
Abstract
In multi-body models of scoliotic spine, personalization of mechanical properties of joints significantly improves reconstruction of the spine shape. In personalization methods based on lateral bending test, simulation of bending positions is an essential step. To simulate, a force is exerted on the spine model in the erect position. The line of action of the force affects the moment of the force about the joints and thus, if not correctly identified, causes over/underestimation of mechanical properties. Therefore, we aimed to identify the line of action, which has got little attention in previous studies. An in-depth analysis was performed on the scoliotic spine movement from the erect to four spine positions in the frontal plane by using pre-operative X-rays of 18 adolescent idiopathic scoliosis (AIS) patients. To study the movement, the spine curvature was considered as a 2D chain of micro-scale motion segments (MMSs) comprising rigid links and 1-degree-of-freedom (DOF) rotary joints. It was found that two MMSs representing the inflection points of the erect spine had almost no rotation (0.0028° ± 0.0021°) in the movement. The small rotation can be justified by weak moment of the force about these MMSs due to very small moment arm. Therefore, in the frontal plane, the line of action of the force to simulate the left/right bending position was defined as the line that passes through these MMSs in the left/right bending position. Through personalization of a 3D spine model for our patients, we demonstrated that our line of action could result in good estimates of the spine shape in the bending positions and other positions not included in the personalization, supporting our proposed line of action.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
Multi-body models of scoliotic spine have gained increasing importance in surgical planning [19] because they can provide surgeons with predictive information about the surgery outcome [13]. As correction of the spine shape is a key factor in the surgery [10], before the models become reliable tools for prediction of the surgery outcome, it is important that the models accurately reconstruct the spine shape in the spine positions, e.g. by placing the vertebrae at their respective locations [15]. Personalization of mechanical properties of the joints in the spine models is an important task in improving the accuracy of the models to place the vertebrae at their respective locations along the spine and thus to reconstruct the spine shape [1, 12, 14]. The mechanical properties of the joints are typically defined by stiffness matrices pioneered by Panjabi [23]. Petit et al. [26] were the first to pave the way for developing a method to personalize the stiffness coefficients, and as a result, provided an important insight that such a personalization could improve the prediction error of Ferguson angle (a key parameter to define the scoliotic spine shape) up to 50 %.
Personalization of the stiffness matrices has been widely done by using Petit et al.’s method [3, 9]. The method is based on lateral bending test in the frontal plane. In this method, a force is exerted on the uppermost vertebra of the spine model in the erect position to simulate the spine in the lateral bending positions. The magnitude of the force is increased until the amplitudeFootnote 1 of the bending is reproduced. The stiffness coefficients are then adjusted to minimize the discrepancy between the Ferguson angles measured on the simulated bending and X-rays. Simulation of the bending positions is an essential step in this personalization method. The way of exerting the force on the model is influential to the adjusted stiffness coefficients. Line of action of the force is one of the critical factors in setting the stiffness coefficients. The line of action affects the moment of the force about the axis of rotation of the joints because it determines the moment arm that is the distance between the line of action and the axis of rotation (Fig. 1). If the line of action is not correctly found, the moment arms become larger/smaller than the actual ones. The larger (smaller) arm leads to overestimation (underestimation) of the stiffness coefficients. For instance, considering the equilibrium equation of the moment (i.e. k·Δθ = d·F), for a known rotation (Δθ) of a joint from the erect to a bending position and a known force (F), the stiffness coefficient (k) is overestimated if the moment arm (d) is larger than the actual arm. In a functional spinal unit, the joint with overestimated (underestimated) stiffness coefficients causes the superior vertebra to make smaller (larger) displacements than the actual ones with respect to the inferior vertebra, affecting the reconstructed spine shape.

