
Abstract
Purpose
This study was undertaken to assess the feasibility of real-time elastosonography (RTE) of Achilles tendon in the clinical evaluation of a cohort of children affected by unilateral clubfoot, not surgically treated.
Materials and methods
Twenty patients affected by unilateral clubfoot were evaluated. The study group consisted of 8 males and 12 females (mean age, 16 ± 7.3 months), all treated with the Ponseti method. Children were divided into two groups according to age: group 1 aged 0–18 months, and group 2 aged 18–60 months. Any further systemic pathological conditions were considered exclusion criteria. For each subject, RTE examination of the Achilles tendons was performed bilaterally, and then regions of interest (ROIs) were positioned.
Results
In children aged 0–18 months, the mean value ROI 1/mean value ROI 2 ratio was 2.0 ± 0.18 and it showed a statistically significant difference if compared to the same ratio from healthy tendons, 2.5 ± 0.17 (p < 0.05). In group 2 (children aged 18–60 months) the mean ROI 1/mean value ROI 2 ratio value was 1.8 ± 0.27, compared to a 2.04 ± 0.21 (p < 0.05) ratio in healthy tendons.
Conclusion
RTE is a feasible, reliable and easily performed technique that allows an accurate study of the mechanical properties of Achilles tendon in children with clubfoot.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Congenital clubfoot is a common disorder present at birth that affects the musculoskeletal system with an overall incidence of 1:1000 newborns. This congenital defect includes four main types of foot alteration: equinus foot, hindfoot varus, forefoot adductus and cavus [1].
Several theories have been suggested in order to explain the pathogenesis of idiopathic congenital clubfoot, including genetic factors and vascular deficiencies. Despite these theories, it is still considered as a multifactorial disease [2], caused by the interaction of different aetiological factors. Abnormal development of leg muscles, genetic defects in growth of the connective tissue, abnormal tendon insertions, and tight deltoid ligaments, have all been described [3–6] as possible aetiologies.
Idiopathic clubfeet usually show resistance to manipulation due to deformity of the affected feet. This pathology has been classified into two systems, the Dimeglio and the Pirani classifications, both correlating the severity of this condition with physical findings [7]. Currently, the Ponseti method is the preferred nonsurgical technique used for treatment, and it consists in a deep stretching of the peronei and foot dorsi-flexor muscles, in order to normalise foot position and to provide correct posture [8].
To the best of our knowledge, there are no studies investigating the properties of mechanical stiffness of Achilles tendon in patients affected by unilateral idiopathic clubfoot. Many pathogenetic theories have been suggested for monolateral clubfoot on the basis of specific anatomical abnormalities, even though this pathological condition still remains idiopathic [9]. It was observed that unilateral clubfoot might be associated with a lower calf circumference, and this may result in quantitative differences of the muscular masses, when two series of patients with unilateral clubfoot are compared [9]. Moreover, it has been reported by several authors, such as Ippolito and Ponseti, that a greater presence of fibrous tissue can be observed in the muscles, in the fascia, in the ligaments and in the tendon sheaths [10]: this may lead to an increased stiffness of all the involved anatomical structures.
Recently, real-time elastosonography (RTE) has been proposed as a technique able to assess the differences in stiffness between diverse tissues using ultrasound (US). It has also been suggested for the evaluation of tissue distortion, as well as of muscle and tendon stiffness [11].
The aim of our study was to assess the usefulness of RTE of the Achilles tendon in the clinical evaluation of a cohort of children affected by unilateral clubfoot, not surgically treated.
Materials and methods
Study population
After the approval from the Ethics Committee of our institution, 20 young patients (8 males and 12 females) affected by unilateral idiopathic clubfoot were consecutively examined. All children were treated with the noninvasive Ponseti method. The mean age of the study population was 16 ± 7.3 months. Written informed consent was obtained from the parents of all children, in accordance with the Declaration of Helsinki.
The clinical evaluation for all enrolled patients was performed by a single orthopaedic surgeon with 35 years of clinical experience at our institution. Children who were found to be affected by any systemic condition, any connective tissue disorder, any metabolic and/or endocrine disease, or patients with a history of tendon injury and surgery were excluded from the study group. The entire study group was then divided into two subgroups, according to age: the first group (group 1) included 13 children aged between 0 and 18 months, while the second group (group 2) included 7 children aged from 18 to 60 months. Each study subject was then referred to perform the US examination for bilateral morphological evaluation and RTE of Achilles tendons. B-mode ultrasound was performed along the entire length of the Achilles tendon, bilaterally, from the distal enthesis to the proximal myotendinous junction, defining its echotexture and searching for sonographic signs of previous traumatic injury or signs of tendon degeneration. After B-mode assessment was completed, sonoelastography with RTE was performed.
