
Abstract
Clinical studies showed that only 10% of patients with metastatic colorectal cancer (mCRC) respond to treatment with the anti-epidermal growth factor receptor (EGFR) monoclonal antibodies panitumumab or cetuximab, regardless of the line of treatment. The current tool used to select patients, i.e. immunohistochemistry (IHC) evaluation of EGFR expression by EGFR pharmDx™ Kit, is not reliable in predicting response. Retrospective analyses of factors such as increased EGFR gene copy number and KRAS and/or BRAF mutations showed that such molecular changes could affect clinical benefit from anti-EGFR monoclonal antibodies. We report here the case of a 66-year-old man with chemorefractory mCRC, considered not eligible to salvage treatment with the anti-EGFR monoclonal antibody cetuximab and irinotecan because the primary adenocarcinoma of the rectum was found not expressing EGFR protein by IHC. However, FISH analysis of EGFR gene copy number and evaluation of KRAS and/or BRAF specific mutations by gene sequencing showed characteristics associated with favourable clinical outcome to anti-EGFR therapy. Based on the EGFR protein expression by IHC in a liver metastasis, the patient was then treated with cetuximab plus irinotecan, obtaining symptoms improvement and a dramatic objective tumor response in all sites of disease, lasting 4.2 months. We also discuss literature findings about the role of different biological characteristics in predicting clinical benefit from anti-EGFR therapy in patients with mCRC.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Case report
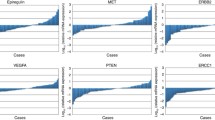
A 66-year-old man with metastatic colorectal cancer (mCRC) in progressive disease after fluoropyrimidine-, irinotecan-, oxaliplatin-, and mytomiycin-containing regimens was initially considered not eligible for salvage treatment with the anti-epidermal growth factor receptor (EGFR) monoclonal antibody (moAb) cetuximab and irinotecan because the primary adenocarcinoma of the rectum was found not to express EGFR protein by immunohistochemistry (IHC; Fig. 1a) [1]. Given that discrepancies between EGFR expression in primary versus metastatic sites can occur in the same patient [2], subsequent evaluation of specimens from liver and abdominal metastases were performed, showing 5% EGFR-positive cells by IHC exclusively in liver metastases (Fig. 1c). Intriguingly, fluorescence-in situ-hybridization (FISH) analysis detected an EGFR gene increased copy number, consisting in a chromosome 7 polysomy in >90% of cells, both in primary and in metastatic sites, with a mean EGFR gene/cell of 3.88 in the primary tumor, 3.64 in liver metastasis and 3.43 in soft tissue metastasis (Fig. 1b,d, and f). Evaluation of specific KRAS (exon 2) and BRAF (exons 15 and 21) mutations, known to be associated with the lack of response [3, 4], showed a wild-type pattern of the genes. Based on the EGFR protein expression by IHC in liver metastases, allowing reimbursement of cetuximab, the patient was then treated with standard doses and schedule of cetuximab plus irinotecan [1], obtaining symptom improvement and a dramatic objective tumor response in all sites of disease, lasting 4.2 months (Fig. 2).

Immunohistochemistry (IHC) and fluorescence-in situ-hybridization (FISH) of EGFR in the primary tumor and metastases of present case report. IHC demonstrated lack of expression in primary tumor (a) and soft tissue metastases (e), with a focal expression in liver metastasis (c). Conversely, an EGFR gene increased copy number was detected by FISH in primary tumor (b), liver (d) and soft tissue (f) metastases, all sites presenting with a diffuse chromosome 7 polysomy

CT-scan images showing the dramatic response achieved by the patient after 8 weeks of treatment with anti-EGFR therapy in lung metastasis (a before and b after treatment) and hilar lymph nodes (c before and d after treatment), with a subtotal resolution of actelectasis
Discussion
This case report is paradigmatic of the role of various mCRC biological characteristics in predicting response to anti-EGFR moAbs. First of all, we observed an objective response despite the lack of EGFR expression in primary tumor and a low degree of expression in the liver metastasis. This confirms the poor value of IHC in predicting clinical outcome to anti-EGFR moAbs [1, 5–7]. As previously described [2], a difference in EGFR protein expression between the primary tumor and related metastatic sites has been found in specimens from the same patient. Thus, even though EGFR tumor expression is mandatory to treat mCRC patients with cetuximab as per the label registration in the European Union [1], the use of such criterion to select patients for treatment is now resulting in a high number of patients submitted to therapy without clinical benefit and in the exclusion from treatment of potentially responsive patients. Conversely, it was recently demonstrated that the evaluation of EGFR gene copy number (GCN) by FISH, as well as of KRAS and/or BRAF specific mutations by gene sequencing, represents an effective tool in selecting patients who are likely to benefit from anti-EGFR moAbs.
