
Abstract
The potential of inertial measurement units (IMUs) for ergonomics applications appears promising. However, previous IMUs validation studies have been incomplete regarding aspects of joints analysed, complexity of movements and duration of trials. The objective was to determine the technological error and biomechanical model differences between IMUs and an optoelectronic system and evaluate the effect of task complexity and duration. Whole-body kinematics from 12 participants was recorded simultaneously with a full-body Xsens system where an Optotrak cluster was fixed on every IMU. Short functional movements and long manual material handling tasks were performed and joint angles were compared between the two systems. The differences attributed to the biomechanical model showed significantly greater (P ≤ .001) RMSE than the technological error. RMSE was systematically higher (P ≤ .001) for the long complex task with a mean on all joints of 2.8° compared to 1.2° during short functional movements. Definition of local coordinate systems based on anatomical landmarks or single posture was the most influent difference between the two systems. Additionally, IMUs accuracy was affected by the complexity and duration of the tasks. Nevertheless, technological error remained under 5° RMSE during handling tasks, which shows potential to track workers during their daily labour.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
1 Introduction
Motion analysis has been confined to laboratory settings for the most part. With the advancement of inertial measurement units (IMUs) over the last decade, in situ motion analysis appears promising for occupational biomechanics and other clinical or sports applications. Prior to testing IMUs directly on the field, validation of the technology against a reference remains important. A common approach is to use an optoelectronic system as a reference because of its established accuracy [12, 17, 19, 22, 27, 33].
As pointed out by Ferrari et al. [12], when comparing an inertial system to an optoelectronic system, it is important to distinguish the differences occurring from the technology to those coming from the models. A previous study compared directly joint angles from the MVN model in Xsens technology against a model respecting the ISB recommendations with an Optotrak system [33]. In this case, it becomes impossible to dissociate differences coming from orientation estimation to those coming from the distinct models which include different definitions of local coordinate systems and centre of rotation.
Previous validation studies of IMUs have been incomplete regarding aspects of complexity of movements, joints analysed, duration of trials, number and type of subjects. First, the movements analysed are often simple tasks of planar motion [9] or straight level walking [12, 20, 21, 33]. Walking remains fairly simple as no large range of motion is achieved and many joints are solicited only in one degree of freedom. In addition, a study showed that RMS errors increase between controlled pendulum trials and more complex motion of sweep, table wash and asymmetric lifting [14], suggesting an effect of task complexity on error measurement. Second, most studies analyse only a few joints typically either lower limbs [12, 20, 21, 33] or upper limbs [9, 11, 14, 34]. Third, the duration of the dynamic trials is typically under 1 min [4, 9, 14, 19]. This aspect is not representative of ergonomics applications, where motion analysis extends over long periods of time is not sufficient to analyse error due to signal drift. Fourth, the number of subjects involved in validation studies is often under five [12, 19, 21, 34]. Since anthropometry can play a large role in the accuracy of motion analysis [18], it seems important to test a sufficient number of subjects of various body dimensions. The main advantage of IMU relies in its portable technology for ergonomics, rehabilitation and sports applications. When validating prior to field testing, the subjects recruited should be similar to the forthcoming expected population.
In order to use IMUs for in situ occupational biomechanics, the technology must show a good response to aspects of duration and complex tasks on various subjects and on all joints. The main objective was to measure the error in whole-body joint angles obtained from the IMUs technology against an optoelectronic system as a reference. A specific objective was to distinguish the differences in joint angles attributed to the technology and those attributed to the biomechanical model. A first hypothesis was that the differences attributed to the biomechanical model will be larger than those attributed to the technology. In addition, a specific aim was to evaluate the effect of task complexity and duration on the technological error. The second hypothesis was that longer and more complex tasks will increase IMUs error.
2 Methods
2.1 Subjects
Twelve participants (9 men, 3 women, age of 26.3 ± 4.4 years, height of 171.4 ± 6.8 cm and weight of 74.4 ± 18.3 kg) completed a consent form prior to participation in the study approved by the Université de Sherbrooke Ethics Committee. Inclusion criteria were a good physical capacity according to the Physical Activity Readiness Questionnaire (PAR-Q) and no self-reported musculoskeletal disorders during the last year. Although not a strict inclusion criteria, we aimed at recruiting subjects differing in height and weight. Exclusion criterion was age over 60 years old.
