
Abstract
Internet Gaming Disorder (IGD) has been introduced as an emerging mental health condition requiring further study. Associations between IGD and gaming presence (i.e., absorption in the virtual environment) have been implied. The aim of the present study was twofold: (a) to evaluate the extent to which presence contributes to IGD severity and (b) to examine longitudinal differences in IGD according to the initial level of presence experienced. The participants comprising 125 emerging adults aged 18 to 29 years completed either (i) three face-to-face assessments (1 month apart, over 3 months) or (ii) a cross-sectional, online assessment. IGD was assessed with the 9-item IGD Scale Short Form and presence was assessed using the Presence Questionnaire. Regression and latent growth modeling analyses were conducted. Findings demonstrated that the level of gaming presence related to IGD severity but not to linear change in severity over a 3-month period. The study shows that emergent adults who play Internet games may be at a high risk of IGD given a more salient sense of being present within the gaming environment. Clinical implications considering prevention and intervention initiatives are discussed.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Excessive online gaming use is a social and mental health phenomenon with implications for emerging adults (ages 18–29; Kuss and Griffiths 2011; Stavropoulos et al. 2016a; Kuss et al. 2012). Internet Gaming Disorder (IGD) was introduced as a condition for further study in the most recent (fifth) edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5; APA 2013). The proposed disorder has been defined as the continuous and ongoing use of playing online games leading to significant impairment or distress (APA 2013). However, there are a number of online game genres that may impact on IGD susceptibility, with Massively Multiplayer Online (MMO) games being consistently associated with IGD (Lemmens and Hendriks 2016; Stetina et al. 2011; Ng and Wiemer-Hastings 2005). MMO games are online worlds that constantly evolve in real time, where players may interact within the game via their virtual characters (avatars), and potentially addressing shared group and/or personal goals (Stetina et al. 2011). Progressive challenges are intertwined with a well-developed reward schedule, enriched with opportunities for online socialization and character development (Thorens et al. 2012). These inherent MMO factors within the game structure appear to contribute to their absorbing nature (Lemmens and Hendriks 2016; Stetina et al. 2011; Ng and Wiemer-Hastings 2005; Thorens et al. 2012).
Psychosocial factors that have been proposed as IGD risks range from those that are identity-related (e.g., role playing, identity-building, and exploration; Kuss et al. 2012) to those involving self-esteem drives (Bessière et al. 2007; King and Delfabbro 2014; Beard and Wickham 2016; Yee 2006; Beard et al. 2017). These individual factors are important for understanding both IGD phenomenology as well as understanding the critical aspects of human-computer interaction that have emerged in relation to Internet gaming (Anderson et al. 2016). Although prior studies have indicated that immersion in the online environment is related to more problematic play (Wood et al. 2004), exploration into the degree of presence in the game is nascent (Milani et al. 2017).
Presence is defined as a psychological state, or a subjective perception, in which an individual may experience the game context as real, feeling as “being there” instead of “being here” (Huang et al. 2011). Therefore, presence within MMOs may serve as a way to transition gamers into a parallel state wherein their perception of reality might fade into the background of their consciousness (Stavropoulos et al. 2013; Kaczmarek and Drążkowski 2014). Within the gaming context, subjective experiences of presence are thought to progressively strengthen the sense of the game world being real, which could in turn increase online gaming involvement (Stetina et al. 2011; Huang et al. 2011; Kaczmarek and Drążkowski 2014). This concurs with cross-sectional findings indicating presence as a factor in Internet abuse (Kuss et al. 2012; Huang et al. 2011; Kaczmarek and Drążkowski 2014). Within the context of online play, the repeated experiences of presence can result in a feeling of belonging to the game environment (Stavropoulos et al. 2013). This sense of belonging and “being there” may act as an incentive to increase and maintain online activity, thus resulting in excessive use (Stavropoulos et al. 2013; Griffiths 2005).
