
Abstract
The mechanism of pain relief of intradiskal electrothermal annuloplasty (IDET) in the treatment of lumbar diskogenic pain is uncertain. Theories include sealing of annular fissures via collagen denaturation and contraction. Prior studies offer conflicting qualitative data on the ability of IDET to denature collagen. The objective of the present study is to evaluate IDET treatment effect onannular collagen using quantitative data supplied by Fourier-transform infrared imaging spectroscopy.
The posterior annulus of disks (n = 3) from an intact human cadaveric spine at room temperature were treated with two different radiothermal catheters using standard intradiskal electrothermal annuloplasty (IDET) heating protocols. Disks were dissected free with catheters in place and fixed in formalin. Channels created by the catheters were marked and catheters were removed. Tissue samples of treated areas adjacent to the channels and internal control areas from the same disk were stained for light microscopy and placed on barium sulfate windows for Fourier transform infrared imaging spectroscopy (FT-IRIS) analysis.
Treated areas showed evidence of disruption in the fibrillar organization of annular collagen by light microscopy compared to intact stroma from control areas. Quantitative FT-IRIS analysis compared ratios of wavenumber regions known to be sensitive to collagen denaturation. Mean values for the ratios amide II/1,338 cm−1 (137.21 ± 25.84 treated, 76.94 ± 16.77 control) and 1,640/1,660 cm−1 (0.98 ± 0.03 treated, 0.89 ± 0.03 control) were significantly different between treated and control samples (p < 0.001), indicating a breakdown in collagen integrity. Separate analysis by catheter type suggests that catheter design may impact treatment effect.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Chronic lumbar diskogenic pain (CLDP) has been largely attributed to internal disk disruption and/or subsequent degenerative disk disease [1–3]. Intradiskal electrothermal therapy (IDET) provides an alternative therapeutic option to lumbar fusion in patients with CLDP unresponsive to more conservative management. Introduced in 1997, the procedure involves fluoroscopically guiding a flexible heating electrode circumferentially into the posterior annulus of a painful disk [4]. Several long-term prospective studies, including a randomized, placebo-controlled trial (January 2004) [5–9], have demonstrated statistically significant improvement in both pain and function following IDET in a selected subset of patients with CLDP.
Despite published clinical and basic science studies, the precise mechanism of pain relief from annular heating remains elusive. Theories address both the anatomic and biochemical aspects of CLDP. Coagulation of annular nociceptors, sealing of annular fissures via collagen denaturation and contraction, and cauterization of granulation tissue have been proposed mechanisms along with changes in concentrations of intradiskal inflammatory mediators [10–12]. Of these theories, collagen denaturation with subsequent disk shrinkage is supported by the application of thermal coagulation for shrinkage and tightening of capsular collagen in the treatment of shoulder and ankle instability [13–15].
Further investigation of the collagen denaturation theory includes biomechanical and histological studies. To date, studies reporting data on the biomechanical effects of the IDET-treated disk have been concordant. In 2001, Shah et al [16] and Kleinstueck et al [17] found no significant acute destabilizing effect on spinal stability in vitro. However, histological studies of the IDET-treated disk have demonstrated conflicting results. In the aforementioned studies, Shah et al also observed collagen coalescence and stromal disorganization consistent with denaturation in human cadaveric IDET-treated disks. In contrast, Kleinstueck et al [18] did not observe any collagen changes or stiffening of the IDET-treated disk and suggested that IDET did not reach temperatures sufficient to induce collagen denaturation and coalescence.
In order to further investigate the theory of collagen denaturation and elucidate its role in the IDET-treated disk, this study utilized the technique of Fourier transform infrared imaging spectroscopy (FT-IRIS). FTIR spectroscopy has been shown to be a powerful tool in the evaluation of collagen cross-linking [19] and in the study of molecular changes associated with collagen structure [20]. Although traditional light and electron microscopy techniques are useful for morphological evaluation of tissues and their components, they are limited in their ability to assess molecular changes. In contrast, FTIR analysis is based on monitoring vibrations that originate from molecular components in tissues. Accordingly, evaluation of changes in molecular structure, such as collagen denaturation, can be carried out by direct analysis of spectral absorbances. In the current study, FT-IRIS was used to quantitatively and qualitatively evaluate the effects of IDET on type II collagen structure in a human cadaveric intervertebral disk annulus.
