
Abstract
Objectives
The objective of this study was to evaluate the feasibility and efficacy of ERAS pathways in patients undergoing emergency simple closure of perforated duodenal ulcer (PDU).
Methods
This single-center, prospective, open-labeled, superiority, RCT was carried out from August 2014 to July 2016. Patients of PDU undergoing open simple closure were randomized preoperatively in 1:1 ratio into standard care and adapted ERAS group. Patients with refractory shock, ASA class ≥3, and perforation size ≥1 cm were excluded. Primary outcome was the length of hospitalization (LOH). Secondary outcomes were functional recovery parameters and morbidity.
Results
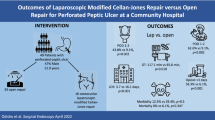
Forty-nine and 50 patients were included in standard care and ERAS group, respectively. Patients in ERAS group had a significantly early functional recovery (days) for the time to first flatus (1.47 ± 0.18; p < 0.001), first stool (2.25 ± 0.20; p < 0.001), first fluid diet (2.72 ± 0.38; p < 0.001), and solid diet (3.70 ± 0.44; p < 0.001). LOH in ERAS group was significantly shorter (mean difference of 4.41 ± 0.64 days; p < 0.001). There was a significant reduction in postoperative morbidity such as superficial SSI (RR 0.35, p = 0.02), postoperative nausea and vomiting (RR 0.28, p < 0.0001), and pulmonary complications (RR 0.24, p = 0.04) in the ERAS vs. standard care group with similar leak rates (1/50 vs.2/49).
Conclusion
ERAS pathways are safe and feasible in select patients undergoing emergency simple closure of PDU.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The advancements in the field of surgery and anesthesia have led to revolutionary revision in the perioperative care referred to as the enhanced recovery after surgery (ERAS) or fast-track protocols. ERAS protocols, pioneered by Henrik Kehlet in the late 1990s, is a streamlined multimodal approach which utilizes various evidence-based modifications of the perioperative care elements with the aim of attenuating the physiological and psychological stress, thus accelerating patients’ recovery [1]. This multifaceted approach aims at a “painless and safe” surgery for the patient.
ERAS protocols have now become the standard of care in many procedures across specialties demonstrating a shorter hospital stay and reduced postoperative morbidity and mortality [2,3,4,5,6,7,8]. Meta-analyses have demonstrated a reduction of 2–4 days in the length of hospitalization (LOH), earlier mobilization, nutrition, and a significant reduction in complication rates following elective upper and lower gastrointestinal surgery [9,10,11,12]. However, despite its success in the elective setting, the perioperative care in the emergency setting still continues to utilize the traditional principles [2]. Recent evidence has found many of these traditional principles to be unnecessary and rather harmful [1]. The higher morbidity and mortality rate following emergency procedures when compared with similar elective procedures underlines the dire need for revising the perioperative care practices in the emergent situations by using a multimodal pathway [13]. Reports of use of ERAS guidelines in emergency situations are sparse, owing to the challenges in implementing all the care elements. ERAS programs have been utilized in various elective situations in a modified form, and hence, its role in emergency situations albeit in an adapted form may be noteworthy [14]. Although challenging, there are reports suggesting the “appropriateness” of the care elements in an emergency setting [15].
There are few reports of its use in emergency situations. A recent randomized controlled trial on 47 patients who underwent laparoscopic Graham patch repair for perforated peptic ulcer demonstrated a reduction of 2 days in the length of hospital stay with no significant difference in the rate of complications with the use of ERAS pathways [16]. Similarly, faster functional recovery of bowel functions, reduced complications, and a shorter hospital stay were reported in patients of urgent colectomy in a few case control studies [17, 18]. However, large prospective randomized studies on the role of ERAS in emergency are sparse.