Masten’s Risk and Resilience Framework (RRF) has previously been adapted to investigate IGD phenomenology (Griffiths 2005; Masten 2001) and used to identify factors that might contribute to the adaptive or maladaptive use of games. This framework has also been applied to other technological addictions, as it has been recognized that excessive Internet use alone does not indicate addiction (i.e., an individual can be highly engaged, but not addicted; Stavropoulos et al. 2016b). The RRF suggests that behaviors constantly fluctuate across the pathological and/or non-pathological range, with their intensity being defined by the longitudinal interplay between individual (e.g., game genre preference; Eichenbaum et al. 2015; Elliott et al. 2012) and contextual (i.e., offline or online) effects (Masten 2001; Douglas et al. 2008). Given the background of immersion as a risk factor for problematic play, the notion of virtual presence in the game is examined in the present study as a potential IGD risk (Faiola et al. 2013).
These issues are particularly salient for emerging adults (i.e., those aged 18–29 years) due to specific developmental goals and needs present during this period of transition from adolescence to full adulthood (Kuss and Griffiths 2011; Stavropoulos et al. 2016a; Kuss et al. 2012). Unsupervised Internet use, along with the lack of matured adult-type roles (prominent through the developmental period of emerging adulthood), appears to pose gamers at higher risk of IGD (Kaczmarek and Drążkowski 2014; Scott and Porter-Armstrong 2013; Hendriks 1990; Stanley 2008). The identification of emerging adulthood as a vulnerable developmental period is consistent with findings in other domains of substance and behavioral addictions (Kaczmarek and Drążkowski 2014; Scott and Porter-Armstrong 2013; Hendriks 1990; Stanley 2008). Accordingly, the present study will seek to build upon the current empirical understanding of IGD within this high-risk population (i.e., emerging adult MMO gamers).
Although prior literature has identified immersion as a risk factor for IGD, the longitudinal association of online presence and IGD has not been explicitly examined (Milani et al. 2017). This preliminary study utilized an RRF perspective to assess the effect of presence on IGD symptomology in a high-risk population of young adults who play MMO games. More specifically, presence was explored as it related to IGD both (i) cross-sectionally and (ii) as a predictor of IGD across a 3-month period.
Method
Participants
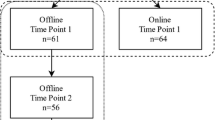
The sample comprised 125 MMO players aged 18–29 years old (64 online, cross-sectional respondents, Mage = 23.34, SD = 3.39, Males = 49, 77.6%; 61 offline, face-to-face, longitudinal, Mage = 23.02, SD = 3.43, Males = 47, 75.4%). Online and face-to-face data (i.e., time-point 1 [T1]) were combinedFootnote 1 in the cross-sectional analyses and face-to-face longitudinal dataFootnote 2 (i.e., time-points 1, 2, 3 [T1, T2, T3]; see Fig. 1). The data were then analyzed separately to assess presence as a predictor of IGD over a 3-month period (in consensus with the frequently used time bracket of assessing short-term changes in other types of addiction forms; D’Amico et al. 2015). Sociodemographic characteristics of the sample are presented in Table 1. The estimated maximum sampling error with a size of 125 is 8.77% and therefore, within the acceptable limits (Salant et al. 1994).

Participant pool
Measures
A battery of scales and a series of demographic information questions were applied.Footnote 3
The Internet Gaming Disorder Scale–Short Form 9 (IGDS-SF9) was used to assess IGD severity. The IGDS-SF9 includes nine items reflecting the DSM-5 IGD criteria (e.g., “Do you systematically fail when trying to control or cease your gaming activity?”; APA 2013; Pontes and Griffiths 2015) Items are addressed on a 5-point Likert scale (1 = never to 5 = very often) yielding total scores ranging from 9 to 45 with higher scores indicating higher IGD severity. Internal reliability in the present study was high, with a Cronbach’s α of .92.
