
Abstract
Drug abuse and co-occurring infections are associated with significant morbidity and mortality. Asian countries are particularly vulnerable to the deleterious consequences of these risks/problems, as they have some of the highest rates of these diseases. This review describes drug abuse, HIV, and hepatitis C (HCV) in Asian countries. The most commonly used illicit drugs include opioids, amphetamine-type stimulants (ATS), cannabis, and ketamine. Among people who inject drugs, HIV rates range from 6.3 % in China to 19 % in Malaysia, and HCV ranges from 41 % in India and Taiwan to 74 % in Vietnam. In the face of the HIV epidemics, drug policies in these countries are slowly changing from the traditional punitive approach (e.g., incarcerating drug users or requiring registration as a drug user) to embrace public health approaches, including, for example, community-based treatment options as well as harm reduction approaches to reduce needle sharing and thus HIV transmission. HIV and HCV molecular epidemiology indicates limited geographic diffusion. While the HIV prevalence is declining in all five countries, use of new drugs (e.g., ATS, ketamine) continues to increase, as well as high-risk sexual behaviors associated with drug use—increasing the risk of sexual transmission of HIV, particularly among men who have sex with men. Screening, early intervention, and continued scaling up of therapeutic options (drug treatment and recovery support, ART, long-term HIV and HCV care for drug users) are critical for effective control or continued reduction of drug abuse and co-infections.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Drug abuse, HIV, and HCV are highly prevalent in Asia. Asian countries are particularly vulnerable to the deleterious consequences of these problems as they have some of the highest rates of drug use (involving opiates/opioids, methamphetamine, alcohol, and tobacco), and HIV and HCV infections. Much of the estimated burden of disease attributable to the use of illicit drugs is due to blood-borne viral infections through unsafe drug injection. Therefore, injection drug users (IDUs) are at high risk of co-infection with both HCV and HIV. The problems are exacerbated by inadequate access to treatment, the criminalization of drug use, and stigma associated with both substance use and HIV/AIDS, combined with limited infrastructure for addressing these issues and a lack of evidence-based research to help guide future policy and treatment plans on a local and national level. Drug abuse is associated with high morbidity and mortality (Degenhardt et al. 2013), and HCV and HIV contribute substantially to morbidity and mortality in this population. For example, in a systematic review based on studies published up to 2009, it was found that the highest opioid-involved mortality rates across the world were in Asia (Degenhardt et al. 2011). Another systematic review of the literature through 2012 (Mathers et al. 2013) reported that Asia has the highest opioid-related mortality rate of any world region.
Recognizing this continuing challenge, a series of conferences promoting global health focusing on Asian countries has been organized. The 2015 conference highlighted presentations from five Asian countries on their status of drug abuse and HIV including China, India, Malaysia, Taiwan, and Vietnam. Here we offer a review of research to illustrate the epidemiology and responses and policy options in these Asia countries. Specifically, we describe the (1) prevalence of drug use and people who inject drugs (PWID), (2) the prevalence of HIV among IDUs, (3) the prevalence of HCV among drug users, and (4) national responses and policy options (e.g., mandatory treatment, medication-assisted therapy, needle exchange programs) in these five countries.
Drug Abuse
Historically, cannabis and opiates were the two most commonly used drugs across Asia (Kulsudjarit 2004). In the past two decades, the Asian region has witnessed an explosive increase in the manufacture and use of amphetamine-type stimulants (ATS) and ketamine, especially among the younger population, and this trend continues to grow unabated. According to the World Drug Report 2015, cannabis, opioids, and ATS are now the drugs most commonly abused globally (UNODC 2015a). These drugs are also common in the five Asian countries, with the addition of ketamine being widely abused in China and Taiwan.
Opioids (heroin, opium, other opiates, prescription opioids) have a long history of use in Asian countries. Opium and its derivatives (e.g., heroin) induce euphoria as well as analgesia and tranquility and therefore have been used for medical purposes (as an analgesic) as well as for delectation. The use of illegal opiate drugs such as heroin and the misuse of legally available pain relievers such as oxycodone and hydrocodone can have serious negative health effects. Intravenous heroin use is complicated by other issues such as the sharing of contaminated needles resulting in the spread of HIV and HCV.
Amphetamine-type stimulant (ATS) drugs are synthetic stimulants that affect the central nervous system; ATS drugs include methamphetamine, amphetamine, MDMA (or Ecstasy), and drugs that have a similar chemical structure as MDMA, often referred to as “designer” or “club” drugs (UNODC 2013). While amphetamine and methamphetamine are psychologically and physically addictive, addiction to MDMA and health risks of MDMA are in considerable debate; use of non-prescribed ATS formulations are criminalized in most countries in the world. Increasing abuse of ATS drugs is occurring in East and Southeast Asian nations. The overall trend in this region is a shift from traditional drugs (e.g., opium or heroin) to ATS drugs as the most prevalent drug on the illegal market. The ATS epidemic is becoming a serious challenge for these regions.
Ketamine or ketamine hydrochloride, a synthetic medicine, is used originally for the induction of anesthesia in humans and animals, but is now also abused as a hallucinogen, particularly among young people. Ketamine, like MDMA, is regarded as one of the “club drugs,” and therefore often used together with MDMA or mixed in MDMA products. Ketamine has been known to produce illusions or hallucinations that are enhanced by environmental stimuli and has become increasingly popular in the past few years in Asia.
Cannabis is by far the most commonly used illicit drug in the world. Cannabis grows wild in various countries including Central Asia, and also has been cultivated in Asia, Africa, and the Americas. While many countries have decriminalized or legalized cannabis, Asian countries have the strictest cannabis laws, with possession and use of cannabis carrying serious legal consequences. Cannabis contains at least 85 cannabinoid compounds, few of which have been studied to provide knowledge on specific effects. Psychotropic actions of cannabidiol, for example, have antipsychotic and antianxiety effects, while THC (tetrahydrocannabinol) can produce adverse psychiatric effects (e.g., precipitating schizophrenia in vulnerable individuals). Cannabis generally exhibits sedative, anesthetic, and hallucinogenic actions.
The epidemiology of drug use and disorders in different Asian countries is distinct from in Western nations and can be different even among areas within the same country. Table 1 lists the top three most used illicit drugs in the five countries.
China
In China, heroin has been and remains the primary drug of addiction, but an increasing number of people are using “new” drugs such as methamphetamine, Ecstasy, and ketamine, and increasing numbers are developing related substance use disorders, including addiction. In China, a national registry has been established for drug users identified or arrested by local police agencies, which are routinely submitted and published in the Annual Report on Drug Control in China. The annual number of registered drug users has been continuously increasing, and the type of drugs being abused has been changing (Zhang and Chin 2016). Among all identified drug users, heroin use decreased from 88.2 % in 2003–04 to 56.8 % in 2008–10, while synthetic drug use increased from 6.5 % to 40.8 % during the same periods, respectively (Jia et al. 2015). Similarly, use of club drugs also increased from 1.3 % in 2004 to 24.4 % in 2011 (Wang et al. 2015a. In 2014, heroin, ATS (particularly methamphetamine), and ketamine were the most commonly used drugs among registered drug users, with 1.46 million opiate users; 1.19 million methamphetamine users; and 222 thousand ketamine users (National Narcotics Control Commission 2015). An estimated 2.17 million people injected drugs in 2011 (www.aidsdatahub.org).
