
Abstract
Objectives
To investigate the prognosis value of lymphatic vessel invasion (LVI) in pN0 gastric cancer patients with insufficient examined lymph nodes (ELNs).
Methods
Clinicopathologic and prognostic data of pN0 gastric cancer patients with insufficient ELNs who underwent radical surgery in our institution were retrospectively studied.
Results
Firstly, we confirmed that less than 16 but not less than 30 ELNs were insufficient ELNs in the present study. Of the 350 pN0 patients with < 16 ELNs, 64 patients (18.29%) had LVI. The overall survival (OS) of patients with LVI was significantly poorer than those without LVI. Multivariate analysis suggested that LVI was one of the independent factors predicting prognosis of pN0 patients with < 16 ELNs. Further analyses suggested that there were similar prognoses between pN0 patients with < 16 ELNs who had LVI and pN1 patients, and between pN0 patients with < 16 ELNs who had no LVI and pN0 patients with ≥ 16 ELNs, respectively. Therefore, we proposed a novel pN classification, in which LVI-positive pN0 gastric cancer with < 16 ELNs was classified as pN1 disease. Two-step multivariate analysis demonstrated that the novel pN classification was more suitable for prognostic assessment than the original one.
Conclusions
LVI is a powerful and independent prognostic factor for pN0 gastric cancer patients with < 16 ELNs, and node-negative gastric cancer with < 16 ELNs which had LVI should be considered as node-positive disease. LVI is an effective indicator identifying patients stage migration happens to in pN0 patients with < 16 ELNs.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Lymph node (LN) metastasis is the most reliable prognostic indicators for patients with gastric cancer who underwent curative resection.1,2,3 The International Union Against Cancer (UICC) and the American Joint Committee on Cancer (AJCC) tumor, node, metastasis (TNM) staging system defines pN0 disease as gastric cancer without LN metastasis, regardless of the number of total examined LNs (ELNs).4 However, the UICC/AJCC TNM staging system also recommends that at least 16 or 30 LNs should be examined to determine pN0 classification. It has been demonstrated that pN0 patients with insufficient ELNs had significantly worse prognosis than those with sufficient ELNs.5,6,7 This is mainly because examining less LNs may lead to missing LN metastasis, resulting in stage migration (Will Rogers phenomenon).8, 9 That is to say, part of pN0 patients with insufficient ELNs actually have already had LN metastasis.
Unfortunately, a considerable number of the gastric cancer patients who were classified as pN0 classification have insufficient LNs examined, especially in western countries.6, 10 To reduce stage migration caused by insufficient ELNs, ratio of metastatic LNs (N-ratio) and log odds of positive LNs (LODDS) have been recently proposed.11, 12 However, N-ratio has no effect on reducing stage migration in pN0 patients because it defines pN0 classification the same as the TNM staging system. On the contrary, LODDS was demonstrated to be a LN staging system which effectively reduced stage migration caused by insufficient examined lymph nodes in node-negative patients.12 Nevertheless, the complicated calculation procedure of LODDS would limit its clinical application. Therefore, to find a simple and effective indicator that could identify that patients’ stage migration happens in pN0 patients with insufficient ELNs is necessary.
Lymphatic vessels are an essential route for lymph node metastasis, and lymphatic vessel invasion (LVI) is considered as the most powerful and independent predictor of LN metastasis in gastric cancer.13, 14 Recently, LVI was also reported to be one of the independent prognostic factors for node-negative gastric cancer.15 Nevertheless, the prognosis value of LVI in pN0 patients with insufficient ELNs is still unknown.
In light of these considerations, the aim of the present study is to investigate the prognosis value of LVI in pN0 patients with insufficient ELNs, and to explore whether LVI was an effective indicator identifying that patients’ stage migration happens in pN0 patients with insufficient ELNs.