Currently, two types of intradiskal catheters are manufactured for electrothermal therapy: the SpineCATH (Smith and Nephew, Andover, MA, USA) and the electrothermal Decompression catheter (Smith and Nephew, Andover, MA, USA). The SpineCATH applicator has a 5-cm heating segment, whereas the decompression catheter consists of a 3-cm heating segment. Studies comparing the ability of both catheters to denature collagen in the IDET procedure have not yet been published. An additional aim of this study was to use FTIR to generate objective evidence of collagen denaturation using two different IDET catheters.
Materials and methods
IDET procedure
Five lumbar disks were treated in a single human cadaveric spine. Prior to use the torso was thawed to allow catheter placement within the disk. Generation II 17-gauge introducers were positioned within the ipsilateral anterior disk quadrant under fluoroscopy. Either a SpineCATH or a Decompression catheter (Smith and Nephew, Boston, MA, USA) were threaded through the introducers and placed across the posterior annulus of each disk. Anterior–posterior, lateral, and oblique fluoroscopic projections were taken to guide the catheter placement.
The standard P90 high heating protocol was used for the SpineCATH catheters, starting at 65°C and advanced 1°C every 30 s up to a 90°C maximum over 16.5 min. The AutoTemp mode on the Ora-50™S generator (Smith and Nephew, Boston, MA) was used for the SpineCATH catheters. The Temperature Control mode was used with the Decompression catheters starting at 50°C and advancing 5°C every 30 s up to a 90°C maximum over 13.5 min. SpineCATH catheters were inserted at the L1–L2, L2–L3, and L5–S1 levels. Decompression catheters were inserted at the L3–L4 and L4–L5 levels. Radiopaque marks on each catheter were clearly observed outside each of the introducer needles.
Preservation of catheter channel
Each disk was dissected free with the catheter left in situ. The specimens were fixed in 10% buffered formalin for 1 week. Using a sewing needle and blue nylon thread, loops were thrown around the catheter's distal segments to immortalize the path of the catheter following histologic processing. The needle was inserted perpendicular to the endplate and redirected until contact was made with the catheter. The needle with thread was then passed completely through the disk immediately adjacent to the catheter. It was then rethreaded through the disk in a similar fashion adjacent to the opposite edge of the catheter, and the ends of the thread were knotted. The catheters were then pulled from the disks.
Slide preparation
Specimens were decalcified in 10% ethylenediaminetetraacetic acid (EDTA) and embedded in paraffin. Sections, 6μm thick, from each disk specimen were microtomed and placed onto barium fluoride infrared windows for evaluation by FTIR spectroscopy. Additional specimens were sectioned, placed on glass microscope slides, and stained for histological analysis.
FTIR imaging spectroscopy
Specimens prepared on barium fluoride windows were imaged in transmission mode at 8 cm−1 under N2 purge using a Digilab (Cambridge, MA, USA) UMA 300A FTIR microscope with an FTS-60A step scanning FTIR spectrometer and a 64×64 MCT Focal Plane Array detector (Santa Barbara Focal Plane, Golota, CA, USA). Spectral information was obtained from 400×400 μm2 regions resulting in 4,096 individual spectra for each scan. Image analysis was performed using Isys Image Analysis software (Spectral Dimensions, Olney, MD, USA).
The spectra were baselined and the collagen absorbances were monitored in the 1,690–1,600, 1,590–1,480, and the 1,338 cm−1 spectral regions. The primary molecular vibrations associated with these wavenumber absorbances are the amide I carbonyl stretch (C=O) [21–25], the amide II out-of-phase, in-phase N–H deformation and C–N stretch [24–28], and the CH2 side chain vibrations [26–28], respectively (Fig. 1). Spectra were evaluated for shifts in the amide I contour and changes in the amide II/1,338 cm−1 area ratio. Ratios were taken to avoid errors that could be incurred as a result of concentration-dependent changes in spectral absorbance.

