
Abstract
Objective Excessive video gaming may represent a behavioural addiction among adolescents. The objective of this study was to identify and describe the taxonomy of problem gamers based on responses to the Problem Video Game Playing (PVP) scale. Methods Data based on 3338 Ontario high schoolers sampled from 103 schools (aged 11–20; male = 51 %) who completed self-administered questionnaires. Following latent class extraction, a regression assessed the association between the derived classes and the covariates sex and socioeconomic status. We also assessed self-rated physical and mental health as auxiliary variables in the model to evaluate the predictive validity of the extracted classes. Results A 4-class model provided the best statistical fit to the nine PVP symptoms. The Severe PVP, High PVP, Low PVP and Normative classes comprised 1.9 %, 12.2 %, 36.0 % and 50.0 % of the sample, respectively. The Severe PVP class was characterized by having the highest probabilities of endorsing the PVP items. The High PVP class was differentiated from the Severe PVP class by having lower probabilities of endorsing the disregard for consequences and the lies and deception items and moderate probabilities of endorsing withdrawal and escape items. Significantly poorer physical and mental health outcomes differentiated the Severe PVP class from the remaining classes. Conclusions Adolescent problem video gamers are not homogeneous. They experience differing patterns of symptoms requiring attention of prevention programmers and clinicians.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
The popularity of computer-based sedentary behaviours among youth, such as video game playing, has raised concerns by health advocates and the research community of potential negative health effects. Moreover, the potential for addiction has also received increasing attention (Kuss and Griffiths 2011). From a clinical perspective, Internet Gaming Disorder, which primarily reflects abusive and dependent video-gaming behaviour (King and Delfabbro 2013) has been included in the emerging measures and models section of the 5th edition of the Diagnostic Statistical Manual (DSM-V) (American Psychiatric Association 2013; see also Griffiths et al. 2014) as a subject of further empirical enquiry. This represents the first time that gaming has been formally recognised as an emerging disorder in clinical nomenclature (King et al. 2013). Reasons for this cautious approach may include the lack of consensus regarding assessment and diagnostic criteria for video game disorders (Ferguson et al. 2011; King et al. 2013) and perhaps, the noted weakening distinction between video gaming and gambling (Griffiths et al. 2011).
One approach to measuring video gaming disorders has applied a ‘pathological gambling’ model in which symptoms of gambling are constructed to appraise pathological video gaming. One such tool is the Problem Video Game Playing (PVP) scale for adolescents (Tejeiro Salguero and Morán 2002) which has been recently described by some as the best overall measure of internet use disorder (King et al. 2013), whereas, the originator of the PVP contends that high scores on the PVP are best viewed as “abuse”, given its adaptation from DSM-IV (Tejeiro Salguero et al. 2012). The 9-item PVP measures the following dimensions of video gaming impairments and disabilities: preoccupation, tolerance, loss of control, repetition/relapse, withdrawal, escape, disregard for consequences and disruptions to family and/or school due to video gaming. Bioulac et al. (2008) suggested a PVP cut score of five or more (i.e., 4/5) to represent problematic video gaming which would be consistent with DSM-IV criteria for pathological gambling. Approximately 10 % of the sample in the original study by Tejeiro Salguero and Morán (2002) met this criteria, an estimate falling within the 6–19 % of 13 recent adolescent video game “addiction” studies (Tejeiro Salguero et al. 2012). In addition, there is some evidence that problem video gaming has remained stable. In a probability sample of Ontario 7th–12th graders surveyed in 2011, 11.9 % (95 % CI: 9.4 %, 14.9 %; n = 4,816) scored positively on the PVP screener (4/5 symptoms), a prevalence which has held steady from 2007 (9.4 %; 95 %CI, 8.2 %, 10.8 %; n = 2,935) and 2009 (10.3 %; 95 % CI, 9.0 %, 11.7 %; n = 4,261) (Paglia-Boak et al. 2011). In a 2007 national survey of 1,178 American youth aged 8–18, it was reported that 8 % of youth could be considered at risk of pathological video gaming using an 11-item scale of video gaming similar to the PVP (Gentile 2009). As reflected in a recent meta-analysis of this literature, studies employing this approach to defining pathological video gaming converge on a prevalence of 8.9 % (Ferguson et al. 2011).
An alternative approach to measuring video game disorders is to emphasize the interfering nature of video gaming behaviour on one’s roles and obligations rather than emphasizing established clinical symptoms of pathological video gaming (Desai et al. 2010; Van Rooij et al. 2010. Such symptom items stress whether video gaming interferes with functioning rather than items that may reflect positive engagement with video gaming as opposed to any form of pathology. Using this approach, prevalence estimates are lower and converge at 3.1 % (Ferguson et al. 2011). In the study of 4,028 US adolescents by Desai and colleagues (2010), 4.9 % reported problem video gaming, similar to the prevalence of 3 % reported by Van Rooij and colleagues (2010) among two large samples of Dutch school children 13–16 years.
These approaches, however, are variable centered – they assess the level and associations found among items or symptoms. This approach does not inform us as to how video gaming behaviours and related consequences are patterned within individuals or types of individuals. In this paper, we describe the person-centered structure of problem video gaming, by clustering PVP symptoms into homogeneous classes or clusters of adolescents. Such person-centered investigations can provide revealing information especially for the purpose of targeting groups for intervention or clinical attention. Indeed, there is precedence in the gambling field of the development of such taxometric models (e.g. see Blaszczynski and Nower 2002; Nower and Blaszczynski 2004; Turner et al. 2008; Turner et al. 2011). In particular, Turner and colleagues (2011) used traditional cluster analysis to identify different subpopulations of adolescent gamblers. Where scales like the PVP are used, it is important to investigate the profile of the negative health outcomes within and across classes/clusters. Indeed, some authorities contend that, “subtypes of gamblers must be studied” (Gupta and Derevensky 2011) to build and tune prevention programs and clinical practice. In a similar vein, others have bemoaned that many studies assume “addicted video gamers” to be a homogeneous group, “but in no case this homogeneity has been tested” (Tejeiro Salguero et al. 2012). Latent class analysis (LCA) is a growing analytic technique that provides such a person-centered approach. Because LCA assesses latent types, variables and structures, it has become a versatile tool with wide applications (Hagenaars and McCutcheon 2002). Moreover, this approach has many advantages over traditional cluster analysis, most noteworthy being the ability to employ mixed-measured indicators and better model testing capabilities. The primary objective of LCA is to extract the most parsimonious number of homogenous classes of individuals that display similar responding patterns among a set of observed variables, and to compare and contrast the extracted classes.