2.2 Instrumentation
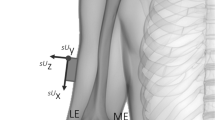
Whole-body kinematics was recorded at 30 Hz simultaneously with an eight-camera Optotrak system (Northern Digital Inc., Ontario, Canada) and a full-body Xsens system (MVN, Xsens technologies, Enschede, Netherlands). The systems were synchronised using MVN Studio 3.5 with a trigger signal coming from the Optotrak system. The Xsens system is composed of 17 IMUs over the feet, shanks, thighs, pelvis, sternum, head, scapulae, upper arms, forearms and hands (Fig. 1). The placement of the sensors intended to be over the bones and not the muscles to reduce soft tissues artefact [18]. For example, the shank sensors were placed on the proximal medial frontal aspect to adapt to the tibia geometry (Fig. 1). For every IMU sensor, a four-light-emitting diode Optotrak cluster was rigidly fixed on top with Velcro and tie wrap (Fig. 1). Optotrak wires were securely attached around the waist to ensure freedom of movement and reduce load on the limbs. The Xsens IMUs were connected between themselves and two XBus attached at the waist which transferred the data wirelessly.

Subject set-up with the 17 Xsens inertial measurement units (IMUs) and Optotrak marker clusters fixed on top of each IMU
3 Experimental protocol
Anthropometrics including height, shoe sole height, arm span, shoulder width, foot length, ankle height, knee height, hip height and hip width were gathered for every subject. These measures are input in the MVN model of Xsens to estimate segment lengths with regression equations [24]. Afterwards, anatomical landmarks respecting the International Society of Biomechanics (ISB) recommendations [30, 31] were identified with a probe from the Optotrak system during a standing static neutral position. The IMUs system was calibrated with a T-pose for the MVN model to establish a relation between sensor and segment orientation. The subjects were passively placed in the desired position, standing straight with arms abducted to 90° and elbows extended and palms facing the ground, by the investigator and were asked to maintain the position for a few seconds.
Series of three repetitions of simple short functional movements were performed by the subjects for each joint. Flexion/extension, abduction/adduction and internal/external rotation were performed separately for the head, trunk, upper arms and upper legs. Elbow flexion/extension and pronation/supination were executed. Wrist flexion/extension, lateral deviation and circumduction were performed. Knee flexion/extension was executed. Finally ankle flexion/extension, inversion/eversion and circumductions were performed.
A period of 32 min of manual material handling tasks was performed by the subjects similarly to a previous study [27]. The subjects were standing on a rectangular wooden platform (size 130 × 190 × 18 cm). At each corner was set up a different station where the first was a conveyor, the second a platform at 106 cm height, the third a platform at 34 cm height and the fourth a platform at 14 cm height (Fig. 2). Five empty boxes (size 26 × 33 × 34 cm, 500 g) were moved one at the time from a station to another. The trial started with the five boxes on the conveyor (station #1). The order of the displacements between each station was randomised. A light was attached to each station. After completion of the five boxes, the light indicated the next station to put the five boxes. Every 25 boxes, the subject paused in the middle of the wooden platform and maintained a static posture for 10 s. A pace was imposed with sounds indicating picking and depositing a box. The allotted time varied according to the distance between the stations, 3 s for the short side (between station #1 and #2 or #3 and #4), 4 s for the long side (between station #1 and #4 or #2 and #3) and 5 s for the diagonal (between station #1 and #3 or #2 and #4). Speed of execution was increased after half of the total 360 boxes. At the 181st box, pace increased to 125 % for the remainder of the trial. The allotted time was reduced to 2.4 s for the short side, 3.2 s for the long side and 4 s for the diagonal. The subjects had to respect the pace, but no instructions were given with regard to technique or handling of the boxes.

