
Abstract
Background
Single-incision laparoscopic cholecystectomy (SILC) has gained acceptance among surgeons as there is a trend to minimize the invasiveness of laparoscopy. The aim of this meta-analysis has been to assess the feasibility and safety of SILC when compared to conventional multiport laparoscopic cholecystectomy (CMLC).
Methods
A literature search for trials comparing SILC and CMLC was performed. Studies were reviewed for the outcomes of interest: patient characteristics; operative time and conversion rate; postoperative pain; length of hospital stay; postoperative complications; and patient satisfactory score (0–10). Standardized mean difference (SMD) was calculated for continuous variables and odds ratio for qualitative variables.
Results
Twelve prospective randomized trials comparing SILC and CMLC were analyzed. Overall, 892 patients were randomized to either SILC (465) or CMLC (427). Operative time was significantly longer in SILC (63.0 vs. 45.8 min, SMD = 1.004, 95% CI = 0.434–1.573). Patient satisfactory score significantly favored SILC (8.2 vs. 7.2, SMD = −0.759, 95% CI = −1.064 to −0.455). No other difference was found.
Conclusions
SILC is a safe and effective procedure for the treatment of uncomplicated benign gallbladder disease with a significant patient satisfaction. New multicenter randomized trials are expected to evaluate SILC in more complex circumstances such as acute cholecystitis, previous abdominal surgery, and severe obesity.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Currently, laparoscopic cholecystectomy is the gold standard for the treatment of benign gallbladder-related disease. After the laparoscopic revolution during the 1980s,1 the tilt from open to laparoscopic cholecystectomy has become definite. This procedure has gained acceptance among surgeons and patients because of its unquestionable advantages in terms of smaller incision, reduced postoperative pain, shorter hospital stay, and faster return to everyday living when compared to the traditional open approach.2
At the end of the 1990s, a second revolution in the field of laparoscopic surgery has been the introduction of the so-called single-incision laparoscopic surgery (SILS), or single-incision laparoscopic cholecystectomy (SILC) when used for gallbladder removal.3–5 Hypothetically, the benefits of SILC would include those of the conventional multiport laparoscopic cholecystectomy (CMLC) in association with improved cosmetic results and patient satisfaction as the operation is performed through just one incision.
Almost all published manuscripts of the 2000s on this subject concluded that prospective randomized studies are needed to determine the true advantages and limits of SILC cholecystectomy. From 2010 and thereafter, 13 prospective randomized clinical trials comparing the clinical outcomes of SILC vs. CMLC cholecystectomy have been published.6–18 However, most studies have been limited by a small sample size and a single-institution design. Up to the present, only some reviews and one meta-analysis have been performed to compare and summarize the results of SILC cholecystectomy with those of the CMLC cholecystectomy by a pooled analysis.19–21 To overcome these limitations, we performed a new meta-analysis which included the largest number of patients from all prospective randomized clinical trials in the literature. The aim of this new study has been to assess and validate the scientific evidence of the feasibility and safety of SILC cholecystectomy when compared to the standard laparoscopic approach and to verify its advantages and limits.
Materials and Methods
A systematic literature search was performed using Embase, Medline, Cochrane, and PubMed databases for studies comparing SILC to CMLC by using the following keywords: “single-incision laparoscopic cholecystectomy” or “single-incision laparoscopic surgery,” or “SILC” or “SILS,” “single-port access” or “SPA,” or “laparoendoscopic single-site” or “LESS,” and “cholecystectomy” and “laparoscopy.” The search was extended by the “related article” function of databases and by scanning the references of all relevant articles. Literature search was completed in March 2012.
For the purpose of this study, we defined SILC cholecystectomy as an operation performed through a single skin incision regardless of the surgical device used and CMLC cholecystectomy as the standard four-port procedure.
To enter our analysis, studies had to meet the following criteria: compare the characteristics and perioperative outcomes of patients undergoing SILC and CMLC for benign gallbladder-related disease (gallstones, mud, polyps); be a prospective randomized study comparing the two techniques; and be written in English. Studies were not considered for meta-analysis if (1) the outcomes of interest (as specified below) were impossible to calculate or the standard deviation and confidence interval of the tested parameters were not reported and (2) they were retrospective or not randomized. Two authors (AP and IR) independently extracted the following data from each study: institution and year of publication, study design, patients’ characteristics and the number of patients operated on with each technique, perioperative outcomes, and postoperative results.
Regarding the outcomes of interest for this meta-analysis, all the studies were reviewed for the following data:
-
Patients’ characteristics: age, gender, and body mass index (BMI)
-
Operative outcomes: operative time and conversion to standard procedure or to laparotomy
-
Postoperative recovery: pain on the day of the operation; pain on postoperative day 1 (evaluated by visual analogue scale (VAS) from 0 to 10, where 0 indicated no pain and 10 the maximum pain); and length of hospital stay