Perforated duodenal ulcer (PDU) is one of the most common surgical emergencies in this region and is associated with a substantial mortality rate of 6–30% [19]. The management of this condition is fairly standardized and is carried out by open or laparoscopic procedures. Application of the evidence-based ERAS protocols has the potential for improvising the outcomes in the perioperative period in open and laparoscopic surgery. Hence, this study was carried out to evaluate the safety, efficacy, and feasibility of an adapted ERAS protocol in patients who underwent simple closure of perforated duodenal ulcer.
Methodology
Study Design
This study was a single-center, prospective, open-labeled, parallel arm, superiority, randomized controlled trial carried out in the Department of Surgery of a tertiary care hospital of South India from August 2014 to July 2016. The study was approved by the Institute Ethics Committee (IEC). Written informed consent was taken from all the participants and patients were given full freedom to withdraw at any point during the study. The study was registered at www.ctri.gov.in (CTRI no: CTRI/2015/02/00554).
Patient Enrollment
All consecutive patients, of age 18 years and above, who were presented to the emergency surgical team and were diagnosed with perforated duodenal ulcer by clinical examination and supported by adjunctive investigations, were recruited and assessed for eligibility. The following patients were excluded from the study: age < 18 years, ASA (American Society of Anesthesiologists) class 3 or 4, coexistent psychiatric or neurological illness, patients with refractory septic shock at presentation, pregnant patients, and patients with history of chronic steroid use. Intraoperatively, after randomization, patients were excluded based on the following criteria: perforated duodenal ulcer ≥10 mm, spontaneously sealed off perforations that did not require any intervention, multiple perforated ulcers, coexistent bleeding and perforated ulcer, and patients who had concomitant definitive surgery or additional procedures done such as truncal vagotomy with drainage procedure.
Randomization
Patients were randomly assigned in 1:1 ratio to receive either standard perioperative care or adapted ERAS pathway group. Block randomization was done using computer program with randomly selected block sizes of 4 and 6. Allocation concealment was performed using a serially numbered opaque sealed envelope (SNOSE) technique. Sealed envelopes were prepared by a person independent of the investigators. The envelopes were opened by the nurse and group allocation was done at the time of decision to proceed with surgery.
Adapted ERAS Pathways vs. Standard Care
Preoperative Care
Preoperative preparation was identical in both the groups in the placement of nasogastric (NG) tube at admission and administration of crystalloids for fluid replacement. They also received empirical intravenous (IV) antibiotic therapy with ceftriaxone (1 g IV Q12h) and metronidazole (500 mg IV Q8h) and IV acid reducing therapy with pantoprazole (40 mg IV Q12h). In the ERAS group, lumbar epidural catheter was secured in the L3–L4 interspace in patients who did not have any contraindications such as coagulopathy and severe sepsis, and age > 60 years [19]. The differences between the two groups in the care pathways are shown in Table 1.
Intraoperative Care
All patients underwent simple closure of the duodenal ulcer perforation by Grahams patch technique under general anesthesia with the standard anesthetic protocols [20]. The differences in the anesthetic protocols between the two groups are shown in Table 1. All patients had the intraoperative central venous pressure-guided fluid management. The surgical procedure was carried out by a surgical resident under the supervision of the registrar. A 28-F Malecot drain was placed in the sub-hepatic space before closure of the abdomen. The size of perforation, nature, and severity of the contamination were noted. The patients’ Boey’s score and Mannheim Peritonitis Index were calculated and recorded [21, 22].
Postoperative Care
Adapted ERAS protocol was based on principles of ERAS care elements such as non-opioid multimodal analgesia, early nutrition, and early mobilization of the patients. An adapted criterion was followed for the use of drains and tubes as the safety of an ERAS protocol in emergency has not been well established. Individual elements of the adapted protocol and how it differs from the conventional pathway have been described in Table 1. In both the groups, the oral intake was stopped immediately in patients who showed intolerance to diet in any form which was defined as any one of the following criteria: pain of moderate or severe intensity (Likert score > 3/5) after resumption of oral feeds, more than two episodes of vomiting of >100 ml over 24 h, one episode of diarrhea, or abdominal distension [23, 24]. In patients who developed intolerance to oral feeds, feeding was re-initiated after the symptoms had completely subsided and active bowel sounds had reappeared. All patients were discharged when they had tolerated solid diet for at least 24 h and had passed stool and in the absence of other factors such as fever, wound infection, anastomotic leakage, etc. All patients were discharged with oral acetaminophen (500 mg on demand) and were advised to continue oral omeprazole (20 mg Q12H) for 3 months. All patients were reviewed on postoperative day 10 and 30 for the presence of any complications or need for readmissions.
