
Abstract
The amount of axial rotation in the tibia caused by high tibial osteotomy is relatively unknown. The authors hypothesize that the coronal plane high tibial osteotomy, a novel technique used to treat varus malalignment, alters the axial rotation of the tibia less than the opening wedge high tibial osteotomy. Eight, embalmed, stripped cadaveric tibia–fibula constructs with intact interosseous membranes were randomized to either opening wedge or coronal plane high tibial osteotomies. Sequential valgus corrections of 5°, 10°, and 15° were performed. The Qualisys Track Manager motion capture system was used to measure axial rotation. Student’s t test was used to compare axial rotation between the two groups. A p value of 0.05 was determined to be significant. The coronal plane technique produced rotations about the tibial axis that were statistically significantly smaller than those of the opening wedge technique for all correction angles (1.2° internal rotation (IR) vs 16° external rotation (ER), respectively, at 5° correction; p = 0.02) (3.5° IR vs 21.2° ER at 10° correction; p = 0.04) (4.5° IR vs 23.0° ER at 15° correction; p = 0.01). The coronal plane high tibial osteotomy alters axial rotation of the tibia significantly less than the opening wedge high tibial osteotomy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Patients with varus deformity of the knee are at risk for developing medial compartment osteoarthritis. High tibial osteotomy is a surgical intervention that can correct the malalignment and either eliminate or slow the progression of osteoarthritis. Coventry [1] popularized the use of the closing wedge osteotomy for treatment of varus gonarthrosis of the knee where a wedge of bone was removed from the lateral aspect of the tibial plateau to correct the varus malalignment. The opening wedge osteotomy is another option for treating varus gonarthrosis of the knee [2–4]. Instead of removing a wedge of bone from the lateral aspect of the tibial plateau, a wedge of autograft, allograft, or bone graft substitute is inserted into the medial aspect of the tibial plateau to correct the varus malalignment. A third type of osteotomy, the coronal plane osteotomy, was developed at this institution to treat varus gonarthrosis. Whereas the closing and opening wedge techniques employ an osteotomy in the axial plane, the coronal plane osteotomy technique uses an osteotomy in the sagittal plane. The distal tibia is then rotated around an axis in the coronal plane to correct the varus malalignment.
Coventry noted in his original paper that “rotation (in the axial plane) is completely controlled” using the closing wedge technique. However, Magyar et al. [5], 1999, using radiostereometric analysis, found that the closing wedge technique had significantly higher rotations about the tibial axis after 1 month and 1 year when compared with the opening wedge surgical technique. The coronal plane osteotomy has not been examined to determine the amount of axial rotation that occurs when valgus correction is performed.
The objective of this study was to compare the valgus-correcting coronal plane high tibial osteotomy with the valgus-correcting opening wedge high tibial osteotomy to determine if there was a difference in the degree of axial rotation.
Method and materials
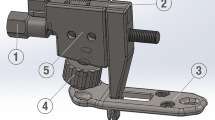
Eight embalmed cadaveric tibia–fibula constructs were dissected free of all muscles and tendons. The interosseous membrane and the proximal and distal tibia–fibula joints remained intact. Each specimen was randomly assigned to either an opening wedge or coronal plane osteotomy group. Plates with infrared reflective markers were attached to the tibial plateau and tibial plafond to define the long axis of the tibia and the rotations about this axis that resulted from the osteotomies (Fig. 1).

Tibia–fibula specimen with marker plates attached and mounted in the clamp. Markers 1 and 2 were positioned to define the long axis of the tibia. The markers on each plate were used to define local coordinate systems from which the relative rotations were determined
After the plates were attached, the specimens were stabilized on a clamp, and the three-dimensional locations of the markers were recorded using a motion capture system (Qualisys Track Manager, Gothenburg, Sweden) (Fig. 2). The specimen was then removed from the clamp, and one of the two osteotomies (opening wedge or coronal plane) was performed to obtain a 5° correction. The specimen was placed back in the clamp and the marker locations recorded once again. This sequence was repeated for additional corrections of 10° and 15°. The order of the osteotomies performed on the eight tibias was alternated (n = 4 for each type).

Qualisys Track Manager motion capture system (Qualisys, Gothenburg, Sweden)
The opening wedge osteotomy technique was performed by making a transverse cut in the tibia proximal to the tibial tubercle in the metaphyseal bone. The cut was started on the medial tibia and taken to the lateral cortex. Care was taken not to perforate the lateral cortex. Next, an osteotome jack (Arthrex, Naples, FL) was inserted into the osteotomy up to the lateral cortex. The transverse width of the tibia was measured at the level of the osteotomy. The desired amount of opening at the medial cortex was determined by the following equation:
Once the desired medial tibial opening was achieved, the correction was fixed using a tibial opening wedge osteotomy plate (Arthrex, Naples, FL) (Fig. 3). For each specimen in the opening wedge osteotomy group, 5°, 10°, and 15° of correction was sequentially obtained, fixed with the medial plate, and measured. All specimens in the opening wedge osteotomy group had an intact fibula and proximal tibia–fibula joint.