-
Postoperative complications such as bleeding, biliary injury, bile leakage, surgical site infection, and incisional hernia (bile spillage from gallbladder rupture or penetration during surgery was not considered in the outcome of interest)
-
Index of postoperative satisfaction and cosmetic results: patient satisfaction score from 0 to 10, where 0 indicated no satisfaction and 10 complete satisfaction
Surgical indications and the inclusion criteria for SILC eligibility were also reviewed as well as the different surgical methods used for single-incision laparoscopy. The presence of an acute cholecystitis was not a criterion of exclusion from the pooled analysis.
Statistical Analysis
Meta-analysis was performed in accordance with the recommendations from the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement.22 Variables were pooled only if evaluated by three or more studies. All statistical analyses were carried out using the MedCalc® 2011 statistical software (version 11.5.1). Meta-analysis was conducted searching for a numerical estimate of the outcomes of interest. For continuous outcomes, the Hedges’ g statistic has been used for the calculation of the standardized mean difference (SMD) under the fixed effects model, which was adjusted for small sample bias (http://www.medcalc.org/manual/meta-continuous.php). Under the fixed effects model, it was assumed that all studies were homogeneous. This assumption has been tested by the heterogeneity test, which was included to calculate the summary SMD under the random effects model according to the method of DerSimonian and Laird.23 We tested for heterogeneity using the random effects model to calculate the Q test and its associated p value. If this test yielded a p value <0.05, then the fixed effects model was considered invalid and the random effects model as appropriate. The results of the individual studies have been listed and the total SMD with 95 % confidence interval (CI) has been given both for the fixed effects model and the random effects model. If the value 0 was not within the 95% CI, then the SMD was considered statistically significant at the 5 % level (p < 0.05).
This method required the standard deviations and the confidence intervals of the tested parameters. Those studies that did not report any of these parameters were excluded from the meta-analysis. The results of the different studies, with 95% CI and the overall SMD, have been summarized and reported using a forest plot.
For data derived from contingency tables (qualitative outcomes), we calculated the odds ratio (OR) and 95% CI (http://www.medcalc.org/manual/meta-oddsratio.php). In descriptive statistics, the OR is the ratio of the odds of an event occurring in one group to the odds of it occurring in another group (http://www.medcalc.org/calc/odds_ratio.php). When the data on ORs from multiple trials are combined, the result is a weighted summary OR, also called pooled OR. Thus, the ORs reported in the results are that of the pooled analysis method (http://www.medcalc.org/manual/meta-oddsratio.php). The Mantel–Haenszel method was used for calculating the weighted summary OR under the fixed effects model. Then, the heterogeneity test was incorporated to calculate the summary OR under the random effects model according to the method of DerSimonian and Laird.23 If this test yielded a p value <0.05, then the fixed effects model was considered invalid and the random effects model as appropriate. The results of individual studies have been listed and the total OR with 95% CI has been given both for the fixed effects model and the random effects model. If the value 1 was not within the 95% CI, then the OR was considered statistically significant at the 5 % level (p < 0.05). The results of different studies, with 95% CI and the overall effect (summary OR) with 95% CI, have been summarized on a logarithmic scale using a forest plot.
Results
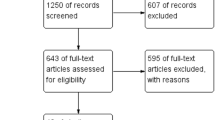
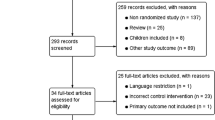
The flowchart for systematic review is shown in Fig. 1. Twelve randomized prospective trials comparing SILC and CMLC were considered suitable for the meta-analysis.6–10,12–18 One prospective randomized trial was excluded because it showed the preliminary data of another study.11 The articles included in the quantitative synthesis were published between February 2010 and February 2012. Three studies were conducted in China, two in the USA, two in Italy, one in Greece, one in Japan, one in Switzerland, one in Taiwan, and one in Turkey. These studies included overall 892 patients with laparoscopic cholecystectomy randomized to either SILC (465, 52.1 %) or CMLC (427, 47.9 %). The methods of randomization used in the included trials were patient random assignment using a closed envelope in three studies6,8,15; envelope opened by an assistant in one study13; blinded envelope system in one study7; envelope by randomization card in one study10; envelope with computer-generated randomization in two studies9,14; allocation by randomization table in one study16; random allocation software in one study;18 and randomization by computerized mathematical algorithm in another study.12 The trial by Asakuma et al.17 was quasi-randomized because allocation to SILC or CMLC cholecystectomy was based only on the day of the week. In the sensitivity analysis, the results were similar after exclusion of this study, so its inclusion did not bias the meta-analysis. Two reviewers were found to be 100 % in agreement about the data extracted from the studies.