Schematic representation of the four stations during the manual material handling tasks
3.1 Biomechanical models
Two segmental biomechanical models were used in this study. The first model was based on anatomical landmarks as in the ISB recommendations [30, 31] and named the ISB model. Joint centres also respected the ISB recommendations. More specifically, the hip joint centre of rotation was calculated with a predictive approach relying on pelvic width, pelvic depth and leg length [15] as suggested in a systematic review [16]. The glenohumeral joint centre was determined functionally with arm flexion/extension, abduction/adduction and circumductions [13]. Finally, the cervical centre of rotation was estimated with a predictive approach using incisura jugularis and C7 anatomical landmarks [23]. Anatomical coordinate systems were built according to the same ISB guidelines. The shank coordinate system was built according to Zatiorsky [32] based on An and Chao method [1]. The second biomechanical model, MVN model, is provided by the Xsens IMUs system. The MVN model uses anthropometric measures to define segment lengths [24]. The calibration is executed during a specific static posture maintained by the subject where the relation between each IMU and segment orientation is established [24]. Since the MVN model separates the spine in multiple sections, the relative quaternion was used to calculate joint angles between the head orientation and thorax orientation for the neck joint and between the pelvis orientation and trunk orientation for the back joint.
3.2 Data analysis
To compare data from IMUs to the optoelectronic system, local coordinate systems of each segment must be aligned. A method relying on angular velocities was used during the simple short functional movements to align the local coordinate systems from the two systems [8]. In order to dissociate the differences attributed to the technology to those rising from the two biomechanical models, three comparisons were computed.
-
Comparison #1: Optotrak model ISB vs Xsens model ISB (error due to technology).
-
Comparison #2: Xsens model ISB vs Xsens model MVN (differences due to biomechanical model).
-
Comparison #3: Optotrak model ISB vs Xsens model MVN (total difference).
In comparison #1, the anatomical coordinate systems were defined according to the identified anatomical landmarks as in the ISB recommendations [30, 31] relative to the clusters fixed on each segment and will be referred to as the ISB model. The same transformation matrix was applied to the IMUs to orient the IMUs according to anatomical landmarks and the ISB model. Joint angles were calculated from the segment orientations following the Z–X–Y sequence of Euler angles with the exception of the shoulder using the X–Z–Y sequence as the Y–X–Y was not available in the MVN model and a few gimbal locks were experienced with the Z–X–Y sequence. Then, joint angles from the Optotrak system and from the IMUs system both using the same ISB model were compared to isolate the “technological error” component where the optoelectronic system acted as a reference. In comparison #2, joint angles were calculated only from the IMUs system, but with the ISB model (using the transformation matrix Opto-Xsens) and with the MVN model (Xsens built-in). Comparison #2 isolates the “model differences” component between ISB using anatomical landmarks and MVN using a specific static posture (T-pose) calibration. In comparison #3, the joint angles were compared between the optoelectronic system using anatomical landmarks (ISB model) and the IMUs using the MVN model. The third comparison evaluated the “total difference” when combining technology and biomechanical model components.
Joint angles for each comparison were assessed with descriptive statistics including root mean square error (RMSE), waveform distortion (WD) [20], coefficient of multiple correlation (CMC) [12] and Bland–Altman limits of agreement (LoA) [2]. Bilateral joint measures were pooled for all the measures as no apparent differences were observed between the right and left side [17]. The Box–Cox transformation was used on the RMSE values to improve normality of distribution and equality of variance according to Shapiro–Wilk and Levene’s tests, respectively. RMSE was used to conduct separate one-way repeated measures ANOVA applied on the eight joints and respective three Euler rotations to contrast the factor comparison (comparison #1, #2 and #3) during the manual material handling tasks. Bonferroni post hoc testing was conducted on the significant effects to identify where the differences occurred between the three comparisons. RMSE was used to conduct separate one-way repeated measures ANOVA applied on the eight joints and respective three rotations to contrast the factor task (simple short vs long complex) for comparison #1. The significance level was set a priori to α = .05 for all statistical analyses. Sphericity was verified with Mauchly’s test and when not met, the Huynh–Feldt correction was used.
