
Abstract
Several studies have been published about the potential health effects due to long-term exposure to sulphur dioxide (SO2) and the relative risks (RRs) for different causes of mortality. Broad differences in the RR values are found, however. In this study, we performed an analysis of these studies aiming finding potential explanations for the high variability of the RR reported. The RRs for stratified subgroups were also analysed to identify more susceptible subgroups. A total of 14 studies were identified. Some of them related strong associations between mortality and long-term ambient SO2 exposure, while others found insignificant or no associations to the same mortality indexes. The mean RR values ranged from 0.95 to 1.14 for mortality due to all causes, 0.99 to 3.05 for lung cancer, 0.87 to 1.3 for respiratory diseases, 0.96 to 1.14 cardiovascular diseases and 0.97 to 1.05 for cardiopulmonary diseases mortality. Among the factors that may affect the RR estimations, only the size of studied population and the spatial scales used in exposure assessment showed notable influences. The female population was found to be more susceptible to long-term SO2 exposure. For other stratified subgroups including age, smoking status and income levels, no obvious relationship with RR was observed.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Ambient air pollution has long been recognized to be associated with various types of adverse effects to human health (WHO 2006). However, the degree of human health effects of each pollutant is still not very clear. Among the pollutants, fine particulate matter (PM2.5; ≤ 2.5 μm in aerodynamic diameter) has been the focus of health impact studies. The PM2.5 concentration is higher in many parts of the world, and their adverse effects were confirmed in several cohort studies (Pope et al. 2002, 2004, 2019; Laden et al. 2006; Krewski et al. 2009; Katanoda et al. 2011; Crouse et al. 2012; Lepeule et al. 2012; Cesaroni et al. 2013; Carey et al. 2013; Bentayeb et al. 2015; Crouse et al. 2015; Thurston et al. 2016). Nitrogen dioxide is also one of the dominant pollutants of interest in recent studies of human health and air quality (Carey et al. 2013; Hoek et al. 2013; Wang et al. 2016). For ozone, although the O3 is more related to short-term mortality (Bell et al. 2005), Jerret et al. (2009) examined the potential contribution of long-term ozone exposure to the risk of cardiopulmonary and respiratory deaths.
Compared to other pollutants, the impacts of sulphur dioxide (SO2) to human health have not been extensively studied, possibly because of its downward trends in emissions and uncertainty in its impact to human health (Lu et al. 2010; Klimont et al. 2013; EEA 2015; USEPA 2016). However, since the threshold concentration of SO2 for adverse health effects is not clear and those below the standard may still affect human health (Riordan and Adeeb 2004), potential health impacts of SO2 should not be neglected. WHO proposed a guideline of 500 μg/m3 for 10-min mean based on controlled studies with people with asthma where changes in pulmonary function and respiratory symptoms after exposure periods as short as 10 min were observed. The uncertainty linked with PM and SO2 in causality in epidemiological studies, the difficulty in reaching levels that are unlikely to have any impact and a prudent precautionary approach were the basis for update the guideline for 24-h mean from 125 to 20 μg/m3 (WHO 2006).
Several studies were conducted to evaluate the associations between long-term SO2 exposure and different causes of mortality (cardiovascular, respiratory and lung cancer, for example), and relative risks for different causes of mortality have been published. Yet, these studies were carried out in limited regions of the world. While relative risks are commonly used in risk assessment for impact estimations, non-portability of relative risks has been realized (Krewski et al. 2009). The values of relative risks vary across studies, and there is no simple clear standard to select relative risks for specific risk assessment studies (Pascal et al. 2016). Each set of population has different characteristics such as sensitivity to pollutants; therefore, it is ideal to use relative risks that were developed from the population of interest. However, due to lack of sufficient data and resources, most of risk assessment studies need to use previously published relative risks which may not be relevant. To avoid inappropriate selections, it is essential to understand the causes of heterogeneity among published relative risks.
In this study, we reviewed published epidemiological studies on health effects, specifically mortality, due to long-term exposure to SO2. The epidemiological studies are the base information for air quality guidelines construction. The articles deal with different RRs not directly linked to other variables such as climate, population and body mass index for example. We focused on SO2 since those for major pollutants such as particulate matter and nitrogen dioxide have been previously done (Hoek et al. 2013; Lipfert 2017; Vodonos et al. 2018), and its influence on health is still considerable uncertainty. The relative risks reported in identified published studies were summarized, and they were analysed for causes of heterogeneity across studies. Relative risks for stratified subgroups of population were also reviewed and evaluated to determine difference between subgroups in susceptibility to SO2 exposure.
Method
Online database searches were conducted by using Scopus and Web of Science with combinations of the following key words and their acronyms: sulphur/sulfur dioxide, relative risk, hazard ratio, air pollution, air quality, human health, burden of disease, mortality and cohort. Using different strings associated with different combinations of search terms resulted in 14 scientific articles from USA, Europe, China, Japan and Hong Kong.
The reference lists of identified peer-reviewed literature were browsed to supplement the database search. In this review, only studies reporting numerical results were included. The identified studies were thoroughly reviewed and analysed to find evidence of health effects due to long-term exposure to ambient SO2 and to determine the cause of heterogeneity of the results across studies.
In some of the identified studies, relative risks for each stratified subgroups of the population were provided. Relative risks for subgroups stratified by population’s age, gender, smoking status and income levels for respiratory mortality were reported by multiple studies. For other causes of mortality, the stratified studies were scarce. Hence, only relative risks of subgroups for respiratory mortality were analysed to determine susceptibility of different subgroups.