Effects of the line of action on the moment arm causing to over/underestimation of stiffness coefficients
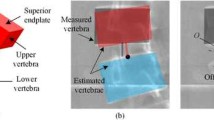
In Petit et al.’s method, the line of action is parallel to the line (iliac line) drawn through the superior tips of the left and right iliac crests in the frontal plane. The force with such a line of action causes the vertebrae to move towards the direction of the bending movement in relation to their inferior vertebrae (Fig. 1). However, in a scoliotic spine, due to the deformity, there is a possibility that a number of the vertebrae move in the opposite direction; an exampleFootnote 2 of a real situation is shared in Fig. 2a. To specify the movement direction of the vertebrae, the relative location of the centreFootnote 3 of the superior (blue, red, and black circles) and inferior (white circles) endplates of the vertebrae is measured on the X-rays of the erect and lateral bending positions (Fig. 2b). The impact of the force (i.e. F and moment τ) with the line of action parallel to the iliac line at the upper centre (black circle) may cause the vertebra to move towards opposite of its actual movement direction. The number of vertebrae with such an opposite movement direction can be large (4 ± 1 out of 14 vertebrae from L4 to T2 [17]), affecting the reconstructed spine shape in the simulated bending.

a Centre of endplates of the vertebrae of a functional spinal unit marked on X-rays of the left bending, erect, and right bending positions of a scoliotic spine and b relative location of the centres and effects of the force to move the centre from its location in the erect position (black circle) to its location in the left/right bending position (blue/red circle) (colour figure online)
Overall, for the purpose of reconstruction of more accurate spine shapes, there is a need to find a better line of action to simulate the bending positions in the personalization. However, to the best of our knowledge, little mention has been made with regard to addressing this need in the existing literature. Therefore, this paper presents a preliminary study on such a line of action and focuses on the frontal plane. The criteria for assessing the performance of the line of action are defined based on the spine shape in the frontal plane; estimation errors of Ferguson angles and locations of the vertebrae measured on the simulated spine positions and their respective X-rays. This study focuses on AIS patients who require surgical treatment to correct the deformity. AIS affects 2–3 % of adolescents and its aetiology is unknown [4]. Besides, it predominantly occurs in females [19].
2 Methods
As force is the cause of movement, we study the spine movement from the erectFootnote 4 to several spine positions to find the line of action of the force. We focus on the frontal plane because firstly, X-rays that are the gold standard to measure the spine geometry [24, 30] are routinely available for several positions in this plane according to scoliosis standard care. Secondly, we adopt Petit et al.’s personalization method that adjusts the stiffness coefficients relating to the lateral rotation of the vertebrae with respect to their inferior vertebra, implying the importance of finding the line of action in the frontal plane. The movement is studied from the erect to four spine positions (left bending, right bending, neutral, and traction). It should be noted that involving the extra two positions (i.e. neutral and traction) in the study helps us to identify a better line of action because it is a critical factor in simulation of not only the lateral bending positions for the personalization but also other spine positions for applications of scoliotic spine models.
Two approaches of multi-body modelling of scoliotic spine are adopted in the present study, one to formulate and the other to test our concept regarding the line of action: (1) a 2D multi-body kinematic modelling [15] approach to conduct an in-depth study on the spine movement by using X-rays for the concept formulation and (2) an existing 3D multi-body modelling approach to test the concept since 3D models are dominant in scoliotic spine multi-body modelling. The 2D model is a chain of micro-scale motion segments (MMS) comprising rotary joints and links. The chain lays on the spine curvatures and gives the angles of the rotary joints to define the spine positions. Thus, the spine movement from a position to another one is defined by the differences between the angles of the joints in the positions. The 3D model is closest in similarity to the model in Petit et al.’s [26] study. The initial 3D geometry of the model was personalized to the patients by using 2D X-rays according to 3D reconstruction method of Cheriet et al.’s [5]. Vertebrae were considered as rigid bodies [1, 29]. The intervertebral discs were defined as spherical joints allowing 3-DOF in rotation [6]. The joints constrained all the relative translations between the vertebrae in a functional spinal unit. They were placed at the posterior extremity of the superior endplate of each vertebra [25]. A linear torsion spring was incorporated into each DOF of the joints [22, 23].
2.1 Subjects and data collection
The current study has been approved by the domain-specific review board (DSRB) and ethics committee. All patients involved in this study had been properly consulted, and their approval and informed consents were obtained. Following the DSRB approval and obtaining the proper informed consents, pre-operative digital X-rays of a cohort of 18 patients with AIS were used for the study (Table 1). The X-rays were taken in five posterior–anterior positions in the frontal plane; one erect position and four prone positions (left bending, right bending, neutral, and traction). The patients had no neurological deterioration, and they were admitted to hospital for surgical treatment. There were 12 female and six male patients between the ages of 12 and 19 years (mean age of 15 years). Cobb angle of the main curves ranged from 46° to 86°, and the average and median Cobb angles were 56° and 53°, respectively.