The Presence Scale was used to assess online presence (Faiola et al. 2013). This includes presence (Griffiths 2005). The scale comprises 10 self-report items which focus on the participants’ experience in the virtual environment (e.g., “I feel like all my senses are engaged in the environment”). Items are rated on a 5-point Likert scale (1 = very little to 5 = very much). Item scores are added resulting to a range between 10 and 50, with higher scores indicating higher levels of perceived presence. Internal reliability in the present study was high, with a Cronbach’s α of .82.
Procedure
Ethics approval was received from the research team’s university ethics committee. Participants were recruited in the general community using both offline methods (i.e., information flyers) and online methods (i.e., e-mail, social media).Footnote 4 The face-to-face, longitudinal component of the study was conducted over a 3-month period, with the three time-point assessments completed between June 2016 and September 2016. Data collection was identical between the three time-points, and participants’ data were matched using a re-identifiable code.
For online collection, eligible individuals interested in participating and unable or unwilling to attend face-to-face testing sessions were invited to register with the study via a SurveyMonkey link available on MMO websites and forums (i.e., http://www.ausmmo.com.au). The link directed them to the plain language information statement where they had to digitally provide informed consent (by clicking a button).
Results
Linear regression analyses were conducted to assess cross-sectional presence scores predicting IGD severity. Bootstrapping on the minimum recommended level of 1000 was applied (Berkovits et al. 2000). Results indicated that the slope of the regression line was statistically significantFootnote 5 (F(1, 123) = 31.54, p < .001). Regarding the overall effect, 20% of the variance of IGD scores was explained by gaming presence (R2 = 0.204). The standardized coefficient (β) indicated that a standard deviation increase in presence was associated with a 0.45 standard deviation increase in IGD (b = 0.42, SE (b) = 0.7, β = 0.45, t = 5.61, p < .001).
Second, a latent growth model (LGM) of IGD behaviors over the three time-points (face-to-face data available only) was calculated using robust maximum likelihood estimation with Mplus software, Version 6.12 (Muthen and Muthen 2010). This approach allowed IGD behaviors at different time-points to be evaluated so that the mean and the variance of the intercept (the initial status of IGD behaviors as measured at T1) and the growth function (change of IGD behaviors across the time-points) were produced. IGD behaviors at the three time-points were fixed at 0, 1, and 2, respectively, to define a linear growth model with equidistant time-points. As part of the parameterization, the intercepts of IGD behaviors at the three time-points were fixed at 0, and their residual variances were freely estimated. The chi-square goodness of fitFootnote 6 (discrepancy index), the root mean square error of approximationFootnote 7 (RMSEA-discrepancy index), the comparative fit indexFootnote 8 (CFI-incremental fit index), the Tucker Lewis indexFootnote 9 (TLI-incremental fit index), the Akaike information criterionFootnote 10 (AIC-information theory goodness of fit), and the Bayesian information criterionFootnote 11 (BIC-information theory goodness of fit) were calculated in order to determine overall model fit. Second, the presence score at T1 was added as a time invariant covariate (predictor) of the IGD intercept and slope. Model fit indices were compared between the two models. Missing values were addressed with full information maximum likelihood (Schafer and Graham 2002) (Table 2).
A path diagram of the final LGM model is shown in Fig. 2. This includes the latent growth curve with intercept (I), linear parameter (S), and the time invariant covariate of presence (pqtott). The observed variables were the repeated measures of IGD behaviors, obtained at the three time-points: Initial (T1), 1 month after the baseline measurement (T2) and 2 months after the initial assessment (T3).

Mean and standard deviation ratings for IGD severity at 0, 1, and 2 months were 19.49 (7.02), 18.71 (6.84), and 17.93 (5.91), respectively. The growth curve model was conducted twice, with presence as a time invariant covariate, and without presence. Analyses indicated that the model which included presence provided better fit than the model without (AIC and BIC values decreased; see Table 2). Presence at T1 failed to predict the IGD-slope; however, it significantly associated with the IGD intercept (b = 0.369; p < .001). Therefore, presence significantly predicted the initial IGD scores, but it was not predictive of change over a 3-month period
Discussion
The present study utilized the RRF, enriching it with key factors from the IGD literature, to explore presence as an IGD risk factor. In line with the relevant findings, MMO gamers who experienced higher presence presented with higher IGD scores (Stavropoulos et al. 2013). The contribution of presence to IGD was notable, as it accounted for over 20% of IGD variance. These empirical findings substantiate presence as an important IGD risk factor.
