In the sample, 51% attended a diabetes education class, 33% engaged in moderate to vigorous physical activity, 26% consumed 5+ servings of fruits and vegetables, 58% did home blood glucose testing at least once daily, 69% did home foot examinations at least daily, and 6% engaged in all 4 self-care behaviors at recommended levels. In stratified analysis, 85% of insulin users did home blood glucose testing at least once daily with a range of 89% in whites, 78% in blacks, 79% in Hispanics, and 81% in “others.” Among non-insulin users, 49% did home blood glucose testing at least once daily with a range of 50% in whites, 55% in blacks, 41% in Hispanics, and 42% in others. In the second stratified analysis, 8% of insulin users engaged in all 4 self-care behaviors at recommended levels, with a range of 9% in whites, 5% in blacks, 2% in Hispanics, and 10% in others. Among non-insulin users, 5% engaged in all 4 self-care behaviors at recommended levels, with a range of 6% in whites, 3% in blacks, 5% in Hispanics, and 5% in others.
Table 2 compares diabetes self-care behaviors by race/ethnicity. Blacks were most likely to attend diabetes education classes while Hispanics were least likely to attend diabetes education classes. Whites and others were more likely to meet physical activity recommendations. There was no significant racial/ethnic difference in consumption of fruits and vegetables. Blacks and whites were more likely to do home blood glucose testing at least once daily and to do home foot examinations at least once daily, while levels of home blood glucose testing and home foot examinations were lower in Hispanics and others.
Table 3 shows the adjusted odds of optimal self-care behaviors by race/ethnicity, using whites as the reference group. For physical activity, blacks were significantly less likely to exercise at recommended levels (OR 0.63, 95% CI 0.51, 0.79) while Hispanics and others were not significantly different from whites. For fruits and vegetables consumption, there were no significant differences across racial/ethnic groups. For home glucose testing, Hispanics (OR 0.64, 95% CI 0.49, 0.82) and others (OR 0.69, 95% CI 0.49, 0.96) were significantly less likely to test at least once daily compared to whites, while blacks were not significantly different from whites. For home foot examination, blacks (OR 1.42, 95% CI 1.12, 1.80) were significantly more likely to do home foot examinations at least once daily compared to whites, while Hispanics and others were not significantly different from whites. For all 4 self-care behaviors, blacks (OR 0.56, 95% CI 0.36, 0.87) were significantly less likely to engage in all 4 self-care behaviors compared to whites, while Hispanics and others were not significantly different from whites.
DISCUSSION
This study has 2 major findings. First, regardless of race/ethnicity, very few patients with diabetes engage in multiple diabetes self-care behaviors at recommended levels. Second, controlling for pertinent confounding variables, there are significant racial/ethnic differences in physical activity, dietary, and foot care behaviors among adults with diabetes.
This is the first population-based study to our knowledge to assess a composite of diabetes self-care behaviors across racial/ethnic groups. Across all racial/ethnic groups, very few patients performed all 4 self-care behaviors at recommended levels. Overall, only 6% of patients engaged in all 4 self-care behaviors at recommended levels. Because of variations in the recommended frequency of home blood glucose testing for diabetic patients not on insulin, we computed frequency of home blood glucose testing and engaging in all 4 self-care behaviors separately for insulin users and nonusers to account for the effect of insulin use. In the stratified analysis, frequency of home blood glucose testing was higher in insulin users (85%) than in non-insulin users (49%) and the proportion that engaged in all 4 self-care behaviors at recommended levels was higher in insulin users (8%) than in non-insulin users (5%). This shows that overall diabetes self-care is better among diabetic patients on insulin; however, the proportion that engaged in all 4 self-care behaviors at recommended levels (8%) is still relatively low and needs to improve. A substantial proportion of patients (∼90%) engaged in at least one self-care behavior, but the numbers declined considerably with the increasing number of self-care behaviors. Patients seemed to pay more attention to foot care and home glucose testing than they did to diet/nutrition and physical activity, even though evidence suggests that physical activity and diet have a very significant impact on metabolic control and risk of complication in patients with diabetes.13,14
There were significant racial/ethnic differences in physical activity and frequency of home blood glucose testing, but no significant racial/ethnic differences in consumption of fruits and vegetables. After adjusting for confounders, blacks were 2-fold less likely to engage in moderate/vigorous physical activity levels, which is consistent with the findings of other population-based studies in patients with diabetes.15,16 In contrast to an earlier finding that blacks and Hispanics were less likely to do home blood glucose testing at recommended levels,4 this study found that after adjusting for confounding, the likelihood of home blood glucose testing in blacks was not significantly different from that of whites, while Hispanics and others were less likely to test at recommended levels compared to whites. There were no significant racial/ethnic differences in consumption of recommended amounts of fruits and vegetables, a finding that is different from that of an earlier study, which found lower levels of fruits and vegetables consumption in Hispanics but not in blacks.5
This study provides new information on frequency of home foot examinations across racial/ethnic groups. The proportion of patients with diabetes who performed self foot examinations at least once daily ranged from 66% in Hispanics to 82% in others. In adjusted models, blacks were 1.4-times more likely to do daily self foot examinations compared to whites. Previous studies have focused on annual foot examination by health care providers.17,18 This study provides new information that can assist health care providers in tailoring foot care education across racial/ethnic groups by identifying groups with particularly low levels of self foot examination. For example, while all patients with diabetes should be educated about self foot examination, health care providers may want to emphasize foot care to Hispanic patients.