Our group initially showed, in a cohort study, that in mCRC increased EGFR GCN relates to propensity to respond to the anti-EGFR antibodies cetuximab and panitumumab [8]. Recently, in a more homogenous series of patients receiving panitumumab as single agent, we stressed the role of non-increased EGFR GCN status as a negative predictive factor of clinical benefit. Patients with tumors harboring a normal disomic EGFR gene pattern are unlikely to respond to therapy and have a worse time-to-progression and overall survival than patients with tumors with an increased GCN. In the latter patient population, a 30% objective response is obtained, which is three percentage points higher than in the unselected population [9]. A correlation between EGFR gene pattern and clinical outcome to anti-EGFR therapy was recently confirmed [10–12] using FISH analysis, even though methods of tissue processing and EGFR GCN scoring systems were not homogeneous in the different studies. However, in all cases quantitative PCR analysis of EGFR GCN proved ineffective to demonstrate a correlation between increased GCN and clinical outcome to anti-EGFR moAbs [8, 13, 14], probably due to tumor DNA dilution by normal cells during DNA extraction. As a matter of fact, CRC rarely presents with high polysomy or amplification of EGFR gene and, even in the case of an increased GCN, in most cases the EGFR gene/cell ratio is not much higher than in normal tissue to be detected by quantitative PCR. Thus, in our opinion, it is indispensable to standardize tissue processing methods and optimize criteria for EGFR signal evaluation in order to bring EGFR FISH analysis into clinical practice.
As far as KRAS and/or BRAF are concerned, the role of specific gene mutations as predictors of resistance to the anti-EGFR moAbs cetuximab and panitumumab has been widely described [3, 4, 10, 13, 15–17], showing a significant clinical benefit in terms of time-to-progression and overall survival in patients with tumors harboring wild-type KRAS and/or BRAF [4]. In these cases, resistance is due to the constitutive activation of the signaling pathways downstream of the receptor by oncogene mutations. Based on the presence of a non-mutated KRAS, the fully human anti-EGFR moAb panitumumab recently received a positive opinion for marketing authorization in the European Union in patients with mCRC (http://www.emea.europa.eu/pdfs/human/opinion/40511307en.pdf). As shown by the dramatic objective tumor response to cetuximab, in our case report tumor growth was mainly driven by the EGFR pathway, and this biological characteristic was evoked by an increase in EGFR gene copy number rather than by IHC findings. Then, the presence of a wild-type genotype for KRAS and BRAF excluded the downstream activation of EGF signaling by specific activating mutations of these genes associated with resistance to anti-EGFR moAbs [3, 4]. Prospective evaluation of factors such as EGFR gene copy number and KRAS and/or BRAF mutations could provide, in a near future, a better understanding of the molecular pathways that could be fruitfully exploited in mCRC patients. As a result, the risk of ineffective therapy with undesired side effects could decrease, possibly with financial savings for healthcare systems [18].