Outcome Measures
The primary endpoint was the length of hospital (LOH) stay between the two groups. The secondary end points included various functional recovery parameters such as time for removal of nasogastric tube, drains, and catheter; duration of ileus; time for first passage of flatus and stool; time elapsed until resumption of oral feeding; and time to first walk. The other secondary endpoints included morbidity parameters such as the need for extra analgesics, need for reinsertion of nasogastric tube, incidence of postoperative nausea and vomiting (PONV) graded using the Apfel score, superficial or organ type SSI (surgical site infection) with and without leak from omentopexy site, pulmonary complications, urinary tract infections, and readmissions, reoperation, and mortality rates [25]. Primary outcome and major secondary outcomes were also compared within patients in ERAS group with and without epidural catheter to study the influence of epidural analgesia in an ERAS setting.
Data Collection and Statistical Analysis
Data was collected on a specified proforma prepared by the investigators. Various demographic variables, telephone numbers (to avoid loss to follow up), clinicopathological variables such as duration of the symptoms at presentation, ASA class, pulse rate, systolic blood pressure, hemoglobin, albumin, lactate, pH, and intraoperative variables such as size of perforation, details of the operative procedure, nature and severity of contamination, Boey’s score, and Mannheim Peritonitis Index (MPI) were recorded [21, 22]. Outcome variables were also recorded by the investigators.
LOH, the primary outcome alone was used for power analysis. A sample size of 45 in each group was calculated based on the requirement to detect a reduction in LOH of 2 days, the level of significance being 5% and power of study set to 90% using Open Epi software (version 3.03) [16]. Expecting a 10% drop out rate including post randomization exclusion, sample size was rounded off to 50 in each group (total = 100).
Statistical analysis was done using SPSS 19.0 software for windows. Continuous variables such as age, duration of surgery, size of perforation, time for removal of NG tube/drain, time for resolution of ileus, and resumption of orals and length of hospitalization were expressed as means with standard deviation. Categorical variables such as gender, need for reinsertion of NG tube/extra analgesia, and complications were expressed as proportions. Continuous variables were analyzed using the independent Student t test or Mann–Whitney U test. Categorical variables were analyzed using chi-square test or Fisher’s exact test. A p value of less than 0.05 was considered as statistically significant.
Results
Patients
From August 2014 through July 2016, of the 135 patients of PDU who were assessed for eligibility, 102 patients were randomized, 52 to standard perioperative care group, and 50 to adapted ERAS group. In the standard care group, intraoperatively three patients who were found to have ileal perforation, DU perforation ≥1 cm, and spontaneously sealed off perforation were excluded after randomization based on the exclusion criteria. A total of 99 patients were included for analysis and there was no loss to follow up during the study period (Fig. 1). The two groups were comparable in terms of all demographic and clinicopathological characteristics (Table 2).

CONSORT diagram for the study
Primary Outcome
The length of hospital stay was reduced by 4.41 ± 0.64 days in adapted ERAS group when compared with standard care group (p < 0.0001, CI 3.14 to 5.68). Similar results were obtained even after excluding the two patients in the standard care group who underwent reoperation in the same admission (mean difference 3.85 ± 0.45, p < 0.0001, CI 2.967 to 4.74). Figure 2 shows the distribution of LOH between the two groups. Seventy-three percent of patients in the standard care group had hospital stay of more than 7 days postoperatively, whereas 8% of patients in adapted ERAS group stayed for more than 7 days.

