
Abstract
Purpose
A fully automated surgical tool detection framework is proposed for endoscopic video streams. State-of-the-art surgical tool detection methods rely on supervised one-vs-all or multi-class classification techniques, completely ignoring the co-occurrence relationship of the tools and the associated class imbalance.
Methods
In this paper, we formulate tool detection as a multi-label classification task where tool co-occurrences are treated as separate classes. In addition, imbalance on tool co-occurrences is analyzed and stratification techniques are employed to address the imbalance during convolutional neural network (CNN) training. Moreover, temporal smoothing is introduced as an online post-processing step to enhance runtime prediction.
Results
Quantitative analysis is performed on the M2CAI16 tool detection dataset to highlight the importance of stratification, temporal smoothing and the overall framework for tool detection.
Conclusion
The analysis on tool imbalance, backed by the empirical results, indicates the need and superiority of the proposed framework over state-of-the-art techniques.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Fast and accurate recognition of surgical workflow plays an important role in modern computer-assisted intervention (CAI). Modern operating rooms (OR) demand monitoring of surgical processes to reduce preventable errors, the absence of which may result in failures up to the loss of human lives [5]. In addition, multitudes of other OR procedures, for example automated clinical assistance, staff assignment, etc., can benefit from surgical workflow recognition [1, 2, 17]. Recent CAI literature [3, 9, 17, 19] has identified that surgical tool occurrences are closely related to the phases of surgical workflow. Moreover, tool detection and tracking on endoscopic images has the potential of controlling a robot-mounted endoscopic camera holder, especially for solo surgeries [11, 18]. Change in illumination, specular reflection and partial occlusion are some of the major challenges that render surgical tool detection a challenging task. This work mainly focuses on a fully automatic identification of surgical tool(s) from endoscopic video streams.

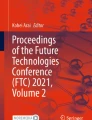
Chord diagram [6] showing the second-order co-occurrences of tools (two tools together) in M2CAI16 tool detection training dataset. Tool usage frequency is color-coded in a discrete fashion: red (0–160), yellow (160–1000) and green (>1000)
State-of-the-art methods treat surgical tool detection as a supervised multi-class or one-vs-all classification task [17]. Based on the observation that multiple tool co-occurrences happen quite often in endoscopic video frames, we have formulated the task as a generalized multi-label classification. The co-occurrence of tools, formally termed as label-sets, forms the output set of multi-label classification. In particular, rather than treating each tool as a stand-alone class, we’ve considered label-sets of multiple tools, along with the introduction of a no-tool (i.e., background) class. Second-order co-occurrences of tools along with frequency of occurrences are visualized in Fig. 1 for intuitive understanding. Interesting tool co-occurrence relationship patterns emerge from such visualization. For example, though hook is the most often used tool in surgical intervention, in second order, it is used only in association with grasper. Other interesting relationships involving two-tool usage can also be inferred from Fig. 1.
One key observation of this work is the imbalance associated with the tool usage (could be understood intuitively from Fig. 1). It has already been proven that the imbalance in data affects the binary and multi-class classification accuracy [4]. However, the imbalance associated with the tool usage during a surgery has not been quantified before. In this work, imbalance in tool usage during an endoscopic intervention is analyzed quantitatively using the measures introduced by Charte et al. [4]. Moreover, the effects of tool usage imbalance on detection accuracy are quantitatively analyzed in a novel experimental setup and specific sampling strategy to address imbalance [13] in tool usage is introduced during CNN training.
Major contributions of this work are twofold. First, surgical tool detection is performed in a generalized multi-label setting, with quantitative analysis focusing on handling surgical tool imbalance. To the best of our knowledge, this is the first work where tool detection is formulated as a general multi-label classification problem. Secondly, a novel transfer learning architecture is proposed for fine tuning and domain adaptation of AlexNet [7] toward a surgical tool identification task. In particular, weighted uni-variate loss (as learning objective) for joint output distribution is adopted for handling residual tool imbalance after stratification.