Systematic search and selection of articles for meta-analysis
The characteristics of the included studies as well as the different surgical methods used for single-incision laparoscopy, surgical indications, and inclusion criteria for SILC eligibility are shown in Tables 1, 2, and 3. Only two prospective randomized trials considered acute cholecystitis as an inclusion criterion for SILC eligibility, which was insufficient for pooled analysis.15,16
Patients’ Characteristics
The baseline characteristics of patients are summarized in Table 1. Patients in both groups were similar with respect to age (50.3 vs. 49.8 years, SMD = 0.134, 95% CI = −0.052 to 0.320; no heterogeneity was found: Q = 13.66, p = 0.057; Fig. 2) and rates of female gender (0.65 vs. 0.63, OR = 0.86, 95% CI = 0.626–1.182; no heterogeneity was found: Q = 6.36, p = 0.70; Fig. 3).

Meta-analysis of patient characteristics with respect to age

Meta-analysis of patient characteristics with respect to gender
BMI was 26.1 vs. 26.7 for the SILC group and the CMLC group, respectively (SMD = −0.121, 95% CI = −0.315 to 0.073; no heterogeneity was found: Q = 8.93, p = 0.177; Fig. 4).

Meta-analysis of patient characteristics with respect to body mass index (BMI)
Operative Outcomes
Mean operative time was significantly longer in the SILC group than in the CMLC group (63.0 vs. 45.8 min, SMD = 1.004, 95% CI = 0.434–1.573). However, the random effects model was considered as appropriate, the test for heterogeneity being statistically significant (Q = 42.09, p < 0.0001; Fig. 5). The conversion rate to laparotomy was similar in the two groups, without significant difference (0.004 vs. 0.007, OR = 0.86, 95% CI = 0.318–2.335; no heterogeneity was found: Q = 1.11, p = 0.99; Fig. 6 and Table 4).

Meta-analysis of patient characteristics with respect to operative time

Meta-analysis of patient characteristics with respect to conversion rate to laparotomy
Postoperative Recovery
The meta-analysis of postoperative abdominal pain evaluation showed no statistical difference between SILC and CMLC with respect to pain 6 h after the operation (mean VAS score = 2.9 vs. 2.7, SMD = −0.02, 95% CI = −0.645 to 0.593; heterogeneity was found for Q = 6.14 and p = 0.04; Fig. 7) and pain 24 h postoperatively (mean VAS score = 2.2 vs. 2.5, SMD = −0.28, 95% CI = −0.861 to 0.296; heterogeneity was found for Q = 15.34 and p = 0.001; Fig. 8).

Meta-analysis of patient characteristics with respect to pain evaluation 6 h after the operation

Meta-analysis of patient characteristics with respect to pain evaluation 24 h after the operation
Despite the mean postoperative hospital stay being shorter in the SILC group than in the CMLC group (2.0 vs. 2.2 days), this difference was not significant (SMD = −0.33, 95% CI = −0.704 to 0.040; heterogeneity was present for Q = 15.68 and p = 0.007; Fig. 9).

Meta-analysis of patient characteristics with respect to postoperative hospital stay
Postoperative Complications
The overall morbidity rate was higher in the SILC group than in the CMLC group, but this difference was not statistically significant (0.13 vs. 0.09, OR = 1.16, 95% CI = 0.740–1.827; no heterogeneity was found for Q = 3.11 and p = 0.98; Fig. 10). Postoperative bleeding was shown in 1.0 % of SILC cholecystectomies and in 0.9 % of CMLC cholecystectomies, but this difference was not significant (0.010 vs. 0.009, OR = 1.19, 95% CI = 0.377–3.813; no heterogeneity was found for Q = 0.99 and p = 0.91; Fig. 11).