FTIR collagen spectrum
As collagen denatures, order within the triple helix becomes disrupted because of the rearrangement of hydrogen bonds and changes in the interactions between amide groups. This results in changes in the conformational arrangement of collagen that can be monitored spectroscopically. Consequently, the structure sensitive peak at 1,338 cm−1 decreases [29, 30], resulting in an increased amide II/1,338 cm−1 ratio [20]. Also, shifts in the amide I contour from 1,660 cm−1 to lower wavenumbers have been known to accompany collagen denaturation [31] resulting in an increase in the 1,640/1,660 cm−1 intensity ratio.
Tissues immediately adjacent to the channels created bythe catheter were chosen as treatment areas for analysis.Internal controls were taken from each disk in areas in the anterior annulus farthest removed from these channels in the posterior annulus as well as from tissue within several millimeters of the channels. Internal controls were chosen so that localized changes due to heating could beeasily assessed adjacent to the channels and away from the channels.
Statistical analysis
Mean values and standard deviations of the peak area ratios (amide II/1,338 cm−1 and 1,640/1,660 cm−1) were calculated for treatment and controls. Student's t-test was applied to the two sets of data with statistical significance determined at p < 0.05. SPSS version 9.0 software was utilized for data analysis.
Results
Annuloplasty
Placement of the catheters within the disk was made with difficulty as a result of the degenerative nature of the cadaveric torso at nonphysiologic temperature. Navigation of the catheter around obstructions in the disk was necessary to attain adequate position. Catheter placement spanning the entire posterior annulus in an optimal position forheating was obtainable in three out of the five disk levels.
Cadaveric spine
The specimen, dissected free of the torso, confirmed the fluoroscopic and procedural impression of moderate to severe lumbar disc degeneration. Diffuse posterior and lateral disk bulges were noted at all levels with the more severe degenerative changes at L3–L4 and inferior levels. There were osteophytic projections of the superior and inferior endplates of L3–L4, L4–L5, and L5–S1 with hypertrophy of the zygapophoseal joints bilaterally at each level.
Disk morphology
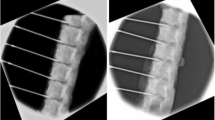
Due to these technical difficulties, only disks at the L1–L2, L2–L3, and L4–L5 levels were included in the analysis. SpineCaths were used at the twohigher levels, whereas a decompression catheter wasused at the L4–L5 level. Disk preparation was successful in preserving the channels created by the catheter at each level. Channels in the posterior annulus bordered by nylon thread clusters were evident on light microscopy (Fig. 2).

Posterior annulus with catheter channel marked by nylon threads (black arrows)
Histology
Tissues in the posterior annulus bordering the channels exhibited loss of organization in the stromal structure. Picrosirius red stain, specific for collagen, and hemotoxylin and eosin staining revealed hyalinization of collagen, globular forms, and apparent vacuole formation (Fig. 3). These changes are consistent with what might be expected as a result of thermal injury to nonvital tissue. Control specimens from the anterior annulus, by contrast, showed no histological evidence of damage. A normal annular appearance and stromal organization with a nondisrupted fibrillar arrangement of collagen was observed in all specimens (Fig. 4).

H/E stain of treated annular tissue adjacent to channel (top)

H/E stain of control annular tissue
FT-IRIS analysis
Quantitative FT-IRIS analysis was performed on treated sections immediately adjacent to the channels. Figure 5 isan FT-IR image showing the amide II/1,338 cm−1 ratio distribution in this area. The mean value of the ratio of thetreated areas was 137.21 ± 25.8, whereas the value forcontrol areas away from the channels was 76.94 ± 16.77. Similarly, Figure 6 shows the FT-IRIS image of the1,640/1,660 cm−1 intensity ratio shift and distribution. Again, higher values indicating greater degradation wereobserved in areas next to the channels (0.98 ± 0.03 vs 0.89 ± 0.03). The increase in values of the treated areas compared to controls was highly significant for both outcome ratios (p < 0.001) (Table 1). This treatment effect was seen at distances up to 1 mm from the channel. The mean values for both ratios dropped to control levels atgreater distances.

a Light microscopy view of the treated disk sample (channel in upper right corner). b Amide II/1,338 cm−1 ratio distribution in treated sample (channel dark blue in upper-right corner)

1,640/1,660 cm−1 ratio distribution. Channel dark blue in upper-right corner
Catheter type
Findings were consistent in histology among levels using the SpineCath and the single level at which a decompression catheter was used. Evidence for stromal disorganization was similar in quality in areas bordering the channels.