4 Results
In general, measures of similarity (Table 1) indicated better agreement with regard to technology (comparison #1) than the biomechanical model (comparison #2). The results between comparison #2 and comparison #3 are closely related (Table 1). The technological error was generally below 5° of RMSE and WD, while CMC was mostly over 0.9 and the LoA bias was generally near 1° with coefficient of repeatability varying from 2.2° to 9.7°. The highest error in comparison #1 was observed on ankle internal/external rotation. The differences according to the biomechanical model were much higher than the technological error and were more contrasted by joints. The shoulder was showing the most differences with values reaching 41.3° of RMSE, 30.5° of WD, 0.35 of CMC and a LoA bias of 27.9° with coefficient of repeatability of 59.8°. Conversely, the ankle, knee and hip were the least affected joints by the model component with similarity values close to the technological error. Joint angles obtained from the two systems and the two biomechanical models during a representative portion of the manual material handling task for a typical subject were presented (Fig. 3).

Joint angles (degrees) obtained from the Optotrak model ISB in dotted black, Xsens model ISB in dashed pale grey and Xsens model MVN in plain dark grey during a representative short portion of the manual material handling task for a typical subject
Significant differences (P < .05) on the factor comparison were observed on all joints (Table 2). Post hoc tests revealed that comparison #1 vs #2 and comparison #1 vs #3 were significantly different (P < .05) on all joint with a total of 18 and 19 joint angles, respectively, out of 24. Significant differences (P < .05) between comparison #2 and #3 were less frequent; they were observed on 6 joints with 11 joint angles out of 24. In general, RMSE was more affected by the type of model (comparison #2) than the technology (comparison #1), with the exception of ankle internal/external rotation that was more affected by technology. Mean ± SD RMSE on all joints was 2.8° ± 1.6° for comparison #1, 9.2° ± 11.1° for comparison #2 and 9.7° ± 10.6° for comparison #3.
Significant differences (P ≤ .01) between tasks were observed on all joints (Table 2). RMSE was systematically higher for the long complex task with a mean ± SD on all joints of 2.8° ± 1.6° compared to 1.2° ± 0.7° during short simple tasks. The RMSE of comparison #1 can be observed for each joint and each axis during the simple short task (Table 3). The maximal differences in RMSE were observed on the ankle joint.
5 Discussion
The performance of commercial IMUs was evaluated against an optoelectronic system as a reference on all joints during manual material handling tasks lasting 32 min. Differences occurring from the technological error and the biomechanical model were dissociated and it was observed as hypothesised that most of the total difference is attributable to the model component, while the technological error is lower. In addition, the IMUs technological error differed according to the tasks performed by the subjects as predicted in our second hypothesis. RMSE was significantly higher for all joints during long complex tasks compared to short simple tasks.
5.1 Comparison #1: Optotrak model ISB vs Xsens model ISB (error due to technology)
Previous IMUs validation studies have mostly been dedicated at evaluating the technological error against an established reference (comparison #1) with various protocols with regard to joints analysed and type of movements executed. Most validation studies report segment orientation errors [5], but our study used segment orientations to measure joint angles in order to estimate the effect of the technological error on joint angles. Between 2.5° and 5.1° RMSE and CMC between 0.66 and 0.97 were reported for thorax relative to pelvis angles during long manual material handling tasks [22]. Another study examined RMSE from segment orientation during short duration asymmetric lifting with values between 4.9° and 23.6° for the back, thorax, head, upper arm and forearm [14]. The results from our study showed lower RMSE and better values of CMC than the latter two studies [14, 22] during similar tasks, which may relate to the improvement of the IMUs and fusion algorithm. Good accuracy was obtained during short trials executed on a pendulum with RMSE between 0.8° and 1.3° [4], similar accuracy was reached in our study during the short simple tasks. Ferrari et al. [12] reported excellent CMC values between 0.95 and 0.99 during short duration walking trials. In our study, CMC values from the hip and knee were similar, but were inferior for the ankle especially for internal/external rotation at 0.77, but the duration of trials and complexity of movements were superior. RMSE of 6.5°on the elbow flexion/extension, of 5.5° on forearm pronation/supination, of 5.5° on shoulder flexion/extension and of 4.4° on shoulder abduction/adduction was reported during short functional movements [9]. The IMUs in our study showed better accuracy than the latter study [9] with RMSE under 3° for the shoulder and elbow angles. Kim and Nussbaum [17] observed mean absolute variability ranging from 0.89° to 5.97° on the back, shoulder, hip and knee during various manual material handling tasks. Although different measures were used, the RMSE we observed is similar to the mean absolute variability reported by Kim and Nussbaum [17]. During simulated milking cluster attachment lasting 8 h, RMSE between 4.1° and 6.2° on the back and between 7.2° and 12.1° on the shoulder joint angles were observed [26]. Lower RMSE was observed in our experiment, but the latter study [26] trials lasted much longer. Swimming simulation with IMUs and optoelectronic system yielded median CMC between 0.90 and 0.99 and RMSE between 3° and 15° on the shoulder, elbow and wrist angles [11]; CMC values in our study were similar, but we observed lower RMSE. The wrist and especially the ankle were more affected by technological error similarly to a study reporting better agreement in proximal joints [11]. A possible explanation is that the feet undergo more acceleration during the manual material handling tasks. Ferrari et al. [12] observed sudden orientation adjustments associated with a sudden change in acceleration, which was related to the Kalman filter. Another possible explanation is that the gyroscopes are sensitive to vibrations shocks [29], which occur when the feet hit the ground. Generally, our technological error compared favourably to the literature, which may be an indication of the improvement of the IMUs over time. Our results combined with two other studies [12, 17] tend to indicate that the Xsens IMUs perform better than other technologies such as APDM [9, 11, 26]. These aspects are both due to the inherent components of the sensors properly calibrated and the algorithm used to estimate orientation.