Meta-analysis of overall postoperative morbidity

Meta-analysis of postoperative outcome with respect to bleeding
The prevalence of surgical site infection was 4.0 % in the SILC group vs. 1.6 % in the CMLC group, and the site of infection was always the umbilical incision in both groups. However, this difference was not statistically significant (0.040 vs. 0.016, OR = 1.84, 95% CI = 0.890–3.821; no heterogeneity was found for Q = 4.86 and p = 0.93; Fig. 12).

Meta-analysis of postoperative outcome with respect to surgical site infection
Postoperative incisional hernia was always found at the umbilical port site in both groups. The prevalence of incisional hernia was 1.3 % in the SILC group vs. 0.2 % in the CMLC group, but this difference was not statistically significant (0.013 vs. 0.002, OR = 2.346, 95% CI = 0.607–9.067; no heterogeneity was present for Q = 0.45 and p = 0.97; Fig. 13 and Table 5).

Meta-analysis of postoperative outcome with respect to incisional hernia
Postoperative Satisfaction and Cosmetic Results
Only three studies reported the results of patient satisfaction score from 0 to 10.7,9,14 Other studies reported no results about patient satisfaction6,17,18 or reported different scores insufficient for pooled analysis.8,10,13,15,16 In the trial by Lee et al.,7 cosmetic outcome was self-assessed by patients 1 and 6 months after surgery using a scale ranging from 1 (poor) to 10 (excellent). During follow-up, a questionnaire was administered, which partly considered the appearance of scars. Zheng et al.9 assessed the degree of satisfaction with the operation by a questionnaire where 0 indicated no satisfaction and 10 complete satisfaction. Lai et al.14 assessed the cosmetic satisfaction of the surgical scar. The appearance of each incision was rated on a scale of 1 (worst) to 10 (best) at the 3-month follow-up visit by patients. Ma et al.12 rated patient cosmetic satisfaction using a ten-point scale, with a 9.3 score in the SILC group vs. 8.9 in the CMLC group, without significance difference between the groups. This study was excluded from the meta-analysis of cosmetic outcome because the standard deviations and the confidence intervals were not reported. Finally, the pooled analysis for patient satisfactory score after the operation favored the SILC group, and this difference was statistically significant with no heterogeneity (8.2 vs. 7.2, SMD = −0.759, 95% CI = −1.064 to −0.455, Q = 0.15, p = 0.92; Fig. 14 and Table 6).