Materials and Methods
Patients and Clinicopathologic Features
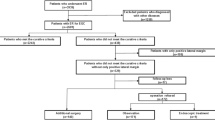
All patients with gastric cancer who underwent surgery at the Department of Surgical Oncology, First Affiliated Hospital of China Medical University, from January 1980 to September 2012 were entered into a prospectively maintained database. In all, there were 768 pN0 patients with < 30 ELNs who had no distant metastasis and underwent radical surgery. A radical surgery was defined as en bloc resection of primary cancer and completed lymphadenectomy (D1 or D2/3 lymphadenectomy) without microscopic or macroscopic residual disease according to the TNM staging system.4 Among them, we excluded patients (1) without pathologic data of the TNM staging system or records of LVI status (nine patients), (2) who died in the postoperative period (five patients), and (3) who were lost during the time of follow-up (eight patients). After these exclusions, a total of 746 pN0 patients with < 30 ELNs were enrolled into this study. Among these 746 patients, there were 350 patients with < 16 ELNs and 396 patients with ELNs between 16 and 30.
Meanwhile, 284 pN0 patients with ≥ 30 ELNs and 536 pN1 patients, who had no distant metastasis and underwent radical surgery during the same study period, were also included as reference groups for prognostic comparisons with pN0 patients with insufficient ELNs.
In the present study, the following clinicopathologic features were obtained: operative period, the range of lymphadenectomy, the range of gastrectomy, age, gender, location of the primary tumor, tumor size, pT classification, pN classification, number of ELNs, histologic type, LVI, and Borrmann type. The pT classification and pN classification were classified according to the eighth UICC/AJCC TNM staging system.4 All patients in the present study did not receive neoadjuvant chemotherapy.
Histopathologic Examination of LVI
The formalin-fixed specimens, containing the carcinoma lesions together with the surrounding gastric wall, were cut into multiple slices, principally parallel to the lesser curature, at an interval of 2 mm. The cut specimens were embedded in paraffin, sectioned and stained with hematoxylin-eosin. LVI was defined as tumor cells present within the lumen of lymphatic vessels. Lymphatic vessels were distinguished from venous vessels on the basis of the features of smooth muscle and elastic fibers and the presence or absence of valvules as defined by Shirouzu et al..16 The sections were independently examined by two pathologists. If there was a disagreement, another pathologist would be invited to review the slides, and a consensus was reached between the three pathologists.
Follow-up
Follow-up of the entire study population was conducted until death or the cutoff date (March 01, 2016) by means of outpatient clinic consultation and/or communication with patients through telephone or letter. Median and mean follow-up periods were 89.50 and 109.81 months (range 2–426 months), respectively.
Statistical Analysis
All statistical analyses were performed with the SPSS 19.0 statistical package (SPSS Inc., Chicago, IL, USA) and R software version 3.2.0 with the rms, Hmisc, and survival package (http://www.r-project.org/). The categorical variables were compared using a two-tailed chi-square test. The continuous data was presented as a mean ± standard deviation, and two-tailed t test (normally distributed) or Mann-Whitney U test (not normally distributed) was used for the statistical comparisons. Overall survival (OS) rates were determined using the Kaplan–Meier estimator. The log-rank test was used to identify differences between the survival curves of different patient groups. All the factors that were significantly associated with overall survival were included in multivariate analysis. Cox’s proportional hazard model (stepwise forwards method) was used as multivariate analysis to identify independent factors predicting patients’ prognosis. For all analyses, P values were two-tailed, and only P values < 0.05 were considered significant.
Results
pN0 Patients with < 16 ELNs Has a Significantly Poorer OS than pN0 Patients with ≥ 16 Examined LN
As the eighth UICC/AJCC TNM staging system provides two numbers to determine insufficient ELNs for gastric cancer (ELNs < 16 and ELNs < 30),4 we first identified which number was more suitable for pN0 classification. As Fig. 1a shows, the OS of pN0 patients with < 16 ELNs was significantly poorer than that of pN0 patients with ELNs between 16 and 30 (P = 0.008) and pN0 patients with ≥ 30 ELNs (P = 0.007), respectively, but the prognosis of pN0 patients with ELNs between 16 and 30 was similar to that of pN0 patients with ≥ 30 ELNs (P = 0.984). Therefore, less than 16 ELNs was defined as insufficient ELNs in the present study.

Comparison of overall survival curves between pN0 patients with < 16 ELNs, pN0 patients with ELNs between 16 and 30, and pN0 patients with ≥ 30 ELNs (a), and between pN0 patients with < 16 ELNs, pN0 patients with ≥ 16 ELNs, and pN1patients (b). ELNs examined lymph nodes, 5-YSR 5-year survival rate
We then confirmed the phenomenon that pN0 patients with insufficient ELNs had a poorer survival than those with sufficient ELNs, which was reported by previous studies.5,6,7 As Fig. 1b shows, the OS of pN0 patients with < 16 ELNs was significantly poorer than that of pN0 patients with ≥ 16 ELNs (P = 0.002), but significantly better than that of pN1 patients (P = 0.000).