Comparison of LOH
Secondary Outcomes
Functional Recovery Parameters
The patients in the adapted ERAS group had a significantly early resolution of ileus and had the nasogastric tube removed earlier when compared to standard care group (Table 3). The difference in the mean volume of the gastric aspirate at the time of removal of NG tube between the two groups was significantly higher in the ERAS group (55.61 ± 3.074 ml vs. 180.9 ± 8.064 ml, p < 0.001, CI 108 to 142.5).
Patients in ERAS group had a significantly early return of bowel functions in terms of appearance of first bowel sounds, first flatus, and first stools, and an earlier resumption of oral feeds (Table 3). Five patients developed postoperative ileus, two in the adapted ERAS group, and three in standard care group, and were managed conservatively with nasogastric tube reinsertion, bowel rest, and hydration. The difference in need for nasogastric tube reinsertion between the two groups however was not significant (2/50 vs. 3/49; p = 0.63).
The patients in the adapted ERAS groups had the drains and the urinary catheter removed significantly early when compared to the standard care group (Table 3). Ninety-eight percent of patients in the standard care group had the abdominal drain in situ for more than 3 days while only 2% in the adapted ERAS group had it for more than 3 days. The difference in the mean volume of drainage at the time of removal of drain (79.49 ± 2.497 ml in ERAS group vs. 32.63 ± 1.239 in standard care group, p < 0.001, CI 41.46 to 52.26) was also significant. The mean time for mobilization was also significantly shorter in the ERAS group (Table 3).
Morbidity Parameters
There was significant reduction in the various postoperative morbidity parameters in the ERAS group when compared with the standard care group (Table 4). The need for extra analgesia was significantly reduced in the ERAS group when compared to standard care group (OR = 0.26, p = 0.007, CI 0.09–0.69). Majority of the patients in both the groups (96% and 88%) belonged to Clavien Dindo Class I [26]. Three patients in the standard care group were assigned Clavien Dindo Class III; however, the difference in distribution of the patients into various classes were not significant (p = 0.30). There was a significant reduction in postoperative morbidity such as superficial surgical site infections (RR 0.35, p = 0.02), incidence of PONV (RR 0.28, p < 0.0001), and pulmonary complications (RR 0.24, p = 0.04) in the ERAS group. Two patients in standard care group and one patient in adapted ERAS group had developed leak from the omentopexy site; the difference was however not significant (p = 0.54). The two patients in the standard care group were reoperated and the patient in the adapted ERAS group was managed conservatively. Two patients in the standard care group and none in the ERAS group developed acute kidney injury in the postoperative period. There was no 30-day morbidity or mortality or readmissions reported in the study in both the arms.
Subgroup analysis within the ERAS group between patients with and without epidural analgesia demonstrated a significant reduction in duration of ileus and hospital stay in patients with epidural catheter (Table 5). However, this subgroup analysis was limited by a lesser number of patients.
Discussion
In this prospective trial, there was a significant reduction in hospital stay with no worsening of the postoperative complication rates in patients managed with ERAS protocols when compared to the standard care. The patients in the ERAS group had a significantly earlier functional recovery in terms of bowel functions, earlier resumption of oral feeds, and earlier mobilization. Hence, it demonstrates the safety, efficacy, and feasibility of an adapted ERAS protocol in emergent situations where an “all-in” approach is often not plausible.
Though there are few reports of successful use of modified ERAS protocols in emergency, these studies were, however, limited by inclusion of few care elements and fewer patients [16,17,18]. Gonenc et al. were the first to evaluate the feasibility of ERAS protocols in a prospective RCT on 47 patients who underwent laparoscopic Grahams patch repair [16]. However, emphasis was given solely on postoperative ERAS care elements such as non-opioid analgesics, omission of nasogastric decompression, and resumption of liquid feeds by 24 h postoperatively. Few observational studies on a limited number of patients of urgent colectomy also demonstrated the success of an adapted ERAS pathway [17, 18]. In the present study, attempt was made to use the maximum possible care elements of preoperative, intraoperative, and postoperative components in patients managed for PDU.