5.2 Comparison #2: Xsens model ISB vs Xsens model MVN (differences due to biomechanical model)
The only previous study that isolated the model component from the analysis, similarly to our comparison #2, is from Ferrari et al. [12] which observed median CMC values between 0.95 and 0.99 and mean absolute variability between 0.6° and 10.6° on the lower limbs. We observed slightly higher mean values on the lower limbs with CMC ranging from 0.79 to 0.97 and RMSE ranging from 2.5° to 7.0°. The better CMC values from Ferrari et al. [12] may indicate that the Outwalk model [6] is more closely related to a model based on anatomical landmarks than the MVN model. Another possible explanation is that complex motion executed over a prolonged period of time induces some displacements of the IMUs over the skin, which can affect joint angles calculated with the two systems. Since the optoelectronic system relies on position and the IMUs on orientation, a translation of the IMU along the longitudinal axis of the segment should affect more the joint angles calculated from the optoelectronic system.
5.3 Comparison #3: Optotrak model ISB vs Xsens model MVN (total difference)
A few studies [12, 17, 33] compared joint angles obtained from an optoelectronic system with a typical model using anatomical landmarks to those obtained from IMUs with calibration based on sensor placement, defined motion or defined posture as in the MVN model. Kim and Nussbaum [17] observed mean absolute error from 0.88° to 5.13° on the back, shoulder, hip and knee during various manual material handling tasks. Ferrari et al. [12] reports CMC values between 0.92 and 0.99 and mean absolute variability between 1.1 and 11.8° on the lower limbs during walking. Zhang et al. [33] observed during walking mean error from 1.81° to 5.09° and CMC from 0.5 to 0.99 on the ankle, knee and hip angles. Our observations yielded CMC values similar to these three previous studies, but Ferrari et al. [12] obtained better results on the ankle and Zhang et al. [33] obtained worse results on the knee and hip. Our observed RMSE is similar to Ferrari et al. [12] mean absolute variability and slightly higher than Kim and Nussbaum [17] mean absolute error, which may be attributed to the amount of movements executed during the protocol. Kim and Nussbaum [17] trials lasted 60 min in total where 135 short tasks were executed, while our subjects displaced 360 boxes during 32 min. The disparity of results on the shoulder in comparison with Kim and Nussbaum [17] are probably due to the latter study measuring the thoracohumeral joint, since the orientation of the glenohumeral coordinate system based on anatomical landmarks is substantially different to the MVN model, which is mentioned in the Xsens user manual. The large differences in glenohumeral angles were expected due to the distinct model definitions in the MVN model which include different joint coordinate system and centre of rotation estimation in comparison with a model respecting ISB recommendations [30, 31].