Meta-analysis of patient satisfactory score
Discussion
Nowadays, SILC cholecystectomy is gaining more and more popularity, and there is a trend to replace CMLC cholecystectomy with the aim of minimizing the invasiveness of the procedure, achieving better quality of life in terms of reduced postoperative pain and optimized cosmesis.13 To the best of our knowledge, this is the second meta-analysis well matching the results of SILC cholecystectomy with those of CMLC cholecystectomy. The previous study included seven randomized clinical trials for a total of 375 patients,21 while our pooled analysis included 12 clinical trials for a total of 892 patients randomized for both techniques. The results of our meta-analysis show that SILC cholecystectomy is a safe and effective procedure for the treatment of non-complicated, benign gallbladder disease with postoperative outcomes comparable to that of the standard laparoscopic cholecystectomy.
This pooled analysis shows no significant difference between groups regarding the demographic characteristics of patients such as age and gender. However, the prerequisite of a BMI <30 or <35 as inclusion criteria in the majority of considered trials does not allow meaningful conclusions about the indications of SILC cholecystectomy in obese patients.
The main disadvantage of SILC cholecystectomy has been the duration of the operation as the mean operative time was significantly longer in the SILC group than in the CMLC group (63.0 vs. 45.8 min, SMD = 1.004, 95% CI = 0.434–1.573). The significantly longer duration of SILC is related to technical problems of a new and evolving technique and to the need of completing a learning curve, as previously documented.11,24 At the beginning, SILC cholecystectomy may be technically cumbersome, and the difficulties include achievement of similar critical views of safety because of the lack of triangulation; multiple collisions of instruments; handling the roticulating instruments on a mirror image because the right hand controls the left-sided instrument on the screen and the left hand operates the right-sided instrument; and the need for both an experienced surgeon and a camera assistant.15,18,20 Education, training, and experience can shorten the operative time, while the evolution of the instrumentation will certainly enhance the overall ergonomics of SILC.13,20 Unfortunately, data from the included trials were insufficient to define a learning curve measuring how quickly surgeons with good experience with CMLC can master SILC safely. Further studies are needed to prospectively evaluate this subject, although a number of cases ranging from 5 to 10 have been suggested to reach a plateau in operative time,12,25 and a learning curve of 20–25 cases has been recommended for the safe handling of SILC.26
In the current meta-analysis, the similar conversion rate to laparotomy of SILC and CMLC and the irrelevant number of SILC converted to CMLC demonstrate the feasibility of the procedure in the case of non-complicated gallbladder disease. All but two of the considered trials excluded patients with acute cholecystitis and those cases submitted to previous abdominal surgery, making applying the results to all patients undergoing cholecystectomy impossible. Our analysis showed that only two trials included patients with acute cholecystitis with similar results when treated with the SILC technique.15,16 Acute cholecystitis has been previously considered as a significant factor for failure of SILC with a cumulative success rate of 59.9 vs. 93 % for studies excluding acute cholecystitis.20
The overall morbidity rate was higher in the SILC group (13.1 vs. 9.8 %), and it was mainly represented by the surgical site infection and postoperative incisional hernia at the umbilical site. However, the difference in total adverse events was not statistically significant, showing that SILC was as safe as CMLC (OR = 1.16, 95% CI = 0.740–1.827). The higher rates of surgical site infection (4.0 vs. 1.6 %) and incisional hernia (1.3 vs. 0.2 %) in SILC than in CMLC, respectively, have been ascribed to local ischemia induced by the placement of a single larger port or by multiple ports at a single site, which could weaken the fascia.10,19 The too short follow-up suggests approaching the result on incisional hernia as no definitive because all included studies have been published from 2010 to 2012. Moreover, the expected cosmetic results could be compromised by these complications in individual patients.19
The safety of the SILC procedure is mainly related to the absence of major biliary injuries both in the SILC group and in the CMLC group, as demonstrated in this study. However, this result must not create a false sense of security in surgeons until the processes of SILC standardization will be completed.21,27 When SILC cholecystectomy is performed in a center specializing in minimally invasive surgery and patients are included in controlled trials, biliary injuries are approaching the nadir incidence without major damage. Indeed, the uncontrolled diffusion of SILC has been considered as responsible for an increased number of bile duct injuries that have already been reported with a complication rate as high as 0.7 %.28