The digital X-rays were analysed to measure the location (LOC) and orientation (Θ) of the vertebrae from L4 to T2 to obtain the spine curvatures in the five positions. The X-rays had pixels with size of 0.1 × 0.1 mm2. L5 and T1 were not considered since the X-rays obtained at these vertebrae were often suboptimal for measurement of LOC and Θ.
LOC was defined as the location of the midpoint of the vertebral body in the frontal plane, white circle in Fig. 3. The midpoint is the intersection of the line drawn from the upper left corner to the lower right of the vertebral body and the line drawn from the upper right to the lower left of the vertebral body [20]. To find the midpoints, landmarks were manually selected at the four corners of the vertebral body. A landmark was a pixel of the X-rays. Θ was considered as the orientation of the line (Fig. 3) passing through the centre of the upper and lower endplates of the vertebra (in accordance with the definition of vertebral lateral rotation [28] provided by Scoliosis Research Society). For Θ, after localizing the midpoint, a line coincident with the midpoint is drawn on the X-ray. This line was manually rotated about the midpoint until it shows the orientation. The step of the rotation was 0.1°, e.g. the immediate smaller and larger angles than 15° were 14.9° and 15.1°, respectively.

Description of the geometry of the scoliotic spine in the frontal plane; the global coordinate system, and the location and orientation of a vertebra
LOC and Θ were defined in the global coordinate system (G in Fig. 3) represented by XYZ on L4. G has its origin at the midpoint of L4. X- and Y-axes define the anterior and left directions. Z-axis is parallel to the line that shows the orientation of L4 (Θ of L4 is 0). The plane YZ is the frontal plane, and LOC is given by the ordered pair of (Y, Z). MATLAB R2013b version 8.2.0.701 (MathWorks, Natick, MA, USA) was used for the analysis of the X-rays.
2.2 Intra- and inter-observer repeatability and reliability of the measurements
Two experts familiar with X-rays of the spine performed the measurements of LOC and Θ three times. Then, the mean values of the measurements were considered. All the measurements were supervised by G. Liu (one of the authors) who is an experienced scoliosis surgeon at National University Hospital, Singapore. The intra- and inter-observer reliabilities of the measurements were evaluated by using Pearson correlation analysis. The intra-observer reliabilities of the measurements were 0.95 ± 0.03 for expert one and 0.92 ± 0.02 for expert two. The inter-observer coefficient was 0.90. These agreements are excellent according to [7] and demonstrate the repeatability and reliability of the measurements.
2.3 Representation of the spine curvatures
Scoliotic spine curvature in the frontal plane is the curved line that passes through LOC of the vertebrae [28] (in the rest of the paper, the term ‘curvature’ refers to the spine curvature in the frontal plane). Polynomials are used to define the curvatures [18] and are fitted to LOC and Θ by using the linear least squares method; detailed description is provided in our previous work [15]. The order of each polynomial is adjusted in order to find the best fitting, i.e. the least root mean square error of LOC and Θ, which were 0.19 ± 0.08 mm and 0.17° ± 0.07°, respectively. These small errors show that the fitted polynomials are good estimates of the curvatures.
By employing the 2D modelling approach, the curvature is considered as a chain of MMSs (Fig. 4). An MMS consists of a rigid link and a 1-DOF rotary joint. The links of MMSs are equal in length. The chain is constrained at the first MMS attached to the midpoint of L4 and cannot translate with respect to this midpoint. The last MMS corresponds to the midpoint of T2. Denavit–Hartenberg convention [8] is adopted to represent the chain of MMSs. To reconstruct the spine curvature in a certain position, the angle (θ) of the rotary joints of all MMSs must be identified according to Denavit–Hartenberg convention. θ of an MMS is defined with respect to X-axis attached to its inferior MMS (Fig. 4).