LVI Is One of the Independent Factors Predicting a Poor OS in pN0 Patients with < 16 ELNs
Of the 350 pN0 patients with < 16 ELNs, there were 286 men (81.71%) and 64 women (18.29%; ratio 4.47:1), with a mean age of 59.26 ± 11.07 years (median 59.50 years; range 25–80 years). Of the 350 patients included in the present study, 68 patients (19.43%) underwent D1 lymphadenectomy and 282 patients (80.57%) underwent D2/3 lymphadenectomy. Of the 350 patients, 235 patients (67.14%) underwent distal gastrectomy, 74 patients (21.14%) underwent proximal gastrectomy, and 41 patients (11.72%) underwent total gastrectomy. Among these patients, 64 (18.29%) had LVI. Table 1 summarizes the clinicopathologic features of the 64 patients with LVI and the 286 patients without LVI. There were significant differences in pT classification and Borrmann types, but not in age, gender, location of the primary tumor, tumor size, histologic type, number of ELNs, the range of lymphadenectomy, the range of gastrectomy, and operative period.
Concerning prognosis, the OS of pN0 patients with < 16 ELNs who had LVI was significantly poorer than that of those who had no LVI (Fig. 2; P = 0.000). When the OS rates were compared as stratified by pT classification, significant differences could be observed in pT1–3 classification but not in pT4 classification (Table 2).

Overall survival curves of pN0 patients with < 16 examined lymph nodes according to the LVI status. LVI lymphatic vessel invasion, 5-YSR 5-year survival rate
Univariate analysis of prognostic factors for pN0 patients with < 16 ELNs suggested that age, location of the primary tumor, tumor size, pT classification, LVI, and Borrmann type were significantly correlated with patients’ prognosis (Table 3). Upon multivariate analysis, age, location of the primary tumor, LVI, and Borrmann type were independent factors predicting patients’ prognosis (Table 3).
The Prognosis of pN0 Patients with < 16 ELNs Who Had LVI Was Homogeneous with that of pN1 Patients
To explore whether LVI was an effective indicator identifying that patients’ stage migration happens in pN0 patients with < 16 ELNs, we compared the prognosis among pN0 patients with < 16 ELNs who had LVI, pN0 patients with < 16 ELNs who had no LVI, pN0 patients with ≥ 16 ELNs, and pN1 patients. Interestingly, as Fig. 3 shows, the OS of pN0 patients with < 16 ELNs who had LVI is similar to that of pN1 patients (P = 0.794), but significantly poorer than that of pN0 patients with ≥ 16 ELNs (P = 0.000). On the contrary, the OS of pN0 patients with < 16 ELNs who had no LVI was similar to that of pN0 patients with ≥ 16 ELNs (Fig. 3; P = 0.128), but significantly better than that of pN1 patients (Fig. 3; P = 0.000).

Comparison of overall survival curves between pN0 patients with < 16 ELNs who had LVI, pN0 patients with < 16 ELNs who had no LVI, pN0 patients with ≥ 16 ELNs, and pN1 patients. LVI lymphatic vessel invasion, ELNs examined lymph nodes, 5-YSR 5-year survival rate)
Based on the above results, we proposed a novel pN classification, in which LVI-positive pN0 gastric cancer with < 16 ELNs was classified as pN1 disease, whereas LVI-negative pN0 gastric cancer with < 16 ELNs was still classified as pN0 disease. To explore which pN classification was more suitable for prognostic assessment, we performed two-step multivariate analysis for the OS of 1566 patients with pN0-pN1 diseases, which included 350 pN0 patients with < 16 ELNs, 680 pN0 patients with ≥ 16 ELNs, and 536 pN1 patients. In step 1 multivariate analysis, the UICC/AJCC pN classification was one of the independent factors predicting patients’ prognosis (Table 4). When the novel pN classification was also considered in step 2 multivariate analysis, it replaced the UICC/AJCC pN classification as one of the most important prognostic factors (Table 4). The C-index of the novel pN classification (C-index 0.606; 95%CI 0.586–0.626) was also higher than that of the UICC/AJCC pN classification (C-index 0.596; 95%CI 0.576–0.616).
