
Abstract
Purpose
This study was done to test a series of magnetic resonance (MR) imaging sequences of the knee after medial unicompartmental arthroplasty.
Materials and methods
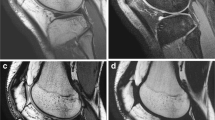
Four patients who had undergone Oxford III medial unicompartmental arthroplasty underwent 1.5-T MR imaging of the operated knee using coronal sequences: T1-weighted spin-echo (SE), T1-weighted turbo SE (TSE), proton-density (PD)- and T2-weighted TSE, T1-weighted gradient echo (GE), short-tau inversion recovery (STIR), multi echo data image combination (MEDIC), T2*-weighted GE, volumetric interpolated breath-hold examination (VIBE), and dual-echo steady state (DESS). For each sequence, we evaluated the visibility of the anatomical structures of the central pivot, lateral compartment, and anterior compartment using a semiquantitative score (0=total masking; 1=insufficient visibility; 2=sufficient visibility; 3=optimal visibility). The sum of the scores given to each sequence was divided by the maximal sum, obtaining a percentage visibility index. Friedman and sign tests were used for statistical analysis.
Results
MR examination time was 30–32 min. No patients reported pain, heat or other local discomfort. The visibility index ranged between 83% and 89% for the first four sequences without significant differences among them, 58% for STIR and 11%–36% for the last five sequences. Significant differences were found between each of the four first sequences and the remaining sequences (p<0.004) and between STIR and the last five sequences (p<0.008).
Conclusions
MR imaging of the knee after medial unicompartmental arthroplasty was not associated with adverse events. An imaging protocol including SE, TSE and STIR sequences could be used to study the knee with unicompartmental arthroplasty.
Riassunto
Obiettivo
Testare una serie di sequenze RM in pazienti portatori di protesi monocompartimentale mediale del ginocchio.
Materiali e metodi
Quattro pazienti portatori di protesi monocompartimentale mediale Oxford III sono stati sottoposti a RM a 1,5 T mediante scansioni coronali: spin-echo (SE) pesata in T1; turbo-SE (TSE) pesata in T1; TSE pesata in densità protonica (DP) e T2; gradient-echo (GE) pesata in T1; short tau inversion recovery (STIR); multi echo data image combination (MEDIC); GE pesata in T2*; volumetric interpolated breath-hold examination (VIBE); dual echo steady state (DESS). Per ciascuna sequenza è stata valutata la visibilità delle strutture anatomiche del pivot centrale, del compartimento laterale e del compartimento anteriore mediante un punteggio semiquantitativo (0=totale mascheramento; 1=insufficiente riconoscibilità; 2=sufficiente riconoscibilità; 3=ottimale riconoscibilità). La somma dei punteggi riportati da ciascuna sequenza è stata divisa per il valore massimo ottenibile, ottenendo un indice percentuale di riconoscibilità. Analisi statistica mediante test di Friedman e test dei segni.
Risultati
L’indagine RM è durata circa 30–32 minuti. Nessun paziente ha lamentato dolore, riscaldamento o altre sensazioni locali. L’indice di riconoscibilità è risultato tra l’83% e l’89% per le prime quattro sequenze, senza differenze significative tra loro, 58% per la STIR e tra l’11% e il 36% per le ultime cinque sequenze. Sono risultate significative le differenze tra le prime quattro sequenze e le rimanenti sei sequenze (p<0,004) e tra la STIR e le ultime cinque sequenze (p<0,008).