Table 1 shows the characteristics of the cohort studies found. The study of Abbey et al. (1999) was conducted in California (USA) as part of the Adventist Health Study of Smog (AHSMOG Study) (Abbey et al. 1991). HEI (2000) study is a reanalysis of Harvard Six Cities Study (Dockery et al. 1993) and American Cancer Society (ACS) Study (Pope et al. 1995) data. Beelen et al. (2008) study is based on Netherlands Cohort Study on Diet and Cancer (NLCS) (van den Brandt et al. 1990). Carey et al. (2013) is a national population-based cohort of adults registered with family practitioners in England. Elliott et al. (2007), otherwise, is a study encompassing a small area across electoral wards in Great Britain. Filleul et al. (2005) study was conducted in 24 areas of seven French towns using the PAARC survey (Pollution Atmosphérique et Affections Respiratoires Chroniques/Air pollution and chronic respiratory diseases) (PAARC 1982). Nafstad et al. (2004)’s study was a city-level cohort conducted in Oslo, Norway. The cohort of Chen et al. (2016) was conducted in four Northern Chinese cities: Tianjin, Shenyang, Taiyuan and Rizhao. Dong et al. (2012) and Zhang et al. (2011) are a population-based retrospective cohort conducted in Shenyang, northeast China. Katanoda et al. (2011) is a Japanese cohort conducted in eight areas of three prefectures (Miyagi, Aichi and Osaka). Lefler et al. (2019) used public National Health Interview Survey (NHIS) data, administered by the National Center for Health Statistics (NCHS), representing civilian non-institutionalized US population (Pope et al. 2019). Hedley et al. (2002) is a middle-term (monthly) study conducted in Hong Kong related to sulphur-rich fuels. We decided to keep this study in the review because of the direct evidence found related to control strategies and immediate and long-term health benefits.
Results and discussion
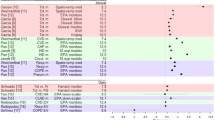
Fourteen published studies on relative risks (RR) for mortality due to long-term SO2 exposure were identified and reviewed. All the RR discussed in this section is related to an increment of 10 μg/m3 in SO2 concentration. The main mortality causes studied were all causes, cardiopulmonary, cardiovascular, respiratory diseases and lung cancer. Figure 1 illustrates the RR for these mortality causes, whose values vary across studies. All the studies except that of Dong et al. (2012) considered multiple causes of mortality in their analyses. Some of the studies showed no associations (lower 95% confidence interval being less than 1) or insignificant associations (mean values being less than 1.05) between mortality and long-term exposure to SO2.

Relative risks for five mortality causes: (a) All cause; (b) Cardiopulmonary disease; (c) Cardiovascular disease; (d) Respiratory disease; and (e) Lung cancer. Notes: References (x-axis): (1) Abbey et al. (1999)—for male; (2) Abbey et al. (1999)—for female; (3) Beelen et al. (2008); (4) Cao et al. (2011); (5) Carey et al. (2013); (6) Chen et al. (2016); (7) Dong et al. (2012); (8) Elliott et al. (2007); (9) Filleul et al. (2005); (10) Hedley et al. (2002); (11) Katanoda et al. (2011); (12) HEI (2000); (13) Nafstad et al. (2004); (14) Zhang et al. (2011); (15) Lefler et al. (2019)
For all-cause mortality, the mean RR values ranged between 0.95 and 1.14. Among the 11 studies that studied all-cause mortality, six showed no association with ambient SO2 concentration. Carey et al. (2013) reported significant association (mean RR equal to 1.14) while the other studies showed very weak and generally insignificant associations (mean RR ≤ 1.04).
For lung cancer mortality, the mean RR values range from 0.99 to 3.05. Seven out of 11 studies that included lung cancer mortality in their studies showed no association between lung cancer mortality and long-term ambient SO2 exposure. Three studies found moderate associations (mean RR between 1.04 and 1.09). The relative risks reported by Abbey et al. (1999) were considerably higher than other studies (mean RR equal to 2.00 for male and 3.05 for female).
Nine studies included respiratory mortality, and six studies included cardiovascular mortality as health outcomes in their analyses. The mean RR values vary between 0.87 and 1.36 for respiratory disease, with five studies showing no association with long-term ambient SO2 exposure. Three studies reported a little significance (mean RR ≤ 1.05) while two studies showed highly significant associations (mean RR ≥ 1.14). For cardiovascular mortality, the mean RR values vary between 0.96 and 1.14. Two of the studies found no association, three found insignificant associations (mean RR between 1.01 and 1.03), and one showed a significant association (mean RR equal to 1.14) between cardiovascular mortality and exposure to ambient SO2.
Six studies included mortality due to cardiopulmonary. Lefler et al. (2019) was the only one presenting strong association with ambient SO2 concentrations (mean RR equal to 1.16, recalculated to 10 μg/m3 in SO2 increase). Among the studies, the mean RR values range between 0.97 and 1.16. Although a few studies also considered mortality due to cerebrovascular disease, ischemic heart disease and/or all-other-cause (all causes except cardiovascular and respiratory disease), these are excluded from further analysis in this review because of the number of studies available and the insignificance of the reported RR.