Such an approach has been taken in examining problematic internet use among Hungarian youth. In a representative sample of 5,045 secondary school students, latent profile analysis found that 4.6 % of the adolescents belonged to a high risk group of problematic online gaming (Pápay et al. 2013). Gamers in this group were more likely to be male, have a lower grade point average, have lower self-esteem and have higher depression scores than youth in a no-risk or low risk groups. Similarly, Demetrovics et al. (2012) reported a four-class structure in a sample of 3,415 young adults (mean age = 21.01 years). A high risk class for problematic online gaming made up 3.4 % of the sample. These studies demonstrate the value of LCA which needs further cross-cultural confirmation (Pápay et al. 2013). In this study, our main objective was to identify the presence of distinct groups of high schoolers endorsing items on the PVP using LCA. Secondly, we examine further what factors distinguish class membership including health behaviours, academic performance and physical and mental health status.
Methods
Study design
We analyzed survey data comprised of 3,338 high schoolers, a subsample derived from the 2011 cycle of the province-wide Ontario Student Drug Use and Health Survey (OSDUHS), a repeated cross-sectional school population surveillance study conducted biennially since 1977 by the Centre for Addiction and Mental Health (CAMH) (Paglia-Boak et al. 2011). Participating students were selected by means of a stratified two-stage cluster sample with a probability design sampling all enrolled students in the 7th through 12th grades in publicly funded middle and high schools in Ontario, which comprise French-language and English-language schools in the public and Catholic sectors. The two stages of sampling consisted of schools (stratified by region and type of school – elementary versus secondary strata) followed by classes (stratified by 2 or 4 grade strata). Signed active parental consent was obtained from parents/guardians and signed consent/assent was obtained from students prior to participating in the survey.
The subsample of 3,338 high schoolers were derived from the full sample of 9,288 7th–12th graders from 181 schools and 581 classes participating in the 2011 cycle between November 2010 and June 2011. Students completed self-administered, anonymous questionnaires in intact classrooms during a regular class period under the supervision of Institute for Social Research administrators. The unweighted high school and student response rates in the 2011 OSDUHS were 71 % and 63 %, respectively. The most common reasons given for school nonparticipation were that schools were “too busy”, or were committed to other research activities. Reasons for students’ nonresponse included absence of active parental consent (26 %) and absenteeism (12 %). We appraised potential nonresponse bias by comparing school classes with response rates of 70 % and higher (n = 258) versus classes with response rates less than 70 % (n = 323). We found no statistically discernible differences between classes with high versus low response rates for both sex and grade composition; moreover, only 3 of 28 measures (past year alcohol, binge drinking and drunkenness) differed between higher and lower responding classes. OSDUHS 2011 used split-ballot random half samples for selected questionnaire items or modules to maximize questionnaire coverage while minimizing the response load on respondents. Because the video gaming questions were asked of a random half-sample of students, the estimation sample for the present study was reduced to 3,338 9th–12th graders enrolled in 103 high schools, of which 51.1 % of students were male and the average age was 15.9 (SD = 1.3). Some 23.0 %, 22.8 %, 23.8 % and 30.6 % of the sample were enrolled in the 9th through 12th grades. Based on a 10-rung ladder scale, mean family SES was 7.0 (SD = 1.4). OSDUHS 2011 received approval from the Research Ethics Boards of CAMH, York University, and the 27 school boards requiring institutional ethical review. Complete questionnaires and further methodological details about the survey are available at the OSDUHS webpage (CAMH, Centre for Addiction and Mental Health 2012).
Measures
Latent Class Indicators: Problem Video Game Playing
The Problem Video Game Playing (PVP) screener, a DSM-IV adaptation, developed in Spain with adolescents was employed as the latent indicators (Tejeiro Salguero and Morán 2002). The PVP comprises nine symptom items relating to problematic video gaming experienced in the 12 months before the survey. The wordings of original items were slightly altered for use with the OSDUHS questionnaire (see Table 1). For the present study, responses were dichotomized (yes = 1; no/don’t play video games= 0). These nine binary symptoms of PVP were then used as indicators to extract latent class membership.
Covariates
Whereas the LC indicators are endogenous to the latent classes, covariates are exogeneous in that they are used to predict class membership (Vermunt and Magidson 2002). We introduced a binary covariate, sex (male = 1; female = 0), and a continuous covariate, subjective socioeconomic status (SES) which was assessed using the youth version of the MacArthur Scale of Subjective Social Status (Goodman et al. 2001), a single item ladder scale ranging from 1–10 with higher scores reflecting higher SES (see question A25 on the OSDUHS webpage questionnaire).
Auxiliary Variables
Frequency of Video Gaming
Frequency of past year video gaming was assessed with the question “In the last 12 months, how often did you play video games [either on a computer or TV, or at an arcade]?” The nine frequency response options were factored as daily/almost daily video gamers (coded 1) vs. others (coded 0).
Mental Health
We used three measures of mental health – social dysfunction, depression/anxiety and self-rated mental health status. The social dysfunction and depression measures, confirmed by a confirmatory factor analysis (details available upon request), were derived from the 12-item General Health Questionnaire (GHQ), a brief screening instrument that assesses change in psychological distress experienced over the past few weeks (Goldberg and William 1998; McDowell 2006). As recommended by Goldberg et al. (1997) we used the binary scoring method (0,0,1,1) with the two least symptomatic responses scored 0 (the 3 response formats were better/same as usual; not at all, no more than usual; more so than/same as usual) and the two most symptomatic responses scored 1 (less/much less than usual; rather/much more than usual; less/much less useful; less/much less able than usual).