In emergency setting, the limited literature available demonstrates a decreased LOH by utilization of ERAS protocols. In the two reported studies on patients of urgent colectomy, a reduction in LOH of 2–3 days was reported [17, 18]. A reduction of LOH by 3 days was reported in patients who underwent laparoscopic Graham patch repair managed by ERAS protocols [16]. In the present study, the hospital stay was reduced by 4 days in the ERAS group in patients managed by open Grahams patch repair. A significant reduction of LOH was found even after excluding the two patients of standard perioperative care group who had reoperation in the same admission. The shortened hospital stay may be attributed to the implementation of more number of ERAS care elements, especially in the preoperative and intraoperative period. Attempt to include these elements in the ERAS pathway is important as the intraoperative management plays a key role in deciding the outcome in the postoperative period [27]. Failure of adherence or implementation of intraoperative elements might lead to poor outcomes even though a strict protocol is followed in the postoperative period.
ERAS protocols for major elective upper gastrointestinal surgery support safe omission of routine nasogastric decompression [28,29,30,31,32]. However, similar reports in an emergency situation are lacking. Lohsiriwat in his study on patients of urgent colectomy supported early removal within 24–48 h of surgery if the drainage was less than 400 ml over a period of 24 h [18]. Gonenc et al. in their study removed the nasogastric tube immediately after the patients’ recovery from anesthesia [16]. In the present study, NG tube was withdrawn if drainage was ≤300 ml over a period of 24 h. There are reports of prolonged ileus, delayed resumption of orals, and increased pulmonary complications with the use of nasogastric decompression [31]. In the present study, a significantly shorter duration of ileus and decreased incidence of pulmonary complications in the adapted ERAS group which had a truncated period (mean of 1.2 days) of NG decompression was found when compared to the standard care. Gonenc et al. reported a mean of 1.5 days for resumption of orals in the ERAS group [16]. In the present study, liquid and solid feeds were resumed at an average of 1.5 and 2.6 postoperative days, respectively, in patients who had open Grahams patch repair combined with ERAS care elements. Likewise, an average of 3.4 days was reported in patients who had urgent colectomy managed with ERAS protocol [17]. In the present study, limited use of drains was preferred as the evidence for omission of drains in emergent situations is lacking. However, majority of the patients in the ERAS group had the drains removed on the first postoperative day. Moreover, with an adapted protocol, it was possible to attain shorter time to first flatus, first feeds, and first walk, thus accelerating patients’ recovery as in the previous reports. Hence, the truncated use of NG decompression and drains in the present study did not interfere with the successful implementation of ERAS protocol.
Wisely et al. in their study had reported a reduction of 20% in the number of patients of emergency laparotomy requiring catheter beyond 2 days owing to the “diffusion” of ERAS practices from elective procedures [33]. In the present study, majority of the patients of the adapted ERAS group had the urinary catheter removed within 24 h and none had the catheter for more than 2 days. The effect of early removal of catheter was also reflected in a significant reduction in incidence of UTI in ERAS group.