Although cross-sectional analyses did indicate presence as an IGD risk factor, the growth model did not support the initial levels of presence related to change in IGD scores over the 3-month period. This may either indicate that (a) other factors (e.g., cognitive or personality traits of the gamer) influence the relationship between IGD and presence, or that (b) the study duration needs to be more prolonged for the relationship to be apparent. Consequently, the results of the present study should be considered as a first step examining the relationship between presence and IGD. Future studies may consider a parallel growth model assessing the level of change of presence in relation to the level of change of IGD to examine the relationship between the relative slopes of IGD and presence over time. Due to statistical limitations related to the sample size of the present study (i.e., model convergence), such a model could not be examined here. Nevertheless, the present findings may have important clinical implications for MMO gamers presenting with IGD.
A strong perception of the online world as real may increase the time spent for gaming, and thus magnify potential problems in real life (e.g., education/occupation underperformance/problems; Anderson et al. 2016). Furthermore, the experience of the gamer as being present in-game should be therapeutically considered because IGD associates with known motivational contributors (e.g., escapism and immersion; Kuss et al. 2012; Bessière et al. 2007; Yee 2006). Presence and immersion within virtual worlds will continue to dominate the gaming landscape via the introduction of more immersive technologies (e.g., virtual reality, realistic in-game graphics; Bessière et al. 2007). It might be important that clinical work further explores what impact this may have on an individuals’ desire to engage with MMO games, and to what extent.
The findings and implications should be considered in relation to the limitations of the study. First, the self-selected sample was mostly male; therefore, the results from a non-representative sample cannot be generalized to female gamers or gamers more generally. In addition, the longitudinal design spanned only a few months, which may not be enough time to provide insight into the associations examined. Similarly, potentially confounding factors related to game use were not addressed (e.g., gaming time). Thirdly, the data were self-report and subject to many well-known biases (including memory recall and social desirability). Despite these limitations, the present study had significant strengths, such as combining online and FTF participants, cross-sectional and longitudinal analyses, and emphasized and an under-researched high-risk population (i.e., emerging adult MMO gamers). In such a context, future research could benefit from the exploration of the over-time interplay of other game-related risk factors, such as flow or user-avatar associations. Furthermore, potential protective factors related to the gamer and/or their real context (i.e., peer and family relationships) could also be explored, allowing for a more holistic understanding of IGD.
Notes
To ensure that there were no significant differences between the online and face-to-face samples considering their demographic and Internet use characteristics, as well as the variables used in the present study, independent sample t tests and chi-square analyses were conducted. Findings did not indicate any significant differences in regard to gender (x2 = .21, df = 1, p = .89), the type of game genre (i.e., MMOs without role development vs MMOs with role development) played (x2 = 2.59, df = 1, p = .61), the age of the participants (t = − .54, df = 120, p = .59), their years of internet use (t = 2.35, df = 122, p = .06), and their reported level of online presence (t = − 1.595, df = 119, p = .113). Therefore, online and face-to-face data (i.e., TP1) were combined (i.e., analyzed together) for the cross-sectional analyses.
The longitudinal design was assessed for attrition. Assessments’ frequency for each participant varied within a range of 1–3 (Maverage = 2.57). T1 comprised 61 participants, T2 comprised 56 participants (8.20% attrition) and T3 comprised 43 participants (29.51% attrition). In line with literature recommendations, attrition, in relation to the studied variables, was assessed using Little’s missing completely at random (MCAR) test, which was insignificant37 (MCAR X2 = 1715.79, p = 1.00; Little and Rubin 2014). In order to avoid list-wise deletion, which would reduce the sample’s power, maximum likelihood imputation (five times) of values was applied (Gold and Bentler 2000).