We generated a count variable measuring social dysfunction based on the following 6 GHQ items: able to concentrate, felt playing a useful part, capable of making decisions, able to enjoy daily activities, able to face problems, and feeling reasonably happy. Next, we generated a symptom count to represent depression/anxiety, from the following 6 GHQ items: lost sleep over worry, felt constant stress, felt couldn’t overcome difficulties, feeling unhappy/depressed, losing self-confidence, and thinking of self as worthless. For both indices, symptom counts range from 0 to 6, with increasing counts indicative of greater symptomatology. The third measure of mental health was a single item summary rating of mental health status: “How would you rate your mental health?” The original 5-point scale was set to 1 to represent those reporting fair or poor (fair/poor) health and set to 0 (good/very good/excellent) otherwise.
Physical Health
Physical health status was appraised by weight status and self-rated physical health. Students reported their height (based on 27 categories of 1 in. increments) and weight (based on 42 categories of 5 lb intervals), from which body mass index (BMI) was calculated (by dividing each student’s mid-category weight in kilograms by her/his mid-category height in meters squared [kg/m2]). Students aged 18 or younger were classed as overweight/obese (BMI ≥ 25.0) according to their age and sex-specific BMI cut-offs defined by international experts (Cole et al. 2000). Students who did not fall within the category of “overweight/obese” were classified as “neither overweight nor obese.” For students aged 19 or older, weight status was based on the International Classification of adult weight status (World Health Organization 2011). Students not meeting current healthy weight guidelines (overweight/obese, coded 1) were compared with those meeting healthy weight guidelines (healthy weight, coded 0). The second measure of physical health status was a single-item summary rating of the respondent’s physical health: “How would you rate your physical health?” and coded as the mental health rating above. The use of self-report to measure adolescent physical health is well established and has been shown to be a reliable indicator of health problems, health care utilization, and longevity (D’Arcy 1998).
Physical Activity
Physical activity was measured with the question, “On how many of the last 7 days were you physically active for a total of at least 60 min each day?” Students were instructed to cumulate time spent in any kind of physical activity that “increased your heart rate and made you breathe hard some of the time (e.g., brisk walking, running, swimming).” Count responses ranged from 0 to 7 days. Students not meeting the current Canadian physical activity recommendations of at least at least 60 min of moderate to vigorous-intensity physical activity daily (Canadian Society of Exercise Physiology 2011) were coded 1 (i.e., meeting the recommendations on 0–6 days) and 0 otherwise (i.e., meeting the recommendations on 7 of 7 days).
Self-rated Academic Performance
Academic performance was assessed with the question, “Overall, what marks do you usually get in school?” Responses of C, D or F were coded 1 (poor academic performance) whereas, A and B were coded 0 (good performance) (a grade of E is not assigned in Ontario).
Analytic Strategy
The nine binary coded PVP symptoms were analysed using an unrestricted latent class analysis (LCA), specifically latent class clustering (Vermunt and Magidson 2002), under the probabilistic parameterization as applied in Mplus (Muthén and Muthén 1998–2011). LCA is a mixture modelling technique that assumes that data arise from two or more unobserved groups that are mixed. It is used to identify and extract the fewest homogenous groups (classes) of units such as individuals that have similar characteristic or response patterns, in our case the constellation of PVP symptoms of high schoolers (Nylund et al. 2007). The first step of analysis involves identifying the fewest optimal number of latent classes. We began with fitting a one-class model and successively increased the number of classes until a model with an acceptable fit was obtained. Decisions about the optimal number of latent classes were based on five statistical criteria, including, Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC) and the sample-size adjusted Bayesian Information Criterion (ABIC), the Lo–Mendell–Rubin’s likelihood ratio test (LMR-LRT) and entropy. For the information indices, the smallest values indicate the best-fitting model, whereas for LMR-LRT, a nonsignificant value (p>0.05) infers that the most parsimonious model with one fewer class should be preferred. Entropy, which ranges from 0 to 1, is a standardized measure of how accurately individuals are assigned into classes based on their model-based posterior probabilities. Higher entropy values (especially those .80 and higher) indicate better classification of individuals (Ramaswany et al. 1993). Of the fit measures, we emphasized BIC because the AIC has been shown to be inconsistent for LC models and simulation studies suggest that the BIC provides the most reliable indicator of the true number of classes (Nylund et al. 2007). In addition to the fit statistics, we assessed model interpretability and the assumption of conditional or local independence that observations should be independent in each class by examining the standardized bivariate residuals.
Following the selection of the best-fitting or optimal latent class model, we included the covariates (sex and SES) in the model in order to control for these variables when the subsequent variables were entered into the analysis. However, first we had to determine whether these demographic factors significantly distinguished membership across classes. With class membership as outcome and sex and SES as predictors, the model is equivalent to a multinomial logistic regression. Next, we sought to determine the predictive validity of the extracted latent classes using our auxiliary variables. In the same LC model with covariates, we tested the equality of the means of the auxiliary variables across classes. The Wald chi-squared test derived from the posterior probability-based multiple imputations was used to conduct pairwise mean comparisons (Muthén and Muthén 1998–2011).
As noted, all statistical analyses were computed with Mplus 6.12 (Muthén and Muthén 1998–2011) using complex survey data estimation methods, which involved maximum likelihood estimation (via the EM algorithm) with robust sandwich estimators for computing standard errors. We used 500 random sets of starting values to ensure that our estimates converged on the true (global) rather than local maxima of the log-likelihood and to assess model identification – whether there is sufficient observed data to estimate the model. The design-based complex survey data features available in Mplus were used to accommodate the overdispersed (i.e. extracorrelated) survey data, without which, variances would be understated and statistical tests would be overstated (Korn and Graubard 1999; Patterson et al. 2002).
Results
Prevalence of PVP Criteria
The 4/5 cut score for past year PVP was met by 12.9 % of Ontario high schoolers. Repetition/relapse (48.0 %), followed by family/school disruption (24.6 %), preoccupation (22.0 %), and loss of control (20.3 %) were the most frequently endorsed criteria, whereas disregard for physical/psychological consequences (5.0 %) and lies and deception (6.1 %) were least commonly endorsed (Table 1).