Configuration of the chain of MMSs and the coordinate systems to represent the chain according to Denavit–Hartenberg convention
The chain is fully characterized to a given patient by specification of the number of MMSs (n) and the length of their links (l). To find n and l, the linear programing problem (or simply the minimization problem) in (1) is defined [15]. The minimization problem identifies l so that a chain with n MMSs can estimate the length of the spine curvatures in the five positions.
To solve (1), first, an l is considered, and then, n is obtained for the curvatures in the five positions, i.e. n 0, n 1, n 2, n 3, and n 4 for the erect, left bending, right bending, neutral, and traction positions, respectively. n i is obtained by laying MMSs with the length of l on the curvatures in position i. The minimization problem sets l so that the difference between n i and n 0 is minimum. The number of MMSs in the erect position (n 0) is considered as n for the chain. For the patients of this study, n and l were 998 ± 3 and 0.39 ± 0.05 mm, respectively. After solving the minimization problem, MMSs nearest (in terms of Euclidian distance) to the inflection points of the spine curvature in the erect position are labelled by INF. The inflection point is the point where the curvature changes direction from convex to concave and vice versa.
3 Results
3.1 Formulation of the concept
Amount of rotation (r) of MMSs from the erect to a position P was obtained as the absolute difference between θ of MMSs in the erect and P, i.e. r P = |θ erect − θ P | where, |·| denotes the absolute operation. r of all MMSs for the four positions was 0.0418° ± 0.0353°. The lower and upper 95 % confidence intervals (CI) of the mean of r were 0.0415° and 0.0421°, respectively. It was found that for each spine curvature, there were two MMSs with a locally least r (Fig. 5); these MMSs are called MMSLeast. The lower MMSLeast was in the thoracolumbar region between midpoints of L2 and T9, and the upper one was in the thoracic region between midpoints of T7 and T4. In total, there were 144 MMSLeast. Footnote 5 r of these MMSs was 0.0019° ± 0.0016°, which is 96 % smaller than the mean r of all MMSs. Such small amounts of rotation show that MMSLeast have almost no rotation when the spine moves from the erect to the four positions.

Amount of rotation of MMSs of the chain from the erect to the four positions for one of the scoliotic patients
It was found that in a region, MMSLeast were within the distance of 0–2 segments from INF (Fig. 6a). In 20 % of the cases, these MMSs were INFs. Around 62 and 18 % of MMSLeast were one and two segments above/below the INFs, respectively. The Euclidian distance between MMSLeast and INFs was 0.36 ± 0.24 mm. Such a short distance shows that the location of INFs is a good estimate of that of MMSLeast. In addition, r of INFs was 0.0028° ± 0.0021° (Fig. 6b), which is 93 % smaller than the mean r of all MMSs, showing small amounts of rotation for INFs. Such a small r of INFs shows that INFs had no significant rotation. Overall, according to the locations and amounts of rotation of INFs, it can be concluded that INFs identified in the erect position can estimate MMSs with the least r in the four positions.

a Location of INFs with respect to location of MMSLeast and b amount of rotation of INFs in the spine movement from the erect to the four positions for all the patients
The small amount of rotations of INFs (Fig. 6b) in the four positions can be due to the weak moments of the force (exerted on the spine to simulate the positions) about their rotary joints. According to the relationship between the force and moment (i.e. τ = d·F), these weak moments result from small moment arms because the force is typically strong to simulate the spine in the positions [22]. The small moment arms show that in a spine position, the line of action is very close to the axis of rotation of the rotary joints of INFs. Therefore, we introduce our concept of the line of action as follows: in the frontal plane, the line of action of the force to simulate the left/right bending position passes through INFs in the left/right bending position. An example of identifying the line of action is shown in Fig. 7. INFs are the ith and jth MMSs on the spine curvature in the erect position (Step 1). Thus, the line of action of the force to simulate position P passes through INFs on the spine in P (Step 2). A force with this line of action is exerted on T2 in the erect position to simulate P (Step 3).