One of the expected outcomes of SILC cholecystectomy is the reduced postoperative pain when compared to traditional CMLC.6,19 The results of the present investigation show that there is no significant difference between SILC and CMLC with respect to postoperative pain intensity when assessed by the VAS score. Difficulty in pain control after SILC has been noted in the literature, and this procedure was shown to be even associated with increased early postoperative pain.10,29 It is likely that the increased size of the incision and the higher pressure around the umbilical port during SILC may increase the intensity of postoperative pain sensation.12,13,20
The analysis of the outcomes of interest showed that the mean postoperative hospital stay was shorter in the SILC group than in the CMLC group (2.0 vs. 2.2 days, respectively), but this difference was not statistically significant. At this point, the hypothesis that the higher operative costs of SILC could be balanced by an earlier patient discharge from the hospital needs to be further verified. The higher operative cost of SILC cholecystectomy depends on the particular dedicated instruments used. In this meta-analysis, only one trial estimated the additional cost of SILC cholecystectomy at US $400 per procedure.16 On the other hand, the cost for SILC does not differ significantly from that for CMLC when standard materials are used.30 However, further prospective studies are expected to better analyze the true cost effectiveness of the SILC procedure.
Only three of the included trials reported the results of patient satisfaction score from 0 to 10, and they were related to the excellent cosmetic outcome assessed from 1 to 6 months after the operation.7,9,14 Other studies reported no results about patient satisfaction and cosmesis or the different scores used being insufficient for pooled analysis. Patient satisfactory score after the operation favored the SILC group with a statistically significant difference (8.2 vs. 7.2, SMD = −0.759, 95% CI = −1.064 to −0.455). On the other hand, the results on the cosmetic outcome after CMLC cholecystectomy are quite high, and the analysis can also be interpreted as there is little difference between SILC and CMLC. Indeed, the satisfactory score of SILC cholecystectomy must be verified by a long-term follow-up as it could depend upon the timing of the survey. A thorough analysis of the outcome of interest for this study shows that the expectation of an excellent cosmetic result is reasonable with the SILC procedure provided that safety is guaranteed by a correct and controlled surgical indication.
Conclusions
SILC cholecystectomy is a safe and effective procedure for the treatment of uncomplicated benign gallbladder disease, and it has a good impact on patient satisfaction and cosmetic results. SILC may be proposed as an alternative for cholecystectomy in properly selected patients and in experienced hands. Nevertheless, there are some unanswered questions that need further investigation, such as the prospective assessment of a learning curve and the cost–benefit analysis of the procedure. The indication for SILC cholecystectomy will be extended on a progressive basis, as happened with CMLC cholecystectomy. New larger prospective, multicenter randomized studies are needed to better assess the technique and to demonstrate the feasibility and safety of SILC in more complex circumstances such as acute cholecystitis, previous abdominal surgery, and severe obesity.
References
Mühe E. Die erste: cholecystecktomie durch das laparoskop (The first laparoscopic cholecystectomy). Langenbecks Arch Surg 1986;369:804.
Keus F, de Jong JA, Gooszen HG, van Laarhoven CJ. Laparoscopic versus open cholecystectomy for patients with symptomatic cholecystolithiasis. Cochrane Database Syst Rev 2006;18,4:CD006231.
Navarra G, Pozza E, Occhionorelli S, Carcoforo P, Donini I. One-wound laparoscopic cholecystectomy. Br J Surg 1997;84:695.
Bresadola F, Pasqualucci A, Donini A, Chiarandini P, Anania G, Terrosu G, Sistu MA, Pasetto A. Elective transumbilical compared with standard laparoscopic cholecystectomy. Eur J Surg 1999;165:29–34.
Piskun J, Rajpal S. Transumbilical laparoscopic cholecystectomy utilizes no incisions outside the umbilicus. J Laparoendosc Adv Surg Tech 1999;9:361–364.
Tsimoyiannis EC, Tsimogiannis KT, Pappas-Gogos G, Farantos C, Benetatos N, Mavridou P, Manataki A. Different pain scores in single transumbilical incision laparoscopic cholecystectomy versus classic laparoscopic cholecystectomy: a randomized controlled trial. Surg Endosc 2010;24:1842–1848.
Lee PC, Lo C, Lai PS, Chang JJ, Huang SJ, Lin MT, Lee PH. Randomized clinical trial of single-incision laparoscopic cholecystectomy versus minilaparoscopic cholecystectomy. Br J Surg 2010;97:1007–1012.
Aprea G, Bottazzi EC, Guida F, Masone S, Persico G. Laparoendoscopic single site (LESS) versus classic video-laparoscopic cholecystectomy: a randomized prospective study. J Surg Research 2011;166:109–112.