Model Fit
Table 2 displays the fit indices for each successive LC model. The 4-class model was deemed to provide the best representation of the data. The BIC (22662.16) and ABIC (22538.24) statistics showed distinct minimum values, and the corresponding LMR-LRT was statistically superior to the 3-class model (p = 0.004), but not to the less parsimonious 5-class model (p = 0.147). The entropy value (0.77), also suggested an acceptable classification accuracy of students into four classes: higher than both the 3-class (0.75) and 5-class (0.73) models. We shall also see that all classes are substantively interpretable and there is no evidence of unscalable respondents.
Profile Plot
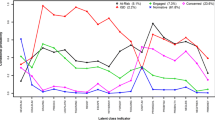
Figure 1 shows the symptom item profile plot displaying the estimated probability of endorsing each PVP symptom for the largely ordered four latent classes. Class 1, comprised 1.9 % (n = 63) of high schoolers, which we labelled the Severe PVP class, was distinguished by having elevated probabilities of endorsing six of the nine PVP symptoms. For instance, probabilities ranged from 0.75 for the escape item to 1.00 for the family/school disruption item. Class 2 – the High PVP class –included 12.2 % (n = 406) of the sample. Similar to the Severe PVP class, the High PVP class showed high probabilities of endorsing items relating to preoccupation, tolerance, loss of control, repetition/relapse, and family/school disruption. However, unlike the Severe PVP class, the High PVP class was defined by moderate probabilities of endorsing the withdrawal (0 .42) and escape (0.48) items. The High PVP class was further distinguished from the Severe PVP class by having low probabilities of endorsing the disregard for consequences (0.21) and the lies and deception (0.14) items. Class 3, represented 36.0 % (n = 1,201) of the sample. Like the Severe and High PVP classses, the Low PVP class had a high probability of endorsing the repetition/relapse item. Also similar to the High PVP class but unlike the Severe PVP class, the Low PVP class was characterized by having low probabilities of endorsing the disregard for consequences and the lies and deception items. However, unlike the Severe and High PVP classses, the Low PVP class had a 50 % probability of endorsing the family/school disruption item combined with the relatively low probabilities (0.07 to 0.30) of endorsing the other items including, preoccupation, tolerance, loss of control, withdrawal, and escape. Finally, Class 4 – Normative class – was, not surprisingly, the most numerous, comprising 50.0 % (n = 1,668) of the sample. The normative class was differentiated from the other classes by having near zero probabilities of endorsing the PVP items. In fact, the highest probability for any item endorsement in the Normative class was for repetition/relapse, with a probability of 0.20.

Profile plot showing the probability of high school students (n = 3,338) endorsing an item on the Problem Video Game Playing (PVP) scale, conditional on belonging to a particular class
Examining Covariates: Sex and SES Associated with Latent Class Membership
Table 3 reports the results (adjusted ORs and their 95 % CIs) of the latent class multinominal regression (with the normative class set as the reference group) that examined the utility of sex and SES in predicting class membership. Accordingly, we made three LC dependent variable contrasts: Membership in the Normative class versus (1) Severe PVP class, (2) High PVP class, and (3) Low PVP class.
Sex
Sex was significantly associated with latent class membership (p < 0.05). More specifically, the net odds of Severe PVP class membership versus Normative class membership were some 16 times greater for male than female students (OR = 15.56, 95 % CI = 4.70–51.55). Further, the net odds of being classed in the High PVP group (OR = 13.18, 95 % CI = 6.07–28.65) or the Low PVP group (OR = 6.32, 95 % CI = 3.63–11.0) versus the Normative group were 13 and 6 times greater for male than female high schoolers.
Socioeconomic Status
SES showed a marginally significant association with latent class membership (p < 0.05). The odds that a high schooler would be classified in the Severe PVP or the High PVP classes than the Normative class were significantly reduced as her/his SES score increased. Specifically, for each unit increase in SES, the net odds of membership in the Severe PVP class than the Normative class decreased by a factor of 0.65 (95 % CI = 0.47–0.89), or by 35 %. Similarly, the net odds of membership in the High PVP class versus the Normative class similarly decreased by a factor of 0.68 (95 % CI = 0.60–0.77) or by 32 % with each unit increase in SES. SES was not significantly related to the remaining contrast between the Low PVP and Normative classes.
External Variables
The means of the 8 health risk outcomes are shown in Figs. 2 and 3 respectively. For each outcome, all six possible pairwise class contrasts were evaluated:

Comparisons on health risk outcomes across latent classes

Comparisons on physical and mental health outcomes
Not Meeting Physical Activity Guidelines
The percentage of high schoolers not meeting physical activity guidelines were 86.3 %, 90.1 %, 79.3 % and 79.8 % for the Severe PVP, High PVP, Low PVP and Normative PVP classes, respectively. Significantly more High PVP students did meet physical activity guidelines than the Low PVP and Normative students. None of the remaining pairwise comparisons were statistically significant (Fig. 2).
Not Meeting Healthy Weight Guidelines
The percentage of high schoolers not meeting healthy weight guidelines (overweight/obese) were 36.1 %, 31.3 %, 29.4 % and 21.6 % for the Severe PVP, High PVP, Low PVP and Normative students, respectively. Each of the 3 PVP classes had significantly higher prevalence of being overweight/obesity in comparison with Normative students. None of the remaining pairwise comparisons were statistically significant (Fig. 2).
Daily Video Gaming
The percentage of daily/almost daily video gamers were 64.5 %, 58.6 %, 29.9 %, and 4.8 % for the Severe PVP, High PVP, Low PVP and Normative classes, respectively. Students in the Severe PVP and High PVP classes did not differ significantly in their daily/almost daily video gaming. All remaining contrasts for daily/almost daily video gaming were statistically significant (Fig. 2).
Physical and Mental Health Outcomes
GHQ Depression/Anxiety
The mean depression/anxiety symptom counts were 3.1, 1.8, 1.6, and 1.8 for the Severe PVP, High PVP, Low PVP and Normative PVP classes, respectively. High schoolers in the Severe PVP class had significantly more depression/anxiety symptoms than students in the High PVP, Low PVP and Normative classes. None of the remaining pairwise comparisons were statistically significant (Fig. 3).