Identification of the line of action of the force exerted on the spine model in the erect position to simulate position P
3.2 Proof of concept
We utilized Petit et al.’s method to personalize the 3D multi-body model of the scoliotic spine. Two personalized models (Model-1 and Model-2) were created for each patient: Model-1 by using our line of action and Model-2 by using the line of action parallel to the iliac line. To compare the performance of the lines of action, the accuracy of the personalized models in reconstruction of the spine shapes was tested by using estimation errors of Ferguson angles in three spine regions (thoracolumbar/lumbar, main thoracic, and proximal thoracic) and estimation errors of LOC. Simulation of the positions is done by fixing all DOFs of the lowest vertebra (L4) and by exerting a force on the uppermost vertebra (T2) until the amplitude (footnote 1 in Introduction) of the lateral bending was reproduced. The equilibrium equations (∑F = 0, ∑τ = 0) were solved since the spine was in static equilibrium (the spine elements were not moving) in the positions. Simulations were performed using Robotics Toolbox version 9.10 (released on February 24, 2015) in MATLAB R2013b version 8.2.0.701 (MathWorks, Natick, MA, USA).
Estimation errors of Ferguson angles were 1.34° ± 1.51° for Model-1 and 2.07° ± 2.20° for Model-2, showing 35 % smaller error when using the proposed line of action. For a more complete analysis of the accuracy of the models to estimate the spine shapes, estimation errors of LOC (E LOC) of the individual vertebrae were obtained (Fig. 8). E LOC was calculated as Euclidian distance between LOCs given by the models and those measured on the X-rays. E LOC of 504 vertebraeFootnote 6 were 0.51 ± 0.41 mm for Model-1 and 1.41 ± 1.09 mm for Model-2, showing 64 % smaller error by our line of action. According to the above results, we hypothesized that the mean value of errors of Ferguson angles by Model-1 was smaller than that by Model-2, and we also made the same hypothesis for E LOC. The null hypotheses (H0) stood for the difference in the other direction. Paired Student’s t test was adopted to test the hypotheses. For the confidence level of 0.05, strong evidence was found against the null hypotheses, showing that our line of action can result in more accurate estimates of Ferguson angles of each spine region and E LOC of each vertebra, p-values of 0.0005 and 0.0000, respectively. Overall, it can be concluded that the personalization using our line of action can result in better estimates of the spine shape in the bending positions.

Box charts of E LOC in the lateral bending positions
4 Discussion
Consideration of the spine curvature as a chain of micro-scale motion segments allowed us to perform a deep analysis of the spine movement. The analysis provided profound insight into the movement to formulate our concept of the line of action. It was shown that the spine model (Model-1) personalized by using the proposed line of action could make better estimates of the spine shape in the lateral bending positions than Model-2; reduction in E LOC by 0.90 mm. This reduction is important as it can have noticeable effects on how well the simulated spines fit a patient’s spine in a position. For example, Fig. 9 illustrates the simulated spines with about 0.90 mm difference in E LOC for the left bending position of one of our patients. As can be seen, this example shows that such an enhancement could be influential in fitting (i.e. the similarity between the spine curvatures) and estimating Ferguson angle (error of 0.85° vs. 4.28°). Therefore, our achievements in estimation of the locations of the vertebrae (0.90 mm less errors) can be noticeable. It should also be noted that the standard deviations of the estimation errors were also reduced by about three times, showing effective reduction in error of LOC (please see the box charts in Fig. 8). Therefore, our line of action can result in better estimates of the spine shape in the lateral bending positions.

Example of two simulations of a spine and their estimated Ferguson angles. The circles show LOC. The white and black circles represent the measured and simulated spines respectively. The simulated spine in the left side has about 0.90 mm smaller E LOC than the simulated spine in the right side
To further test our concept of the line of action, Model-1 was also utilized to simulate the other two spine positions (neutral and traction). The force with the proposed line of action was exerted on T2, and its magnitude was increased until the measured LOC of T2 was reproduced. The estimation errors of Ferguson angels and locations were 1.63° ± 1.98° and 0.78 ± 0.65 mm, respectively. These errors by Model-1 in the neutral and traction positions were smaller (21 and 45 % for Ferguson angles and locations, respectively) than the errors by Model-2 in the bending positions. Considering the errors of Model-2 as the small estimation errors, the errors of Model-1 in the neutral and traction positions are regarded small, showing that personalization by using our line of action could also result in good estimates of the spine shape in the positions not included in the personalization. This further supports our concept regarding the line of action.