Adequate pain relief is the keystone for success of any ERAS protocol. Fast-track pathways utilize balanced or multimodal analgesia by combining various analgesics with regional blockade technique [2, 34, 35]. However, the use of epidural analgesia in the setting of sepsis is controversial. In the present study, analgesia was dealt as a continuum of various elements in the perioperative period. Relieving patient anxiety by preoperative counseling is of utmost importance especially in an emergent situation. Intraoperatively, short acting opioids with lesser carry over effect were utilized. Regional blockade in the form of a thoracic epidural catheter is an established component of ERAS protocols as it is associated with shortened ileus owing to the opioid sparing effect [36]. The authors have however used lumbar epidural catheter in patients without contraindications for the same owing to the ease of the technique and the lesser expertise needed. Postoperative analgesia was with epidural infusion (when feasible) or by utilizing NSAIDs. Gonenc et al. in their study resorted to NSAIDs for management of postoperative pain with opioids for breakthrough pain [16]. The need for extra analgesia was however not significant in the patients managed with ERAS protocols. This may be attributed to the limited sample size. However, in the present study, the need for extra analgesia was significantly higher in the standard care group when compared with the adapted ERAS group. The subgroup analysis within the ERAS group, surprisingly, demonstrated the role of epidural analgesia, in hastening bowel functions and shortening the hospital stay in the setting of ERAS in contrast to the reports refuting the same [37]. These results may be attributed to the limited number of patients who had epidural catheters. None of the patients had any complications such as hypotension or urinary retention following the use of regional blockade. The present study thus demonstrates the safe and successful implementation of adapted analgesic care elements in the emergency setting.
Wisely et al. in their study comparing all emergency laparotomies in pre- and post-ERAS period reported a significant reduction in the complications in the post-ERAS period suggesting its safe role in emergency [33]. Lohsiriwat reported a non-significant reduction in the overall complication rates in patients of urgent colectomy managed with ERAS protocol when compared with conventional care [18]. Gonenc et al. did not report any significant difference in the postoperative complications, readmission, or reoperation rates owing to the limited sample size [16]. In the present study, there was a significant reduction in the rates of superficial SSI, pulmonary complications, UTI, and incidence of PONV in the ERAS group. The rates of omentopexy site leak was however similar in both the groups. There was no readmission in the present study. Patients who developed minor complications before discharge continued to stay in the hospital; however, none of the patients who were discharged early in the adapted ERAS group had readmissions within 30 days of discharge. Two patients were reoperated in the standard care group and none in the ERAS group. The significance in difference however could not be established due to low incidence.
Patients with perforation of size more than 10 mm have been excluded in the present study as these patients tend to require adjunctive procedures such as feeding jejunostomy, truncal vagotomy and gastrojejunostomy, and the homogeneity of the groups is likely to be disturbed. Moreover, large perforations are known to be associated with an increased complication rates in postoperative period. Similar exclusion criteria were followed in the previous RCT on use of ERAS in perforated peptic ulcer by Gonenc et al. [16]. Hence, the authors chose to exclude large perforations as the evidence for use of ERAS in emergency is limited and safety has not been established in the previous studies.
The present study is not without limitations of its own. The exclusion of high-risk patients such as patients of ASA class 3 and 4 and those with irreversible shock may have contributed to the favorable outcomes [16]. The implementation of care elements such as a laparoscopic approach and dynamic goal directed fluid therapy was not plausible due to logistic reasons. The translation of an early functional recovery into cost savings could not be assessed as the study was carried out in a non-paying facility.
In conclusion, ERAS pathways, in a modified form, are feasible and safe for application in select patients undergoing simple closure of perforated duodenal ulcer without an increase in the rate of complications. Further studies will be needed for formulating precise protocols for its use in other emergency settings.
References
Kehlet H, Wilmore DW. Evidence based surgical care and the evolution of fast-track surgery. Ann Surg. 2008; 248: 189–98.
Sánchez-Jiménez R, Álvarez AB, López JT, Jiménez AS, Conde FG, Sáez JAC. ERAS (Enhanced Recovery after Surgery) in Colorectal Surgery. In: Khan JS (Ed.). Colorectal Cancer - Surgery, Diagnostics and Treatment. First Ed. Rijeka:In Tech; 2014; 487–503.
Nelson G, Altman AD, Nick A, Meyer LA, Ramirez PT, Achtari C et al. Guidelines for pre- and intra-operative care in gynecologic/oncology surgery: Enhanced Recovery After Surgery (ERAS®) Society recommendations. Gynecol Oncol. 2016; 140:313–22.