India
Cannabis and opium have been traditionally used in India for centuries. The use of synthetic drugs and psychotropic substances is comparatively new. Information on substance use in India is mostly anecdotal due to the scarcity of data and reports available only from small-scale surveys. The latest national epidemiologic study (Ray 2004) about substance use in India was the National Household Survey (NHS) in 2000–01, with 40,697 male respondents age 12 to 60 years in 25 states included in this study. Alcohol, cannabis, and opiates were found to be the three most commonly used substances and also the primary substances associated with the development of a substance use disorder. In the preceding month, 21.4 % used alcohol; 3.0 % used cannabis; and 0.7 % used opiates, which translated to 8.7 million users of marijuana and 2 million users of opioids. These data from the year 2004 are the most comprehensive data on drug use in the country till now (Pawar et al. 2015). Some researchers estimated between 180,000 and 1.1 million users of injected drugs in the country (Bergenstrom et al. 2013; Solomon et al. 2015).
Malaysia
In Malaysia, according to the World Drug Report 2014, the three most commonly used drugs among persons in prison were heroin/morphine, “syabu” (methamphetamine), and “ganja” (marijuana) in 2011 (UNODC 2014). Like China, Malaysia puts drug users in prison. According to UNODC estimates, the annual prevalence of use as a percentage of the population age 15–64 is 0.94 % for opiates, 1.6 % for cannabis, and 0.6 % for amphetamines. However, the estimates of UNODC for the prevalence of cannabis and amphetamines were based on estimates in 2003 (UNODC 2011). The estimated number of people who inject drugs was 170,000 in 2014 (www.aidsdatahub.org).
Taiwan
In Taiwan, according to the National Household Survey (based on a multistage stratified sampling strategy, with approximately 18,000 individuals interviewed each year when the survey was conducted), the prevalence of illicit substance use was 1.2 % in 2005, 1.4 % in 2009, and 1.29 % in 2014. Based on data regarding treatment admission and urine testing among drug offenders, the major drug problems in Taiwan are heroin, methamphetamine, and ketamine (Yu et al. 2013). Aceijas et al. (2004) estimated that there are 60,000 people who inject drugs in Taiwan; a more updated estimate is unavailable.
Vietnam
In Vietnam, the UNODC World Drug Report 2013 indicates that heroin was still the most popular drug, while ATS drugs had become the second most popular in Vietnam (UNODC 2013). According to the estimates of UNODC, the annual prevalence of drug use as a percentage of the population age 15–64 is 0.27 % for opiates, 0.3 % for cannabis, 0.2 % for amphetamines, and 0.2 % for Ecstasy (UNODC 2011). By the end of 2013, 181,396 people were registered in Vietnam as drug dependent (UNODC 2014). In 2011, an estimated 335,990 people—approximately 0.53 % of the population—injected drugs. The number of people who inject drugs continues to increase, partly due to the increased popularity of intravenous crystal methamphetamine consumption (National Committee for AIDS, Drugs and Prostitution Prevention and Control of Vietnam 2012).
HIV among Drug Users
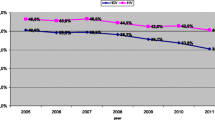
According to the latest estimates from UNAIDS, there are approximately 35 million people currently living with HIV in 2013, of whom 4.9 million people are living with HIV (PLWHIV) in Asia and the Pacific Islands and about 350,000 individuals were newly infected (UNAIDS 2014). The HIV epidemic in East Asia started in the 1990s, relatively late compared to the rest of the world. Nevertheless, East and South-East Asia soon were regions with particularly high rates of new HIV infections among individuals who inject drugs (Petersen et al. 2013). Injection drug use was the major driving force of HIV transmission and infection in these regions. Following the global trend, unsafe sexual contact has now become a major route of infection across the regions. In Asia, an estimated 3 to 4 million people inject drugs (UNODC 2015b). There is great heterogeneity in infection rates across nations, which suggests region-specific estimates are more informative. Based on the latest UNAIDS report and on data compiled by AIDS Data Hub, the prevalence estimates of HIV among people who inject drugs in these five countries are provided in Fig. 1. Estimates of HIV among non-injection drug users are generally unknown.

Prevalence of HIV and HCV among people who inject drugs
In China, it was estimated that in 2013 there were approximately 810,000 people living with HIV (www.aidsdatahub.org). Needle sharing among IDUs and sexual contact between IDUs and sex workers are the major drivers of later sub-epidemics across mainland China (Saidel et al. 2003). In 1999, HIV prevalence peaked at 30.3 % among IDUs, and then decreased gradually to 10.9 % by 2011 (Wang et al. 2015a, with the number of people infected with HIV via injection drug use estimated at some 221,000 at the end of 2011 (Ministry of Health 2014). A decline in needle sharing among IDUs from 19.5 % in 2006 to 11.3 % in 2011 was also observed. The most current data available showed that in 2013, the HIV rate among IDUs is 6.3 % (National Health and Family Planning Commission of the People’s Republic of China’s 2015). These dramatic reductions in injection-related risk behaviors and HIV infection among this group have been attributed to the rapid scale-up of harm reduction strategies (e.g., scaling up of methadone maintenance treatment, needle exchange programs).
In India, the estimated number of adults and children living with HIV in 2013 was 2,100,000 (www.aidsdatahub.org). The annual report from Department of AIDS Control (2014) mentioned that female sex workers at the national level and in most states show declining HIV trends. However, men who have sex with men (MSM), IDUs and single male migrants are emerging as important risk groups in many states. As indicated earlier, India has a large group of IDUs. The overall national HIV prevalence in 2010–2011 was around 7.15 % among IDUs, which is the second highest among all key populations in the country including antenatal care attendees, female sex-workers, MSMs, transgenders, and patients with sexually transmitted infections (STIs) (National AIDS Control Organization 2012).
In Malaysia, the 2014 estimated number of people living with HIV was about 100,000. Opioids are the most commonly injected substances; 1.3 % of adults or about 170,000 individuals inject drugs (PWID), which is among the highest rates of injection drug use globally (Bachireddy et al. 2011; Fu et al. 2012a; Mathers et al. 2008). Among PWID in Malaysia, HIV prevalence is estimated at 18.9 % in 2012, or by some at the range of 15.9 %–19.0 % (Bazazi et al. 2014; Ngadiman et al. 2014).