Furthermore, as an observation, in 11 spine curvatures out of 72 (4 positions × 18 patients), our proposed line of action went through three points: two at INFs and one at another MMS in the lumbar region. Interestingly, similar to INFs, r of the extra MMSs (0.0020° ± 0.0015°) was almost the least in the lumbar region. This can reaffirm that the small r of MMSs can be due to the small moment arms about the joints of MMSs (Sect. 3.1), supporting our justification for formulation of the line of action.
We analysed amounts of rotation of the micro-scale motion segments in two more positions (neutral and traction positions) in addition to the lateral bending positions. This potentially helped us in formulating and supporting the proposed line of action. We initially considered several alternatives for estimation of the MMSs with the least r, e.g. the mean of MMSLeast (MMSMean) in the left and right bending positions for a spine region as a worth mentioning alternative. In a region, MMSMean is an MMS located between MMSLeast in the left bending and the one in the right bending. The distance between MMSMean and MMSLeast was calculated in terms of the number of segments (Fig. 10a), and r of MMSMean was also obtained (Fig. 10b) for the four positions. For both distance and r in the bending positions, there is no significant difference between the results of MMSMean and INFs (Table 2). In the neutral and traction positions, the results are better for INFs compared to those for MMSMean. Besides, the maximum distance for INFs did not exceed 2 segments, while for MMSMean, it increased to 3 segments. Through t-test, we found strong evidence that INFs were better than MMSMean to estimate MMSLeast in the neutral and traction positions (Table 2). Overall, it can be concluded that INFs can be good estimates of MMSLeast in all the four positions, whereas MMSMean may only give good estimates in the lateral bending positions. Therefore, INFs were chosen over MMSMean to formulate the concept of the line of action because the line of action is a critical factor not only in simulation of the lateral bending positions for the personalization but also in simulation of other spine positions for the applications of a scoliotic spine model in scoliosis treatment.

Estimation of MMSLeast by INF and MMSMean a estimation errors for the left and right bending positions and b estimation errors for the neutral and traction positions not included in the personalization
As the stiffness determines the displacement response to load, one factor that can show how well the stiffness is estimated is the spine shape. For this end, we studied the accuracy of the spine shape reconstructed by the personalized models; the more accurate shapes can imply the better estimates of the stiffness. As an example from our cohort of patients, Fig. 11 shows a spine in the right bending position. In the example, the magnitude of the force was increased from zero to reconstruct the measured spine shape. By referring to the spine with triangle symbols, the model first well reconstructed the lumbar spine, while the thoracic spine was not well estimated. This can imply that the model made larger displacements in the lumbar region due to the underestimated stiffness in this region, or it made smaller displacements in the thoracic region due to the overestimated stiffness in this region. By further increasing the force, the situation was reversed according to the spine with square symbols, i.e. the model well reconstructed the thoracic spine when it was bending more than the actual curve in the lumber region. These situations can show underestimation of the stiffness of the lumbar spine or overestimation of the stiffness of the thoracic spine.

An example of effects of over/underestimation of the stiffness coefficients on the reconstruction of the spine shapes. The symbols show LOC
The line of action was formulated by analysing the movement of 2D spine curvatures in the frontal plane, and then, as a limitation, the orientation of the line in the sagittal and transverse planes remains unknown. In this case, the force can cause the motions in the sagittal and transverse planes and also coupled motions between the planes that affect placing the vertebrae in 3D space, and accordingly, the spine shape in the frontal plane. Thus, error will be induced in the personalization so that the reconstructed spine shape in the frontal plane becomes similar to the X-rays. Finding the line of action in 3D space can be helpful to improve the accuracy of the personalization for achieving the better reconstructed 3D spine shape. X-rays of the lateral bending positions in the sagittal plane may be required to find the 3D line. However, these X-rays are not part of the scoliosis routine standard care. Finding the 3D line of action can be a significant challenge, and solving such challenge is demanded in scoliotic spine multi-body modelling. Another limitation in this study is that L5 and T1 were excluded from the characterization of the spine curvature. This can change the geometry of the spine curvatures and thus affect the identification of INFs. But, as INFs are typically located far from L5 and T1 (please see Sect. 3.1), the change in the geometry can be negligible around INFs. Therefore, the effects on the identification of INFs may not be significant. As another limitation, the majority of the patients in this study had curve types of 1, 2, and 3 according to Lenke classification [21], considering that these types affect around 75 % of the population of the scoliotic patients [27]. Involving more samples of the other curve types can help to better generalize the results.