GHQ Social Dysfunction
The mean social dysfunction symptom counts were 2.0, 1.0, 0.9, and 1.0 for the Severe PVP, High PVP, Low PVP and Normative PVP classes respectively. High schoolers in the Severe PVP class had significantly more social dysfunction symptoms than students in the High PVP, Low PVP and Normative classes (Fig. 3). None of the remaining pairwise comparisons were statistically significant (Fig. 3).
Self-rated Mental Health
The percentage of high schoolers who rated their mental health as fair or poor were 41.2 %, 18.6 %, 15.7 %, and 13.2 % for the Severe PVP, High PVP, Low PVP and Normative PVP classes, respectively. Severe PVP students had significantly poorer mental health ratings than the remaining 3 classes. As well, High PVP students had significantly poorer self-rated mental health than students in the Normative class. None of the remaining pairwise comparisons were statistically significant (Fig. 3).
Poor Academic Performance
The percentage of high schoolers reporting poor academic performance was 17.2 %, 17.6 %, 13.1 % and 8.9 % for the Severe PVP, High PVP, Low PVP and Normative PVP classes, respectively. Poor academic performance was significantly higher in the High PVP class than in the Normative class. None of the remaining pairwise comparisons were statistically significant (Fig. 2).
Fair/Poor Self-rated Physical Health
The percentages of high schoolers rating their physical health as fair or poor were 37.1 %, 21.0 %, 15.6 %, and 17.8 % for the Severe PVP, High PVP, Low PVP and Normative PVP classes, respectively. Self-rated physical health was significantly poorer for Severe PVP students relative to High PVP, Low PVP and Normative students. None of the remaining pairwise comparisons were statistically significant (Fig. 3).
Discussion
Building on the earlier OSDUHS work of Turner et al. (2012) who reported the prevalence of problem video gaming among Ontario 7th through 12th graders in 2009, we found a similar prevalence of high schoolers meeting the PVP threshold in 2011 (12.9 % versus 9.4 %). In addition we used an approach similar to Turner et al. (2011) to explore clusters, but in this case related to video gamers. Our person-centered latent class clustering proved revealing in identifying differing subtypes of adolescent video gamers. The severe PVP class (1.9 %) may provide a better estimate of problematic video gaming among adolescents. This class had elevated probabilities of endorsing six of the nine PVP symptoms and this estimate was similar to that reported in other LCA studies of problematic online gaming among Hungarian youth (Demetrovics et al. 2012; Pápay et al. 2013). Students in the Severe PVP class displayed more depression/anxiety symptoms, reduced social functioning, and poorer mental health than most other classes. Another study similarly found addicted heavy (55.3 h/week) video gamers to have higher depressed mood than non-addicted heavy (45.5 h/week) video gamers (Van Rooij et al. 2010). We found no differences between the High PVP class and the Low and Normative classes on these outcomes, suggesting that the prevalence of problematic video gaming is low but it does carry significant burden for the gamer regarding poorer mental health and social functioning. These findings support the possibility that measures like the PVP may produce inflated prevalence estimates (Ferguson et al. 2011).
While the relative size of problem video gamers in the population is small, their risk factor profile showing poorer physical and mental health is not inconsequential. Problematic video gaming is associated with poorer academic performance. Indeed, we found prevalence of poor academic performance was significantly higher in the High PVP class as reported by others (Pápay et al. 2013). In a national survey of 44,610 German ninth-graders, video-game dependent boys had lower grades, skipped more classes and were more likely to be absent from school (Rehbein et al. 2010). Thus, it is not surprising that small but significant associations have been reported between pathological video gaming and academic problems in a recent meta-analysis (Ferguson et al. 2011).
Regarding health status, students in both the Severe and High PVP classes were less likely to meet physical activity guidelines and more likely to be overweight or obese. This may reflect differing mechanisms – that video gaming displaces the time available for physical activity (Biddle et al. 2004) and/or video gaming covaries with unhealthy eating behaviours like increased snacking (Pearson and Biddle 2011). Previous research on correlates of video gaming is inconsistent regarding physical activity. One study did not find a relationship between amount of exercise and videogame use (Mentzoni et al. 2011), whereas another reported that video game dependent boys were less likely to report participating in any regular, organized leisure time activities (Rehbein et al. 2010). Increased screen time (e.g., TV viewing; computer use; video gaming) is consistently associated with physical inactivity and overweight status (Tremblay et al. 2011a). Our findings contribute to this limited literature concerning the impact of specific screen time behaviours, other than TV, on the health of adolescents. Importantly, the prevalence of poor physical health was significantly higher in the Severe PVP class than all others. Problem video gaming is associated with physical health risks. This indicates a need for targeting intervention at adolescents who engage in problematic video gaming where physical functioning is being compromised. As a basis for intervention, limiting screen time to two hours or less each day is currently recommended for youth (Tremblay et al. 2011b).
The odds of membership in the Severe PVP class were greater for males than females and lower versus higher SES youth. Such gender differences are uniformly reported in the literature whereas there is little uniformity concerning SES. Video gaming time is usually higher in adolescents with lower educational achievement (Rehbein et al. 2010) and education is a dominant proxy for SES. Speculatively, this relationship might be influenced by safety concerns. Based on data from 15,917 youth in grades 6–10 (aged 10–16) who participated in the Canadian 2009/10 Health Behaviour in School-aged Children survey (Carson and Janssen 2012), high social and physical neighborhood disorder was associated with approximately 40–60 % increased odds of elevated television, computer, and video game use. Thus, youth residing in low SES neighbourhoods with elevated neighborhood disorder may be more inclined to remain indoors to avoid potentially dangerous exposure to victimization. In turn, they are then more likely to engage in screen-based activities. While challenging, elevated neighborhood disorder may be one environmental factor that could be addressed in future, public health interventions and strategies (or methods, such as resiliency development, to mitigate health compromising exposures) aimed at reducing screen time among youth (Carson and Janssen 2012).