According to the CDC in Taiwan (Taiwan CDC, 2015), as of the end of 2013, the total number of HIV cases amounted to 26,475 (11,176 of whom had developed full-blown AIDS and 4171 cases had died). The number of HIV infections among IDUs began to surge in 2003 and then consistently decreased since the commencement of Taiwan’s national harm reduction programs. In 2008 and thereafter, the epidemic took a turn; infections mainly occurred through sexual encounters. An analysis of risk factors showed that in 2013, the highest proportion of HIV infections was a result of unsafe sexual transmission, with MSM accounting for 80 % of all cases. The second largest proportion (12 %) of infections was attributable to heterosexual contact. The estimated number of injection drug users living with HIV was 5315 and the HIV prevalence rate among IDU was at 8.9 % in 2014 (Taiwan CDC 2015).
In Vietnam, at the start of 2014, an estimated 256,000 people—0.26 % of the general population older than 15—were living with HIV (Ministry of Health of Vietnam 2015). The HIV rate was estimated at 10.3 % among injection drug users in 2013. According to Hammett et al. (2012), the HIV epidemic in Vietnam was driven by three key factors: the country’s location on a major heroin trafficking route from the Golden Triangle region with large-scale cultivation of opium poppies, rising income levels, and strong social stigma that makes people who inject drugs harder to reach with prevention information and treatment options. Roughly 14,000 new infections were annually reported between 2010 and 2013. While prevalence has dropped from its peak in the early-2000s, Vietnam continues to have one of fastest growing HIV rates in Asia. Intravenous drug use is the primary means of contracting HIV in Vietnam: around 60 % of all new HIV cases are contracted through needle sharing.
Overall, the HIV epidemic in many parts of the Asia is now declining. While much progress has been achieved in this region, with the epidemic among other key populations relatively stable, the emerging epidemic among MSM via sex between men is a growing concern. Recent estimates suggest that HIV prevalence among MSM has reached 3.7 % in Vietnam, 4.4 % in India, 7.3 % in China, and ranges between 8.1 %-10.7 % in Taiwan, and 12.6 % in Malaysia (www.aidsdatahub.org). There is urgent need to address issues of discrimination and stigma toward homosexuality, and to strengthen the strategies to reach and care for this population.
Hepatitis C (HCV) among Drug Users
An estimated 184 million people worldwide are infected with HCV (Mohd Hanafiah et al. 2013). High HCV prevalence has been reported in many Asia countries. People who inject drugs have a disproportionate prevalence (60–80 %) of HCV infection compared with people who do not inject drugs (Aceijas and Rhodes 2007; Nelson et al. 2011). Chronic HCV infection is associated with substantial morbidity and mortality. However, most individuals infected with HCV are unaware of their infection because HCV can be symptom-free for decades. Epidemiology data on HCV in Asian countries have been limited, but a recent systematic review by Nelson et al. (2011) provided the first regional estimates of the number of IDUs living with HCV. Figure 1 included mid-point prevalence estimates of the percentages of individuals testing positive for HCV-antibodies among IDUs for the 5 countries: 41 % in Taiwan (2001) and India (2006), 67 % in China (2010) and Malaysia (2007–2007), and 74.1 % in Vietnam (2003).
As is the case with HIV, there is great heterogeneity in HCV infection rates across nations, which suggests region-specific estimates are more informative. A systematic review of HCV infection among drug users in China (Bao and Liu 2009) reported that the HCV prevalence rate ranged from 11.43 % (Shannxi) to 90.77 % (Hubei) among IDUs, and from 0 % (Anhui) to 40.00 % (Fujian) among non-IDUs. A recent large survey of drug users from 15 cities across India reported a high burden of HCV (37.2 %) and HIV/HCV co-infection (13.2 %) (Solomon et al. 2015). Several more recent studies in Taiwan reported a prevalence range of 53–90 %. In Vietnam, highest prevalence rates have been observed in Ho Chi Minh City (85–100 %). On the other hand, low HCV prevalence in Malaysia was observed in a sample of IDUs in a medical setting in Kuala Lumpur (30 %). The varying estimates of the prevalence rates even within the country reflect heterogeneity of the target samples, geographic areas, data collection methods, and timeframes used in the specific studies.
HCV/HIV co-infections are highly prevalent in Asia. HCV/HIV co-infection may accelerate the clinical progression of both HCV and HIV. The high prevalence of HCV/HIV co-infection in Asia underscores the need to improve prevention and control measures, as fewer evidence-based prevention strategies are available.
HIV and HCV Molecular Epidemiology
Examining HIV viral sequences downloaded from HIV databases (hiv.lanl.gov/content/index), evolution tree analysis shows the geographic distribution of HIV-1 subtypes by the five Asia countries. For example, the major HIV genotype transmitted among IDUs in China were BC recombination viruses (CRF07_BC or CRF08_BC), which was also presented in Taiwan but not much in other countries except in some special cases (e.g., cross-border travelers entering China from Vietnam [Wang et al. 2015b]). The predominant genotype among IDUs in Malaysia is the 01B recombinant virus. Similar data are not available from the HIV database for India and Vietnam. Nevertheless, the available literature reported that in India, subtype C is the predominant subtype, which has been reported as one of the parental strains of CRF07_BC and CRF08_BC in China (Tee et al. 2008; Liu and Zhang 2011; Ronsard et al. 2014). HIV-1 CRF01_AE genotype is dominant in Northern Vietnam, which is closely related with the HIV-1 CRF01_AE sequences from Southern China (Tran 2008; Bontell et al. 2012). These patterns suggest some limited interaction of populations between countries, with some HIV genetic clusters circulating among selected countries.
Available evidence from molecular epidemiology suggests longstanding endemic HCV infection of populations in Africa and Asia, with movement into new transmission networks in industrialized nations, resulting in the recent epidemic in both blood transfusion recipients and IDUs. In Asia, while HCV and HIV share similar transmission routes, the lack of HCV prevention knowledge and treatment further heightens the risk for HCV infection (Piao et al. 2014). For example, a study has identified history of hospitalization and tattoo as significant factors associated with HCV patients in Vietnam (Nguyen et al. 2007). Similar to HIV, the spread of HCV virus transmission among injecting drug users is limited between countries in Asia. For example, HCV genotype 6, which transmitted rapidly during the 20th century in specific locations in Asia injecting drug users, but did not spread internationally as the “global epidemic” subtypes 1a, 1b, and 3a (Stumpf and Pybus 2002). These previous evolution studies indicate that individual Asian countries typically have local epidemic subtypes (e.g., subtype 6d from Vietnam or subtype 6q from Cambodia), often by different transmission routes, and less often shared by two neighboring countries (e.g., subtype 6a from China/Vietnam or subtype 6n from Thailand/Myanmar) (Pybus et al. 2009). The HCV phylogenetic trees show similar profiles among injecting drug users in Asia.