White JE, Clemmey RH, Marval P. Enhanced recovery after surgery (ERAS): an orthopaedic perspective. J Perioper Pract 2013; 23 :228–32.·
Cerantola Y, Valerio M, Persson B, Jichlinski P, Ljungqvist O, Hubner M et al. Guidelines for perioperative care after radical cystectomy for bladder cancer: Enhanced Recovery After Surgery (ERAS(®)) society recommendations. Clin Nutr. 2013; 32:879–87.
Gotlib Conn L, Rotstein OD, Greco E, Tricco AC, Perrier L, Soobiah C et al. Enhanced recovery after vascular surgery: protocol for a systematic review. Syst Rev. 2012;1:52.
Alarcon JP, Cuesta JCP. Experience with Lung Resection in a Fast-Track Surgery Program. Arch Broncopneumol. 2013; 49:89–93.
Batdorf NJ, Lemaine V, Lovely JK, Ballman KV, Goede WJ, Martinez-Jorge J et al. Enhanced recovery after surgery in microvascular breast reconstruction. J Plast Reconstr Aesthet Surg. 2015; 68:395–402.
Greco M, Capretti G, Beretta L, Gemma M, Pecorelli N, Braga M. Enhanced recovery program in colorectal surgery: a meta-analysis of randomized controlled trials. World J Surg. 2014; 38:1531–41.
Dorcaratto D, Grande L, Pera M. Enhanced Recovery in Gastrointestinal Surgery: Upper Gastrointestinal Surgery. Dig Surg. 2013; 30:70–8.
Varadhan KK, Neal KR, Dejong CH, Fearon KC, Ljungqvist O, Lobo DN. The Enhanced Recovery after Surgery (ERAS) pathway for patients undergoing major elective open colorectal surgery: a meta-analysis of randomized controlled trials. Clin Nutr. 2010; 29:434–40.
Gouvas N, Tan E, Windsor A, Xynos E, Tekkis PP. Fast-track vs standard care in colorectal surgery: a meta-analysis update. Int J Colorectal Dis. 2009; 24:1119–31.
Quiney N, Aggarwal G, Scott M, Dickinson M. Survival After Emergency General Surgery: What can We Learn from Enhanced Recovery Programmes. World J Surg. 2016; 40:1283–7.
Lyon A, Payne CJ, Mac Kay GJ. Enhanced recovery programme in colorectal surgery: Does one size fit all. World J Gastroenterol. 2012; 18: 5661–3.
Khan S, Gatt M, Horgan A, Anderson I, MacFie J. Guidelines for implementation of enhanced recovery protocols. Issues in Professional Practice. 2009.
Gonenc M, Dural AC, Celik F, Akarsu C, Kocatas A, Kalayci MA et al. Enhanced postoperative recovery pathways in emergency surgery: a randomized controlled clinical trial. Am J Surg. 2014; 207:807–14.
Roulin D, Blanc C, Muradbegovic M, Hahnloser D, Demartines N, Hübner M. Enhanced recovery pathway for urgent colectomy. World J Surg. 2014; 38:2153–9.
Lohsiriwat V. Enhanced recovery after surgery vs. conventional care in emergency colorectal surgery. World J Gastroenterol.2014; 20:13950–5.
Low J, Johnston N, Morris C. Epidural analgesia: first do no harm. Anaesthesia. 2008; 63:1–3.
Graham R. The treatment of perforated duodenal ulcers. Surg Gynec Obstet. 1937; 64:235–38
Boey J, Choi SK, Poon A, Alagaratnam TT. Risk stratification in perforated duodenal ulcers. A prospective validation of predictive factors. Ann Surg. 1987; 205:22–6.
Ohmann C, Hau T. Prognostic indices in peritonitis. Hepatogastroenterology. 1997; 44:937–46.
Pragatheeswarane M, Muthukumarassamy R, Kadambari D, Kate V. Early oral feeding vs. traditional feeding in patients undergoing elective open bowel surgery-a randomized controlled trial. J Gastrointest Surg. 2014; 18:1017–23.
Likert R. A technique for the measurement of attitudes. Arch Psychol. 1932; 22:55.