Discussion
Because of the prognostic difference between pN0 patients with insufficient and those with sufficient ELNs, which is reported widely,5,6,7 the UICC/AJCC TNM staging system recommends that at least 16 LNs should be examined to determine pN0 classification in gastric cancer.4 Stage migration is the major reason causing the prognostic difference, meaning that node-positive patients may be underestimated as pN0 classification due to insufficient ELNs.8, 9 In the present study, we confirmed that pN0 patients with < 16 ELNs had a significantly poorer OS than those with ≥ 16 ELNs. However, we also found that the OS of pN0 patients with < 16 ELNs was significantly better than that of pN1 patients, suggesting that stage migration happened to part of but not all of the pN0 patients with < 16 ELNs. Nevertheless, how to identify that patients’ stage migration happens in pN0 patients with < 16 ELNs is still highly unknown until now.
In the present study, we found that pN0 patients with < 16 ELNs who had LVI had a significant poorer survival compared to those who had no LVI. Furthermore, LVI was demonstrated to be one of the independent factors predicting a poor OS in pN0 patients with < 16 ELNs. Most importantly of all, we found that the OS of pN0 patients with < 16 ELNs who had LVI was similar to that of pN1 patients, but significantly poorer than that of pN0 patients with ≥ 16 ELNs, and on the contrary, the OS of pN0 patients with < 16 ELNs who had no LVI was similar to that of pN0 patients with ≥ 16 ELNs, but significantly better than that of pN1 patients. The results suggest that pN0 patients with < 16 ELNs who had LVI and pN1 patients have the same malignant potential, whereas pN0 patients with < 16 ELNs who had no LVI and pN0 patients with ≥ 16 ELNs have the same malignant potential. Based on the above results, we speculated that LVI was an effective indicator identifying that patients’ stage migration happens in pN0 patients with < 16 ELNs.
To confirm our speculation, we proposed a novel pN classification, which incorporated node-negative gastric cancer with < 16 ELNs which had LVI into pN1 classification, whereas still classified node-negative gastric cancer with < 16 ELNs which had no LVI as pN0 classification. Two-step multivariate analysis demonstrated that the novel pN classification was more suitable for prognostic assessment than the original one. In addition, the C-index of the novel pN classification was also higher than that of the UICC/AJCC pN classification. Therefore, we conclude that LVI is an effective indicator identifying that patients’ stage migration happens in pN0 patients with < 16 ELNs, and node-negative gastric cancer with < 16 ELNs which had LVI should be considered as node-positive disease.
LVI has been reported to be associated with LN metastasis in various cancers, including gastric cancer. A study by Morita et al., which aimed to identify histopathological predictors for regional LN metastasis in 210 gastric cancer patients, demonstrated that LVI was the only factor which independently predicted LN metastasis at any depth of tumor invasion.13Kamata et al., in a study which explored the significance of LVI on LN metastasis in gastric cancer, found that LVI was one of the independent predictive factors of LN metastasis.14 Similar results have been observed in breast cancer, non-small cell lung cancer, and colorectal cancer.17,18,19 Therefore, LVI is considered as one of the most powerful and independent predictors of LN metastasis in cancers. Nevertheless, to our knowledge, this is the first study reporting that LVI is an effective indicator identifying that patients’ stage migration happens in node-negative cancer patients with insufficient ELNs.
The present study provides useful and new insights into reducing stage migration in node-negative disease caused by insufficient ELNs, as our findings suggest that the predictor of LN metastasis could be considered as the indicator identifying that patients’ stage migration happens in pN0 patients with insufficient ELNs. In fact, besides LVI, some molecules regulating LN metastasis, such as MMP-1, VEGF-C, and JAM-A, and so on, has also been reported to be the predictors of LN metastasis in cancers.20,21,22 Nevertheless, whether expression of these molecules is the indicator identifying that patients’ stage migration happens in pN0 patients with insufficient ELNs is still uncertain. Therefore, further studies are needed to clarify this issue in the future.