5.4 Comparison #1 vs #2 vs #3
When observing the results across the three comparisons, it clearly indicates that the difference is mainly attributed to the distinct biomechanical models. The results from comparison #2 and #3 are closely related, while comparison #1 yields much lower values. Comparison to the study of Kim and Nussbaum [17] is difficult as the model component was not isolated in the analyses. Nevertheless, as noted by the authors, caution must be taken when directly comparing joint angles obtained from an optoelectronic system to those obtained from IMUs due to model definitions. Only six joint angles showed insignificant differences in RMSE between comparison #1 and #2 and they were generally around the Y axis often corresponding to the longitudinal axis of the segment. The technological error is generally low, so the challenge is in the interpretation of the data in comparison to laboratory motion analyses. The calibration of the IMUs as in the MVN model is executed with a single defined posture. Since the ISB model orients coordinate systems according to anatomical landmarks, it introduces a misalignment in anatomical coordinate systems between the two technologies that can be observed on joint angles in comparison #2. Part of this difference is also attributable to definition of centre of rotation, segment lengths, signal processing methods and kinematical constraints in the model. Other calibration approaches exist for the IMUs [3, 20, 21], which may be more closely related to the ISB model than a single posture. Nevertheless, a misalignment will not affect the validity of the results, but the interpretation of the data and inter-study comparison will require caution. For example, a crosstalk could be observed on the elbow angles hampering the analysis of simple movements such as elbow flexion/extension. In addition, the precision of the various IMUs calibration methods gains importance to ensure inter-observer and intra-observer reliability [3].
5.5 Task complexity and duration
Manual material handling tasks in the study of Kim and Nussbaum [17] were executed during three time blocks of 20 min; the first block showed less error than the second and third blocks especially for the Y axis, but the mean absolute error reached a maximum of 3.63°. These authors mention that their data were more affected by the tasks executed, while the performance of the IMUs was rather stable over the time [17]. Other studies support that IMUs are dependent on task complexity [4, 14]. These observations indicate that our observations of more technological error during long complex tasks could be more attributed to the task complexity. However, another study measuring back joint angles showed lower RMSE during short than long duration trials [22], which indicates the duration of the trials can also influence IMUs accuracy.
5.6 Limitations
A few limitations must be noted within the study. The optoelectronic system was used as a reference, since it can measure positions accurately. However, the joint angles measured with this system remain affected by soft tissues artefact [18], but represents a valid reference for orientation estimation. IMUs are affected by ferromagnetic objects, although the laboratory environment was verified with the magnetometers prior to testing, some minor local magnetic field disturbances may still occur during data collection. The results reported are specific to the Xsens IMUs and the Kalman filter fusion algorithm used to estimate orientation. The scapulothoracic joint angles were not reported, because the IMUs positioned over the scapulae within the Xsens suit are not able to track properly the scapular motion. To obtain scapulothoracic angles, IMUs should be positioned closer to the acromion on the skin [7] and not restrained in a suit. While the current study represents an improvement in number of joints and subjects analysed and in complexity and duration of trials, further researches with larger sample size including differences in anthropometry and dedicated at aspects of magnetic distortions, segment velocity, calibration approach and sensor position are still warranted.
5.7 Field application
LoA has often been identified as a better indicator of agreement than CMC or coefficient of correlation [25], but it was sparsely used in previous IMUs validation studies [27]. The determination of the amount of acceptable error remains a clinical and not a statistical decision [2]. Based on previous recommendations [10, 27], a 10° lower or upper LoA was deemed acceptable for occupational biomechanics applications, which is often reached in comparison #1 and attained for 14 of the 25 joint angles in comparison #2. Large errors observed in comparison #2 were caused by the model differences to align similar local coordinate system especially for the elbow and shoulder. This could be partially corrected by improving the static calibration of the IMUs to be closer to the anatomical landmarks (ISB model). The IMUs were evaluated in a laboratory setting; the accuracy of the IMUs in a work environment containing ferromagnetic objects creating magnetic distortions remains unclear. Considering that ergonomic assessment of manual task is often based on qualitative tools [28], the implementation of IMUs directly on the workers during their daily labour would provide quantitative data likely to improve current ergonomic feedback.