Considering each study, RR for mortality related to respiratory system tend to be higher than those of other causes, with the exceptions of Filleul et al. (2005) and the Harvard Six City study (HEI 2000), where the RRs of all-cause mortality were higher.
Potential cause of heterogeneity in RR values across studies
To investigate the causes of the diversity, the studies were analysed according to the region of study, population size and age, exposure assessment method, time of study conducted, health outcome classifications and covariates used for adjustment of statistical model.
Study regions
The geographical variety of the identified studies is somewhat limited, with studies from USA, Europe (England, France, Netherlands and Norway) and Asia (China, Hong Kong and Japan). Three of the studies that found no association between SO2 and any type of mortality considered in their analyses were from Europe and one was from China.
All four European studies showed no obvious association between ambient SO2 and lung cancer while some studies from Asia and USA reported moderate to strong associations. As shown in Table 1, the average SO2 concentration was much higher in the studies conducted in China. No study from Asia included cardiopulmonary mortality, and no US study included cardiovascular mortality.
Spatial scale
Several studies used residential address while others used postal codes, cities and districts as the spatial scale for exposure assessment. For all the causes besides lung cancer, lager spatial scales resulted in higher RR, with the exception of studies from Dong et al. (2012) and Zhang et al. (2011). Use of smaller spatial scale should improve the accuracy of exposure assessment which helps to produce more reliable results in general.
Population size
The population size in the cohort studies ranged from less than 40,000 to over 800,000. Elliott et al. (2007) and Hedley et al. (2002) did not follow a particular group of population. Instead, they have included all the residents in a region of interest who fall into certain age brackets by using census data. The advantage of this approach is that it facilitates to study a large population; however, it lacks personal details of the studied population such as smoking habits, what can be a major disadvantage.
Except for lung cancer, the studies with larger population size tend to show significant associations between long-term SO2 exposure and mortality, since the statistical analysis would generally be more reliable when sample sizes become larger. In case of lung cancer, although none of the European studies showed the association with SO2 concentration, the mean relative risk values were larger for studies with larger population size except for Elliott et al. (2007). However, this tendency cannot be seen among studies in Asia and USA. The number of lung cancer mortality cases in one of the US studies (Abbey et al. 1999) was only 18 and 12 for male and female, respectively. These are extremely small numbers compared to the number of cases in other studies which ranged between 140 (Chen et al. 2016) and over 28,000 (Elliott et al. 2007). Due to this small number of cases of Abbey et al. (1999), their results may not be as reliable.
Age of population
In this review, only the RRs for adult population were considered. An exception to this was the work of Hedley et al. (2002) where population older than 15 years old was included. The selection of the age bracket for the studied population may influence the result of RR since susceptibility to diseases may depend on the age of population. Since few studies disclosed the average age or the age distribution of the population, it is not feasible to clearly see the influence of this parameter on the RR reported. Studies with narrower age range (Beelen et al. 2008; Filleul et al. 2005; Nafstad et al. 2004) showed no association with SO2 exposure and mortality of any cause included in their studies, which may be associated with not including the elderly age group in the analysis. The elderly is considered to be one of the most affected age group by air pollution, as reported by Carey et al. (2013), who found older group (≥ 65 years old) to be more susceptible to long-term SO2 exposure.
Gender
Four studies considered subgroups depending on gender, and all showed stronger effects to female population (Abbey et al. 1999; Carey et al. 2013; Dong et al. 2012; Katanoda et al. 2011). The difference between male and female was significant in all studies except for Dong et al. (2012). One thing to note is that the values of relative risks for both male and female vary across the studies. For instance, Carey et al. (2013) reported the mean relative risk to be 1.54 for female while that of Abbey et al. (1999) was 0.98.
Intensified health effects have been observed in male population for other health outcomes or other pollutants such as particulate matter and ozone, which was attributed to differences in exposures to other pollutants, such as tobacco smoke and occupational sources (involving airborne contaminants), time spent outdoors, and size of population sample (Abbey et al. 1999; Beeson et al. 1998; Katanoda et al. 2011). For SO2, the possible explanation for female population resulting in higher mortality RR for respiratory mortality is the differences in size, development and reactivity of airways between male and female (Becklake and Kauffmann 1999; Yunginger et al. 1992; Dong et al. 2012), when a dose-response relationship could be more easily detected in women (Dong et al. 2012), and body mass index for women is rather smaller (Di Angelantonio et al. 2016).
Exposed concentration estimation
The work of Elliott et al. (2007) indicated that the excess risks become higher when shorter length of exposure period was used. Use of annual average of certain years in exposure assessment was an approach often used in the studies reviewed. Alternatively, some studies used average concentrations over surviving years of each participant (Zhang et al. 2011). This approach also may produce highly biased results. When the concentration is in steep down trend, for example, survivors through entire follow-up period may be assigned much lower concentrations compared to those who died during the study (Chen et al. 2016). Chen et al. (2016) using different estimation methods for exposed concentrations found significant difference in resulted RR: (a) time-varying method, (b) fixed 1-year average and (c) average of entire surviving years of participants. The mean RR values for all-cause mortality estimated with these three methods ranged between 0.971 and 1.028, and those for lung cancer mortality ranged between 1.018 and 1.224.
Elliott et al. (2007) examined the influence of exposure period selection in their RR calculations by using multiple different time windows of exposure. They found greater mortality risks when most proximal windows of exposure were used except for the case of lung cancer mortality. While Hansell et al. (2016) also stated that risks of mortality were generally higher in years immediately following the exposure, Lee et al. (2002) and Krewski et al. (2009) did not find significant difference among the exposure windows they considered. Krewski et al. (2009) stated that the reason for this insignificance might be the high correlations between exposure levels of the time windows they used.