There are 2 major implications of this study. First, there is a dire need to improve diabetes self-care behaviors in all patients with diabetes regardless of race and ethnicity. Diabetes is a complex and progressive metabolic disease that often requires major lifestyle changes. Evidence from multiple trials have shown that glycemic control is critical to the management of diabetes19,20 and that regular exercise training, appropriate dietary intake, and home blood glucose monitoring are important adjuncts to good glycemic control.13,14,21 The findings of this study suggest that more aggressive strategies to improve self-care skills are needed across all racial/ethnic groups. A good starting point could be more widespread implementation of the American Diabetes Association National Standards for Diabetes Self-Management Education22 in most clinical settings. Second, interventions that are tailored to the diverse needs of diabetic patients from different ethnic groups are needed. For example, based on the findings of prior studies,16,23,24 physical activity interventions may need to be tailored to address barriers to physical activity in blacks with diabetes. Similarly, interventions that address established health literacy, linguistic, and access barriers25–27 in blacks and Hispanics are likely to be more effective than generic interventions. It is also important that future studies examine the effects of recommended self-care behaviors on clinical outcomes across different racial/ethnic groups.
This study has some limitations. First, the brief dietary recall used in the BRFSS may not be as reliable as multiple 24-hour recalls; however, a previous study has shown that daily fruit/vegetable intake measured by the BRFSS telephone survey was similar to intakes estimated by multiple diet records or recalls in diverse ethnic populations.28 Second, this study only assessed leisure-time physical activity and did not measure physical activity from occupation transportation, or housework; hence total activity levels may be underestimated. Third, telephone surveys may yield biased estimates because of the exclusion of households without telephones. However, studies have established the validity of the BRFSS telephone survey.29,30 Finally, expectation bias is a potential limitation. Patients may overreport good habits, and this may vary by race/ethnicity.
In conclusion, this study shows that, among adults with diabetes, few patients engage in multiple self-care behaviors at recommended levels regardless of race/ethnicity and that there are significant racial/ethnic differences in physical activity, dietary, and foot care behaviors.
References
National Institute of Diabetes and Digestive and Kidney Diseases. National Diabetes Statistics fact sheet: general information and national estimates on diabetes in the United States, 2003. Bethesda, MD: U.S. Department of Health and Human Services, National Institute of Health, 2003. Rev. ed. Bethesda, MD: U.S. Department of Health and Human Services, National Institute of Health, 2005.
Saaddine JB, Engelgau MM, Beckles GL, Gregg EW, Thompson TJ, Narayan KM. A diabetes report card for the United States: quality of care in the 1990s. Ann Intern Med. 2002;136(8):565–74.
Norris SL, Engelgau MM, Narayan KM. Effectiveness of self-management training in type 2 diabetes: a systematic review of randomized controlled trials. Diabetes Care. 2001;24(3):561–87.
Harris MI. Frequency of blood glucose monitoring in relation to glycemic control in patients with type 2 diabetes. Diabetes Care. 2001;24:979–82.
Nelson KM, Reiber G, Boyko EJ. Diet and exercise among adults with type 2 diabetes: findings from the third national health and nutrition examination survey (NHANES III). Diabetes Care. 2002;25(10):1722–8 (Oct).
Thackeray R, Merrill RM, Neiger BL. Disparities in diabetes management practice between racial and ethnic groups in the United States. Diabetes Educ. 2004;30(4):665–75.
Centers for Disease Control and Prevention (CDC). Behavioral Risk Factor Surveillance System Survey Data. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, 2003.
Center for Disease Control and Prevention. Behavioral Risk Factor Surveillance System Operational and User’s Guide. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, 2005.