HCV can be separated into 7 genotypes and more than 50 sub-genotypes. Genotypes 1a and 1b are the oldest and most popular in global infections. For example, subtype 1b is most prevalent in China, followed by genotypes 2, 3 and 6, with substantial regional variation (Peng et al. 2015). Beside sporadic cases in old genotype 1 and 3 that had outbreak during 2009–2010, most of genotypes1–3 were originally tracing before 1991 and the new genotype 6 no later than 2005 in China. Even the specific genotype 6 strains which originated from Vietnam during 1984–1994 were only detected among IDUs in limited regions in China (Fu et al. 2012b). HCV subtypes 3a, 1a, and 1b were identified in patients at Malaysia with subtype 3a being the most prevalent (Mohamed et al. 2013). HCV subtype 3a and 1b were reported among IDUs at India (Mehta et al. 2010). Taiwan had a similar pattern with most of the HCV endemic occurred earlier than HIV transmission among co-infected injecting drug users. The HCV genotypes among injecting drug users in a local survey (Lan et al. 2014) indicated genotype 1a, 1b, 2b, 3a, 6a, 6n, 6w. In this survey, all these viruses were related with local community sequences and did not cluster with the virus from other countries.
National Responses and Policy Options
Most Asian countries traditionally take a punitive approach to drug use by incarcerating drug users or requiring registration as a drug user or “addict.” In the face of the HIV epidemics, drug policies in these countries are slowing changing to embrace harm reduction approaches such as needle exchange programs to reduce sharing of injection equipment and thus reduce HIV transmission. Punitive responses to drug users have been shown to increase HIV risk behaviors, such as equipment sharing during intensified police activity, avoiding drug treatment or needle exchange programs out of fear of police surveillance, or decreasing access and use of services (Hammett et al. 2007; Tanguay et al. 2015). In contrast, public health approaches to prevent and treat drug abuse, HIV, and HCV have been demonstrated to work (Hammett et al. 2007; Tanguay et al. 2015). Policy responses in the five countries are summarized in Table 2, presenting the limited relevant information that is available.
Mandatory Treatment in Compulsory Drug “Rehabilitation” Centers
In many Asian countries including China, Malaysia, and Vietnam, a primary response to drug use is the practice of detaining drug users in compulsory drug “rehabilitation” centers (Kamarulzaman and McBrayer 2015; WHO 2009). These facilities are usually operated by the criminal justice systems and provide little if any evidence-based treatment. The duration of incarceration in these centers varies from country to country, but often the term is for several years.
In China, drug use and dependence are unlawful and subject to administrative punishment and placement on the national register of drug users. Arrested by the police and determined by the police to be drug users, a person may be detained in compulsory drug rehabilitation for 1 to 3 years. The Anti-Drug Law of 2008 stipulates that first offenders are subject to community treatment for their substance use and repeat offenders are subject to 2 years of detention.
In Malaysia, as of legislation in 1983, drug users are sent to detention facilities for a mandatory two-year sentence and 2 years of community supervision following release (Gill et al. 2011; Kamarulzaman 2009). These centers are operated by the Malaysian National Anti-Drug Agency under the Ministry of Home Affairs. Up until 3 years ago, the programs conducted in these centers had an emphasis on forced work regimens, grueling physical exercise, and military style training (Pearshouse 2009; Human Rights Watch 2010; Fu et al. 2012a.
In Vietnam, terms of detention (known as 06 Centers) initially were as long as 5 years: two of “treatment” and three of labor in facilities built near the detention centers. Vietnam has since moved to 2 years of detention followed by an evaluation for post rehabilitation which may include an additional 2 years in the compulsory detention centers (National Committee for AIDS, Drugs and Prostitution Prevention and Control of Vietnam 2014).
Because of ethical concerns and lack of evidence for effectiveness in reducing drug use via compulsory detention, the United Nations has recently called on countries to close all compulsory rehabilitation centers and to end the practice of compulsory treatment of drug dependence. In response, Malaysia and Vietnam have begun converting some compulsory centers to being open and voluntary (Baldwin 2013; UNODC Drug Dependence 2014). Similarly, China created non-custodial treatment orders allowing a three-year period of rehabilitation in the community or 1 to 3 years of recovering after release from a compulsory treatment center; the use of re-education through labor has supposedly been abolished since 2008. These recent shifts in drug policy suggest a more health-oriented approach to drug use in China, Malaysia, and Vietnam, although drug prohibition continues to dominate responses by these nations.
Therapeutic Options and Harm Reduction Strategies
While change to the policy focus on criminal justice monitoring and punishment has been slow, several positive signs are emerging. UNAIDS/WHO have suggested nine different interventions for countries to set targets for universal access to HIV prevention, treatment, and care of IDUs. To control HIV transmission, many Asian countries have committed to expanding access to methadone maintenance therapy (MMT) as well as HIV/HCV care. From the initial pilot studies mostly conducted in the mid-2000s, these governments have scaled up MMT to reach a target number of opioid-dependent people. Nevertheless, MMT coverage continues to be inadequate. While free antiretroviral therapy (ART) is available in all five countries, access and coverage varies across countries, and most people living with HIV/HCV or at risk for HIV/HCV do not have access to prevention, care, and treatment. It is estimated that in Asia and the Pacific islands, the overall treatment coverage is approximately 30 % only (WHO 2014a).
In response to the HIV epidemic, China has adopted a comprehensive HIV/AIDS strategy to confront the growth of HIV infection among opioid users (Wu et al. 2015). The two largest of these programs aimed at harm reduction among IDUs are the methadone maintenance treatment (MMT) program and needle exchange program (NEP) implemented throughout the country (Sullivan and Wu 2007; Wu et al. 2015). The first eight MMT clinics were set up in early 2004, and by 2014, China had opened 767 MMT clinics. Opiate users covered by the MMT program increased from 1209 in 2004 to 37,345 in 2006 and to 344,254 in 2011 (Wang et al. 2015a, b). Similar to the MMT program, expansion of NEP also occurred after 2006, increasing to 775 sites in 2007 and to 937 sites in 2011 and to 814 in 2014. These large-scale harm reduction programs have significantly impacted the HIV epidemic among the drug-using population. There is a growing acceptance of the need to strengthen harm reduction programs, to increase the availability of opportunities for voluntary rehabilitation, and to coordinate drug control policies better with harm reduction strategies. Starting in 2009, Chinese authorities declared that labor camps were no longer available for drug treatment purposes. Instead, chronic addicts are now “committed to community-based treatment programs.” Nevertheless, a disproportionately low number of HIV-infected drug users in China receive ART (Zhang et al. 2011). Additionally, the sexual transmission of HIV among drug users is now considerable, particularly with the rapid increase in club drug use and highly prevalent alcohol use (Wu et al. 2015). High-risk sexual behaviors are common among users of club drugs in China. Prevention and intervention efforts targeting club drug use could decrease the risk of sexual behaviors which further prevent HIV transmission and other sexually transmitted infections (STI) in China.