Related work
Surgical tool detection within endoscopic videos has received increasing attention in recent years [3, 15]. For the sake of brevity, we have mainly considered works where endoscopic video streams are considered as the sole input source. Tool detection procedures from video streams often consider the task as both tool identification and localization problem [3]. For example, Speidel et al. [14] suggested a tool identification pipeline that consists of segmentation and 3D model-based processing. Sahu et al. [11] proposed detection and tracking of surgical tools over the virtual control interface on endoscopic stream to control a robot.
This work, however, similar to Twinanda et al. [17], considers tool detection as a tool presence detection task without explicit localization. For the rest of the paper, “tool detection” is commonly used to refer to automatic tool identification from endoscopic video frames. Twinanda et al. [17] proposed deep learning-based features to be used in one-vs-all classification framework for tool identification without localization. Most recently, performance of different tool detection techniques [10, 12, 16] is quantitatively evaluated in M2CAI16 tool detection challenge. In particular, Twinanda et al. [16] used ToolNet—a network very similar to AlexNet with a final tool detection layer. Raju et al. [10] used an ensemble of two networks and Sahu et al. [12] consisted of a multi-label learning approach with no stratification, followed by random forest for classification. In this work, unlike other proposed techniques, we have generalized the problem as multi-label classification task, quantitatively analyzed the imbalance and adopted strategies to overcome imbalance-related issues.

Upset [8] visualization of the third-order co-occurrence (three tools appearing together) of the tools in M2CAI16 tool detection training dataset. It shows possible three tool combinations (bottom right) with orange and black color representing presence and absence of these combinations in the training dataset respectively. The third-order co-occurrences of the tools are shown on top with corresponding individual tool distribution on bottom left
Method
In this section, we first provide an overview of multi-label classification for tool detection task. Next, we describe metrics used for defining levels of imbalance in a multi-label dataset in “Imbalance quantification” section, followed by a description of stratification technique used to address multi-label imbalance in “Stratification” section. In “ZIBNet” section, ZIBNet architecture is introduced with novel design choices that are incorporated during learning. Finally, we propose temporal smoothing as an online post-processing step which suppresses false positives during prediction.
Multi-label classification
Supervised classification-based surgical tool detection have focused on formulating the problem in a one-vs-all or multi-class setting. Even though simple and intuitive, in this paper we argue that these settings do not address the problem in its general sense. In particular, due to the co-occurrence of multiple surgical tools at different endoscopic video frames, general multi-label classification should be used to model tool presence instead. Multi-label classification is the generalization of binary or multi-class classification. In this scenario, no a priori limit on the number of tools present in the output set is imposed during classification.
For example, second-order co-occurrences of surgical tools (i.e., two tools appearing together) are reported in Fig. 1. In one-vs-all or multi-class classification setting, the desired chord diagram would be an empty circle, penalizing all the interconnected entries. However, plotting the ground truth annotation in Fig. 1 suggests the existence of interconnected entries (more than one tool), which would have been penalized in the earlier settings. Similarly, third-order tool co-occurrence with respect to instrument distribution is visualized in Fig. 2 which shows distribution of three tools appearing together. The presence of the co-occurrences in Figs. 1 and 2 violates the mutually exclusive class assumption of one-vs-all or multi-class classification. This motivates us to model the problem as a multi-label classification one where co-occurrence entries are also considered valid and not penalized during classification.
Formally, for all N annotated video frames in our training dataset \(F \in \{f_i\} \) where \(i=1,2,\ldots , N\), a multi-label classifier C learns to represent the total set of tool labels \(T \in \{t_j\} \) where \(j = 1,2,\ldots ,M\). For a testing video stream, C must produce as output a set \(Z_i \subseteq T\) with predicted tool labels for the i-th video frame. Note that, this generalization results in \(2^M\) potential combinations , which are termed as label-sets. In a general setting, this might result in many practical constraints (e.g., memory for storing, representation and performing actual classification). However due to the practicalities of endoscopic intervention, where only a limited number of tools (maximum three for this particular dataset) and combinations (see Figs. 1 and 2) can be present at once, the multi-label problem remains tractable. In particular, the seven-tool M2CAI16 tool detection dataset has resulted in approximately twenty label-sets spanning from order zero to three.