To ascertain that the data collection type did not confound the association between presence and IGD scores, the linear regression analysis (bootstrapping at 1000) of presence predicting IGD was additionally conducted separately for the online [F(1, 63) = 10.12, p = .003, R2 = .17, b = 0.44, SE (b) = 0.14, t = 3.18, p = .003] and the face to face [F(1, 60) = 14.59, p = .000, R2 = .20, b = 0.38, SE (b) = 0.10, t = 3.82, p = .000] data resulting to similar findings with those of the unified sample. Furthermore, a moderation analysis was conducted using the process software (Hayes 2013). The model examined the potential moderating effect of the data collection type (0 = online, 1 = face-to-face) on the association between presence (IV) and IGD (DV). Results indicated that presence and the type of data collection did not significantly interact in predicting IGD score [b = .06, SE = 0.17, t(543) = .34, p = .731, (lower level confidence interval = − .273 upper level confidence interval = .388)].
The current study is part of a wider project (redacted for review) that addresses the interplay between individual, Internet, and proximal context factors in the development of Internet Gaming Disorder symptoms among emerging adults. Instruments used in the data include the following: (1) Internet Gaming Disorder 9-Short Form (Pontes and Griffiths 2015); (2) Beck Depression Inventory–2nd edition (21 items; Beck et al. 1996); (3) Beck Anxiety Inventory (21 items; Beck and Steer 1990); (4) Hikikomori-Social Withdrawal Scale (five items; Teo et al. 2015); (5) Attention Deficit Hyperactivity Self-Report Scale (18 items; Kessler et al. 2005); (6); 10-Item Personality Inventory (Gosling et al. 2003); (7) The Balanced Family Cohesion Scale (seven items; Olson 2000); (8) Presence Questionnaire (10 items; Ratan and Hasler 2010); (9); Online Flow Questionnaire (five items; Chen et al. 2000); (10) Self-Presence Questionnaire (Ratan and Hasler 2010); (11) The Gaming-Contingent Self-Worth Scale (12 items; Beard and Wickham 2016); and (12) Demographic and Internet Use Questions. The battery of questionnaires was utilized for both online and face-to-face data collection. The use of the fitness tracker (Fitbit flex) was used only for face-to-face data collection. Data have not been used in any previous published studies.
In line with the approval received by the ethics committee of (redacted for review), the flyers (a) indicated that participants were required to participate on three separate measurement occasions approximately 1 month apart; (b) included an email address to contact the investigators; and (c) clearly described the process and stages of the data collection (face-to-face and online). MMO and MMORPG players, aged between 18 and 29 years old, interested in the study received the Plain Language Information Statement (PLIS). The PLIS clearly indicated that participation was voluntary and that participants could independently decide to withdraw from the study at any point. Individuals who choose to participate were required to provide informed consent.
The model is regarded as acceptable if the chi-square is not significant. That is, the observed covariance matrix is similar to the matrix predicted by the model. However, this index is disregarded when the sample size exceeds 200 and in the cases that the assumption of multivariate normality is violated.
The RMSEA represents the square root of the average or mean of the covariance residuals (the differences between corresponding elements of the observed and predicted covariance matrix). Zero represents a perfect fit. Literature indicates that RMSA should be less than .08 (Browne and Cudeck 1992)—and ideally less than .05 (Steiger 1990). Alternatively, the upper confidence interval of the RMSEA should not exceed .08 (Hu and Bentler 1998).
The CFI compares the examined model of interest with the null or independence model (variables are assumed to be uncorrelated). In this context, the CFI represents the extent to which the model of interest is better than is the independence model. Values that approach 1 indicate acceptable fit. CFI is not too sensitive to sample size (Fan et al. 1999).
The TLI is computed by the division of the chi-square for the target model and the null model by their corresponding df vales (relative chi-squares), which are then subtracted from each other, and their difference is finally divided by the relative chi-square for the null model minus 1. According to Marsh et al. (1988), the TLI is relatively independent of sample size and over .90 or over .95 are considered acceptable (Hu and Bentler 1998).