5 Conclusion
This paper presented a preliminary study to identify the line of action of the force to simulate the lateral bending positions in the personalization based on the lateral bending test. We focused on identification of the line of action in the frontal plane. It was found that the line of action passes through two points on the spine curvature in the left/right bending position. The two points correspond to the inflection points of the spine curvature in the erect position. We showed that the spine model personalized by using our line of action could well reconstruct the spine shape in the lateral bending positions, supporting the proposed concept. Moreover, the model could also give good estimates of the spine shape in the neutral and traction positions not included in the personalization. This is a very important achievement because the line of action is a critical factor in simulation of not only the lateral bending positions for the personalization but also other spine positions for other applications of scoliotic spine models. This further supports our concept regarding the line of action.
Notes
The amplitude is measured on the X-rays. It is ‘the angle between the line drawn through the mid points of T1 and L5 and the normal to the line drawn through the superior tips of the left and right iliac crests’ [26].
The example is based on the measurements done on the X-rays of a scoliotic patient included in this study. The measurements and their accuracy and reliability are explained in Sect. 2.2.
144 MMSs = 1 MMS × 2 regions × 4 positions × 18 patients.
504 vertebrae = 14 vertebrae excluding L4 × 2 positions × 18 patients.
References
Abouhossein A, Weisse B, Ferguson SJ (2011) A multibody modelling approach to determine load sharing between passive elements of the lumbar spine. Comput Methods Biomech Biomed Eng 14:527–537
Aubin C-E, Petit Y, Stokes I, Poulin F, Gardner-Morse M, Labelle H (2003) Biomechanical modeling of posterior instrumentation of the scoliotic spine. Comput Methods Biomech Biomed Eng 6:27–32
Aubin CE, Labelle H, Chevrefils C, Desroches G, Clin J, Eng ABM (2008) Preoperative planning simulator for spinal deformity surgeries. Spine 33:2143–2152
Chalmers E, Westover L, Jacob J, Donauer A, Zhao V, Parent E, Moreau M, Mahood J, Hedden D, Lou EM (2015) Predicting success or failure of brace treatment for adolescents with idiopathic scoliosis. Med Biol Eng Comput 53:1001–1009. doi:10.1007/s11517-015-1306-7
Cheriet F, Dansereau J, Petit Y, Aubin C-E, Labelle H, De Guise JA (1999) Towards the self-calibration of a multiview radiographic imaging system for the 3D reconstruction of the human spine and rib cage. Int J Pattern Recognit Artif Intell 13:761–779
Christophy M, Senan NAF, Lotz JC, O’Reilly OM (2012) A musculoskeletal model for the lumbar spine. Biomech Model Mechanobiol 11:19–34
Colton T (1974) Statistics in medicine. Little, Brown, Boston 164
Denavit J (1955) A kinematic notation for lower-pair mechanisms based on matrices. Trans ASME J Appl Mech 22:215–221
Desroches G, Aubin C-E, Sucato DJ, Rivard C-H (2007) Simulation of an anterior spine instrumentation in adolescent idiopathic scoliosis using a flexible multi-body model. Med Biol Eng Comput 45:759–768
Duke K, Aubin C-E, Dansereau J, Labelle H (2005) Biomechanical simulations of scoliotic spine correction due to prone position and anaesthesia prior to surgical instrumentation. Clin Biomech 20:923–931
Gardner-Morse M, Stokes IA (1994) Three-dimensional simulations of the scoliosis derotation maneuver with Cotrel-Dubousset instrumentation. J Biomech 27:177–181
Huynh K, Gibson I, Jagdish B, Lu W (2015) Development and validation of a discretised multi-body spine model in LifeMOD for biodynamic behaviour simulation. Comput Methods Biomech Biomed Eng 18:175–184