Proposed CNN architecture. The input layer (blue) size and fully connected layers (orange) are adapted to tool detection task, while the convolution layers are similar to the AlexNet [7] architecture
Imbalance quantification
Even though imbalance in binary and multi-class classifications is a well-studied problem, quantitative analysis of imbalance in multi-label dataset is proposed in very few occasions [4, 13]. Conventional imbalance analysis methods, designed for binary/multi-class classification, assume only the ratio of majority to minority class labels as imbalance measure, therefore, not suitable for multi-label datasets. There exist some traditional metrics notably label cardinality and label density which characterize multi-label datasets. Label cardinality is the average number of active labels per sample, and label density denotes average of label cardinality over the total number of labels. Mathematically, these measures can be defined as follows [4]:
With the presence of multiple label-sets, special metrics are needed for analyzing imbalance in multi-label datasets in detail. In this work, we have exploited imbalance ratio per label (IRLbl), the mean imbalance ratio (MeanIR) and the coefficient of variation of IRLbl (CVIR) introduced in [4] to analyze the imbalance in our tool dataset:
Here IR per label, \(\text {IRLbl}(T_i)\), is calculated as the ratio between the majority (most frequent) label and label \(T_i\). As a result, the majority label will always have \(\text {IRLbl}=1\) and rest of the labels will have higher \(\text {IRLbl}>1\). MeanIR computes the average level of imbalance of the dataset, while CVIR measures variation of IRLbl, i.e., similarity of level of imbalance between all labels. For a perfectly balanced dataset, all IRLbl values would be 1, which results in values of MeanIR and CVIR being 1 and 0, respectively. The joint use of MeanIR and CVIR with values greater than 1 and 0, respectively, denotes the level of imbalance in a multi-label dataset. Moreover, the values of IRLbl greater than 1 can be used for measuring individual label imbalance.
Stratification
Stratification is the process of sampling, where the proportion of disjoint groups is maintained [13]. Stratification in the multi-label data context is a challenging task. Improper stratification might significantly reduce the performance of classifiers as demonstrated by Sechidis et al. [13].
The most intuitive stratification in the tool detection setting would be to consider a balanced strategy. In this setting, the occurrence frequency of the least frequent tool would be considered as the desired sample size and the rest of the tools would be sampled accordingly. However, co-occurrence of tools in different frames actually results in an unbalanced training and validation set.
A better way of handling the problem would be to consider stratification on label-sets. Here, the frequency of label-sets is considered for sampling of image frames. A stratification threshold \(\psi \) is applied, where for more frequent label-sets, \(\psi \) occurrences are sampled randomly, and for less frequent (\({<}\psi \)) label-sets, all samples are considered for training.
ZIBNet
Our proposed CNN architecture (Fig. 3) is composed of three main parts:
-
Input layer which accepts an input image of size \(384\times 256\) pixels.
-
Convolutional layers which are similar to AlexNet architecture.
-
Fully connected layers which are specific to tool detection task with size 512, 64 and 8, respectively.

Appearances of different surgical tools from M2CAI16 tool detection dataset. The tools used during the surgical procedure (left to right) are grasper, bipolar, hook, clipper, scissors, irrigator and specimen bag
Before the learning step, the convolutional layers weights are initialized with AlexNet convolutional weights and the fully connected layers are initialized with random weights. The rectify units are applied to the output of convolutional and fully connected layers except the last fully connected layer which is connected to sigmoid nonlinearity. Since our network contains pre-trained convolutional weights of AlexNet which are generic for earlier convolution layers and become specific to ImageNet objects for higher layers, we assign layer-specific learning rates
where \(\eta \) is the learning rate and \(c_i = [0.1, 0.2, 0.3, 0.4, 0.5, 1.0, 1.0, 1.0]\) is the learning coefficient for each layer. The learning coefficient becomes higher with subsequent convolutional layer, except for the fully connected layers whose coefficients remain fixed since these layers have been randomly initialized. The output layer contains eight units for seven tools and an additional “no-tool” label, which is added to the ground truth and represents that none of the given tools are present in the image, i.e., background.