Levels of ambient SO2 concentration
The influence of the average ambient SO2 concentration to the resulting RR is not clear for any of the causes of mortality. The SO2 average concentration varied from 3.9 μg/m3 (RR equal to 1.36 for respiratory diseases) (Carey et al. 2013) to 73 μg/m3 (RR equal to 1.03 for respiratory diseases) (Cao et al. 2011). Consequently, the heterogeneity found in RR may be associated to differently ambient SO2 concentrations.
The ambient SO2 concentrations in many parts of the world have decreased drastically in the last decades; therefore, the rate of change may also need to be considered. However, the detailed SO2 concentration trends were not provided in most of the studies. Nonetheless, even when studies in the similar region where the reduction rate of SO2 are comparable were considered separately, no clear indication of influence of ambient concentration levels can be observed. Moreover, the selection of the period that is to be used for an estimation of exposed concentration may influence the relative risk calculations.
Another concern is that most the studies only considered outdoor concentrations of SO2. The quality of air and time spent at participants’ residence, work, commuting and travelling should be considered. For indoor air quality, consideration of use of air conditioner and rate of ventilation may also be important as these vary significantly between regions and individuals.
Period of data collection
The period when studies were conducted considerably differ among studies. For instance, Abbey et al. (1999) started their follow up in 1966 and continued until 1992 while the study of Lefler et al. (2019) was carried out between 1987 and 2014. As the methods used for exposure assessment such as measurement of concentration and pollutant dispersion modelling advance with time, the precision of the results likely improved with time. Moreover, the activities of population may have changed over time which influences the time spent outdoors. Indoor air quality might have improved as the efficiency of ventilation and the prevalence of air conditioner have increased. These factors affect the degree of exposure to pollutants. However, no trend in relative risk values with the time of study was observed among the studies. Duration of the follow up period also did not seem to influence the resulting relative risk values.
Covariates for adjustment
With the exception of Elliott et al. (2007) and Hedley et al. (2002), Cox proportional hazard regression models were used to estimate RR by using some adjustments. Covariates considered for the adjustments are shown in Table 2. All the studies which contained both genders in their study population adjusted for gender. Smoking status was used for adjustment in all the studies. Most of the studies also adjusted for age and educational level. Lesser number of studies adjusted for body mass index, occupational exposure and activity level. Alcohol consumption, diet, socioeconomic status and passive smoking were also considered in a few studies.
Some of the covariates often used for adjustments such as smoking status are certainly associated with mortality; however, their influence to the estimation of relative risks of air pollutant exposure is not very clear (Dockery et al. 1993). Some of the studies calculated RR with different sets of covariates for adjustment. Carey et al. (2013) provided RR for different mortality causes by varying the selection of covariates. For all the causes, additional covariates in adjustment reduced the RR values. For example, the RR for all-cause mortality decreased from 1.07 to 1.03 per 2.2 μg/m3 of ambient SO2 concentration, when smoking status, body mass index and education level were added to the basic model where only age and gender were included as covariates. Similar degree of reduction can be observed for other causes of mortality. On the other hand, the study of Cao et al. (2011) showed increased RR values for respiratory and lung cancer mortality when additional covariates were included. Katanoda et al. (2011) calculated the RR for lung cancer mortality with three different adjustments. Firstly, the estimation was done adjusting only with age and gender. The second model was adjusted for age, gender, smoking status, number of cigarettes smoked, smoking status of family members, fruit and vegetable (yellow and green) consumption and indoor air emission. The third model contained smoking status of parents in childhood, vegetable (non-yellow and green) consumption, occupation and type of health insurance as a socioeconomic indicator in addition to the second model. The RR decreased with the additional covariates for adjustment. On the other hand, two different sets of covariates were used for respiratory mortality and the relative risks increased with additional covariates.
The importance of consideration of level of education and socio-economic status as covariates has been raised as these may be a measure of some unmeasurable confounders including diet and nutrition (Atkinson et al. 2013; Hoek et al. 2013). Although limited number of studies stratified the population according to the levels of body mass index for RR estimations, population with higher body mass index was consistently shown to be more vulnerable (Cao et al. 2011; Dong et al. 2012; Zhang et al. 2011).
Climate-related factors such as temperature and humidity are not commonly considered, although some studies mention about an association between climate and mortality (Choi et al. 1997; Jerrett et al. 2004). The climate also affects the behaviour of population. The time spent outdoor likely to depend on the climate of the region, which influence the degree of exposure to air pollutants and hence the relative risk estimations.
Regarding the smoking status, three studies provided the results for different subgroups. Dong et al. (2012) found higher association with current smokers while Carey et al. (2013) and Katanoda et al. (2011) showed the highest association for never smokers. In the study of Carey et al. (2013), past smokers are more susceptible than current smokers; however, Katanoda et al. (2011) showed current smokers are more susceptible.
Two studies considered subgroups depending on the income levels. In the study of Carey et al. (2013), relative risk for subgroup with higher income level was found to be much higher than those with lower income. Dong et al. (2012) divided the population into four groups according to their income levels; however, no statistically significant differences between mortality and income was found, besides middle groups obtained higher hazard ratios compared to the groups with lowest and highest income.