Amide II/1,338 cm−1 ratios were significantly increased relative to controls in all treated specimens regardless of catheter type. However, analysis of 1,640/1,660 cm−1 ratios by catheter type revealed treatment areas in the SpineCath disks to be significantly increased relative to controls (p = 0.01), whereas no significant difference was found in the disk treated with the Decompression catheter (p = 0.67).
Discussion
In this study, qualitative visual evidence of collagen denaturation by light microscopy following IDET annuloplasty in human cadaveric disks is supported by the quantitative evidence of alteration in collagen structure as determined by FT-IRIS analysis. The spectral peak area ratios in treated areas were significantly increased relative to control areas indicative of disruption in collagen secondary structure and conformational changes accompanying denaturation. A separate analysis of the quantitative data suggests that catheter design may affect the efficiency in heating annular collagen to temperatures sufficient to cause denaturation of its secondary structure.
The effect of annuloplasty on collagen was noted only in the tissues immediately adjacent to the channels created by the catheters. Several factors in the present study worked to mitigate the size of this effect. These include the partially frozen nature of the specimen and the advanced native degeneration of the cadaveric disks.
Reduced disk temperatures have an obvious impact on the thermal treatment of annular collagen. The standard heating protocols were not altered for the study; there was no increase in temperature or prolongation of time of application. Temperature within the specimens was above freezing but lower than room temperature and far below physiologic temperatures of the in vivo disk. It is reasonable to assume that the time required to reach the maximum temperatures within the disks were prolonged thus shortening the heating time and possibly reducing the maximum temperatures attained. More than the other factors, this would greatly attenuate the IDET treatment effect on collagen both at the immediate interface with the catheter as well as in adjacent annular tissue. Nevertheless, temperatures created by the catheter were sufficient to effect conformational change in collagen structure however blunted the treatment may have been by the nonphysiologic temperatures in the disk at the time of procedure.
The degenerative condition of the cadaveric spine used for the study may also have reduced the potential treatment effect. These factors may have contributed to pretreatment collagen denaturation in the disks sufficient to raise baseline values of the spectral peak ratios sensitive to such changes thus narrowing the difference in ratio values between treated and control areas. In other words, healthier, less-degenerated disks at baseline may have shown a greater treatment effect because they had more intact collagen to denature.
The main difference in design of the two catheter types used in this study is the length of the distal heating coil. The SpineCath catheter is longer at 5 cm compared with 3 cm in the decompression catheter. As a result, the effective channel length created by each catheter differs as well. During catheter preservation, every effort was made to mark the annulus in the most distal portion of the channels. However, there is an increased margin for error with a smaller effective channel length. Mismarking the decompression catheter channel proximal to the heating filament could have adversely affected the FTIR data.
More pertinent than catheter design may be the differences in the associated heating protocols. Both reached maximum temperatures of 90°C but the SpineCath protocol begins at a higher temperature (65 vs 50°C) and lasts longer (16.5 vs 13.5 min). Greater thermal energy applied for a greater period of time may equal greater efficiency in altering collagen secondary structure.
It is also important to note that the sample size, two disks compared with one, in the analysis of the SpineCath and decompression catheters, may simply have been too small for an accurate comparison of type.
Findings of this study confirm that both catheter types denature the collagen of the annulus as confirmed by FT-IRIS analysis. The clinical relevance of these findingslies in the alteration of intervertebral disk annular structure. Although they do not establish the mechanism of pain relief obtainable through IDET in patients with lumbar diskogenic pain, the data support the proposed anatomic theories mentioned previously. Neither do they exclude possible biochemical changes induced within the disk thatmay also contribute to the clinical effect of the procedure.
The significance of this study is that FT-IRIS allows for a quantitative analysis of the thermal effects on disk collagen of these treatment methods. Further studies with larger sample sizes are needed to determine which catheter may have a better potential therapeutic effect. In addition, FT-IRIS analysis can be used to evaluate not only the effects of different catheter designs, but also of different heating protocols.