Examination protocol
Morphological (B-mode) examination and RTE were both performed using a commercially available US system (iU22, Philips Medical Electronics Systems N.V. Corporation) with multifrequency US probe (7.5–12 MHz), by three radiologists experienced in paediatric musculoskeletal imaging (M.S. with 22 years of experience, A.M. with 13 years of experience, M.D. with 11 years of experience).
The radiologists selected a region of interest (ROI) within the Achilles tendons, on the short and on the long axis of the tendon. We agreed on positioning the ROI on the distal third of the Achilles tendon in order to standardise the evaluation of the tendon itself. For all patients, Achilles tendons were assessed bilaterally in order to obtain two values from each subject, and to compare data from healthy tendons with those from affected sides.
Correlation between RTE-Me of Achilles tendon in clubfeet (Figs. 2, 4) and healthy Achilles tendons was obtained (Figs. 1, 3). Colour-coded images were evaluated to obtain a ratio between the values of ROI 1 and ROI 2.

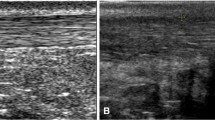
a Conventional axial B-mode ultrasound scan and superimposed, b sonoelastogram of a normal Achilles tendon, at the distal third. Elastography was obtained by positioning two circular ROIs, measuring about 4 mm in diameter, respectively, on the Achilles tendon and on bone tissue. c The strain index and the ratio were calculated between the Achilles tendon and the bone
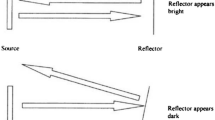
Postprocessing software (Philips Medical Electronics Systems N.V. Corporation) with associated screen indicator provided the operator with real-time feedback for the appropriate amount of deformation of recorded elastogram for each site. The total amount of deformation used to compute the strain of elastogram is represented by the sum of the inherent or physiologic patient-motion and the external compression form the probe.
The probe is held in place manually, while the patient is kept at rest. Analysis of the elastosonogram begins with a strain indicator of the probe that expresses the exact pressure exerted by the radiologist. A range of colours shows the relative hardness and softness of the ROI, conventionally varying from blue to red.
First, tendons from the affected clubfoot were evaluated, and then measurements were obtained from the contralateral healthy tendons. Examinations were performed consecutively, and all the study population was examined in one time. Overall examination time was approximately 14 min for each patient (7 min per side).
The colour-coded images were analysed on a personal computer using the QLAB (developed by Philips Medical Systems), which allows the operator to select a 30-frame images/cine-loop and to position manually two circular ROIs, with the same area of 4 mm, identified in our study as ROI 1 and ROI 2.
ROI 2 was used as a reference standard and it was positioned on the bone tissue. ROI 1 was placed on the central segment, on the proximal or distal segment of Achilles tendons, in order to obtain the value of strain index (SI = ROI 1/ROI 2) (Figs. 1, 2, 3, 4). All pixels data from the colour-coded images were converted into a histogram and values of RTE-Mean elasticity (RTE-Me) were calculated. RTE-Me was reported in arbitrary units (a.u.) (Figs. 1c, 2c, 3c, 4c). Analysis was repeated in quadruplets (one for each examination) and final data were expressed as an average value of the different results.

a Conventional axial B-mode ultrasound scan and superimposed, b sonoelastogram of the Achilles tendon, at the distal third, in clubfoot showing a diffuse hyperechoic pattern, in grey scale, associated with low elasticity of the structure, evaluated by sonoelastography. Elastography was evaluated by positioning two circular ROIs, about 4 mm in diameter, respectively, on the Achilles tendon and on the bone tissue. c The strain index and the ratio were calculated between the Achilles tendon and the bone

a Longitudinal B-mode ultrasound scan and superimposed, b sonoelastogram of the Achilles tendon, at the distal third. The elastography was evaluated positioning two circular ROIs, measuring about 4 mm in diameter, respectively, on the Achilles tendon and on the bone tissue. c The strain index and the ratio were calculated between the Achilles tendon and the bone

a Longitudinal B-mode ultrasound scan and superimposed, b sonoelastogram of the Achilles tendon, at the distal third, in clubfoot showing a diffuse hyperechoic pattern highlighted in grey scale, associated with low elasticity of the structure, evaluated by sonoelastography. Elastography was evaluated by positioning two circular ROIs, measuring about 4 mm in diameter, respectively, on the Achilles tendon and on the bone tissue. c The strain index and the ratio were calculated between the Achilles tendon and the bone
Data analysis
The Student’s t test and standard deviation (SD) were used to assess variation of continuous parameters in order to obtain an average value of the different real-time measurements. Categorical data were evaluated using percentage values. The elastographic images with the concomitant histogram were reported in table format and processed using statistical software (IBM SPSS Statistics for Microsoft Excel).