The AIC is regarded as an information theory goodness of fit measure—applicable when maximum likelihood estimation is used (Anderson et al. 1998). This index is used to compare different models. Like the chi-square index, the AIC also reflects the extent to which the observed and predicted covariance matrices differ from each other. Models that generate the lowest values are optimal.
The BIC is similar to the AIC and expresses the log of a Bayes factor of the target model compared to the saturated model and penalizes against complex models. Furthermore, a penalty against small samples is included in BIC calculation (Raftery 1995).
References
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders. Arlington: American Psychiatric Publishing.
Anderson, D., Burnham, K., & White, G. (1998). Comparison of Akaike information criterion and consistent Akaike information criterion for model selection and statistical inference from capture-recapture studies. Journal of Applied Statistics, 25(2), 263–282.
Anderson, E. L., Steen, E., & Stavropoulos, V. (2016). Internet use and problematic Internet use: a systematic review of longitudinal research trends in adolescence and emergent adulthood. International Journal of Adolescence and Youth, 22(4), 430–454.
Beard, C. L., & Wickham, R. E. (2016). Gaming-contingent self-worth, gaming motivation, and Internet gaming disorder. Computers in Human Behavior, 61, 507–515.
Beard, C. L., Haas, A. L., Wickham, R. E., & Stavropoulos, V. (2017). Age of initiation and Internet gaming disorder: the role of self-esteem. Cyberpsychology, Behavior, and Social Networking, 20(6), 397–401.
Beck, A. T., & Steer, R. A. (1990). Manual for the Beck anxiety inventory. San Antonio: Psychological Corporation.
Beck, A., Steer, R. A., & Brown, G. K. (1996). BDI-II, Beck depression inventory manual. San Antonio: Psychological Corporation.
Berkovits, I., Hancock, G. R., & Nevitt, J. (2000). Bootstrap resampling approaches for repeated measure designs: relative robustness to sphericity and normality violations. Educational and Psychological Measurement, 60(6), 877–892.
Bessière, K., Seay, A. F., & Kiesler, S. (2007). The ideal elf: identity exploration in World of Warcraft. Cyberpsychology & Behavior, 10(4), 530–535.
Browne, M. W., & Cudeck, R. (1992). Alternative ways of assessing model fit. Sociological Methods & Research, 21(2), 230–258.
Chen, H., Wigand, R. T., & Nilan, M. (2000). Exploring web users’ optimal flow experiences. Information Technology & People, 13(4), 263–281.
D’Amico, E. J., Houck, J. M., Hunter, S. B., Miles, J. N., Osilla, K. C., & Ewing, B. A. (2015). Group motivational interviewing for adolescents: change talk and alcohol and marijuana outcomes. Journal of Consulting and Clinical Psychology, 83(1), 68–80.
Douglas, A. C., Mills, J. E., Niang, M., Stepchenkova, S., Byun, S., Ruffini, C., et al. (2008). Internet addiction: meta-synthesis of qualitative research for the decade 1996–2006. Computers in Human Behavior, 24(6), 3027–3044.
Eichenbaum, A., Kattner, F., Bradford, D., Gentile, D. A., & Green, C. S. (2015). Role-playing and real-time strategy games associated with greater probability of Internet gaming disorder. Cyberpsychology, Behavior, and Social Networking, 18(8), 480–485.
Elliott, L., Golub, A., Ream, G., & Dunlap, E. (2012). Video game genre as a predictor of problem use. Cyberpsychology, Behavior, and Social Networking, 15(3), 155–161.
Faiola, A., Newlon, C., Pfaff, M., & Smyslova, O. (2013). Correlating the effects of flow and telepresence in virtual worlds: enhancing our understanding of user behavior in game-based learning. Computers in Human Behavior, 29(3), 1113–1121.