In India, the National AIDS Control Organization (NACO) provides HIV prevention services to high-risk groups, including IDUs, through targeted interventions (TI) delivered by non-governmental organizations (NGOs) (Government of India, Ministry of Health & Family Welfare, National AIDS Control Organisation (2014)). For IDUs, TI services include behavior change communication, provision of sterile needles and syringes, condom provision, treatment for STIs, oral substitution therapy and referrals for HIV testing and anti-retroviral treatment. NGOs implement TI work through outreach workers (ORWs) and peer educators who are often individuals with a history of injection drug use. In recent years, NACO has considerably scaled up HIV prevention and harm reduction efforts (NACO 2015), providing an important opportunity for treatment of HIV-positive IDUs. As of 2014, India had 401 NEP sites and 178 treatment sites (aidsdatahub 2015). Nevertheless, despite the widespread availability of antiretroviral treatment, only 11.7 % of injecting drug users who are HIV positive received treatment (Wherley and Chatterjee 2015). A recent study (Chakrapani et al. 2014) showed that stigma and discrimination related to HIV-positive status prevented both current and former IDUs from disclosing their HIV status to their families and even to peer outreach workers of agencies working with IDUs. Also, actual or perceived unfriendly hospital environment and procedures discouraged some IDUs from attending government ART centers.
In Malaysia, harm reduction initiatives involving medication assisted therapy (MAT, but locally called Opiate Substitution Therapy) and needle and syringe exchange program (NSEP) have been part of the Malaysian response for several years. By 2014, provision of harm reduction services continues and up-scaled through 692 NSEP sites and 838 MAT outlets established in government health facilities, NGO sites, private health facilities, National Anti-Drug Agency (NADA) service outlets and prisons (UNAIDS 2015). Unlike the remainder of Southeast Asia where HIV-related mortality has decreased, HIV-related mortality has increased in Malaysia (Joint United Nations Programme on HIV/AIDS (UNAIDS 2014). Despite the harm reduction initiatives in the country there was still inadequate access to harm reduction programs and to antiretroviral therapy (ART) for PWID, which contributed to the high HIV-related mortality (Degenhardt et al. 2013). There is also a large gap in TB/HIV care; low early TB screening and awareness lead to late TB diagnosis resulting in high mortality among PLHIV due to TB. The government also considers it a priority to eliminate stigma and discrimination among key populations as well as within the community and healthcare providers.
Taiwan has conducted a series of harm reduction programs, including health education, HIV-testing, providing clean syringes, and methadone treatment to reduce the risk of HIV and viral hepatitis transmission among IDUs. After its initial success in controlling the transmission of HIV among IDUs in less than 5 years in Taiwan (Yang et al. 2008), these harm reduction programs have become routinized medical and public health practice.
In Vietnam, there has been a significant decline in HIV prevalence among PWID thanks in large part to targeted harm reduction interventions (National Committee for AIDS, Drugs and Prostitution Prevention and Control of Vietnam 2014). By the end of 2013, the MMT program had been expanded to 134 sites in 32 provinces serving 18,000 PWID. AIDS-related morbidity and mortality have decreased thanks to the scale up of testing, treatment and care of PLHIV. Despite these considerable achievements, HIV remains a formidable challenge as AIDS is still among the top causes of premature death. Harm reduction intervention coverage is still far below the level required to contain the epidemic: e.g., needle and syringe program coverage is only 29 %, while MMT service coverage is only 15 % of the need. Stigma and discrimination are also significant barriers to the uptake of HIV services across Vietnam. Confidentiality concerns are particularly challenging. In a 2011 survey, nearly 30 % of PLHIV said that their serostatus had been disclosed without their consent (VNP+, 2012). Vietnam also is concerned about rapidly declining donor contributions, which presents a major threat to the sustainability of current achievements, and to future progress in preventing new infections and providing treatment for PLHIV.
Discussion and Future Directions
This review details the prevalence of drug use, HIV, HCV, and the type of responses and policy options in five Asian countries. Varying rates of prevalence and varying levels of treatment and services have been noted, but there are also many similarities among these countries in the patterns of drug use, HIV, and HCV, as well as responses to these problems.
Largely driven by the rapid spread of HIV among people who inject drugs, responses to drug use in many Asian countries have undergone considerable transformation in the past decade. These Asian countries have begun to seek some balance between law enforcement and public health approaches to drug use. Over the recent years, despite persistent law enforcement approaches to drug use, harm reduction interventions have become increasingly accepted to varying degrees by several Asian governments. Nevertheless, access to treatment and care is limited and many barriers remain to be overcome. For example, many countries cite considerable stigma associated with drug use and HIV, which presents challenges to voluntary screening and disclosure (Joint United Nations Programme on HIV/AIDS (2014)). For infected persons with access to ART, HIV infection has become a manageable chronic condition, but few countries have plans or are prepared for meeting the need for longer term care. MMT admission is declining despite continued high prevalence of opioid use. The concept of MAT is not conducive to most Asian cultural norms, and none of the MMT programs in Asia has take-home options. Extended-release depot naltrexone (an opioid antagonist administered by monthly injection) should also be considered for use by Asian countries in the future.
In the past decades, considerable progress has been achieved in containing the spread of HIV among IDUs. However, even relatively low prevalence rates translate into large numbers of people in countries such as China and India that are among the most populous nations in the world. Injection drug use continues to be a critical contributor to HIV and HCV infection, but types of drug used by drug users have gone beyond heroin, with increasing use of methamphetamine across the regions and of ketamine in Taiwan and China. Changes in the drug use and HIV epidemics call for new approaches. ATS drugs present new challenges. While transmission of HIV is well documented in the context of heroin injection, ATS use carries the risk of increasing HIV transmission through sexual risk behavior and pathological immune processes (Colfax et al. 2010). Most of the responses to the drug situation in Asia have been developed in response to opioid use. While ATS has recently become the leading drug problem in these regions, Asian countries generally are among the least equipped to respond to the ATS situation. Additionally, following a global trend, unsafe sex has become a major route of infection in many Asian countries. While much progress has been achieved in this region, with the epidemic among other key populations relatively stable, the emerging epidemic among MSM is a growing concern. The lack of data on HIV and HCV rates among ATS users and other non-injection drug users should be a matter of concern. This lack of knowledge affects planning prevention and harm reduction services for this high-risk population.