Our study is not without its limitations. First, although the response rate of 62 % is fairly standard, it does mean we were successful in surveying only some two-thirds of our selected sample, and we cannot know whether the inclusion of non-responders would alter the structure or size of our latent classes. Fortunately, nonresponse rates do not singly generate nonresponse bias unless differences between respondents and non-respondents are sizeable (Groves and Peytcheva 2008). Moreover, we noted earlier that our classroom nonresponse assessment showed no evidence of nonresponse bias for most health behaviours. Second, self-report data carries a risk of bias, which again may alter the latent classes identified in our data. Additionally, each dimension of the Problem Video Game Playing (PVP) scale is only measured by one item. Third, although LCA has many strengths, it has its limitations as well. LCA is a data-driven, descriptive method. It describes multi-occurring patterns, not associations between predictor and response variables. Given the cross-sectional nature of the study, causality cannot be inferred. This leads to the question as to whether video game addiction is a unique phenomenon or whether it reflects the co-occurring symptoms of underlying mental health impairments. For example, depressed youth may seek social isolation or comfort by video gaming. Clearly, more longitudinal research is required to examine the temporal mechanisms of the progression and impact of video game addiction. In a two year, panel study in Singapore, greater amount of time spent video gaming, lower social competence and greater impulsivity were apparent risk factors for the onset of pathological video gaming (Gentile et al. 2011). Critically, these youth had elevated depression, anxiety, and social phobia. Further research is needed to establish the stage sequencing of these behaviours – whether video game addiction predates mental health disablements or disorders, or vice versa.
Despite these limitations, we contend that our study makes several important contributions to the video gaming literature. First, we believe this study to be one of the first person-centered investigations of video gaming disorders as measured by DSM-based symptoms of the PVP screener, demonstrating appreciable variability in the subtypes of adolescent video gamers. Indeed, although there is much comment given to the multi-occurring symptoms of problematic video gaming within individuals, few studies have directly investigated this matter. Our findings are consistent with studies using the Problematic Online Gaming Questionnaire Short-Form Questionnaire among Hungarian youth (e.g., Demetrovics et al. 2012). Our findings are strengthened by aspects of the study design. Our data are based on a large probability sample of adolescents, not only covering the spectrum of video gaming behaviours, but providing a heterogeneous sample with wide age and other demographic variation. In addition to identifying video gaming subtypes, when applied to population data, LCA also identifies the population size of the classes. Moreover, because the PVP scale was a module embedded in a wide-scope study, the resulting latent classes benefitted from a range of multi-occurring health compromising and health enhancing behaviours.
There are several directions that future research can take to contribute to this area of investigation. First and foremost is the need to assess class invariance – whether our derived classes can be replicated across populations (e.g., cross-nationally), across subpopulations (e.g., sex, age, ethnic group) and across time. Although such a matter was beyond the scope of our study, an especially useful future analysis would be to test the structural equivalence of the latent classes – i.e. that observed PVP symptoms are independent of sex. Our emphasis here has been largely epidemiological. It is for this reason to establish population risk that we have analyzed data based on video gamers and non-gamers alike. Future analyses based on those scoring positive on the PVP should appraise the clinical heterogeneity, structure and size of the derived classes. Given our student population, there also remains the question whether latent classes vary by school characteristics. That is, does school climate and structural characteristics influence the development, structure or size of latent subtypes? Such a matter can now be addressed by newer multilevel latent class models (Asparouhov and Muthén 2008; Vermunt 2008). As mentioned, we should also evaluate whether and how subtypes may be shifting in size or structure with time. A specific issue related to the changing structure of latent classes is whether elevated video gaming developed during late adolescence migrates into early adulthood or whether video gaming retains the status of an adolescent limited behaviour similar to other antisocial activities (Moffitt 2006). Also for consideration is whether the expansion of gambling has influenced successive cohorts of adolescents to develop disordered gambling behaviours. Such are matters that future OSDUHS cycles can readily examine. Although our four latent classes infer class severity (i.e. ordering), we did not test for this ordinality, although newer LC models could investigate this matter (Croon 2002). Although it was our intention to assess a basic unrestricted model, another matter that future work should resolve is whether there is a need to fix a pure zero class, i.e. a class whose members do not experience any of the PVP symptoms (see Muthén 2002). Future research should also identify the possible mechanisms and implications for our finding as to why SES predicted membership in the Severe and High PVP classes, but not in the Low PVP class, and whether the structure and size of our latent classes has implications for the cut scores used in the PVP scale. Finally, our investigation here has been largely empirical. Future work needs to identify and develop what prevention, intervention and clinical efforts arise from our findings. Indeed, we hope that this study will spark discussion among prevention and clinical specialists.
In summary, we identified four homogenous, substantively meaningful subtypes of adolescent video gamers. Those working with adolescent problem video gamers should be aware that this population is not homogeneous; indeed, the severity-ordered subtypes engender differing clinical issues and treatment approaches. For example, although the traditional PVP threshold would identify both Severe and High class members, their symptom profiles differ importantly. Further research is needed to assess demographic group class invariance and the potential application of the subtypes for prevention, intervention and clinical programs and practice.
References
American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders (5th ed.). Arlington, VA: American Psychiatric Publishing.
Asparouhov, T., & Muthén, B. (2008). Multilevel mixture models. In G. R. Hancock & K. M. Samuelsen (Eds.), Advances in latent variable mixture models (pp. 27–51). Charlotte, NC: Information Age.
Biddle, S. J. H., Gorely, T., Marshall, S. J., Murdey, I., & Cameron, N. (2004). Physical Activity and Sedentary Behaviours in Youth: Issues and Controversies. Journal of the Royal Society for the Promotion of Health, 124, 29–33. doi:10.1177/146642400312400110.
Bioulac, S., Arfi, L., & Bouvard, M. P. (2008). Attention Deficit/Hyperactivity Disorder and Video Games: a Comparative Study of Hyperactive and Control Children. European Psychiatry, 23, 134–141. doi:10.1016/j.eurpsy.2007.11.002.
Blaszczynski, A., & Nower, L. (2002). A Pathways Model of Problem and Pathological Gambling. Addiction, 97, 487–499. doi:10.1046/j.1360–0443.2002.00015.x.
Canadian Society of Exercise Physiology. (2011). Canadian Physical Activity Guidelines. Retrieved September 27, 2013, from http://www.csep.ca/CMFiles/Guidelines/CSEP-InfoSheets-youth-ENG.pdf.