Apfel CC, Kranke P, Eberhart LH, Roos A, Roewer N. Comparison of predictive models for postoperative nausea and vomiting. Br J Anaesth. 2002; 88:234–40.
Clavien PA, Barkun J, De Oliveira ML, Vauthey JN, Dindo D, Schulick RD et al. The Clavien-Dindo classification of surgical complications: five year experience. Ann Surg. 2009; 250:187–9.
Ljungqvist O, Scott M, Fearon KC. Enhanced Recovery After Surgery: A Review. JAMA Surg. 2017. doi: 10.1001/jamasurg.2016.4952.
Nelson R, Edwards S, Tse B. Prophylactic nasogastric decompression after abdominal surgery. Cochrane Database Syst Rev. 2007. doi:10.1002/14651858.CD004929.pub2.
Gustafsson UO, Scott MJ, Schwenk W, Demartines N, Roulin D, Francis N et al. Guidelines for perioperative care in elective colonic surgery: Enhanced Recovery After Surgery (ERAS ®) Society recommendations. World J Surg. 2013; 37:259–84.
Mortensen K, Nilsson M, Slim K, Schäfer M, Mariette C, Braga M et al. Consensus guidelines for enhanced recovery after gastrectomy: Enhanced Recovery After Surgery (ERAS®) Society recommendations. Br J Surg. 2014; 101:1209–29.
Cheatham ML, Chapman WC, Key SP, Sawyers JL. A meta-analysis of selective versus routine nasogastric decompression after elective laparotomy. Ann Surg.1995; 221:469–76.
Rao W, Zhang X, Zhang J, Yan R, Hu Z, Wang Q. The role of nasogastric tube in decompression after elective colon and rectum surgery: a meta-analysis. Int J Colorect Dis 2011; 26: 423–9.
Wisely JC, Barclay KL. Effects of an enhanced Recovery after surgery programme on emergency surgical patients. ANZ J Surg. 2016. DOI:10.1111/ans.13465.
Kehlet H, Wilmore DW. Multimodal strategies to improve surgical outcome. Am J Surg. 2002; 183:630–41
Miller TE, Gan TJ, Thacker JKM. Enhanced recovery pathways for major abdominal surgery. 2nd enhanced recovery after surgery (ERAS) USA symposium; 2014. New Orleans
Kehlet H. Modification of responses to surgery by neural blockade: clinical implications. In: Cousins MJ, Bridenbaugh PO (Eds). Neural blockade in clinical anesthesia and management of pain. Philadelphia: Lippincott, 1998:129–75
Hughes MJ, Ventham NT, McNally S, Harrison E, Wigmore S. Analgesia After Open Abdominal Surgery in the Setting of Enhanced Recovery Surgery A Systematic Review and Meta-analysis. JAMA Surg.2014; 149:1224–30.
Acknowledgments
The authors acknowledge the support of Jawaharlal Institute of Post Graduate Medical Education and Research (JIPMER, Pondicherry) towards the conduct of the study.
Author information
Authors and Affiliations
Contributions
All the authors were involved in the acquisition and analysis of the data. Dr. Vikram Kate contributed towards the conception of the work and also revised the manuscript critically for intellectual content. Dr. Mohsina Subair was the principal investigator and contributed towards acquisition and analysis of data and preparation of the manuscript. Dr. Sureshkumar, Dr. Shanmugam, Dr. Mahalakshmy, and Dr. Pankaj Kundra contributed towards analysis of data and preparation of manuscript and its critical evaluation.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflicts of interests.
Funding
There are no grants/funds used for this research project.
Rights and permissions
About this article

Cite this article
Mohsina, S., Shanmugam, D., Sureshkumar, S. et al. Adapted ERAS Pathway vs. Standard Care in Patients with Perforated Duodenal Ulcer—a Randomized Controlled Trial. J Gastrointest Surg 22, 107–116 (2018). https://doi.org/10.1007/s11605-017-3474-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-017-3474-2