Opening Wedge High Tibial Osteotomy
The coronal plane osteotomy requires a fibular osteotomy to allow for valgus correction after the tibial osteotomy. The fibular osteotomy was made with a sagittal saw in the midshaft fibula in a supero-lateral to infero-medial direction. Before creation of the tibial osteotomy, two preliminary drill holes were drilled in the tibial tubercle with a 4.5-mm drill. Next, the tibial osteotomy was started on the lateral aspect of the tibia proximal to the tibial tubercle. The osteotomy was made obliquely starting at the anterior cortex and extending distally to the posterior cortex. Once the cut was started at this oblique angle, it was continued to the medial cortex. A sagittal saw was used to start the osteotomy, and osteotomes were used to complete it. Just before completion of the osteotomy, a smooth Steinman pin was temporarily placed across the osteotomy site to act as a pivot and provide rotational control. After completion of the osteotomy, a valgus force was placed on the distal piece, and the angular correction was performed. A bone holding forceps was used to hold the proximal and distal fragments stable once the appropriate correction was made. A goniometer was used to confirm precise angular correction. Two 4.5-mm cortical screws were used to compress and stabilize the osteotomy site in an anterior to posterior direction. Sequential 5°, 10°, and 15° corrections were made, fixated, and measured for each specimen in the coronal plane osteotomy group.
The marker coordinates from the intact specimens and the 5°, 10°, and 15° osteotomies were input into EVaRT software (Motion Analysis Corporation, Santa Rosa, CA). The multiple markers on the two plates were used to define local coordinate systems. The marker closest to the bone defined the long axis of the tibia. The relative rotation of the proximal coordinate system with respect to the distal coordinate system was determined for each step (intact, 5°, 10°, and 15°) and the rotation with respect to the intact determined by subtracting the intact rotation from those determined in each of the subsequent osteotomy steps.
For each of the three corrections, the rotations with the opening wedge technique were compared with those from the coronal plane technique using Student’s t tests. Because the goal of the osteotomy is to avoid rotation, t tests were also performed to compare results from each technique to 0° of rotation. All p values were considered statistically significant at 0.05.
Results
The coronal plane technique produced rotations about the tibial axis that were significantly smaller than those of the opening wedge technique (Tables 1 and 2, Fig. 4). The reduction in rotation with the coronal plane techniques was significantly smaller at all correction angles (5°: p = 0.02; 10°: p = 0.04; and 15°: p = 0.01). The rotations measured after the coronal plane osteotomies were not significantly different from 0 (p = 0.88), while those measured after the opening wedge osteotomies were significantly different from 0 (p = 0.03). For both osteotomy groups, a linear increase in axial rotation occurred with the degree of valgus correction.

Rotations about the long axis of the tibia for the coronal plane and opening wedge osteotomies. External rotation is positive, and internal rotation is negative. Asterisks = significantly larger than with the coronal plane technique
Discussion
This study suggests that the coronal plane high tibial osteotomy does not significantly alter axial rotational alignment, whereas the opening wedge high tibial osteotomy does. Changes in axial alignment may affect knee kinematics, contact forces across the knee, and gait. Thus, the coronal plane osteotomy may have a clinical advantage in improving outcomes that depend on rotational alignments. Further studies will have to be performed to determine the significance of axial rotation alterations.
The increased external rotation after the opening wedge osteotomy is likely due to the intact fibula and tibia–fibula joint. The intact fibula acts as a strut resisting angular correction, and increased tension develops in the tibia–fibula construct that is relieved by the tibia rotating around the intact fibula. The coronal plane osteotomy requires a fibular osteotomy, which allows for a coronal plane correction without the concomitant alteration in the rotation of the lower extremity.
A limitation of this study was that the bones had been stripped of muscles and tendons and the knee and ankle joints disarticulated. Thus, the effects of the superficial soft tissues on rotation are not accounted. As the objective was to measure relative change in rotation before and after osteotomies, the lack of soft tissue and joints should not affect the results. In addition, this study does not examine the dynamic effects of the rotation or the ramifications of these rotational changes on gait, kinematics, or force transmission at the knee. Another limitation was that the specimens were embalmed which changes the material properties of the bone. This was not considered a factor in this study because biomechanical testing was not performed.
Conclusions
The coronal plane high tibial osteotomy, a novel technique for correcting valgus malalignment at the knee, alters axial rotation of the tibia significantly less than the opening wedge high tibial osteotomy.
References
Coventry MB (1965) Osteotomy of the upper portion of the tibia for degenerative arthritis of the knee. A preliminary report. J Bone Jt Surg Am 47:984–990
Hernigou P, Medevielle D, Debeyre J, et al. (1987) Proximal tibial osteotomy for osteoarthritis with varus deformity. A ten to thirteen-year follow-up study. J Bone Jt Surg Am 69(3):332–354
Koshino T, Murase T, Saito T (2003) Medial opening-wedge high tibial osteotomy with use of porous hydroxyapatite to treat medial compartment osteoarthritis of the knee. J Bone Jt Surg Am 85-A(1):78–85
Kwok T (1992) Open wedge high tibial osteotomy using allo and autogenous bone grafts. J West Pac Orthop Assoc 29:93–97
Magyar G, Toksvig-Larsen S, Lindstrand A (1999) Changes in osseous correction after proximal tibial osteotomy: radiostereometry of closed- and open-wedge osteotomy in 33 patients. Acta Orthop Scand 70(5):473–477
Acknowledgements
We would like to thank the Arthrex Corporation for donating their Tibial Opening Wedge Osteotomy System. In addition, we would like to thank Mark Lenhoff for assistance in reducing the axial rotation data.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Baumgarten, K.M., Meyers, K.N., Fealy, S. et al. The Coronal Plane High Tibial Osteotomy. Part II: A Comparison of Axial Rotation with the Opening Wedge High Tibial Osteotomy. HSS Jrnl 3, 155–158 (2007). https://doi.org/10.1007/s11420-007-9046-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11420-007-9046-3