There were some limitations existing in the present study. First, the presence of LVI was only detected by hematoxylin-eosin staining and van Gieson staining. Currently, several studies have reported that immunostaining with antibodies against lymphatic endothelial-specific proteins, such as LYVE-1 and D2–40, could improve sensitivity and specificity of LVI detection.23 Therefore, in theory, the presence of LVI detected by immunostaining may identify that patients’ stage migration happens in pN0 patients with insufficient ELNs more accurately than that detected by hematoxylin-eosin staining and van Gieson staining. We plan to clarify this issue in our future studies. Nevertheless, there is no doubt that hematoxylin-eosin staining and van Gieson staining are more simple and convenient than immunostaining in clinical practice. Second, in our institution, only the presence or absence of LVI was recorded in the “Histopathology Reports,” whereas the pathologic characteristics of LVI such as location (i.e., intratumoral LVI or peritumoral LVI) and extent (i.e., minimal LVI, moderate LVI or marked LVI) were not regularly recorded. Therefore, whether all kinds of LVI can be considered as the indicator identifying patients’ stage migration happens in pN0 patients with < 16 ELNs remains unclear. Third, in the present study, we included patients of a long time period of 32 years, and significant differences of overall survival were observed between different operative periods. This may be accounted for the change of surgery and adjuvant therapy during the long time. Also, adjuvant chemotherapy was not included in this study because of incomplete information. These will limit the strength of our observations. Therefore, further studies are needed to confirm our results.
Conclusion
LVI is a powerful and independent prognostic factor for pN0 gastric cancer patients with < 16 ELNs, and node-negative gastric cancer with < 16 ELNs which had LVI should be considered as node-positive disease. LVI is an effective indicator identifying that patients’ stage migration happens in pN0 gastric cancer patients with < 16 ELNs.
References
Siewert JR, Böttcher K, Stein HJ, Roder JD. Relevant prognostic factors in gastric cancer: ten-year results of the German Gastric Cancer Study. Ann Surg 1998;228: 449–61.
Hohenberger P, Gretschel S. Gastric cancer. Lancet 2003;362: 305–15.
Huang JY, Xu YY, Li M, Sun Z, Zhu Z, Song YX, Miao ZF, Wu JH, Xu HM. The prognostic impact of occult lymph node metastasis in node-negative gastric cancer: a systematic review and meta-analysis. Ann Surg Oncol 2013;20: 3927–34.
Amin MB, Edge SB, Greene FL, et al. AJCC cancer staging manual. 8th ed. New York: Springer, 2017.
Son T, Hyung WJ, Lee JH, Kim YM, Kim HI, An JY, Cheong JH, Noh SH. Clinical implication of an insufficient number of examined lymph nodes after curative resection for gastric cancer. Cancer 2012;118: 4687–93.
Smith DD, Schwarz RR, Schwarz RE. Impact of total lymph node count on staging and survival after gastrectomy for gastric cancer: data from a large US-population database. J Clin Oncol 2005;23: 7114–24.
Li B, Li Y, Wang W, Qiu H, Seeruttun SR, Fang C, Chen Y, Liang Y, Li W, Chen Y, Sun X, Guan Y, Zhan Y, Zhou Z. Incorporation of N0 Stage with insufficient numbers of lymph nodes into N1 stage in the seventh edition of the TNM classification improves prediction of prognosis in gastric cancer: results of a single-institution study of 1258 Chinese patients. Ann Surg Oncol 2016;23(1):142–8.
Lee HK, Yang HK, Kim WH, Lee KU, Choe KJ, Kim JP. Influence of the number of lymph nodes examined on staging of gastric cancer. Br J Surg 2001;88: 1408–12.
Feinstein AR, Sosin DM, Wells CK. The Will Rogers phenomenon. Stage migration and new diagnostic techniques as a source of misleading statistics for survival in cancer. N Engl J Med 1985;312: 1604–8.
Estes NC, MacDonald JS, Touijer K, Benedetti J, Jacobson J. Inadequate documentation and resection for gastric cancer in the United States: a preliminary report. Am Surg 1998;64: 680–5.
Sun Z, Zhu GL, Lu C, Guo PT, Huang BJ, Li K, Xu Y, Li DM, Wang ZN, Xu HM. The impact of N-ratio in minimizing stage migration phenomenon in gastric cancer patients with insufficient number or level of lymph node retrieved: results from a Chinese mono-institutional study in 2159 patients. Ann Oncol 2009;20: 897–905.