Fan, X., Thompson, B., & Wang, L. (1999). Effects of sample size, estimation methods, and model specification on structural equation modeling fit indexes. Structural Equation Modeling: A Multidisciplinary Journal, 6(1), 56–83.
Gold, M. S., & Bentler, P. M. (2000). Treatments of missing data: a Monte Carlo comparison of RBHDI, iterative stochastic regression imputation, and expectation-maximization. Structural Equation Modeling, 7(3), 319–355.
Gosling, S. D., Rentfrow, P. J., & Swann, W. B. (2003). A very brief measure of the big-five personality domains. Journal of Research in Personality, 37(6), 504–528.
Griffiths, M. (2005). A ‘components’ model of addiction within a biopsychosocial framework. Journal of Substance Use, 10(4), 191–197.
Hayes, A. F. (2013). Introduction to mediation, moderation, and conditional process analysis: a regression-based approach. New York: Guildford Press.
Hendriks, V. (1990). Addiction and psychopathology: a multidimensional approach to clinical practice. Rotterdam: Erasmus University.
Hu, L.-t., & Bentler, P. M. (1998). Fit indices in covariance structure modelling: sensitivity to under parameterized model misspecification. Psychological Methods, 3(4), 424–453.
Huang, L. T., Chiu, C. A., Sung, K., & Farn, C. K. (2011). A comparative study on the flow experience in web-based and text-based interaction environments. Cyberpsychology, Behavior and Social Networking, 14(1–2), 3–11.
Kaczmarek, L. D., & Drążkowski, D. (2014). MMORPG escapism predicts decreased well-being: examination of gaming time, game realism beliefs, and online social support for offline problems. Cyberpsychology, Behavior, and Social Networking, 17(5), 298–302.
Kessler, R. C., Adler, L., Ames, M., Demler, O., Faraone, S., Hiripi, E., et al. (2005). The World Health Organization Adult ADHD Self-Report Scale (ASRS): a short screening scale for use in the general population. Psychological Medicine, 35(2), 245–256.
King, D. L., & Delfabbro, P. H. (2014). The cognitive psychology of Internet gaming disorder. Clinical Psychology Review, 34(4), 298–308.
Kuss, D., & Griffiths, M. D. (2011). Internet gaming addiction: a systematic review of empirical research. International Journal of Mental Health and Addiction, 10(2), 278–296.
Kuss, D. J., Louws, J., & Wiers, R. W. (2012). Online gaming addiction? Motives predict addictive play behavior in massively multiplayer online role-playing games. Cyberpsychology, Behavior, and Social Networking, 15(9), 480–485.
Lemmens, J. S., & Hendriks, S. J. (2016). Addictive online games: examining the relationship between game genres and internet gaming disorder. Cyberpsychology, Behavior, and Social Networking, 19(4), 270–276.
Little, R. J. & Rubin, D. B. (2014). Statistical analysis with missing data. 2nd Edition, Hoboken: John Wiley & Sons.
Marsh, H. W., Balla, J. R., & McDonald, R. P. (1988). Goodness-of-fit indexes in confirmatory factor analysis: the effect of sample size. Psychological Bulletin, 103(3), 391–410.
Masten, A. S. (2001). Ordinary magic: resilience processes in development. American Psychologist, 56(3), 227–238.
Milani, L., La Torre, G., Fiore, M., Grumi, S., Gentile, D. A., Ferrante, M., et al. (2017). Internet gaming addiction in adolescence: risk factors and maladjustment correlates. International Journal of Mental Health and Addiction, 1–17. https://doi.org/10.1007/s11469-017-9750-2.
Muthen, L., & Muthen, B. (2010). Mplus 6.12. CA: Muthen & Muthen.
Ng, B. D., & Wiemer-Hastings, P. (2005). Addiction to the internet and online gaming. Cyberpsychology & Behavior, 8(2), 110–113.
Olson, D. H. (2000). Circumplex model of marital and family systems. Journal of Family Therapy, 22(2), 144–167.