Other pollutants were also considered as covariates. In the study of Carey et al. (2013), SO2 was moderately positively correlated to PM10 (r = 0.45), PM2.5 (r = 0.46) and NO2 (r = 0.37) and negatively correlated to O3 (r = − 0.39). On the other hand, SO2 coefficient remained stable in two-pollutant models with PM10 and O3 in the study of Abbey et al. (1999) for lung cancer mortality because of the low SO2 correlations with other pollutants. The effect of multiple pollutant models conducted by Cao et al. (2011) also showed no percent increase for total, cardiovascular, respiratory and lung cancer mortality when the model was adjusted for TSP and NOx. In the study of Beelen et al. (2008), the correlations between different air pollutants were greater than 0.8, except for SO2 (r > 0.6). Negative correlation to NO (r = − 0.01) and NO2 (r = − 0.10) was also found by Filleul et al. (2005). When considering other pollutants (PM2.5, O3, CO, NO2) as covariates, the RR calculated by Lefler et al. (2019) decreased for both all-cause and cardiopulmonary mortality, from 1.023 to 1.017 and from 1.050 to 1.027, respectively. Considering the interactivity between SO2 and particle matter, especially in secondary particles formation (Albuquerque et al. 2019), it seems reasonable considering at least PM as covariate in future SO2 analysis.
Conclusion
Some of the studies reviewed in this work found strong associations between mortality and long-term ambient SO2 exposure while others found insignificant or no associations. It seems that exposure to SO2 has stronger association with respiratory system-related mortality than other causes of mortality such as cardiovascular diseases. The number of published studies as well as the geographic regions where studies have been conducted is still limited. Hence, a definite and quantitative conclusion about the relationship between long-term SO2 exposure in the inspired air and mortality rate cannot be drawn by now.
The heterogeneity across the studies is likely to be caused by several different factors, starting with SO2 concentration, which widely varied across the studies. As its influence is still considerable uncertainty, it is assumed that reduction in exposure is achieved by reducing SO2 concentrations. Another factor to consider is the outcome. The relative risk for lung cancer mortality did not follow the trend of other mortality. This may be because lung cancer takes longer to develop compared to other causes of mortality including cardiovascular and respiratory diseases. This suggests that risks of lung cancer may need to be studied separately using longer interval time between exposure and health outcomes.
Any of the factors investigated in this work did not seem to have notable influence on relative risk estimates except for the studied population size and spatial scale used for exposure assessment. The studies in larger population size tend to show higher values of RR except for lung cancer mortality. As individuals may react to pollutants differently, studies with larger number of subjects with diverse levels of susceptibility would be more reliable for RR representing the general population. The precision of exposure assessment is a crucial factor in risk estimation. Overall, use of smaller spatial scale would provide more accurate exposure estimates which enhance the accuracy of resulting relative risks. The result of this review indicated the estimated relative risks were lower when smaller spatial scales were used except for lung cancer mortality. This indication is contradictory to the tendency found with population size. The reason may be the difference in other component of exposure assessment.
Susceptibility of subgroups could be examined only for respiratory mortality and to a limited extent. Except for the gender, results were contradictory between studies. The number of studies is still small to determine more vulnerable populations at this point.
To understand how long-term exposure to ambient SO2 concentration associates with human mortality more clearly, further studies need to be conducted. In a mean time, for studies where relative risks are used, including risk analysis studies, performing uncertainty analysis is recommended to realize the range of possible outcomes.
References
Abbey DE, Mills PK, Petersen FF, Beeson WL (1991) Long-term ambient concentrations of total suspended particulates and oxidants as related to incidence of chronic disease in California Seventh-day Adventists. Environ Health Perspect 94:43–50. https://doi.org/10.1289/ehp.94-1567944
Abbey DE, Nishino N, McDonnell WF, Burchette RJ, Knutsen SF, Beeson WL, Yang JX (1999) Long-term inhalable particles and other air pollutants related to mortality in nonsmokers. Am J Resp Crit Care 159:373–382. https://doi.org/10.1164/ajrccm.159.2.9806020