Sun Z, Xu Y, Li de M, Wang ZN, Zhu GL, Huang BJ, Li K, Xu HM. Log odds of positive lymph nodes: a novel prognostic indicator superior to the number-based and the ratio-based N category for gastric cancer patients with R0 resection. Cancer 2010;116: 2571–80.
Morita H, Ishikawa Y, Akishima-Fukasawa Y, Ito K, Akasaka Y, Nishimura C, Igarashi Y, Miki K, Ishii T. Histopathological predictor for regional lymph node metastasis in gastric cancer. Virchows Arch 2009;454: 143–51.
Kamata I, Ishikawa Y, Akishima-Fukasawa Y, Ito K, Akasaka Y, Uzuki M, Fujimoto A, Morita H, Tamai S, Maehara T, Ogata K, Shimokawa R, Igarashi Y, Miki K, Ishii T. Significance of lymphatic invasion and cancer invasion-related proteins on lymph node metastasis in gastric cancer. J Gastroenterol Hepatol 2009;24: 1527–33.
Liu E, Zhong M, Xu F, Liu W, Huang J, Zeng S, Lu J, Li B, Li J, Jiang H. Impact of lymphatic vessel invasion on survival in curative resected gastric cancer. J Gastrointest Surg 2011;15: 1526–31.
Shirouzu K, Isomoto H, Morodomi T, Kakegawa T. Carcinomatous lymphatic permeation. Prognostic significance in patients with rectal carcinoma—a long term prospective study. Cancer 1995;75: 4–10.
Viale G, Zurrida S, Maiorano E, Mazzarol G, Pruneri G, Paganelli G, Maisonneuve P, Veronesi U. Predicting the status of axillary sentinel lymph nodes in 4351 patients with invasive breast carcinoma treated in a single institution. Cancer 2005;103: 492–500.
Kang DY, Lee S. Lymphatic vessel invasion and lymph node metastasis in patients with clinical stage I non-small cell lung cancer. Thorac Cardiovasc Surg 2014;62: 521–4.
Lin M, Ma SP, Lin HZ, Ji P, Xie D, Yu JX. Intratumoral as well as peritumoral lymphatic vessel invasion correlates with lymph node metastasis and unfavourable outcome in colorectal cancer. Clin Exp Metastasis 2010;27: 123–32.
Huang JY, Xu YY, Sun Z, Wang ZN, Zhu Z, Song YX, Luo Y, Zhang X, Xu HM. Low junctional adhesion molecule A expression correlates with poor prognosis in gastric cancer. J Surg Res 2014;192: 494–502.
Li Y, Cai G, Yuan S, Jun Y, Li N, Wang L, Chen F, Ling R, Yun J. The overexpression membrane type 1 matrix metalloproteinase is associated with the progression and prognosis in breast cancer. Am J Transl Res 2015;7: 120–27.
Achen MG, Stacker SA. Molecular control of lymphatic metastasis. Ann N Y Acad Sci 2008;1131: 225–34.
Gujam FJ, Going JJ, Mohammed ZM, Orange C, Edwards J, McMillan DC. Immunohistochemical detection improves the prognostic value of lymphatic and blood vessel invasion in primary ductal breast cancer. BMC Cancer 2014; 14:676.
Funding
This work was supported by the National Science Foundation of China (No. 81372550, No. 81602522) and Key Laboratory Programme of Liaoning Province (LZ2015080).
Author information
Authors and Affiliations
Contributions
Hui-mian Xu, Ying-ying Xu, and Jin-yu Huang were involved in study concept and design and writing the article; Jin-yu Huang, Ya-nan Xing, Xin Wang, and Zhi Zhu were involved in analysis and interpretation of data; Zhen-ning Wang, Wen-bin Hou, and Song-cheng Yin were involved in data collection.
Corresponding author
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Huang, Jy., Xing, Yn., Wang, X. et al. The Prognosis Value of Lymphatic Vessel Invasion in pN0 Gastric Cancer Patients with Insufficient Examined Lymph Nodes. J Gastrointest Surg 24, 299–306 (2020). https://doi.org/10.1007/s11605-018-04101-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-018-04101-z