Pontes, H. M., & Griffiths, M. D. (2015). Measuring DSM-5 internet gaming disorder: development and validation of a short psychometric scale. Computers in Human Behavior, 45, 137–143.
Porter-Armstrong, A. P. (2013). Impact of multiplayer online role-playing games upon the psychosocial well-being of adolescents and young adults: reviewing the evidence. Psychiatry Journal, 2013, 1–8.
Raftery, A. E. (1995). Bayesian model selection in social research. Sociological Methodology, 25, 111–163.
Ratan, R., & Hasler, B. S. (2010). Exploring self-presence in collaborative virtual teams. Psychnology Journal, 8(1), 11–31.
Salant, P., Dillman, I., & Don, A. (1994). How to conduct your own survey. USA: Wiley.
Schafer, J. L., & Graham, J. W. (2002). Missing data: our view of the state of the art. Psychological Methods, 7(2), 147–177.
Stanley, P. (2008). The risk and resilience framework and its implications for teachers and schools. Waikato Journal of Education, 14, 139–153.
Stavropoulos, V., Alexandraki, K., & Motti-Stefanidi, F. (2013). Flow and telepresence contributing to Internet abuse: differences according to gender and age. Computers in Human Behavior, 29(5), 1941–1948.
Stavropoulos, V., Gentile, D., & Motti-Stefanidi, F. (2016a). A multilevel longitudinal study of adolescent Internet addiction: the role of obsessive–compulsive symptoms and classroom openness to experience. European Journal of Developmental Psychology, 13(1), 99–114.
Stavropoulos, V., Kuss, D., Griffiths, M., & Motti-Stefanidi, F. (2016b). A longitudinal study of adolescent internet addiction: the role of conscientiousness and classroom hostility. Journal of Adolescent Research, 31(4), 442–473.
Steiger, J. H. (1990). Structural model evaluation and modification: an interval estimation approach. Multivariate Behavioral Research, 25(2), 173–180.
Stetina, B. U., Kothgassner, O. D., Lehenbauer, M., & Kryspin-Exner, I. (2011). Beyond the fascination of online-games: probing addictive behavior and depression in the world of online-gaming. Computers in Human Behavior, 27(1), 473–479.
Teo, A. R., Fetters, M. D., Stufflebam, K., Tateno, M., Balhara, Y., Choi, T. Y. ... Kato, T. A. (2015). Identification of the hikikomori syndrome of social withdrawal: psychosocial features and treatment preferences in four countries. International Journal of Social Psychiatry, 61(1), 64–72.
Thorens, G., Wullschleger, A., Khan, R., Achab, S., & Zullino, D. F. (2012). What is addictive in Internet. The Open Addiction Journal, 5(1), 14–19.
Wood, R. T. A., Griffiths, M. D., Chappell, D., & Davies, M. N. O. (2004). The structural characteristics of video games: a psycho-structural analysis. CyberPsychology and Behavior, 7, 1–10.
Yee, N. (2006). Motivations for play in online games. Cyberpsychology & Behavior, 9(6), 772–775.
Author information
Authors and Affiliations
Contributions
VS and TLB contributed to the literature review, hypotheses formulation, data collection and analyses, and the structure and sequence of theoretical arguments. CLB contributed to the theoretical consolidation of the current work and revised and edited the final manuscript. RZ contributed to the theoretical consolidation of the current work. MDG contributed in revisions and editing of the final manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Standards—Animal Rights
All procedures performed in the study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Confirmation Statement
Authors confirm that this paper has not been either previously published or submitted simultaneously for publication elsewhere.
Copyright
Authors assign copyright or license to the publication rights in the present article.
Rights and permissions
About this article

Cite this article
Stavropoulos, V., Burleigh, T.L., Beard, C.L. et al. Being There: A Preliminary Study Examining the Role of Presence in Internet Gaming Disorder. Int J Ment Health Addiction 17, 880–890 (2019). https://doi.org/10.1007/s11469-018-9891-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11469-018-9891-y