Results
Among our study population, no statistically significant difference was observed in the characteristics of the tendons and the sex of the patients.
Decreased elasticity of the Achilles tendon was observed in clubfoot (Figs. 1, 2, 3, 4), and this finding was more remarkable in younger patients. Statistically significant differences were found in pathological Achilles tendons from both subgroups (group 1 and group 2), when compared to healthy tendons. In group 1 (children aged 0–18 months) the value of mean ROI 1/mean value ROI 2 ratio was 2.0 ± 0.18, compared to the 2.5 ± 0.17 (p < 0.05) ratio of healthy tendons. The same ratio in group 2 (patients aged 18–60 months patients) was statistically different, but a lower discrepancy could be observed between the values from the two different groups (Table 1). In group 2 (children aged 18–60 months) the value of mean ROI 1/mean ROI 2 ratio was 1.8 ± 0.27, compared to the 2.04 ± 0.21 (p < 0.05) ratio of healthy tendons.
Morphological (B-mode) assessment, performed by longitudinal and transverse scans, did not show any significant focal lesions, and did not reveal significantly different results in bilateral Achilles tendons. In longitudinal scans, homogenous, hyperechoic, linear continuous shadows with regular margins appeared, in the Achilles tendons; while, in transverse scans, the Achilles tendons were elliptical, homogenous and echogenic in appearance.
Discussion
Idiopathic clubfoot is one of the most common musculoskeletal congenital disorders with several deformities affecting bone, ligaments and tendons [12, 13]. A nonsurgical treatment technique, named the Ponseti method, is the currently preferred treatment method and is usually performed in infants affected by congenital clubfoot with defective or absent muscles [14]. In this setting, a correct evaluation of every aspect concerning the Achilles tendon may be helpful in the approach to treatment planning. In our study, a sonoelastosonography evaluation was performed to obtain a tensile test which shown a condition of chronic tendinopathy involving the entire Achilles tendon.
A chronic state of tendinopathy might lead to softening and weakening of collagenic and elastin structures increasing the risk of tendon rupture [15]. Although no signs of achillodynia were present, after RTE a decreased elasticity of Achilles tendons was observed in clubfoot.
While B-mode morphological ultrasound provided structural information, sonoelastography showed a light red colour code along the structure of Achilles tendon with reduced values of elasticity comparing to the normal internal control (healthy) contralateral tendons [16]. Therefore US sonoelastography is considered to be a helpful technique for detection and characterisation of Achilles tendinopathy for its high sensitivity and specificity in the detection of intratendon alterations [17]. Main RTE alterations were observed on the distal portion of the tendon, which was represented by a weaker structure, both at rest and on stress, characterised by decreased values of elasticity and a green colour [18]. We decided to position the ROI in the distal third of the Achilles tendon, in order to standardise the evaluation of the tendon itself. In fact, during the growth of the tendons, these structures undergo morphological changes, such as an increased vascularisation occurring on the distal and proximal thirds and an associated loss of vascularisation in the middle third [19]. Moreover, De Zordo et al. [17] have observed a distinct softening of symptomatic Achilles tendons, occurring on the distal and middle third more frequently than the proximal third of the tendon.
A strongly heterogeneous pattern was found, and this result is probably associated with the different mechanical properties of the various tissue components within normal and pathologic tendons [18]. Previous magnetic resonance imaging studies reported heterogeneous appearance of Achilles tendons, especially in the distal portion, correlated to different viscoelastic properties [20]. These findings are supported by our ultrasonographic data and RTE. Moreover, we were able to assess both resting and stress conditions of the tendon in real time, using sonoelastography. In our present study, a strong correlation was found between the patient’s age and RTE appearance, without any influence of the patient’s sex.
One of the main limitations of the study is that intra- and inter-observer agreement of RTE is still an open question, which has been little investigated in the medical literature. However, all the operators had the same learning curve with regard to RTE examination, each with 32 months of experience. In addition, a previous study demonstrated an excellent inter-operator reproducibility rate for the RTE evaluation [20]. Therefore, we decided to perform the statistical analysis on the mean values of elastic ratios obtained in the different subgroups of patients by three independent operators with the same level of expertise in RTE.