References
Cunningham D, Humblet Y, Siena S et al (2004) Cetuximab monotherapy and cetuximab plus irinotecan in irinotecan-refractory metastatic colorectal cancer. N Engl J Med 351:337–345
Scartozzi M, Bearzi I, Beardi R, Mandolesi A, Fabris G, Cascinu S (2004) Epidermal growth factor receptor (EGFR) status in primary colorectal tumor does not correlate with EGFR expression in related metastatic sites: implication for treatment with EGFR-targeted monoclonal antibodies. J Clin Oncol 22:4772–4778
Lievre A, Bachet JB, Le Corre D et al (2006) KRAS mutation status is predictive of response to cetuximab therapy in colorectal cancer. Cancer Res 66:3992–3995
Benvenuti S, Sartore-Bianchi A, Di Nicolantonio F et al (2007) Oncogenic activation of the RAS-RAF signaling pathway impairs the response of metastatic colorectal cancers to anti EGFR antibody therapies. Cancer Res 67:2643–2648
Van Cutsem E, Peeters M, Siena S et al (2007) Open-label phase III trial of panitumumab plus best supportive care compared with best supportive care alone in patients with chemotherapy-refractory metastatic colorectal cancer. J Clin Oncol 25:1658–1664
Chung KY, Shia J, Kemeny NE et al (2005) Cetuximab shows activity in colorectal cancer patients with tumors that do not express the epidermal growth factor receptor by immunohistochemistry. J Clin Oncol 23:1803–1810
Pippas AW, Lenz HJ, Mayer RJ, Mirtsching B, Cohn AL, Windt P, Van Cutsem E (2005) Analysis of EGFR status in metastatic colorectal cancer patients treated with cetuximab monotherapy. J Clin Oncol 23 (Proc ASCO 2005): Abstract 3595
Moroni M, Veronese S, Benvenuti S et al (2005) Gene copy number for epidermal growth factor receptor (EGFR) and clinical response to antiEGFR treatment in colorectal cancer: a cohort study. Lancet Oncol 6:279–286
Sartore-Bianchi A, Moroni M, Veronese S et al (2007) Epidermal growth factor receptor gene copy number and clinical outcome of metastatic colorectal cancer treated with panitumumab. J Clin Oncol 25:3238–3245
Frattini M, Saletti P, Romagnani E et al (2007) PTEN loss of expression predicts cetuximab efficacy in metastatic colorectal cancer patients. Br J Cancer 97:1139–1145
Cappuzzo F, Finocchiaro G, Rossi E et al (2007) EGFR FISH assay predicts for response to cetuximab in chemotherapy refractory colorectal cancer patients. Ann Oncol (in press), DOI 10.1093/annonc/mdm492
Gravalos C, Sastre J, Aranda E et al (2007) Analysis of potential predictive factors of clinical benefit in patients (pts) with metastatic colorectal cancer (mCRC) treated with single-agent cetuximab as first-line treatment. J Clin Oncol 25 (Proc ASCO 2007): Abstract 4120
Khambata-Ford S, Garrett CR, Meropol NJ et al (2007) Expression of epiregulin and amphiregulin and K-ras mutation status predict disease control in metastatic colorectal cancer patients treated with cetuximab. J Clin Oncol 25:3230–3237
Lenz HJ, Van Cutsem E, Khambata-Ford S et al (2006) Multicenter phase II and translational study of cetuximab in metastatic colorectal carcinoma refractory to irinotecan, oxaliplatin, and fluoropyrimidines. J Clin Oncol 24:4914–1421
Finocchiaro G, Cappuzzo F, Jänne PA et al (2007) EGFR, HER2 and Kras as predictive factors for cetuximab sensitivity in colorectal cancer. J Clin Oncol 25 (Proc ASCO 2007): Abstract 4021
Di Fiore F, Blanchard F, Charbonnier F et al (2007) Clinical relevance of KRAS mutation detection in metastatic colorectal cancer treated by cetuximab plus chemotherapy. Br J Cancer 96:1166–1169
De Roock W, De Schutter J, De Hertogh G et al (2007) KRAS mutations preclude tumor shrinkage of colorectal cancers treated with cetuximab. J Clin Oncol 25 (Proc ASCO 2007): Abstract 4132
Schrag D (2004) The price tag on progress—chemotherapy for colorectal cancer. N Engl J Med 351:317–319
Conflict of interest statement
No funds or benefits in any form have been or will be received from a commercial party related directly or indirectly to the subject of this article.
Author information
Authors and Affiliations
Corresponding author
Additional information
Supported by research grants from Associazione Italiana Ricerca Cancro (AIRC) and Oncologia Ca’ Granda ONLUS Fondazione.
Rights and permissions
About this article
Cite this article
Moroni, M., Veronese, S., Sartore-Bianchi, A. et al. Controversial evaluation of EGFR protein and gene status in predicting response to anti-EGFR monoclonal antibodies in metastatic colorectal cancer: a case report and review of the literature. Targ Oncol 3, 127–130 (2008). https://doi.org/10.1007/s11523-008-0073-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11523-008-0073-x