Zheng M, Qin M, Zhao H. Laparoendoscopic single-site cholecystectomy: a randomized controlled study. Minim Invasive Ther Allied Technol 2012; 21:113–17.
Phillips MS, Marks JM, Roberts K, Tacchino R, Onders R, DeNoto G, Rivas H, Islam A, Soper N, Gecelter G, Rubach E, Paraskevas P, Shah S. Intermediate results of a prospective randomized controlled trial of traditional four-port laparoscopic cholecystectomy versus single-incision laparoscopic cholecystectomy. Surg Endosc 2012; 26:1296–303.
Marks J, Tacchino R, Roberts K, Onders R, Denoto G, Paraskeva P, Rivas H, Soper N, Rosemurgy A, Shah S. Prospective randomized controlled trial of traditional laparoscopic cholecystectomy versus single-incision laparoscopic cholecystectomy: report of preliminary data. Am J Surg 2011;201:369–373.
Ma J, Cassera MA, Spaun GQ, Hammill CW, Hansen PD, Aliabadi-Wahle S. Randomized controlled trial comparing single-port laparoscopic cholecystectomy and four-port laparoscopic cholecystectomy. Ann Surg 2011;254:22–27.
Lirici MM, Califano AD, Angelini P, Corcione F. Laparo-endoscopic single site cholecystectomy versus standard laparoscopic cholecystectomy: results of a pilot randomized trial. Am J Surg 2011;202:45–52.
Lai ECH, Yang GPC, Tang CN, Yih PCL, Chan OCY, Li MKW. Prospective randomized comparative study of single incision laparoscopic cholecystectomy versus conventional four-port laparoscopic cholecystectomy. Am J Surg 2011;202:254–258.
Cao GZ, Cai WC, Qin MF, Zhao HZ, Yue P, Li Y. Randomized clinical trial of single-incision versus conventional laparoscopic cholecystectomy: short-term operative outcomes. Surg Laparosc Endosc Percutan Tech 2011;21:311–313.
Bucher P, Pugin F, Buchs NC, Ostermann S, Morel P. Randomized clinical trial of laparoendoscopic single-site versus conventional laparoscopic cholecystectomy. Br J Surg 2011;98:1695–1702.
Asakuma M, Hayashi M, Komeda K, Shimizu T, Hirokawa F, Miyamoto Y, Okuda J, Tanigawa N. Impact of single-port cholecystectomy on postoperative pain. Br J Surg 2011; 98:991–995.
Sinan H, Demirbas S, Ozer MT, Sucullu I, Akyol M. Single-incision laparoscopic cholecystectomy versus laparoscopic cholecystectomy: a prospective randomized study. Surg Laparosc Endosc Percutan Tech 2012;22:12–16.
Chamberlain RS, Sakpal SV. A comprehensive review of single-incision laparoscopic surgery (SILS) and natural orifice transluminal endoscopic surgery (NOTES) techniques for cholecystectomy. J Gastrointest Surg 2009;13:1733–1740.
Antoniou SA, Pointner R, Granderath FA. Single-incision laparoscopic cholecystectomy: a systematic review. Surg Endosc 2011;25:367–377.
Markar SR, Karthikesalingam A, Thrumurthy S, Muirhead L, Kinross J, Paraskeva P. Single-incision laparoscopic surgery (SILS) vs. conventional multiport cholecystectomy: systematic review and meta-analysis. Surg Endosc 2012;26:1205–213.
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, Clarke M, Devereaux PJ, Kleijnen J, Moher D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ 2009; 339:b2700.
DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials 1986;7:177-188.
Philipp SR, Miedema BW, Thaler K. Singl-incision laparoscopic cholecystectomy using conventional instruments: early experience in comparison with the gold standard. J Am Coll Surg 2009;209:632–637.
Kravetz AJ, Iddings D, Basson MD, Kia MA. The learning curve with single-port cholecystectomy. JSLS 2009;13:332–336.
Gill IS, Advincula AP, Aron M, Cadeddu J, Canes D, Curcillo PG 2nd, Desai MM, Evanko JC, Falcone T, Fazio V, Gettman M, Gumbs AA, Haber GP, Kaouk JH, Kim F, King SA, Ponsky J, Remzi F, Rivas H, Rosemurgy A, Ross S, Schauer P, Sotelo R, Speranza J, Sweeney J Teixeira J. Consensus statement of the consortium for laparoendoscopic single-site surgery. Surg Endosc 2010;24:762–768.
Allemann P, Schafer M, Demartines N. Critical appraisal of single port access cholecystectomy. Br J Surg 2010;97:1476–1480.
Hodgett SE, Hernandez JM, Morton CA, Ross SB, Albrink M, Rosemurgy AS. Laparoendoscopic single site (LESS) cholecystectomy. J Gastrointest Surg 2009;13:188–189.
Love KM, Durham CA, Meara MP, Mays AC, Bower CE. Single-incision laparoscopic cholecystectomy: a cost comparison. Surg Endosc 2011;25:1553–58.
Rivas H, Varela E, Scott D. Single-incision laparoscopic cholecystectomy: initial evaluation of a large series of patients. Surg Endosc 2010;24:1403–1412.
Acknowledgments
This study was supported by a grant from the University of Cagliari, Italy (quota ex 60 %). We would like to thank Dr. Eric C.H. Lai from the Department of Surgery, Pamela Youde Nethersole Eastern Hospital, Hong Kong SAR, China, for the help in calculating patient satisfactory scores.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Pisanu, A., Reccia, I., Porceddu, G. et al. Meta-analysis of Prospective Randomized Studies Comparing Single-Incision Laparoscopic Cholecystectomy (SILC) and Conventional Multiport Laparoscopic Cholecystectomy (CMLC). J Gastrointest Surg 16, 1790–1801 (2012). https://doi.org/10.1007/s11605-012-1956-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-012-1956-9