Conclusion
RTE is a feasible and simple technique, which allows the evaluation of mechanical properties of the Achilles tendons in clubfoot, including homogeneous or relatively homogeneous patterns. The strain index can be used as a comparative index between healthy and clubfoot tendons. Overall, RTE may represent a reliable technique for everyday use in clinical practice. One of the main limitations of this study was a lack of correlation of the US data with the histopathological findings in Achilles tendons from the patients affected by clubfoot. Another limitation was the overall small cohort of children enrolled, as well as the wide range included in group 2, (relatively too small a subgroup for such a broad range). This limitation may be the cause for the nonsignificant difference in the second group relative to normal tendons despite a trend towards a difference. On that basis, we believe that further studies of both B-mode and RTE on wider cohorts of patients are needed, in order to obtain additional preliminary RTE data. Further larger studies should also be conducted double-blind and, if possible, with correlation with the histological findings so as to increase the significance of the data.
References
Wynne-Davies R (1964) Family studies and the cause of congenital club foot, talipes equinovarus, talipes calcaneo-valgus and metatarsus varus. J Bone Joint Surg Br 46:445–463
Hootnick DR, Levinsohn EM, Crider RJ, Packard DS Jr (1982) Congenital arterial malformation associated with clubfoot. A report of two cases. Clin Orthop Relat Res 167:160–163
Bechtol CO, Mossman HW (1950) Clubfoot: an embryological study of associated muscle abnormalities. J Bone Joint Surg 32:827
Hoffa A (1905) Lehrbuch der otthopaedischen Chirurgie, 5th edn. Ferrdinand Enke, Stuttgart, p 734
Stewart SF (1951) Clubfoot: its incidence, cause and treatment; an anatomical-physiological study. J Bone Joint Surg 33:577
Hirsch C (1960) Observation on early operative treatment of congenital clubfoot. Bull Hosp Joint Dis 31:173
Flynn JM, Donohoe M, Mackenzie WG (1998) An independent assessment in two clubfoot classification system. J Pediatr Orthop 18:323–327
Ponseti IV (1992) Treatment of congenital clubfoot. J Bone Joint Surg Am 74:448–454
Dobbs MB, Gurnet CA (2012) Genetics of clubfoot. J Pediatr Orthop B 21:7–9
Miedzybrodzka Z (2003) Congenital talipes equinovarus (clubfoot): a disorder of the foot but not the hand. J Anat 202:37–42
Frey H (2003) Realtime elastography: a new ultrasound procedure for the reconstruction of tissue elasticity. Radiologe 43:850–855
Laaveg SJ, Ponseti IV (1980) Long-term result of treatment of congenital clubfoot. J Bone Joint Surg Am 62:23–31
Dobbs MB, Gurnett CA (2009) Update on clubfoot: etiology and treatment. Clin Orthop Relat Res 467:1146–1153
Ponseti IV, Campos J (2009) The classic: observations on pathogenesis and treatment of congenital clubfoot. 1972. Clin Orthop Relat Res 467:1124–1132
Klauser AS, Faschingbauer R, Jaschke WR (2010) Is sonoelastography of value in assessing tendons? Semin Musculoskelet Radiol 14:323–333
Palle L, Reddy MB, Reddy KJ, Kumari MV (2011) Technical note: real-time sonoelastography evaluation of Achilles tendon. Indian J Radiol Imaging 21:267–269
De Zordo T, Chhem R, Smekal V et al (2010) Real-time sonoelastography: findings in patients with symptomatic Achilles tendons and comparison to healthy volunteers. Ultraschall Med 31:394–400
Tan S, Kudaş S, Ozcan AS et al (2011) Real-time sonoelastography of the Achilles tendon: pattern description in healthy subjects and patients with surgically repaired complete ruptures. Skeletal Radiol 41:1067–1072
Daftary A, Adler RS (2009) Sonographic evaluation and ultrasound-guided therapy of the Achilles Tendon. Ultrasound Q 25:103–110
Drakonaki EE, Allen GM, Wilson DJ (2009) Real-time ultrasound elastography of the normal Achilles tendon: reproducibility and pattern description. Clin Radiol 64:1196–1202
Conflict of interest
Salvatore Masala, Guglielmo Manenti, Marco Antonicoli, Daniele Morosetti, Giulia Claroni, Giuseppe Guglielmi, Giovanni Simonetti declare no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Masala, S., Manenti, G., Antonicoli, M. et al. Real time evaluation of monolateral clubfoot with sonoelastography. Radiol med 119, 601–606 (2014). https://doi.org/10.1007/s11547-013-0378-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11547-013-0378-4