Despite the high burden of HCV, few drug users are familiar with the disease, and of those who were infected with HCV, few are aware of their infection. Harm reduction interventions (e.g., MAT and needle exchange programs) targeting individuals who inject drugs will be crucial to minimize onward transmission of HCV, but poor HCV knowledge coupled with low HCV treatment access suggests the critical need for scaling up educational efforts. HCV medication therapies are rapidly evolving, but access and awareness and other considerable barriers need to be overcome to control worldwide HCV infection. In addition to cost, many countries report that legal and stigma issues are continuing barriers for infected individuals to access HIV/HCV testing and care. There is a particularly urgent need to address issues of discrimination and stigma toward homosexuality, and to strengthen the strategies to reach and care for this population. Given the shared infection routes and high co-infection rates, integration of HIV and HCV services is highly recommended (WHO 2014b). Finally, long-term HIV and HCV care for drug users may become increasingly necessary as more infected individuals now live longer.
Although the five Asian countries have made impressive progress in their responses to drug use and HIV problems, information is lacking on the availability, access, and coverage regarding the additional interventions in the nine comprehensive approaches for drug use suggested by WHO, including prevention and treatment of sexually transmitted infections (STI); condom use programs for IDUs and partners; targeted information, education and communication, hepatitis diagnosis, treatment (hepatitis A, B, and C) and vaccination (hepatitis A and B), and tuberculosis (TB) prevention, diagnosis, and treatment. Even in the areas reported in this article, most data from these five countries are sketchy, fragmentary, or outdated; few good and recent studies are available. National-level epidemiological data are almost completely absent or outdated, particularly the drug use data, which are often based on specific samples or governmental registry. The rapid social, economic, cultural, and political transformations are adding to the complexity of drug use patterns and associated drug-related problems in Asia and worldwide. In order to guide effective country-level responses to drug abuse and related HIV/HCV infections, improved surveillance and monitoring systems are needed to provide updated information on drug use (injection and non-injection) rates, prevalence of HIV and HCV among drug users, and the type of prevention and treatment services available as well as the degree of service coverage.
References
Aceijas C, Rhodes T (2007) Global estimates of prevalence of HCV infection among injecting drug users. Int J Drug Policy 18(5):352–358
Aceijas C, Stimson GV, Hickman M, Rhodes T; United Nations Reference Group on HIV/AIDS Prevention and Care among IDU in Developing and Transitional Countries. (2004). Global overview of injecting drug use and HIV infection among injecting drug users. AIDS, 19; 18(17):2295–303
aidsdatahub (2015) www.aidsdatahub.org. Accessed 2015
Bachireddy C, Bazazi AR, Kavasery R, Govindasamy S, Kamarulzaman A, Altice FL (2011) Attitudes toward opioid substitution therapy and pre-incarceration HIV transmission behaviors among HIV-infected prisoners in Malaysia: Implications for secondary prevention. Drug Alcohol Depend 116(1–3):151–157
Baldwin S (2013) Emerging from a black box: Drug policymaking in Vietnam. In: Rahman F, Crofts N (eds) Drug law reform in East and Southeast Asia. Lexington Books, Lanham, MD, pp. 211–219
Bao YP, Liu ZM (2009) Systematic review of HIV and HCV infection among drug users in China. Int J STD AIDS 20(6):399–405
Bazazi AR, Zelenev A, Fu JJ, Yee I, Kamarulzaman A, Altice FL (2014) High prevalence of non-fatal overdose among people who inject drugs in Malaysia: Correlates of overdose and implications for overdose prevention from a cross-sectional study. Int J Drug Policy 26(7):675–681. doi:10.1016/j.drugpo.2014.11.010
Bergenstrom, A., Andreeva, V., & Reddy, A. (2013). Overview of epidemiology of injection drug use and HIV in Asia 2013. Retrieved from www.unodc.org/documents/southeastasiaandpacific//poster/Regional_overview_of_IDU_and_HIV_in_Asia_final_3_Jun_2013.pdf
Bontell I, Cuong d D, Agneskog E, Diwan V, Larsson M, Sönnerborg A (2012) Transmitted drug resistance and phylogenetic analysis of HIV CRF01_AE in Northern Vietnam. Infect Genet Evol 12(2):448–452
Chakrapani V, Velayudham J, Shunmugam M, Newman PA, Dubrow R (2014) Barriers to antiretroviral treatment access for injecting drug users living with HIV in Chennai, South India. AIDS Care 26(7):835–841
Colfax G, Santos GM, Chu P, Vittinghoff E, Pluddemann A, Kumar S, Hart C (2010) Amphetamine-group substances and HIV. Lancet 376(9739):458–474. doi:10.1016/S0140-6736(10)60753-2
Control VAoHA (2014) The annual review of HIV/AIDS control and prevention in 2013 and action plan in 2014. Hanoi: Ministry of Health
Degenhardt L, Bucello C, Mathers B, Briegleb C, Ali H, Hickman M (2011) Mortality among regular or dependent users of heroin and other opioids: a systematic review and meta-analysis of cohort studies. Addiction 106:32–51
Degenhardt L, Whiteford HA, Ferrari AJ, Baxter AJ, Charlson FJ, Hall WD, et al. (2013) Global burden of disease attributable to illicit drug use and dependence: Findings from the Global Burden of Disease Study 2010. Lancet 382(9904):1564–1574
Department of AIDS Control. (2014). India department of aids control ministry of health & family welfare annual report 2011–12. Retrieved from http://www.naco.gov.in/upload/2014%20mslns/NACO_English%202013-14.pdf
Fu JJ, Bazazi AR, Altice FL, Mohamed MN, Kamarulzaman A (2012a) Absence of antiretroviral therapy and other risk factors for morbidity and mortality in Malaysian compulsory drug detention and rehabilitation centers. PLoS One 7(9):e44249
Fu Y, Qin W, Cao H, Xu R, Tan Y, Lu T, Wang H, Tong W, Rong X, Li G, Yuan M, Li C, Abe K, Lu L, Chen G (2012b) HCV 6a prevalence in Guangdong province had the origin from Vietnam and recent dissemination to other regions of China: phylogeographic analyses. PLoS One 7(1):e28006
Gill JS, Abdul Rashid R, Ong Hui K, Jawan R (2011) History of illicit drug use in Malaysia - a review. Int J AddicSci 1(1):1–6
