
Abstract
Purpose
This study aimed to assess the usefulness of multiplanar reformations (MPR) during multidetector-row computed tomography (MDCT)-guided percutaneous needle biopsy of lung lesions difficult to access with the guidance of the native axial images alone owing to overlying bony structures, large vessels or pleural fissures.
Materials and methods
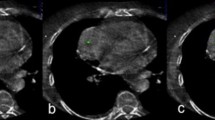
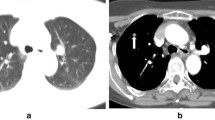
MDCT-guided transthoracic needle biopsy (TNB) was performed on 84 patients (55 men and 29 women; mean age 65 years) with suspected lung neoplasm by using a spiral MDCT scanner with the simultaneous acquisition of six slices per rotation. We determined the site of entry of the 22-gauge Chiba needle on native axial images and coronal or sagittal MPR images. We took care to ensure the shortest needle path without overlying large vessels, main bronchi, pleural fissures or bony structures; access to the lung parenchyma as perpendicular as possible to the pleural plane; and sampling of highly attenuating areas of noncalcified tissue within the lesion.
Results
Diagnostic samples were obtained in 96% of cases. In 73 patients, lesions appeared as a solid noncalcified nodule <;2 cm; 11 lesions were mass-like. In 22, the biopsy required MPR guidance owing to overlying ribs (18), fissures (2) or hilar-mediastinal location (2).
Conclusions
MDCT MPR images allowed sampling of pulmonary lesions until now considered unreachable with axial MDCT guidance because of overlying bony structures (ribs, sternum and scapulae) or critical location (hilar-mediastinal, proximity to the heart or large vessels). Compared with the conventional procedure, the use of MPR images does not increase the rate of pneumothorax or the procedure time.
Riassunto
Obiettivo
Valutare l’utilità delle immagini multiplanar reformations (MPR), durante agobiopsia percutanea TC spirale multidetettore (TCMD) guidata, nelle lesioni polmonari difficilmente raggiungibili con la sola guida delle immagini assiali, in quanto coperte da strutture scheletriche, grossi vasi o scissure pleuriche.
Materiali e metodi
Eseguita agobiopsia transtoracica (TNB, transthoracic needle biopsy) TCMD-guidata in 84 pazienti (55 maschi e 29 femmine, età media 65 anni) con lesione polmonare sospetta per neoplasia. Impiegato scanner TCMD a scansione elicoidale, con acquisizione simultanea di sei strati per ogni rotazione completa. Sulla base di immagini assiali native ed MPR sagittali o coronali è stato introdotto un ago “Chiba Point” centimetrato da 22 gauge (G) scegliendo: il tragitto più breve in cui non si sovrappongano grossi vasi, bronchi principali e lobari, scissure pleuriche e strutture scheletriche; ingresso nel parenchima polmonare il più perpendicolare possibile al piano pleurico; le zone di tessuto non calcifico più dense della lesione da sottoporre a biopsia.
Risultati
Nel 96% dei casi si è ottenuto un prelievo diagnostico. In 73 pazienti le lesioni sottoposte ad agobiopsia avevano caratteristiche di nodulo solido non calcifico di dimensioni inferiori ai 2 cm; 11 lesioni erano masse neoplastiche. In ventidue noduli è stato necessaria la guida bioptica con immagini MPR in quanto lesioni “coperte” da coste (18 noduli), da scissure (2 noduli) o a localizzazione ilo-mediastinica (2 noduli).
Conclusioni
Le immagini MPR ottenute con TCMD hanno permesso di raggiungere lesioni polmonari considerate un tempo inaccessibili con la sola guida delle immagini TCMD assiali. L’impiego della immagini MPR, inoltre, non incrementa, rispetto alla procedura convenzionale né i casi di pneumotorace (PNX) né il tempo di esecuzione del prelievo.
Article PDF
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
References/Bibliografia
Manhire A, Charig M, Clelland C et al (2003) BTS Guidelines. Guidelines for radiologically guided lung biopsy. Thorax 58:920–937
Ernst A, Silvestri A, Johnstone D (2003) Guidelines from the ACCP Interventional pulmonary procedures. Chest 123:1693–1717
Tan BB, Flaherty KR, Kazerooni EA, Iannettoni MD (2003) American College of Chest Physicians. The solitary nodule. Chest 123 [Suppl 1]:89S–96S
Schreiber G, McCrory D (2003) Performance characteristics of different modalities for diagnosis of suspected lung cancer: Summary of published evidence. Chest 123:115S–128S
Wallace MJ, Krishnamurthy S, Broemeling LD et al (2002) CT-guided percutaneous fine needle aspiration biopsy of small (<;or=1cm) pulmonary lesions. Radiology 225:823–828
Haaga JR, Alfidi RJ (1976) Precise biopsy localization by computer tomography. Radiology 118:603–607
Lacasse Y, Wong E, Guyatt GH, Cook DJ (1999) Transthoracic needle aspiration biopsy for diagnosis of localised pulmonary lesions: a metaanalysis. Thorax 54:884–893
Kim JH, Kim YT, Lim HK et al (2003) Management for chest wall implantation of non-small cell lung cancer after fine needle aspiration biopsy. Eur J Cardiothorac Surg 23:828–832
Ohno Y, Hatabu H, Takenaka D et al (2003) CT-guided transthoracic needle aspiration biopsy of small (<; or = 20mm) solitary pulmonary nodules. AJR Am J Roentgenol 180:1665–1669
Wescott JL, Rao N, Colley DP (1997) Transthoracic needle biopsy of small pulmonary nodules. Radiology 202:97–103
Gupta S, Krishnamurthy S, Broemeling LD et al (2005) Small (<;or=2cm) subpleural pulmonary lesions: shortversus long-needle-path CT-guided biopsy. Comparison of diagnostic yield and complications. Radiology 234:631–637
Dalquen P, Oberholzer M (1979) Lung biopsy: methods value, complications, timing and indications. Pathol Res Pract 164:95–103
Herman PG, Hessel SJ (1977) The diagnostic accuracy and complications of closed lung biopsies. Radiology 25:11–14
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
De Filippo, M., Onniboni, M., Rusca, M. et al. Advantages of multidetector-row CT with multiplanar reformation in guiding percutaneous lung biopsies. Radiol med 113, 945–953 (2008). https://doi.org/10.1007/s11547-008-0325-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11547-008-0325-y