6 Conclusion
The observed differences between IMUs and an optoelectronic system were predominantly attributed to the biomechanical model confirming our hypothesis. Caution should be taken for inter-study comparison involving IMUs and optoelectronic systems. The error due to technology stayed under 5° of mean waveform distortion and mean coefficient of repeatability remained under 10°. In addition, IMUs accuracy is affected by the complexity and duration of the tasks highlighted by increased RMSE as hypothesised. Nevertheless, most joint angles remained under an acceptable level of 5° RMSE during manual material handling tasks. IMUs show potential to track workers’ motion during their daily labour without magnetic distortions, which could help in the management of musculoskeletal disorders.
References
An KN, Chao EYS (1991) Kinematic analysis. In: An KN, Berger RA, Cooney WP III (eds) Biomechanics of the wrist joint. Springer, New York, pp 21–36
Bland JM, Altman DG (1986) Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1:307–310
Bouvier B, Duprey S, Claudon L, Dumas R, Savescu A (2015) Upper limb kinematics using inertial and magnetic sensors: comparison of sensor-to-segment calibrations. Sensors 15:18813–18833. doi:10.3390/s150818813
Brodie MA, Walmsley A, Page W (2008) Dynamic accuracy of inertial measurement units during simple pendulum motion. Comp Methods Biomech Biomed Eng 11:235–242
Cuesta-Vargas AI, Galan-Mercant A, Williams JM (2010) The use of inertial sensors system for human motion analysis. Phys Ther Rev 15:462–473. doi:10.1179/1743288X11Y.0000000006
Cutti AG, Ferrari A, Garofalo P, Raggi M, Cappello A, Ferrari A (2010) ‘Outwalk’: a protocol for clinical gait analysis based on inertial and magnetic sensors. Med Biol Eng Comput 48:17–25. doi:10.1007/s11517-009-0545-x
Cutti AG, Giovanardi A, Rocchi L, Davalli A, Sacchetti R (2008) Ambulatory measurement of shoulder and elbow kinematics through inertial and magnetic sensors. Med Biol Eng Comput 46:169–178. doi:10.1007/s11517-007-0296-5
de Vries WHK, Veeger HEJ, Baten CTM, van der Helm FCT (2009) Magnetic distortion in motion labs, implications for validating inertial magnetic sensors. Gait Posture 29:535–541
El-Gohary M, McNames J (2012) Shoulder and elbow joint angle tracking with inertial sensors. IEEE Trans Biomed Eng 59(9):2635–2641
El-Zayat BF, Efe T, Heidrich A, Anetsmann R, Timmesfeld N, Fuchs-Winkelmann S, Schofer MD (2013) Objective assessment, repeatability, and agreement of shoulder ROM with a 3D gyroscope. BMC Musculoskelet Disord 14:72. doi:10.1186/1471-2474-14-72
Fantozzi S, Giovanardi A, Magalhaes FA, Di Michele R, Cortesi M, Gatta G (2015) Assessment of three-dimensional joint kinematics of the upper limb during simulated swimming using wearable inertial-magnetic measurement units. J Sports Sci:1–8. doi:10.1080/02640414.2015.1088659
Ferrari A, Cutti AG, Garofalo P, Raggi M, Heijboer M, Cappello A, Davalli A (2010) First in vivo assessment of “Outwalk”: a novel protocol for clinical gait analysis based on inertial and magnetic sensors. Med Biol Eng Comput 48:1–15. doi:10.1007/s11517-009-0544-y
Gamage SS, Lasenby J (2002) New least squares solutions for estimating the average centre of rotation and the axis of rotation. J Biomech 35:87–93
Godwin A, Agnew M, Stevenson J (2009) Accuracy of inertial motion sensors in static, quasistatic, and complex dynamic motion. J Biomech Eng 131:114501. doi:10.1115/1.4000109
Harrington ME, Zavatsky AB, Lawson SE, Yuan Z, Theologis TN (2007) Prediction of the hip joint centre in adults, children, and patients with cerebral palsy based on magnetic resonance imaging. J Biomech 40:595–602. doi:10.1016/j.jbiomech.2006.02.003
Kainz H, Carty CP, Modenese L, Boyd RN, Lloyd DG (2015) Estimation of the hip joint centre in human motion analysis: a systematic review. Clin Biomech 30:319–329. doi:10.1016/j.clinbiomech.2015.02.005