Government of India, Ministry of Health & Family Welfare, National AIDS Control Organisation (2014) Annual report 2013–2014. Author, New Delhi, India
Hammett TM, Des Jarlais D, Johnston P, Kling R, Ngu D, Liu W, Chen Y, Van LK, Donghua M (2007) HIV prevention for injection drug users in China and Vietnam: policy and research considerations. Glob Public Health 2(2):125–139
Hammett TM, Des Jarlais DC, Kling R, Kieu BT, McNicholl JM, Wasinrapee P, et al. (2012) Controlling HIV epidemics among injection drug users: Eight years of Cross-Border HIV prevention interventions in Vietnam and China. PLoS One 7(8):e43141
Human Rights Watch. (2010). Where darkness knows no limits: Incarceration, ill-treatment, and forced labor as drug rehabilitation in China. Retrieved from http://www.hrw.org/en/reports/2010/01/07/where-darkness-knows-no-limits
Jia Z, Liu Z, Chu P, McGoogan JM, Cong M, Shi J, Lu L (2015) Tracking the evolution of drug abuse in China, 2003-10: A retrospective, self-controlled study. Addiction 110(Suppl 1):4–10
Joint United Nations Programme on HIV/AIDS (UNAIDS). (2014). UNAIDS report shows that 19 million of the 35 million people living with HIV today do not know that they have the virus. Retrieved from http://www.unaids.org/sites/default/files/web_story//20140716_ PR_GapReport_en.pdf
Kamarulzaman A (2009) Impact of HIV prevention programs on drug users in Malaysia. J Acquir Immune Defic Syndr 52(Suppl 1):S17–S19
Kamarulzaman A, McBrayer JL (2015) Compulsory drug detention centers in East and Southeast Asia. Int J Drug Policy 26(Suppl 1):S33–S37
Kulsudjarit K (2004) Drug problem in Southeast and Southwest Asia. Ann N Y Acad Sci 1025:446–457
Lan YC, Yang YC, Chi TW, Chen KH, Wang RY, Chiang YC, Huang CL, Ho IK, Hser YI (2014) HCV Genotype distribution among injection drug users in Taiwan. In: CPDD 76th Annual Meeting • San Juan. Rico, Puerto
Liu J, Zhang C (2011) Phylogeographic analyses reveal a crucial role of Xinjiang in HIV-1 CRF07_BC and HCV 3a transmissions in Asia. PLoS One 6(8):e23347
Mathers BM, Degenhardt L, Phillips B, Wiessing L, Hickman M, Strathdee SA, et al. (2008) Global epidemiology of injecting drug use and HIV among people who inject drugs: A systematic review. Lancet 372(9651):1733–1745
Mathers BM, Degenhardt L, Bucello C, Lemon J, Wiessing L, Hickman M (2013) Mortality among people who inject drugs: a systematic review and meta-analysis. Bull World Health Organ 91:102–123
Mehta SH, Vogt SL, Srikrishnan AK, Vasudevan CK, Murugavel KG, Saravanan S, Anand S, Kumar MS, Ray SC, Celentano DD, Solomon S, Solomon SS (2010) Epidemiology of hepatitis C virus infection & liver disease among injection drug users (IDUs) in Chennai, India. Indian J Med Res 132:706–714
Ministry of Health Malaysia (2015). Global AIDS response progress report Malaysia 2015. Retrieved from http://www.unaids.org/sites/default/files/country/documents/MYS_narrative_report_2015.pdf
Ministry of Health of Vietnam. (2015). Optimizing Viet Nam’s HIV response: an investment case Retrieved from http://www.unaids.org/sites/default/files/en/dataanalysis/knowyourresponse/countryprogressreports/2012countries/ce_VN_Narrative_Report.pdf
Mohamed NA, Zainol Rashid Z, Wong KK, Abdullah SA, Rahman M (2013) Hepatitis C genotype and associated risks factors of patients at University KebangsaanMalaysia Medical Centre. Pak J Med Sci 29(5):1142–1146
Mohd Hanafiah K, Groeger J, Flaxman AD, Wiersma ST (2013) Global epidemiology of hepatitis C virus infection: New estimates of age-specific antibody to HCV seroprevalence. Hepatology 57(4):1333–1342
National AIDS Control Organization (NACO). (2012). Annual report 2014–15. Retrieved from http://www.naco.gov.in/upload/Publication/Annual%20Report/Annual%20report%202012-13_English.pdf
National AIDS Control Organization (NACO). (2015). Part-B national aids control organization annual report 2014–15. Retrieved from http://www.naco.gov.in/upload/2015% 20MSLNS/Annual%20report%20_NACO_2014-15.pdf
National Committee for AIDS, Drugs and Prostitution Prevention and Control of Vietnam. (2012). Viet Nam AIDS response progress report. Retrieved from http://www.unaids.org/en/dataanalysis/knowyourresponse/countryprogressreports/2012countries/ceVN Narrative Report.pdf
National Committee for AIDS, Drugs and Prostitution Prevention and Control of Vietnam. (2014). Vietnam AIDS response progress report 2014. Retrieved from http://www.aidsdatahub.org/sites/default/files/publication/Vietnam narrative report 2014.pdf
National Health and Family Planning Commission of the People’s Republic of China (2014). 2014 China AIDS response progress report Retrieved from http://www.unaids.org/sites/default/files/documents/CHN_narrative_report_2014.pdf
National Health and Family Planning Commission of the People’s Republic of China (2015). 2015 China AIDS response progress report Retrieved from http://www.unaids.org/sites/default/files/country/documents/CHN_narrative_report_2015.pdf
Nelson PK, Mathers BM, Cowie B, Hagan H, Des Jarlais D, Horyniak D, Degenhardt L (2011) Global epidemiology of hepatitis B and hepatitis C in people who inject drugs: Results of systematic reviews. Lancet 378(9791):571–583
Ngadiman, S., Suleiman, A., Taib, S., & Yuswan, F. (2014). Global AIDS response progress report 2014: Malaysia Retrieved from http://www.unaids.org/sites/default/files/en/dataanalysis/knowyourresponse/countryprogressreports/2014countries/MYS_narrative_report_2014.pdf
Nguyen VTT, McLaws M-L, Dore GJ (2007) Prevalence and risk factors for hepatitis C infection in rural north Vietnam. Hepatol Int 1(3):387–393
Pawar A, Rajalakshmi AK, Upadhyay RP (2015) Pentazocine use among people who inject drugs in India. Asian J Psychiatr 16:3–6
Pearshouse R (2009) “Patients, not criminals”? An assessment of Thailand’s compulsory drug dependence treatment system. HIV AIDS Policy Law Rev 14(1):11–17
Peng J, Lu Y, Liu W, Zhu Y, Yan X, Xu J, Wang X, Wang Y, Liu W, Sun Z (2015) Genotype Distribution and Molecular Epidemiology of Hepatitis C Virus in Hubei, Central China. PLoS ONE 10(9):e0137059
Petersen Z, Myers B, van Hout MC, Pluddemann A, Parry C (2013) Availability of HIV prevention and treatment services for people who inject drugs: Findings from 21 countries. Harm Reduct J 10:13
Piao HX, Yang AT, Sun YM, Kong YY, Wu XN, Zhang YZ, Ding B, Wang BE, Jia JD, You H (2014) Increasing newly diagnosed rate and changing risk factors of HCV in Yanbian Prefecture, a high endemic area in China. PLoS ONE 9(1):e86190