Albuquerque TTA, West J, Andrade MF, Ynoue RY, Andreão WL, Santos FS, Maciel FM, Pedruzzi R, Mateus VO, Martins JA, Martins LD, Nascimento EGS, Moreira DM (2019) Analysis of PM2.5 concentrations under pollutant emission control strategies in the metropolitan area of São Paulo, Brazil. Environ Sci Pollut Res. https://doi.org/10.1007/s11356-019-06447-6
Atkinson RW, Carey IM, Kent AJ, Van Staa TP, Ross Anderson H, Cook DG (2013) Long-term exposure to outdoor air pollution and incidence of cardiovascular diseases. Epidemiology 2013:44–53. https://doi.org/10.1097/EDE.0b013e318276ccb8
Becklake MR, Kauffmann F (1999) Gender differences in airway behaviour over the human life span. Thorax 54:1119–1138. https://doi.org/10.1136/thx.54.12.1119
Beelen R, Hoek G, van den Brandt PA, Goldbohm RA, Fischer P, Schouten LJ, Jerrett M, Hughes E, Armstrong B, Brunekreefet B (2008) Long-term effects of traffic-related air pollution on mortality in a Dutch cohort (NLCS-AIR Study). Environ Health Perspect 116:196–202. https://doi.org/10.1289/ehp.10767
Beeson WL, Abbey DE, Knutsen SF (1998) Long-term concentrations of ambient air pollutants and incident lung cancer in California adults: results from the AHSMOG study. Environ Health Perspect 106:813–822
Bell ML, Dominici F, Samet JM (2005) A meta-analysis of time-series studies of ozone and mortality with comparison to the national morbidity, mortality, and air pollution study. Epidemiology 16:436–445
Bentayeb M, Wagner V, Stempfelet M, Zins M, Goldberg M, Pascal M, Larrieu S, Beaudeau P, Cassadou S, Eilstein D, Filleul L, Le Tertre A, Medina S, Pascal S, Prouvost H, Quénel P, Zeghnoun A, Lefranc A (2015) Association between long-term exposure to air pollution and mortality in France: a 25-year follow-up study. Environ Int 85:5–14. https://doi.org/10.1016/j.envint.2015.08.006
Cao J, Yang C, Li J, Chen R, Chen B, Gu D, Kan H (2011) Association between long-term exposure to outdoor air pollution and mortality in China: a cohort study. J Hazard Mater 186:1594–1600. https://doi.org/10.1016/j.jhazmat.2010.12.036
Carey IM, Atkinson RW, Kent AJ, Van Staa T, Cook DG, Anderson HR (2013) Mortality associations with long-term exposure to outdoor air pollution in a national English cohort. Am J Resp Crit Care 187:1226–1233. https://doi.org/10.1164/rccm.201210-1758OC
Cesaroni G, Badaloni C, Gariazzo C, Stafoggia M, Sozzi R, Davoli M, Forastiere F (2013) Long-term exposure to urban air pollution and mortality in a cohort of more than a million adults in Rome. Environ Health Perspect 121:324–331. https://doi.org/10.1289/ehp.1205862
Chen X, Zhang LW, Huang JJ, Song FJ, Zhang LP, Qian ZM, Trevathan E, Mao HJ, Han B, Vaughn M, Chen KX, Liu YM, Chen J, Zhao BX, Jiang GH, Gu Q, Bai ZP, Dong GH, Tang NJ (2016) Long-term exposure to urban air pollution and lung cancer mortality: a 12-year cohort study in northern China. Sci Total Environ 571:855–861. https://doi.org/10.1016/j.scitotenv.2016.07.064
Choi KS, Inoue S, Shinozaki R (1997) Air pollution, temperature, and regional differences in lung cancer mortality in Japan. Arch Environ Health 52:160–168. https://doi.org/10.1080/00039899709602881
Crouse DL, Peters PA, Van Donkelaar A, Goldberg MS, Villeneuve PJ, Brion O, Khan S, Atari DO, Jerrett M, Pope CA III, Brauer M, Brook JR, Martin RV, Stieb D, Burnett RT (2012) Risk of nonaccidental and cardiovascular mortality in relation to long-term exposure to low concentrations of fine particulate matter: a Canadian national-level cohort study. Environ Health Perspect 120:708–714. https://doi.org/10.1289/ehp.1104049
Crouse DL, Peters PA, Hystad P, Brook JR, van Donkelaar A, Martin RV, Villeneuve PJ, Jerrett M, Goldberg MS, Pope CA III, Brauer M, Brook RD, Robichaud A, Menard R, Burnett RT (2015) Ambient PM2.5, O3, and NO2 exposures and associations with mortality over 16 years of follow-up in the Canadian Census Health and Environment Cohort (CanCHEC). Environ Health Perspect 123:1180–1186. https://doi.org/10.1289/ehp.1409276
Di Angelantonio E, Bhupathiraju SN, Wormser D, Gao P, Kaptoge S, Gonzales AB, Cairns BJ, Huxley R, Jackson CL, Joshy G, Lewington S, Manson JE, Murphy N, Patel AV, Samet JM, Woodward M, Zheng W, Zhou M, Bansal N, Barricarte A, Carter B, Cerhan JR, Collins R, Smith GD, Fang X, Franco OH, Green J, Halsey J, Hildebrand JS, Jung KL, Korda RJ, McLerran DF, Moore SC, O’Keeffe LM, Paige E, Ramond A, Reeves GK, Rolland B, Sarcedote C, Sattar N, Sofianopoulou E, Stevens J, Thun M, Ueshima H, Yang L, Yun YD, Willeit P, Banks E, Beral V, Chen Z, Gapstur SM, Gunter MJ, Hartge P, Jee SH, Lam T-H, Peto R, Potter JD, Willett WC, Thompson SG, Danesh J, Hu FB (2016) Body-mass index and all-cause mortality: individual-participant-data meta-analysis of 239 prospective studies in four continents. Lancet 288:776–786. https://doi.org/10.1016/S0140-6736(16)30175-1