Conclusioni
L’indagine RM del ginocchio con protesi monocompartimentale mediale non comporta l’insorgenza di eventi avversi. Le sequenze SE, TSE e STIR potrebbero essere utilmente incluse in un protocollo per lo studio del ginocchio con protesi monocompartimentale mediale.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References/Bibliografia
Laurencin CT, Zelicof SB, Scott RD, Ewald FC (1991) Unicompartmental versus total knee arthroplasty in the same patient. A comparative study. Clinic Orthop Relat Res 273:151–156
Price AJ, Webb J, Topf H et al (2001) Rapid recovery after Oxford unicompartmental knee arthroplasty through a short incision. J Arthroplasty 16:970–976
Robertsson O, Knutson K, Lewold S, Lidgren (2001) The routine of surgical management reduces failure after unicompartmental knee arthroplasty. J Bone Joint Surg Br 83:45–49
Robertsson O (2007) Knee arthroplasty registers. J Bone Joint Surg Br 89:1–4
Murray DW (2007) Mobile bearing unicompartmental knee replacement. Orthopedics 30:768–769
Murray DW, Goodfellow JW, O’Connor JJ (1998) The Oxford medial unicompartmental arthroplasty: a ten-year survival study. J Bone Joint Surg Br 80:983–989
Price AJ, Waite JC, Svard U (2005) Long-term clinical results of the medial Oxford unicompartmental knee arthroplasty. Clin Orthop Relat Res 435:171–180
Walton MJ, Weale AE, Newman JH (2006) The progression of arthritis following lateral unicompartmental knee replacement. Knee 13:374–377
Weale AE, Murray DW, Crawford R et al (1999) Does arthritis progress in the retained compartments after ‘Oxford’ medial unicompartmental arthroplasty? A clinical and radiological study with a minimum ten-year follow-up. J Bone Joint Surg Br 81:783–789
Tibrewal SB, Grant KA, Goodfellow JW (1984) The radiolucent line beneath the tibial components of the Oxford meniscal knee. J Bone Joint Surg Br 66:523–528
Keyes GW, Carr AJ, Miller RK, Goodfellow JW (1992) The radiographic classification of medial gonarthrosis. Correlation with operative methods in 200 knees. Acta Orthop Scand 63:497–501
Lee J, Robinson G, Finlay K et al (2006) Evaluation of the quadriceps tendon, patellar tendon, and collateral ligaments after total knee arthroplasty: appearances in the early postoperative period. Can Assoc Radiol J 57:291–298
Caumo F, Russo A, Faccioli N et al (2007) Autologous chondrocyte implantation: prospective MRI evaluation with clinical correlation. Radiol Med 112:722–731
Genovese E, Angeretti MG, Ronga M et al (2007) Follow-up of collagen meniscus implants by MRI. Radiol Med 112:1036–1048
Sofka CM, Potter HG, Figgie M, Laskin R (2003) Magnetic resonance imaging of total knee arthroplasty. Clin Orthop Relat Res 406:129–135
Naraghi AM, White LM (2006) Magnetic resonance imaging of joint replacements. Semin Musculoskelet Radiol 10:98–106
Olsen RV, Munk PL, Lee MJ et al (2000) Metal artifact reduction sequence: early clinical application. Radiographics 20:699–712
Viano AM, Gronemeyer SA, Haliloglu M, Hoffer FA (2000) Improved MR imaging for patients with metallic implants. Magn Reson Imaging 18:287–295
Guermazi A, Miaux Y, Zaim S et al (2003) Metallic artefacts in MR imaging: effects of main field orientation and strength. Clin Radiol 58:322–328
Lee MJ, Kim S, Lee SA et al (2007) Overcoming artifacts from metallic orthopedic implants at high-field-strength MR imaging and multidetector CT. Radiographics 27:791–803
Tarhan NC, Chung CB, Mohana-Borges AV et al (2004) Meniscal tears: role of axial MRI alone and in combination with other imaging planes. AJR Am J Roentgenol 183:9–15
Cittadini G, Cittadini Gjr, Sardanelli F (2008) La risonanza magnetica. In: Diagnostica per immagini e Radioterapia. Ecig, Genova, p 137
Vanhoenacker FM, Snoeckx A, Vandaele L et al (2005) Bone marrow changes in sports injuries. JBR-BTR 88:332–335
Genson CC, Blane CE, Helvie MA et al (2007) Effects on breast MRI of artifacts caused by metallic tissue marker clips. AJR Am J Roentgenol 188:372–376
Herold T, Caro WC, Heers G et al (2004) Influence of sequence type on the extent of the susceptibility artifact in MRI—a shoulder specimen study after suture anchor repair. Rofo 176:1296–1301
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Aliprandi, A., Perona, F., Bandirali, M. et al. MR imaging of the knee in patients with medial unicompartmental arthroplasty: comparison among sequences at 1.5 T. Radiol med 114, 301–311 (2009). https://doi.org/10.1007/s11547-008-0356-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11547-008-0356-4