American Diabetes Association. Standards of medical care in diabetes—2006 (position statement). Diabetes Care. 2006;29(1 suppl):S4–S42.
American Association of Clinical Endocrinologists. American Association of Clinical Endocrinologists medical guidelines for management of diabetes mellitus: the AACE system of intensive diabetes self-management—2002 update. Endocr Pract. 2002;8(1 suppl):40–82.
Veterans Affairs/Department of Defense. Diabetes mellitus: clinical practice guidelines [article online]. Available from http://www.oqp.med.va.gov/cpg/DM/DM3_cpg/frameset.htm. Accessed August 24, 2006.
StataCorp: Stata statistical software: release 8.0. College Station, TX. Stata Corporation, 2004.
American Diabetes Association. Physical activity/exercise and diabetes (position statement). Diabetes Care. 2004;27(1 suppl):S58–S62.
American Diabetes Association. Nutrition principles and recommendations in diabetes (position statement). Diabetes Care. 2004;27(1 suppl):S36–S46.
Egede LE, Zheng D. Modifiable cardiovascular risk factors in adults with diabetes: prevalence and missed opportunities for physician counseling. Arch Intern Med. 2002;162(4):427–33.
Egede LE, Poston ME. Racial/ethnic differences in leisure-time physical activity levels among individuals with diabetes. Diabetes Care. 2004;27(10):2493–4.
Martin TL, Selby JV, Zhang D. Physician and patient prevention practices in NIDDM in a large urban managed-care organization. Diabetes Care. 1995;18(8):1124–32.
Brown AF, Gregg EW, Stevens MR, et al. Race, ethnicity, socioeconomic position, and quality of care for adults with diabetes enrolled in managed care: the Translating Research into Action for Diabetes (TRIAD) study. Diabetes Care. 2005;28(12):2864–70.
The Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329:977–86.
The UK Prospective Diabetes Study Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352:837–53.
Benjamin, EM. Self-monitoring of blood glucose: the basics. Clin Diabetes. 2002;20:45–7.
Mensing C, Boucher J, Cypress M, et al. National standards for diabetes self-management education. Diabetes Care. 2006;29(1 suppl):S78–S85.
Crespo CJ, Smit E, Andersen RE, Carter-Pokras O, Ainsworth BE. Race/ethnicity, social class and their relation to physical inactivity during leisure time: results from the Third National Health and Nutrition Examination Survey, 1988–1994. Am J Prev Med. 2000;18(1):46–53.
Eyler AA, Matson-Koffman D, Vest JR, et al. Environmental, policy, and cultural factors related to physical activity in a diverse sample of women: The Women’s Cardiovascular Health Network Project—summary and discussion. Women Health. 2002;36(2):123–34.
Schillinger D, Grumbach K, Piette J, et al. Association of health literacy with diabetes outcomes. JAMA. 2002;288:475–82.
Karter AJ, Ferrara A, Darbinian JA, Ackerson LM, Selby JV. Self-monitoring of blood glucose: language and financial barriers in a managed care population with diabetes. Diabetes Care. 2000;23:477–83.
Nelson KM, Chapko MK, Reiber G, Boyko EJ. The association between health insurance coverage and diabetes care; data from the 2000 Behavioral Risk Factor Surveillance System. Health Serv Res. 2005;40(2):361–72.
Serdula M, Coates R, Byers T, et al. Evaluation of a brief telephone questionnaire to estimate fruit and vegetable consumption in diverse study populations. Epidemiology. 1993;4:455–63.
Shea S, Stein AD, Lantigua R, Basch CE. Reliability of the behavioral risk factor survey in a triethnic population. Am J Epidemiol. 1991; 133:489–500.
Bowlin SJ, Morrill BD, Nafziger AN, Lewis C, Pearson TA. Reliability and changes in validity of self-reported cardiovascular disease risk factors using dual response: the behavioral risk factor survey. J Clin Epidemiol. 1996;49:511–7.
Acknowledgments
Dr. Egede is supported by grant #5K08HS11417 from the Agency for Health Care Research and Quality. Dr. Nwasuruba is supported by R24 MD000536 from the National Center on Minority Health and Health Disparities.
Author information
Authors and Affiliations
Corresponding author
Additional information
Potential Financial Conflicts of Interest:
The authors do not have any conflicts of interest to report.
Rights and permissions
About this article
Cite this article
Nwasuruba, C., Khan, M. & Egede, L.E. Racial/Ethnic Differences in Multiple Self-Care Behaviors in Adults with Diabetes. J GEN INTERN MED 22, 115–120 (2007). https://doi.org/10.1007/s11606-007-0120-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-007-0120-9