Dockery DW, Pope CA III, Xu X, Spengler JD, Ware JH, Fay ME, Ferris BG Jr, Speizer FE (1993) An association between air pollution and mortality in six U.S. cities. New Engl J Med 329:1753–1759. https://doi.org/10.1056/nejm199312093292401
Dong GH, Zhang P, Sun B, Zhang L, Chen X, Ma N, Yu F, Guo H, Huang H, Lee YL, Tang N, Chen J (2012) Long-term exposure to ambient air pollution and respiratory disease mortality in Shenyang, China: a 12-year population-based retrospective cohort study. Respiration 84:360–368. https://doi.org/10.1159/000332930
EEA (2015) Sulphur dioxide (SO2) emissions. European Environment Agency. http://www.eea.europa.eu/data-and-maps/indicators/eea-32-sulphur-dioxide-so2-emissions-1/assessment-1. Accessed April 7th, 2018
Elliott P, Shaddick G, Wakefield JC, De Hoogh C, Briggs DJ (2007) Long-term associations of outdoor air pollution with mortality in Great Britain. Thorax 62:1088–1094. https://doi.org/10.1136/thx.2006.076851
Filleul L, Rondeau V, Vandentorren S, Le Moual N, Cantagrel A, Annesi-Maesano I, Charpin D, Declercq C, Neukirch F, Paris C, Vervloet D, Brochard P, Tessier JF, Kauffmann F, Baldi I (2005) Twenty five year mortality and air pollution: results from the French PAARC survey. Occup Environ Med 62:453–460. https://doi.org/10.1136/oem.2004.014746
Hansell A, Ghosh RE, Blangiardo M, Perkins C, Vienneau D, Goffe K, Briggs D, Gulliver J (2016) Historic air pollution exposure and long-term mortality risks in England and Wales: prospective longitudinal cohort study. Thorax 71:330–338. https://doi.org/10.1136/thoraxjnl-2015-207111
Hedley AJ, Wong CM, Thach TQ, Ma S, Lam TH, Anderson HR (2002) Cardiorespiratory and all-cause mortality after restrictions on sulphur content of fuel in Hong Kong: an intervention study. Lancet 360:1646–1652. https://doi.org/10.1016/S0140-6736(02)11612-6
HEI (2000) Reanalysis of the Harvard Six Cities study and the American Cancer Society study of particulate air pollution and mortality: a special report of the Institute’s particle epidemiology reanalysis project. Health Effects Institute, Cambridge
Hoek G, Krishnan RM, Beelen R, Peters A, Ostro B, Brunekreef B, Kaufman JD (2013) Long-term air pollution exposure and cardio-respiratory mortality: a review environmental health. Environ Health 12:43. https://doi.org/10.1186/1476-069X-12-43
Jerret M, Burnett RT, Pope CA III, Ito K, Thurston G, Krewski D, Shi Y, Calle E, Thun M (2009) Long-term ozone exposure and mortality. New Engl J Med 360:1085–1095. https://doi.org/10.1056/NEJMoa0803894
Jerrett M, Burnett RT, Brook J, Kanaroglou P, Giovis C, Finkelstein N, Hutchison B (2004) Do socioeconomic characteristics modify the short term association between air pollution and mortality? Evidence from a zonal time series in Hamilton, Canada. J Epidemiol Community Health 58:31–40. https://doi.org/10.1136/jech.58.1.31
Katanoda K, Sobue T, Satoh H, Tajima K, Suzuki T, Nakatsuka H, Takezak T, Nakayama T, Nitta H, Tanabe K, Tominaga S (2011) An association between long-term exposure to ambient air pollution and mortality from lung cancer and respiratory diseases in Japan. J Epidemiol 21:132–143. https://doi.org/10.2188/jea.JE20100098
Klimont Z, Smith SJ, Cofala J (2013) The last decade of global anthropogenic sulfur dioxide: 2000-2011 emissions. Environ Res Lett 8. https://doi.org/10.1088/1748-9326/8/1/014003
Krewski D, Jerrett M, Burnett RT, Ma R, Hughes E, Shi Y, Turner MC, Pope CA III, Thurston G, Calle EE, Thun MJ, Beckerman B, DeLuca P, Finkelstein N, Ito K, Moore DK, Newbold KB, Ramsay T, Ross Z, Shin H, Tempalski B (2009) Extended follow-up and spatial analysis of the American Cancer Society study linking particulate air pollution and mortality. Res Rep Health Eff Inst 140:5–114
Laden F, Schwartz J, Speizer FE, Dockery DW (2006) Reduction in fine particulate air pollution and mortality: extended follow-up of the Harvard six cities study. Am J Resp Crit Care 173:667–672. https://doi.org/10.1164/rccm.200503-443OC
Lee WJ, Teschke K, Kauppinen T, Andersen A, Jäppinen P, Szadkowska-Stanczyk I, Pearce N, Persson B, Bergeret A, Facchini LA, Kishi R, Kielkowski D, Rix BA, Henneberger P, Sunyer J, Colin D, Kogevinas M, Boffetta P (2002) Mortality from lung cancer in workers exposed to sulfur dioxide in the pulp and paper industry. Environ Health Perspect 110:991–995
Lefler JS, Higbee JD, Burnett RT, Ezzati M, Coleman NC, Mann DD, Marshall JD, Bechle M, Wang Y, Robinson AL, Pope CA III (2019) Air pollution and mortality in a large, representative U.S. cohort: multiple pollutant-analyses, and spatial and temporal decompositions. Environ Health 18:101. https://doi.org/10.1186/s12940-019-0544-9
Lepeule J, Laden F, Dockery D, Schwartz J (2012) Chronic exposure to fine particles and mortality: an extended follow-up of the Harvard Six Cities study from 1974 to 2009. Environ Health Perspect 120:965–970. https://doi.org/10.1289/ehp.1104660