Kim S, Nussbaum MA (2013) Performance evaluation of a wearable inertial motion capture system for capturing physical exposures during manual material handling tasks. Ergonomics 56:314–326. doi:10.1080/00140139.2012.742932
Leardini A, Chiari L, Della Croce U, Cappozzo A (2005) Human movement analysis using stereophotogrammetry. Part 3. Soft tissue artifact assessment and compensation. Gait Posture 21:212–225. doi:10.1016/j.gaitpost.2004.05.002
Luinge HJ, Veltink PH, Baten CT (2007) Ambulatory measurement of arm orientation. J Biomech 40:78–85. doi:10.1016/j.jbiomech.2005.11.011
Palermo E, Rossi S, Marini F, Patanè F, Cappa P (2014) Experimental evaluation of accuracy and repeatability of a novel body-to-sensor calibration procedure for inertial sensor-based gait analysis. Measurement 52:145–155
Picerno P, Cereatti A, Cappozzo A (2008) Joint kinematics estimate using wearable inertial and magnetic sensing modules. Gait Posture 28:588–595
Plamondon A, Delisle A, Larue C, Brouillette D, McFadden D, Desjardins P, Lariviere C (2007) Evaluation of a hybrid system for three-dimensional measurement of trunk posture in motion. Appl Ergon 38:697–712
Reed M, Manary MA, Schneider LW (1999) Methods for measuring and representing automobile occupant posture. SAE Technical Paper
Roetenberg D, Luinge H, Slycke P (2009) Xsens MVN: full 6DOF human motion tracking using miniature inertial sensors. Xsens Motion Technologies BV, TechRep
Roislien J, Skare O, Opheim A, Rennie L (2012) Evaluating the properties of the coefficient of multiple correlation (CMC) for kinematic gait data. J Biomech 45:2014–2018. doi:10.1016/j.jbiomech.2012.05.014
Schall MC, Jr., Fethke NB, Chen H, Oyama S, Douphrate DI (2015) Accuracy and repeatability of an inertial measurement unit system for field-based occupational studies. Ergonomics:1–23. doi:10.1080/00140139.2015.1079335
Schiefer C, Ellegast RP, Hermanns I, Kraus T, Ochsmann E, Larue C, Plamondon A (2014) Optimization of inertial sensor-based motion capturing for magnetically distorted field applications. J Biomech Eng 136:121008
Vignais N, Miezal M, Bleser G, Mura K, Gorecky D, Marin F (2013) Innovative system for real-time ergonomic feedback in industrial manufacturing. Appl Ergon 44:566–574. doi:10.1016/j.apergo.2012.11.008
Weinberg H (2011) Gyro mechanical performance: The most important parameter. Technical article MS-2158 Analog Devices, Inc:1–5
Wu G, Siegler S, Allard P, Kirtley C, Leardini A, Rosenbaum D, Whittle M, D’Lima DD, Cristofolini L, Whittle H, Schmid O, Stokes I, Standardization, Terminology Committee of the International Society of B (2002) ISB recommendation on definitions of joint coordinate system of various joints for the reporting of human joint motion–part I: ankle, hip, and spine. International society of biomechanics. J Biomech 35:543–548
Wu G, van der Helm FC, Veeger HE, Makhsous M, Van Roy P, Anglin C, Nagels J, Karduna AR, McQuade K, Wang X, Werner FW, Buchholz B (2005) ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion–Part II: shoulder, elbow, wrist and hand. J Biomech 38:981–992
Zatsiorsky VM (1998) Kinematics of human motion. Human Kinetics, Champaign
Zhang J-T, Novak AC, Brouwer B, Li Q (2013) Concurrent validation of Xsens MVN measurement of lower limb joint angular kinematics. Physiol Meas 34:N63–N69
Zhou H, Hu H, Tao Y (2006) Inertial measurements of upper limb motion. Med Biol Eng Comput 44:479–487
Acknowledgments
The authors are grateful to the IRSST for financial support of the study through grant (2012-0040) and postdoctoral scholarship program and wish to recognise the technical assistance from Sophie Bellefeuille.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Robert-Lachaine, X., Mecheri, H., Larue, C. et al. Validation of inertial measurement units with an optoelectronic system for whole-body motion analysis. Med Biol Eng Comput 55, 609–619 (2017). https://doi.org/10.1007/s11517-016-1537-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11517-016-1537-2