Carson, V., & Janssen, I. (2012). Neighborhood Disorder and Screen Time Among 10–16 Year old Canadian Youth: a Cross-Sectional Study. International Journal of Behavioural Nutrition and Physical Activity, 9, 66. doi:10.1186/1479–5868–9–66.
Centre for Addiction and Mental Health. (2012). Ontario Student Drug Use and Health Survey. Retrieved September 27, 2013, from http://www.camh.ca/research/osduhs.aspx.
Cole, T. J., Bellizzi, M. C., Flegal, K. M., & Dietz, W. H. (2000). Establishing a Standard Definition for Child Overweight and Obesity Worldwide: International Survey. British Medical Journal, 320, 1240–1243.
Croon, M. (2002). Ordering the Classes. In J. A. Hagenaars & A. L. McCutcheon (Eds.), Applied Latent Class Analysis (pp. 137–162). New York: Cambridge University Press.
D’Arcy, C. (1998). Social distribution of health among Canadians. In D. Coburn, C. D’Arcy, & G. M. Torrance (Eds.), Health and Canadian Society: Sociological Perspectives (3rd ed., pp. 73–101). Toronto: University of Toronto Press.
Demetrovics, Z., Urban, R., Nagygyorgy, K., Farkas, J., Griffiths, M. D., Papay, O., Kokonyei, G., Felvinczi, K., & Olah, A. (2012). The Development of the Problematic Online Gaming Questionnaire (POGQ). PloS One, 7(5), e36417.
Desai, R. A., Krishnan-Sarin, S., Cavallo, D., & Potenza, M. N. (2010). Video-Gaming Among High School Students: Health Correlates, Gender Differences, and Problematic Gaming. Pediatrics, 126, e1414–1424. doi:10.1542/peds.2009–2706.
Ferguson, C. J., Coulson, M., & Barnett, J. (2011). A Meta-Analysis of Pathological Gaming Prevalence and Comorbidity with Mental Health, Academic and Social Problems. Journal of Psychiatric Research, 45, 1573–1578. doi:10.1016/j.jpsychires.2011.09.005.
Gentile, D. A. (2009). Pathological Video-Game Use Among Youth Ages 8 to 18: a National Study. Psychological Science, 20, 594–602. doi:10.1111/j.1467–9280.2009.02340.x.
Gentile, D. A., Choo, H., Liau, A., Sim, T., Li, D., Fung, D., & Khoo, A. (2011). Pathological Video Game use Among Youths: a Two-Year Longitudinal Study. Pediatrics, 127, e319–e20. doi:10.1542/peds.2010–1353.
Goldberg, D. P., & William, P. (1998). A user’s guide to the General Health Questionnaire. Windsor, UK: NFER-N.
Goldberg, D. P., Gater, R., Sartorius, N., Ustun, T. B., Piccinelli, M., Gureje, O., & Rutter, C. (1997). The Validity of Two Versions of the GHQ in the WHO Study of Mental Illness in General Health Care. Psycholical Medicine, 27, 191–197.
Goodman, E., Adler, N. E., Kawachi, I., Frazier, A. L., Huang, B., & Colditz, G. A. (2001). Adolescents’ Perceptions of Social Status: Development and Evaluation of a New Indicator. Pediatrics, 108, e31. doi:10.1542/peds.108.2.e31.
Griffiths, M. D., Parke, J., & Derevensky, J. L. (2011). Remote gambling in adolescence. In J.L. Derevensky, D.T. Shek & J. Merrick J (Eds.), Youth Gambling: The Hidden Addiction (pp. 125–143). Berlin/Boston: De Gruyter.
Griffiths, M. D., King, D. L., & Demetrovics, Z. (2014). DSM-5 Internet Gaming Disorder Needs a Unified Approach to Assessment. Neuropsychiatry, 4, 1–4.
Groves, R., & Peytcheva, E. (2008). The Impact of Nonresponse on Nonresponse Bias: a Meta-Analysis. Public Opinion Quarterly, 72, 167–189.
Gupta, R., & Derevensky, J. (2011). Defining and assessing binge gambling. In J.L. Derevensky, D.T. Shek & J. Merrick J (Eds.), Youth Gambling: The Hidden Addiction (pp. 79–97). Berlin/Boston: De Gruyter.
Hagenaars, J. A., & McCutcheon, A. L. (2002). Applied Latent Class Analysis. New York: Cambridge University Press.
King, D. L., & Delfabbro, P. H. (2013). Issues for DSM-5: Video-Gaming Disorder? Australia and New Zealand Journal of Psychiatry, 47, 20–22. doi:10.1177/0004867412464065.
King, D. L., Delfabbro, P. H., Zwaans, T., & Kaptsis, D. (2013). Clinical Departures and Axis 1 Comorbidity of Australian Adolescent Pathological Internet and Video Game Users. Australia and New Zealand Journal of Psychiatry, 47, 1058–1067. doi:10.1177/0004867413491159.
Korn, E., & Graubard, B. I. (1999). The Analysis of Health Surveys. New York: John Wiley.
Kuss, J. D., & Griffiths, M. D. (2011). Internet Gaming Addiction: A Systematic Review of Empirical Research. International Journal of Multimedia & its Applications, 10, 278–296. doi:10.1007/s11469-011-9318-5.
McDowell, I. (2006). Measuring health: A guide to rating scales and questionnaires (3rd ed.). New York: Oxford University Press.
Mentzoni, R. A., Brunborg, G. S., Molde, H., Myrseth, H., Skouverøe, K. J., Hetland, J., & Pallesen, S. (2011). Problematic Video Game use: Estimated Prevalence and Associations with Mental and Physical Health. Cyberpsychology, Behavior and Social Networking, 14, 591–596. doi:10.1089/cyber.2010.0260.
Moffitt, T. E. (2006). Life-course-persistent versus adolescence-limited antisocial behavior. In D. Cicchetti & D. J. Cohen (Eds.), Developmental psychopathology (Risk, disorder, and adaptation, 2nd edition, Vol. 3, pp. 570–598). Hoboken, NJ: John Wiley & Sons.
Muthén, B. (2002). Should Substance use Disorder be Considered as Categorical or Dimensional? Addiction, 101, 6–16. doi:10.1111/j.1360–0443.2006.01583.x.