Lipfert FW (2017) A critical review of the ESCAPE project for estimating long-term health effects of air pollution. Environ Int 99:87–96. https://doi.org/10.1016/j.envint.2016.11.028
Lu Z, Streets DG, Zhang Q, Wang S, Carmichael GR, Cheng YF, Wei C, Chin M, Diehl T, Tan Q (2010) Sulfur dioxide emissions in China and sulfur trends in East Asia since 2000. Atmos Chem Phys 10:6311–6331. https://doi.org/10.5194/acp-10-6311-2010
Nafstad P, Håheim LL, Wisløff T, Gram F, Oftedal B, Holme I, Hjermann I, Leren P (2004) Urban air pollution and mortality in a cohort of Norwegian men. Environ Health Perspect 112:610–615. https://doi.org/10.1289/ehp.6684
PAARC, Groupe coopératif (1982) Pollution atmosphérique et affections respiratoires chroniques ou à répétition. Méthodes et matériel. Bull Europ Physiopath Resp 18:87–99
Pascal M, de Crouy CP, Wagner V, Corso M, Tillier C, Bentayeb M, Blanchard M, Cochet A, Pascal L, Host S, Goria S, Le Tertre A, Chatignoux E, Ung A, Beaudeau P, Medina S (2016) The mortality impacts of fine particles in France. Sci Total Environ 571:416–425. https://doi.org/10.1016/j.scitotenv.2016.06.213
Pope CA III, Thun MJ, Namboodiri MM, Dockery DW, Evans JS, Speizer FE, Heath CW Jr (1995) Particulate air pollution as a predictor of mortality in a prospective study of U.S. adults. Am J Respir Crit Care Med 151:669–674. https://doi.org/10.1164/ajrccm/151.3_Pt_1.669
Pope CA III, Burnett RT, Thun MJ, Calle EE, Krewski D, Ito K, Thurston GD (2002) Lung cancer, cardiopulmonary mortality, and long-term exposure to fine particulate air pollution. J Am Med Assoc 287:1132–1141. https://doi.org/10.1001/jama.287.9.1132
Pope CA III, Burnett RT, Thurston GD, Thun MJ, Calle EE, Krewski D, Godleski JJ (2004) Cardiovascular mortality and long-term exposure to particulate air pollution: epidemiological evidence of general pathophysiological pathways of disease. Circulation 109:71–77. https://doi.org/10.1161/01.CIR.0000108927.80044.7F
Pope CA III, Lefler JS, Ezzati M, Higbee JD, Marshall JD, Kim S-Y, Bechle M, Gilliat KS, Vernon SE, Robinson AL, Burnett RT (2019) Mortality risk and fine particulate air pollution in a large, representative cohort of U.S. adults. Environ Health Perspect 127:077007-1–077007-9. https://doi.org/10.1289/EHP4438
Riordan D, Adeeb F (2004) Air quality monitoring for sulphur dioxide in metropolitan Adelaide. Environment Protection Authority South Australia, Adelaide
Thurston GD, Burnett RT, Turner MC, Shi Y, Krewski D, Lall R, Ito K, Jerrett M, Gapstur SM, Diver WR, Pope CA III (2016) Ischemic heart disease mortality and long-term exposure to source-related components of U.S. fine particle air pollution. Environ Health Perspect 124:785–794. https://doi.org/10.1289/ehp.1509777
USEPA, 2016. Sulfur dioxide trends. U.S. Environmental Protection Agency. https://www.epa.gov/air-trends/sulfur-dioxide-trends. Accessed April 7th, 2018
van den Brandt PA, Goldbohm RA, van‘t Veer P, Volovics A, Hermus RJ, Sturmans F (1990) A large-scale prospective cohort study on diet and cancer in the Netherlands. J Clin Epidemiol 43:285–295. https://doi.org/10.1016/0895-4356(90)90009-e
Vodonos A, Awad YA, Schwartz J (2018) The concentration-response between long-term PM2.5 exposure and mortality; a meta-regression approach. Environ Res 166:677–689. https://doi.org/10.1016/j.envres.2018.06.021
Wang L, Zhong B, Vardoulakis S, Zhang F, Pilot E, Li Y, Yang L, Wang W, Krafft T (2016) Air quality strategies on public health and health equity in Europe - a systematic review. Int J Environ Res Public Health 13. https://doi.org/10.3390/ijerph13121196
WHO (2006) Air quality guidelines: global update 2005. World Health Organization, Copenhagen
Yunginger JW, Reed CE, O'Connell EJ, Melton LJ III, O'Fallon WM, Silverstein MD (1992) A community-based study of the epidemiology of asthma: incidence rates, 1964-1983. Am Rev Respir Dis 146:888–894. https://doi.org/10.1164/ajrccm/146.4.888
Zhang P, Dong G, Sun B, Zhang L, Chen X, Ma N, Yu F, Guo H, Huang H, Lee YL, Tang N, Chen J (2011) Long-term exposure to ambient air pollution and mortality due to cardiovascular disease and cerebrovascular disease in Shenyang, China. PLoS One 6. https://doi.org/10.1371/journal.pone.0020827
Funding
This research was partially funded by Fundação de Amparo à Pesquisa do Espírito Santo (FAPES), Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) and Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), Brazil.
Author information
Authors and Affiliations
Corresponding author
Additional information
Responsible editor: Philippe Garrigues
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Kobayashi, Y., Santos, J.M., Mill, J.G. et al. Mortality risks due to long-term ambient sulphur dioxide exposure: large variability of relative risk in the literature. Environ Sci Pollut Res 27, 35908–35917 (2020). https://doi.org/10.1007/s11356-020-07867-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-020-07867-5