References
AC Schwarzer CN Aprill R Derby et al. (1995) ArticleTitleThe prevalence and clinical features of internal disc disruption in patients with chronic low back pain Spine 20 1878–1883 Occurrence Handle1:STN:280:DyaK28%2FmtVWntA%3D%3D Occurrence Handle8560335
M Karasek N Bogduk (2000) ArticleTitleTwelve-month follow-up of a controlled trial of intradiscal thermal annuloplasty for back pain due to internal disc disruption Spine 25 IssueID20 2601–2607 Occurrence Handle1:STN:280:DC%2BD3M%2FkvVWnsw%3D%3D Occurrence Handle11034644
C O'Neill R Derby L Kenderes (1999) ArticleTitlePrecision injection techniques for diagnosis and treatment of lumbar disc disease Semin Spine Surg 11 104–118
JS Saal JA Saal (2000) ArticleTitleManagement of chronic discogenic low back pain with a thermal intradiscal catheter: a preliminary report Spine 25 382–388 Occurrence Handle10.1097/00007632-200002010-00021 Occurrence Handle1:STN:280:DC%2BD3c7mslOmuw%3D%3D Occurrence Handle10703114
KJ Pauza S Howell P Dreyfuss JH Peloza K Dawson N Bogduk (2004) ArticleTitleA randomized, placebo-controlled trial of intradiscal electrothermal therapy for the treatment of discogenic low back pain Spine J 4 27–35 Occurrence Handle10.1016/j.spinee.2003.07.001 Occurrence Handle14749191
C Lutz GE Lutz PM Cooke (2003) ArticleTitleTreatment of chronic lumbar diskogenic pain with intradiskal electrothermal therapy: a prospective outcome study Arch Phys Med Rehabil 84 IssueID1 23–28 Occurrence Handle10.1053/apmr.2003.50059 Occurrence Handle12589616
MS Lee G Cooper GE Lutz C Lutz HM Hong (2003) ArticleTitleIntradiscal electrothermal therapy (IDET) for treatment of chronic lumbar discogenic pain: a minimum 2-year clinical outcome study Pain Physician 6 IssueID4 443–448 Occurrence Handle16871296
JA Saal JS Saal (2002) ArticleTitleIntradiscal electrothermal treatment for chronic discogenic low back pain. Prospective outcome study with a minimum 2-year follow-up Spine 27 966–974 Occurrence Handle11979172
N Bogduk M Karasek (2002) ArticleTitleTwo-year follow-up of a controlled trial of intradiscal electrothermal anuloplasty for chronic low back pain resulting from internal disc disruption Spine J 2 343–350 Occurrence Handle10.1016/S1529-9430(02)00409-6 Occurrence Handle14589465
BJC Freeman RM Walters RJ Moore RD Fraser (2003) ArticleTitleDoes intradiscal electrothermal therapy denervate and repair experimentally induced posterolateral annular tears in an animal model? Spine 28 IssueID23 2602–2608 Occurrence Handle14652477
M Karasek N Bogduk (2001) ArticleTitleIntradiscal electrothermal annuloplasty: percutaneous treatment of chronic discogenic low back pain Tech Reg Anesth Pain Manag 5 130–135 Occurrence Handle10.1053/trap.2001.25284
JC Houpt ES Conner EW McFarland (1996) ArticleTitleExperimental study of temperature distributions and thermal transport during radiofrequency current therapy of the intervertebral disc Spine 21 1808–1813 Occurrence Handle10.1097/00007632-199608010-00018 Occurrence Handle1:STN:280:DyaK2s%2FgvVehsQ%3D%3D Occurrence Handle8855467
MS Wall XH Deng P Torzilli et al. (1999) ArticleTitleThermal modulation of collagen J Shoulder Elb Surg 8 339–344 Occurrence Handle1:STN:280:DyaK1MvgtFahtQ%3D%3D
K Hayashi KL Massa GR Thabit et al. (1999) ArticleTitleHistologic evaluation of the glenohumeral joint capsule after the laser-assisted capsular shift procedure for glenohumeral instability Am J Sports Med 27 162–167 Occurrence Handle1:STN:280:DyaK1M3gt1ehsQ%3D%3D Occurrence Handle10102095