Pybus OG, Barnes E, Taggart R, Lemey P, Markov PV, Rasachak B, Syhavong B, Phetsouvanah R, Sheridan I, Humphreys IS, Lu L, Newton PN, Klenerman P (2009) Genetic history of hepatitis C virus in East Asia. J Virol 83(2):1071–1082
Ray, R. (2004). The extent, pattern and trends of drug abuse in India: National Survey Ministry of Social Justice and Empowerment. Govt. of India & United Nations Office on Drugs and Crime, Regional Office for South Asia. Retrieved from http://www.unodc.org/pdf/india/presentations/india_national_survey_2004.pdf
Ronsard L, Lata S, Singh J, Ramachandran VG, Das S, Banerjea AC (2014) Molecular and Genetic Characterization of Natural HIV-1 Tat Exon-1 Variants from North India and Their Functional Implications. PLoS One 9(1):e85452
Saidel TJ, Jarlais DD, Peerapatanapokin W, Dorabjee J, Singh S, Brown T (2003) Potential impact of HIV among IDU on heterosexual transmission in Asian settings: Scenarios from the Asian Epidemic Model. Int J Drug Policy 14:63–74
Solomon SS, Mehta SH, Srikrishnan AK, Solomon S, McFall AM, Laeyendecker O, et al. (2015) Burden of hepatitis C virus disease and access to hepatitis C virus services in people who inject drugs in India: A cross-sectional study. Lancet Infect Dis 15(1):36–45
Stumpf MPH, Pybus OG (2002) Genetic diversity and models of viral evolution for the hepatitis C virus. FEMS Microbiol Lett 214:143–152
Sullivan SG, Wu Z (2007) Rapid scale up of harm reduction in China. Int J Drug Policy 18(2):118–128
Taiwan CDC. (2015). Health topics. Retrieved from http://www.cdc.gov.tw/english/page.aspx?treeid=e79c7a9e1e9b1cdf&nowtreeid=6bb9113c9e323e98
Tanguay P, Kamarulzaman A, Aramrattana A, Wodak A, Thomson N, Ali R, Vumbaca G, Lai G, Chabungbam A (2015) Facilitating a transition from compulsory detention of people who use drugs towards voluntary community-based drug dependence treatment and support services in Asia. Harm Reduct J 12:31
Tee KK, Pybus OG, Li XJ, Han X, Shang H, Kamarulzaman A, Takebe Y (2008) Temporal and spatial dynamics of human immunodeficiency virus type 1 circulating recombinant forms 08_BC and 07_BC in Asia. J Virol 82(18):9206–9215
Tran, T. T. (2008). HIV-1 genotype and vertical transmission in northern Vietnam (Thesis at the Karolinska Institutet). Retrieved from https://openarchive.ki.se/xmlui/handle/10616/39900
UNAIDS (2014) The Gap Report. Author, Geneva, Switzerland
UNAIDS (2015) Global AIDS response progress report. Author, Malaysia
UNODC. (2011). World drug report 2011. New York: United Nations. Retrieved from https://www.unodc.org/unodc/en/data-and-analysis/WDR-2011.html
UNODC. (2013). ATS second-most popular illicit drug in Viet Nam, heroin still no 1 Retrieved from https://www.unodc.org/southeastasiaandpacific/en/vietnam/2013/07/wdd/story.html
UNODC. (2014). World drug report 2014. New York: United Nations. Retrieved from https://www.unodc.org/documents/wdr2014/World_Drug_Report_2014_web.pdf
UNODC. (2015a). World drug report 2015. (United Nations publication, Sales No. E.15.XI.6). New York: Author
UNODC. (2015b). Southeast Asia and Pacific: HIV and AIDS Retrieved from http://www.unodc.org/southeastasiaandpacific/en/topics/hiv-and-aids/index.html
UNODC Drug Dependence. (2014). Viet Nam is discussing voluntary community based treatment and care [news release, June 9, 2014]. Retrieved from http://www. unodc.org/southeastasiaandpacific/en/vietnam/2014/06/drug-workshop/story.html
Wang L, Guo W, Li D, Ding Z, McGoogan JM, Wang N, et al. (2015a) HIV epidemic among drug users in China: 1995-2011. Addiction 110(Suppl 1):20–28
Wang Y, Liang Y, Feng Y, Wang B, Li Y, Wu Z, et al. (2015b) HIV-1 prevalence and subtype/recombinant distribution among travelers entering China from Vietnam at the HeKou port in the Yunnan province, China, between 2003 and 2012. J Med Virol 87(9):1500–1509
Wherley S, Chatterjee S (2015) India’s growing problem of injecting drug misuse. BMJ 350:h397
World Health Organization (WHO). (2009). Assessment of compulsory treatment of people who use drugs in Cambodia, China, Malaysia and Viet Nam: An application of selected human rights principles. Manila: Author. Retrieved from http://www.wpro.who.int/publications/docs/FINALforWebMar17 Compulsory Treatment.pdf
World Health Organization (WHO). (2014a). The global health sector strategy on HIV/AIDS 2011–2015: An interim review of progress. Retrieved from http://apps.who.int/iris/bitstream/10665/112790/1/9789241507295_eng.pdf
World Health Organization (WHO) (2014b). Guidelines for the screening, care and treatment of persons with hepatitis C infection. Retrieved from http://apps.who.int/iris/bitstream/10665/111747/1/9789241548755_eng.pdf?ua=1&ua=1
Wu Z, Wang Y, Detels R, Bulterys M (2015) Towards ending HIV/AIDS among drug users in China. Addiction 110(Suppl 1):1–3
Yang C-H, Yang S-Y, Shen M-H, et al. (2008) The changing epidemiology of prevalent diagnosed HIV infections in Taiwan, 1984–2005. Int J Drug Policy 19:317–323
Yu WJ, Tsay WI, Li JH (2013) Current status of substance abuse and HIV in Taiwan. J Food Drug Anal 21(4):S27–S32
Zhang, S. X., & Chin, K. L. (2016). A people’ war: China’ struggle to contain its illicit drug problem. Improving Global Drug Policy: Comparative perspective and UNGASS 2016. Retrieved from: http://www.brookings.edu/~/media/Research/Files/Papers/2015/04/global-drug-policy/A-Peoples-War-final.pdf?la=en
Zhang F, Dou Z, Ma Y, Zhang Y, Zhao Y, Zhao D, et al. (2011) Effect of earlier initiation of antiretroviral treatment and increased treatment coverage on HIV-related mortality in China: a national observational cohort study. Lancet Infect Dis 11(7):516–524
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This study was funded by the National Institute on Drug Abuse (P30DA016383 & R13 DA035084; PI:Hser), and Universiti Sains Malaysia (Grant No. 1002/CDADAH/910402; PI: Vicknasingam).
Conflict of Interest
All authors declare no conflict of interest.
Ethical approval.
This article does not contain any studies with human participants or animals performed by any of the authors.
Rights and permissions
About this article

Cite this article
Hser, YI., Liang, D., Lan, YC. et al. Drug Abuse, HIV, and HCV in Asian Countries. J Neuroimmune Pharmacol 11, 383–393 (2016). https://doi.org/10.1007/s11481-016-9665-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11481-016-9665-x