Jalalian A, Gibson I, Tay EH (2013) Computational biomechanical modeling of scoliotic spine: challenges and opportunities. Spine Deformity 1:401–411
Jalalian A, Gibson I, Tay EH, Liu G (2014) A review of computer simulation of spine biomechanics for the treatment of scoliosis. In: The 5th TSME international conference on mechanical engineering, The Empress, Chiang Mai, Thailand, pp 17–19
Jalalian A, Tay EH, Arastehfar S, Liu G (accepted) A patient-specific multibody kinematic model for representation of the scoliotic spine movement in frontal plane of the human body. Multibody Syst Dyn
Jalalian A, Tay EH, Liu G (2016) Data mining in medicine: relationship of scoliotic spine curvature to the movement sequence of lateral bending positions. In: 15th Industrial conference on data mining ICDM 2016, New York, USA, 12–14 July 2016
Jalalian A, Tay EH, Liu G (2016) A hypothesis about line of action of the force exerted on spine based on lateral bending test in personalized scoliotic spine models. In: The Canadian Society for mechanical engineering international congress, Kelowna, BC, Canada, 26–29 June 2016
Kadoury S, Shen J, Parent S (2014) Global geometric torsion estimation in adolescent idiopathic scoliosis. Med Biol Eng Comput 52:309–319. doi:10.1007/s11517-013-1132-8
Keenan BE, Izatt MT, Askin GN, Labrom RD, Pettet GJ, Pearcy MJ, Adam CJ (2014) Segmental torso masses in adolescent idiopathic scoliosis. Clin Biomech 29:773–779
Lenke L (2000) SRS terminology committee and working group on spinal classification revised glossary of terms. http://www.srs.org/professionals/glossary/SRS_revised_glossary_of_terms.htm. Accessed 21 July 2015
Lenke LG, Betz RR, Harms J, Bridwell KH, Clements DH, Lowe TG, Blanke K (2001) Adolescent idiopathic scoliosis a new classification to determine extent of spinal arthrodesis. J Bone Joint Surg 83:1169–1181
Oxland TR, Lin RM, Panjabi MM (1992) Three-dimensional mechanical properties of the thoracolumbar junction. J Orthop Res 10:573–580
Panjabi MM, Brand RA Jr, White AA III (1976) Three-dimensional flexibility and stiffness properties of the human thoracic spine. J Biomech 9:185–192
Perret C, Poiraudeau S, Fermanian J, Revel M (2001) Pelvic mobility when bending forward in standing position: validity and reliability of 2 motion analysis devices. Arch Phys Med Rehabil 82:221–226
Petit Y, Aubin C-E, Labelle H (2004) Spinal shape changes resulting from scoliotic spine surgical instrumentation expressed as intervertebral rotations and centers of rotation. J Biomech 37:173–180
Petit Y, Aubin C, Labelle H (2004) Patient-specific mechanical properties of a flexible multi-body model of the scoliotic spine. Med Biol Eng Comput 42:55–60
Sponseller PD, Flynn JM, Newton PO, Marks MC, Bastrom TP, Petcharaporn M, McElroy MJ, Lonner BS, Betz RR, Group HS (2012) The association of patient characteristics and spinal curve parameters with Lenke classification types. Spine 37:1138–1141
Stokes IA (1994) Three-dimensional terminology of spinal deformity: a report presented to the Scoliosis Research Society by The Scoliosis Research Society Working Group on 3-D terminology of spinal deformity. Spine 19:236–248
Wagnac E, Arnoux P-J, Garo A, Aubin C-E (2012) Finite element analysis of the influence of loading rate on a model of the full lumbar spine under dynamic loading conditions. Med Biol Eng Comput 50:903–915. doi:10.1007/s11517-012-0908-6
Wong KW, Leong JC, M-k Chan, Luk KD, Lu WW (2004) The flexion–extension profile of lumbar spine in 100 healthy volunteers. Spine 29:1636–1641
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Jalalian, A., Tay, F.E., Arastehfar, S. et al. Finding line of action of the force exerted on erect spine based on lateral bending test in personalization of scoliotic spine models. Med Biol Eng Comput 55, 673–684 (2017). https://doi.org/10.1007/s11517-016-1550-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11517-016-1550-5