Muthén, L. K., & Muthén, B. O. (1998–2011). Mplus User’s Guide Version 11.2. Los Angeles, CA: Muthén and Muthén.
Nower, L., & Blaszczynski, A. (2004). The Pathways Model as Harm Minimization for Youth Gamblers in Educational Settings. Child and Adolescent Social Work Journal, 21, 25–45. doi:10.1023/B:CASW.0000012347.61618.f7.
Nylund, K. L., Asparouhov, T., & Muthén, B. (2007). Deciding on the Number of Classes in Latent Class Analysis and Growth Mixture Modeling: a Monte Carlo Simulation Study. Structural Equation Modeling, 14, 535–569.
Paglia-Boak, A., Adlaf, E. M., & Mann, R. E. (2011). Drug use among Ontario students, 1977–2011: Detailed OSDUHS findings (CAMH Research Series Document 33). Toronto, ON: Centre for Addiction and Mental Health.
Pápay, O., Urban, R., Griffiths, M. D., Nagygyorgy, K., Farkas, J., Kokonyei, G., Felvinczi, K., Olah, A., Elekes, Z., & Demetrovics, Z. (2013). Psychometric Properties of the Problematic Online Gaming Questionnaire Short-Form (POGQ-SF) and Prevalence of Problematic Online Gaming in a National Sample of Adolescents. Cyberpsychology, Behavior and Social Networking, 16, 340–348.
Patterson, B. H., Dayton, M., & Graubard, B. I. (2002). Latent Class Analysis of a Complex Sample Survey Data: Application to Dietary Data. Journal of the American Statistical Association, 97, 721–741. doi:10.1198/016214502388618465.
Pearson, N., & Biddle, S. J. (2011). Sedentary Behavior and Dietary Intake in Children, Adolescents, and Adults: a Systematic Review. American Journal of Preventive Medicine, 41, 178–188. doi:10.1016/j.amepre.2011.05.002.
Ramaswany, V., De Sarbo, W., Reibstein, D., & Robinson, W. (1993). An Empirical Pooling Approach for Estimating Marketing Mix Elasticities with PIMS Data. Marketing Science, 12, 103–124.
Rehbein, F., Psych, G., Kleimann, M., Mediasci, G., & MoBle, T. (2010). Prevalence and Risk Factors of Video Game Dependency in Adolescence: Results of a German Nationwide Survey. Cyberpsychology, Behavior and Social Networking, 13, 269–277. doi:10.1089/cyber.2009.0227.
Tejeiro Salguero, R. A., & Morán, R. M. B. (2002). Measuring Problem Video Game Playing in Adolescents. Addiction, 97, 1601–1606. doi:10.1046/j.1360–0443.2002.00218.x.
Tejeiro Salguero, R. A., Gomez-Vallecillo, J. L., Pelegrina, M., Wallace, A., & Emberley, E. (2012). Risk Factors Associated with the Abuse of Video Games in Adolescents. Psychology, 3, 310–314. doi:10.4236/psych.2012.34044.
Tremblay, M. S., LeBlanc, A. G., Kho, M. E., Saunders, T. J., Larouche, R., Colley, R. C., Goldfield, G., & Connor Gorber, S. (2011a). Systematic Review of Sedentary Behaviour and Health Indicators in School-Aged Children and Youth. International Journal of Behavioural Nutrition and Physical Activity, 8, 98. doi:10.1186/1479–5868–8–98.
Tremblay, M. S., Leblanc, A. G., Janssen, I., Kho, M. E., Hicks, A., Murumets, K., Colley, R. C., & Duggan, M. (2011b). Canadian Sedentary Behaviour Guidelines for Children and Youth. Applied Physiology, Nutrition, and Metabolism, 36, 59–71. doi:10.1139/H11–012.
Turner, N. E., Jain, U., Spence, W., & Zangeneh, M. (2008). Pathways to Pathological Gambling: Component Analysis of Variables Related to Pathological Gambling. International Gambling Studies, 8, 281–298.
Turner, N. E., Ialomiteanu, A., Paglia-Boak, A., & Adlaf, E. M. (2011). A Typological Study of Gambling and Substance Use Among Adolescent Students. Journal of Gambling Issues, 25, 88–107. doi:10.4309/jgi.2011.25.7.
Turner, N. E., Paglia-Boak, A., Ballon, B., Cheung, J. T. W., Adlaf, E. M., Henderson, J., Chan, V., Rehm, J., Hamilton, H., & Mann, R. E. (2012). Prevalence of Problematic Video Gaming Among Ontario Adolescents. International Journal of Mental Health and Addiction, 10, 877–889. doi:10.1007/s11469–11012–19382–11465.
Van Rooij, A. J., Schoenmakers, T. M., Vermulst, A. A., van den Eijnden, R. J. J. M., & van de Mheen, D. (2010). Online Video Game Addiction: Identification of Addicted Adolescent Gamers. Addiction, 106, 205–212. doi:10.1111/j.1360–0443.2010.03104.x.
Vermunt, J. K. (2008). Latent Class and Finite Mixture Models for Multilevel Data Sets. Statistical Methods in Medical Research, 17, 33–51.
Vermunt, J. K., & Magidson, J. (2002). Latent Class Cluster Analysis. In J. A. Hagenaars & A. L. McCutcheon (Eds.), Applied Latent Class Analysis (pp. 89–106). New York: Cambridge University Press.
World Health Organization. (2011). BMI Classification. Retrieved September 27, 2013, from http://apps.who.int/bmi/index.jsp?introPage=intro_3.html.
Acknowledgments
Preparation of this work was funded in part by ongoing support from the Ontario Ministry of Health and Long Term Care. We would like to thank all the schools and students that participated in the study, and the Institute for Social Research at York University for assistance with the survey design and data collection.
Conflict of Interest
The authors do not have a financial relationship with the organization that sponsored the research. Guy Faulkner, Hyacinth Irving, Edward Adlaf and Nigel Turner declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Faulkner, G., Irving, H., Adlaf, E.M. et al. Subtypes of Adolescent Video Gamers: a Latent Class Analysis. Int J Ment Health Addiction 13, 1–18 (2015). https://doi.org/10.1007/s11469-014-9501-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11469-014-9501-6