SL Obrzut P Hecht K Hayashi et al. (1998) ArticleTitleThe effect of radiofrequency energy on the length and temperature properties of the glenohumeral joint capsule Arthroscopy 14 395–400 Occurrence Handle1:STN:280:DyaK1c3otF2ksQ%3D%3D Occurrence Handle9620651 Occurrence Handle10.1016/S0749-8063(98)70007-6
RV Shah GE Lutz J Lee SB Doty S Rodeo (2001) ArticleTitleIntradiskal electrothermal therapy: a preliminary histologic study Arch Phys Med Rehabil 82 1230–1237 Occurrence Handle10.1053/apmr.2001.23897 Occurrence Handle1:STN:280:DC%2BD3Mrgt1ygsw%3D%3D Occurrence Handle11552196
FS Kleinstueck CJ Diederich WH Nau CM Puttlitz JA Smith DS Bradford JC Lotz (2001) ArticleTitleAcute biomechanical and histological effects of intradiscal electrothermal therapy on human lumbar discs Spine 26 IssueID20 2198–2207 Occurrence Handle10.1097/00007632-200110150-00009 Occurrence Handle1:STN:280:DC%2BD3Mrlt1Wjuw%3D%3D Occurrence Handle11598508
FS Kleinstueck CJ Diederich WH Nau et al. (2003) ArticleTitleTemperature and thermal dose distributions during intradiscal electrothermaltherapy in the cadaveric lumbar spine Spine 28 IssueID15 1700–1708 Occurrence Handle10.1097/00007632-200308010-00013 Occurrence Handle12897495
EP Paschalis K Verdelis SB Doty AL Boskey et al. (2001) ArticleTitleSpectroscopic characterization of collagen cross-links in bone J Bone Miner Res 16 IssueID10 1821–1828 Occurrence Handle1:CAS:528:DC%2BD3MXnsVKqt7c%3D Occurrence Handle11585346
PA West MPG Bostrom PA Torzilli PA Camacho (2004) ArticleTitleFourier transform infrared spectral analysis of degenerative cartilage: an infrared fiber optic probe and imaging study Appl Spectrosc 58 IssueID4 367–381 Occurrence Handle10.1366/000370204773580194
T Miyazawa T Shimanouchi S Mizushima (1958) J Chem Phys 29 611 Occurrence Handle1:CAS:528:DyaG1MXhtVemsw%3D%3D
JL Arrondo A Muga J Castresana FM Goni (1993) Prog Biophys Mol Biol 59 23 Occurrence Handle1:CAS:528:DyaK3sXns1ehtA%3D%3D Occurrence Handle8419985
Griebenow K, Santos A, Carrasqillo, K (1998) Secondary structure of proteins in the amorphous dehydrated state probed by FTIR spectroscopy. Internet J. Vib. Spectrosc. Bol. 3, Ed. 1
B Stuart B George P McIntyre (1996) Modern Infrared Spectroscopy Wiley New York
Jackson M, Choo LP, Watson PH, Halliday WC, Mantsch HH (1995) Biochim Biophys Acta 1270
M Reza Oboodi C Alva M Diem (1984) J Phys Chem 88 501
GM Roberts O Lee J Calienni M Diem (1998) J Am Chem Soc 110 1749
M Diem O Lee GM Roberts (1992) J Phys Chem 96 548 Occurrence Handle10.1021/j100181a011 Occurrence Handle1:CAS:528:DyaK38XntV2isQ%3D%3D
Jackson M, Choo LP, Watson PH, Halliday WC, Mantsch HH (1995) Biochim Biophys Acta 1270
Y Lazarev AV Lazareva (1978) Biopolymers 17 1197 Occurrence Handle1:CAS:528:DyaE1cXltFSgt7Y%3D
KJ Payne A Veis (1988) ArticleTitleFourier transform IR spectroscopy ofcollagen and gelatin solutions: deconvolution of the amide I band for conformational studies Biopolymers 27 IssueID11 1749–1760 Occurrence Handle10.1002/bip.360271105 Occurrence Handle1:CAS:528:DyaL1MXjs1eguw%3D%3D Occurrence Handle3233328
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Southern, D., Lutz, G., Bracilovic, A. et al. Histological and Molecular Structure Characterization of Annular Collagen after Intradiskal Electrothermal Annuloplasty. HSS Jrnl 2, 49–54 (2006). https://doi.org/10.1007/s11420-005-0126-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11420-005-0126-y