During the learning step, the network minimizes the joint label distribution through a uni-variate loss function \(\mathcal {L}\) defined as:
where w(t) is a weighting function that normalizes loss in terms of output \(z_t\), and \(y_t\) is prediction for tool t. Intuitively, even after label-set stratification, imbalance on the tool label would not be omitted completely. \(\mathcal {L}\) is formulated as a uni-variate loss function where cross entropy is weighted with tool occurrence frequency in the training data, to manage the residual imbalance after stratification.
To avoid over-fitting, we perform real-time data augmentation (flipping, mirroring and cropping) during learning, apply dropout units for “FC6” and “FC7” layers and use a weight decay of \((10^{-5})\) for every layer. Finally, the network is trained using stochastic gradient descent (\(\eta \) of \((10^{-2})\)) with momentum of 0.9 using the holdout scheme.
Temporal smoothing
Due to the stochastic nature of the classification process, false detections would occur during the testing step. For reducing such false detections, we have adopted a temporal smoothing (TS) approach as an online post-processing step. It assumes that each tool transition within the endoscopic videos is smooth and takes previous frame detections into account in a weighted scheme. A window of five frames (including current and four previous frames) with normalized linear weights determines the current output detection. Mathematically, TS is defined as follows:
where \(y_\mathrm{ts}\) is the temporally smooth output for the current time step, t = 4 and \(w_i = [1.0, 0.8, 0.6, 0.4, 0.2]\) is the weight coefficient for each time step.
Results
This section provides a quantitative analysis of the proposed method, as well as quantitative comparison w.r.t. state-of-the-art methods, to demonstrate its effectiveness for surgical tool detection from endoscopic video streams.
Data preparation
All our quantitative experiments were performed on the M2CAI Tool Detection Challenge 2016 training and testing dataset [16]. The dataset contains 15 clinical cholecystectomy surgical procedures (one video per surgical procedure), which were performed using seven surgical tools (as shown in Fig. 4). The dataset is divided into 10 training and 5 testing videos. The videos were captured at 25 frames per second, but the ground truth (GT) annotation was done at 1 frames per second. A tool was considered to be present only if at least half of the tool tip was visible.

Receiver operating characteristic (ROC) curve for presence detection of each tool
To provide a fair comparison, we only considered average precision (AP) per tool and mean average precision (mAP) for all tools [17] as the comparison metric. For all the experiments, M2CAI tool detection training dataset was used for training and the results were reported on M2CAI Tool Detection Testing dataset with stratification threshold \(\psi = 300\).
Comparison with state-of-the-art methods
The proposed framework (label-set based stratification and weighted uni-variate loss for training ZIBNet followed by TS) results in state-of-the-art performance when relying on mAP for evaluation. We compared the results of our proposed method with the top performing methods from M2CAI Tool Detection Challenge, all of which [10, 12, 16] relied on CNN for tool detection. All the results are taken from M2CAI Tool Detection Challenge website where the respective authors used their own software for training and testing. As Table 1 shows, our proposed method outperformed all other methods. In particular, ZIBNet significantly outperformed [16, 17] in a paired t test with \(p<0.05\). We attribute the superior performance of our proposed method to our particular formulation of the problem as a multi-label one and our novel stratification technique.
For a detailed performance evaluation of our proposed framework, a receiver operating characteristic (ROC) curve for each tool is shown in Fig. 5. Apart from Irrigator and Scissors, all the other tools performed sufficiently well. Difficulties in detecting Scissors is already known [16, 17]; however, the reason behind low performance on Irrigator is analyzed in the remainder of this work (“Discussion and conclusion” section).
Imbalance analysis
We have performed a detailed imbalance analysis of all the tools present in the training and testing dataset. Rather than reporting the exact number of occurrences for each tool, we concentrated on the IRLbl measure for each tool (Table 2). As described in “Imbalance quantification” section, the value of the most frequent tool is 1 and rest have higher values (ideally 1, higher IRLbl means higher imbalance for the associated tool). As we can see in Table 2, the most frequent tool is Hook with IRLbl 1.0. It is interesting to note that Irrigator is almost three times more frequent in training dataset compared to Testing dataset. The effects of imbalance are further reported through other metrics in Tables 2 and 3.
Traditionally, for one-vs-all or multi-class classification, imbalance is reported over the whole dataset using cardinality and density, as shown in Eqs. (1) and (2). However, it is evident from the Eqs. (3) and (4) that overall imbalance of a multi-label dataset can be appreciated only by looking at MeanIR and CVIR together. Imbalance in the training dataset resulted in MeanIR value of approximately 14 times higher than ideal (ideally 1) with 83% variance (ideally 0%) in IRLbl values as reported in Table 3.
Analysis of stratification techniques
We performed quantitative comparison of different sampling approaches to highlight the importance of stratification on the performance of ZIBNet for tool detection. Label-sets-based stratification (“Stratification” section) is compared to unbalanced sampling and tool-level balanced stratification (“Stratification” section). Average precision for each tool and overall mAP is reported in Table 4. In particular, the baseline strategy (no stratification at all)—termed as “Unbalanced” in Table 4, performed worst. Tool-level balanced stratification resulted in an overall increase of 3% over “Unbalanced,” whereas the proposed label-set stratification increased mAP by 9%, as shown in Table 4. It is worth noting that Unbalanced approach favored most frequent tools. Stratification, on the other hand, adapted the network to alleviate this bias and enhanced detection of less frequent tools.
Analysis of temporal smoothing
The last part of our design is to apply TS to decrease stand-alone activations as described in “Temporal smoothing” section. We have run experiments to quantitatively demonstrate the importance of TS. TS is independent of the rest of the proposed framework and as shown in Table 5, consistently improved the performance of both stratification techniques by reducing false positives. In particular, the simple stratification benefited more from TS with an overall mAp increase of 8%, whereas 6% boost in performance was observed for label-set stratification.
Discussion and conclusion
Detection of surgical tools in endoscopic video is an important problem requiring a rigorous understanding of the data as well as an effective handling approach. A successful surgical tool detection technique can potentially improve a multitude of CAI applications. For example, detection of surgical workflow phases can directly benefit from tool detection results. However, tool co-occurrences, change of illumination, specular reflection and partial occlusion make the detection problem significantly more difficult.
This work clearly showed that generalizing the classification problem with domain adaptation can significantly improve classification results. Our proposed method demonstrates that fully automatic tool detection results in an acceptable level of agreement with the manual annotations. By modeling tool co-occurrences as label-sets, we can better handle the inherent structure of surgical tool presence during interventions. Moreover, a detailed study of imbalance in label-sets has motivated us to develop stratification methods for CNN training.
Note that, IRLbl in Table 2 suggests that irrigator has significantly different imbalance ratio between training and testing dataset. Not only our results consistently lead to lowest AP as reported in Tables 4 and 5, ToolNet results by Twinanda et al. [16] also reported the same. This suggests that along appearance difficulties (in case of scissors), label imbalance significantly challenges the performance of CNN.
An important observation of our study is the boost in performance by addition of temporal smoothing as an online post-processing method (no future information is considered). TS consistently enhances detection results for both stratification approaches as reported in Table 5.
This study solely concentrated on tool presence identification; however, future studies of surgical workflow phase recognition can benefit from the insights. In particular, the co-relation of surgical phases with the tools being used therein can be exploited further in the label-set setting. The imbalance of label-sets also suggests special tool co-occurrences which could be used as important phase-transition cues.
In conclusion, this study motivates us to rethink about the standard assumptions regarding surgical tool presence detection. Deviating from de facto supervised one-vs-all or multi-class techniques (the performance of which heavily depends on the co-occurrence frequencies) toward multi-label settings can provide multiple benefits. Finally such fully automatic techniques are expected to be instrumental in advancing the computer assistance during surgical intervention.
References
Allan M, Chang PL, Ourselin S, Hawkes DJ, Sridhar A, Kelly J, Stoyanov D (2015) Image based surgical instrument pose estimation with multi-class labelling and optical flow. In: International conference on medical image computing and computer-assisted intervention, Springer, pp 331–338
Blum T, Feußner H, Navab N (2010) Modeling and segmentation of surgical workflow from laparoscopic video. In: International conference on medical image computing and computer-assisted intervention, Springer, pp 400–407
Bouget D, Benenson R, Omran M, Riffaud L, Schiele B, Jannin P (2015) Detecting surgical tools by modelling local appearance and global shape. IEEE Trans Med Imaging 34(12):2603–2617
Charte F, Rivera AJ, del Jesus MJ, Herrera F (2015) Addressing imbalance in multilabel classification: measures and random resampling algorithms. Neurocomputing 163:3–16
Donaldson MS, Corrigan JM, Kohn LT (2000) To err is human: building a safer health system, vol 6. National Academies Press, Washington
Gu Z, Gu L, Eils R, Schlesner M, Brors B (2014) circlize implements and enhances circular visualization in R. Bioinformatics. Oxford Univ Press, p btu393
Krizhevsky A, Sutskever I, Hinton GE (2012) Imagenet classification with deep convolutional neural networks. In: Advances in neural information processing systems, pp 1097–1105
Lex A, Gehlenborg N, Strobelt H, Vuillemot R, Pfister H (2014) Upset: visualization of intersecting sets. IEEE Trans Visual Comput Graphics 20(12):1983–1992
Padoy N, Blum T, Ahmadi SA, Feussner H, Berger MO, Navab N (2012) Statistical modeling and recognition of surgical workflow. Med Image Anal 16(3):632–641
Raju A, Wang S, Huang J (2016) M2cai surgical tool detection challenge report. http://camma.u-strasbg.fr/m2cai2016/reports/Raju-Tool.pdf
Sahu M, Moerman D, Mewes P, Mountney P, Rose G (2016a) Instrument state recognition and tracking for effective control of robotized laparoscopic systems. Int J Mech Eng Rob Res 5(1):33
Sahu M, Mukhopadhyay A, Szengel A, Zachow S (2016b) Tool and phase recognition using contextual CNN features. arXiv preprint arXiv:1610.08854
Sechidis K, Tsoumakas G, Vlahavas I (2011) On the stratification of multi-label data. In: Joint European conference on machine learning and knowledge discovery in databases, Springer, pp 145–158
Speidel S, Benzko J, Krappe S, Sudra G, Azad P, Müller-Stich BP, Gutt C, Dillmann R (2009) Automatic classification of minimally invasive instruments based on endoscopic image sequences. In: SPIE medical imaging, International society for optics and photonics, p 72,610A
Sznitman R, Becker C, Fua P (2014) Fast part-based classification for instrument detection in minimally invasive surgery. In: International conference on medical image computing and computer-assisted intervention, Springer, pp 692–699
Twinanda AP, Mutter D, Marescaux J, de Mathelin M, Padoy N (2016a) Single- and multi-task architectures for tool presence detection challenge at M2CAI 2016. arXiv preprint arXiv:1610.08851
Twinanda AP, Shehata S, Mutter D, Marescaux J, de Mathelin M, Padoy N (2016b) Endonet: a deep architecture for recognition tasks on laparoscopic videos. arXiv preprint arXiv:1602.03012
Voros S, Long JA, Cinquin P (2007) Automatic detection of instruments in laparoscopic images: a first step towards high-level command of robotic endoscopic holders. Int J Rob Res 26(11–12):1173–1190
Zappella L, Béjar B, Hager G, Vidal R (2013) Surgical gesture classification from video and kinematic data. Med Image Anal 17(7):732–745
Acknowledgements
This study was funded by German Federal Ministry of Education and Research (BMBF) under the project BIOPASS (Grant No. 16 5V 7257).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Human and animal rights statement
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
This article contains patient data from a publically available dataset.
Rights and permissions
About this article

Cite this article
Sahu, M., Mukhopadhyay, A., Szengel, A. et al. Addressing multi-label imbalance problem of surgical tool detection using CNN. Int J CARS 12, 1013–1020 (2017). https://doi.org/10.1007/s11548-017-1565-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11548-017-1565-x