
Abstract
Although the growths of ambient pollutants have been attracting public concern, the characteristic of the associations between air pollutants and mortality remains elusive. Time series analysis with a generalized additive model was performed to estimate the associations between ambient air pollutants and mortality outcomes in Shenzhen City for the period of 2012–2014. The results showed that nitrogen dioxide (NO2)-induced excess risks (ER) of total non-accidental mortality and cardiovascular mortality were significantly increased (6.05% (95% CI 3.38%, 8.78%); 6.88% (95% CI 2.98%, 10.93%), respectively) in interquartile range (IQR) increase analysis. Also, these associations were strengthened after adjusting for other pollutants. Moreover, similar associations were estimated for sulfur dioxide (SO2), particulate matter with an aerodynamic diameter of <10 μm (PM10), and total non-accidental mortality. There were significant higher ERs of associations between PM10 and mortality for men than women; while there were significant higher ERs of associations between PM10/NO2 and mortality for elders (65 or elder) than youngers (64 or younger). Season analyses showed that associations between NO2 and total non-accidental mortality were more pronounced in hot seasons than in warm seasons. Taken together, NO2 was positively associated with total non-accidental mortality and cardiovascular mortality in Shenzhen even when the concentrations were below the ambient air quality standard. Policy measures should aim at reducing residents’ exposure to anthropogenic NO2 emissions.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Recently, wide-range, recurrent, and continuous haze has disturbed the daily life of Chinese residents and threated to their health.
The associations of morbidity and mortality of many diseases with air pollutants have been extensively noted and recognized by numerous researchers in different countries and regions. For example, the stroke morbidity may be associated with the lag effect of particulate matter (PM) exposure (Scheers et al. 2015). Samoli et al. reported the adverse effects of ambient PM on mortality in Europe and North America (Samoli et al. 2008). In addition, associations of PM10, SO2, and NO2 with coronary heart disease mortality in eight Chinese cities were found (Li et al. 2015). Furthermore, some other studies indicate the associations between childhood emergency department (ED) visits/hospitalizations and ozone (O3)/PM2.5 (Gleason & Fagliano 2015, Silverman & Ito 2010).
However, most of the studies on the effects of air pollutants on morbidity and mortality of relative diseases were performed in Canada, USA, and Europe (Chen et al. 2014, Ferrari et al. 2015, Rodopoulou et al. 2015). Their findings might not be suitable for China, especially Shenzhen, since Shenzhen has unique region, local meteorology, demography, and pollutants.
Shenzhen locates at the southeast of China and next to Hong Kong. Shenzhen has subtropical monsoon climate. The method which delimits four seasons is not suitable for the characteristics of the long summer of Shenzhen. Thus, the seasonal division rule of warm and hot climate is more appropriate to indicate the climate situation of Shenzhen (Dai et al. 2015, Liu et al. 2014). The population and economy grew rapidly since Shenzhen Special Economic Zone was established. As a vibrant city, the median age of Shenzhen is 30.73 in the period of 2012–2014 (Shenzhen Statistics Bureau 2015).
Automobile exhaust contributes major ambient air pollution in Shenzhen. The chemical components of automobile are complicated, and some of them may have synergistic effects. The rapid economic growth in Shenzhen boosted the car ownership (Xie et al. 2016). From 2012 to 2014, the growth rates of motor vehicles are 15, 16.5, and 17.44%, respectively. By the end of 2014, vehicle population is more than 3.19 million (Shenzhen Traffic Management Bureau 2015). The increase in number of motor vehicles exacerbates ambient air pollution (Chen et al. 2004).
Generally, Shenzhen is not an industrial city, and its air quality is better compared to those of many other cities of China. Shenzhen residents are younger; therefore, they may have better health and less susceptibility to pollutants. However, Shenzhen’s annual non-accidental morality raised continually, and the growth is 14.83% during 2012–2014. We hypothesize that the pollutant levels positively correlate to the mortalities in Shenzhen even when the pollution is mild, and that different chemical pollutants have diverse association to the mortalities.
To validate the hypothesis, we studied the relationship between air pollutant exposure and characteristics of mortality in Shenzhen. To obtain better accuracy, we conducted a time series analysis to evaluate the trends of total non-accidental mortality, cardiovascular mortality, and respiratory mortality in Shenzhen, based on a 3-year analysis during the period of 2012–2014. This study also attempts to analyze the disparities in mortalities as well as the temporal trends according to sex and age of subgroups.
Methods
Air pollution and death data
This study was performed based on the death registry system (2012–2014) in Shenzhen. Individual records of all deaths were collected in Shenzhen between 2012 and 2014, with “CUMULATIVE OFFICIAL UPDATES TO ICD-10” (WHO 2006) for information on causes of deaths (A00-R94), cardiovascular diseases (ICD-10, I00-I99), and respiratory diseases (ICD-10, J00-J99). Personal information of all deceased individuals was collected on sex, age of death, date of death, and ICD code.
We calculated daily concentrations of sulfur dioxide (SO2), nitrogen dioxide (NO2), ozone (O3), and particle matter 10 (PM10). The measurements of SO2, NO2, O3, and PM10 were retrieved from Shenzhen Environmental Monitoring Center. The daily 24-h SO2 mass concentrations were detected by pulse fluorescence SO2 analyzer (43i, Thermo, MA, USA). The daily 24-h NO2 mass concentrations were detected by a chemiluminescence NO-NO2-NOx analyzer (42i, Thermo, MA, USA). The daily 8-h O3 mass concentrations were detected by an ultraviolet spectrophotometry O3 analyzer (49i, Thermo, MA, USA) (Rodopoulou et al. 2015). The daily 24-h PM10 mass concentrations were detected by the air particle monitor (TEOM 1405, Thermo, MA, USA), and the measurement principle of which is taking continuous direct mass measurements of particulates using a tapered element oscillating microbalance (TEOM). The data were obtained from ten monitoring points: Baoan, Honghu, Huaqiaocheng, Liyuan, Lixiang, Longgang, Nanhu, Nanyou, Yantian, and Xixiang (Fig. 1). The daily concentrations provided in this study were daily mean values measured from these ten monitoring stations. There were no pollution sources around the monitoring points. The quality control processes of monitoring data were in charged by professional personnel.

Locations of the ten monitoring stations in the district map of Shenzhen, China
According to the standard of climatology division in Shenzhen, we distinguish the seasons by air temperature. Five-day moving average of temperature ≥22 °C was regarded as hot season, while five-day moving average of temperature <22 °C was regarded as warm season.
Time series analysis
Relative to the total resident population, the daily mortality is a small-probability event. Therefore, it is approximate to the Poisson distribution. Since the relationship between death and the variables is usually non-linear, time series analysis approach was applied using generalized additive Poisson regression models (semi-parametric general additive model, GAM) by the R Project for Statistical Computing, with package “mgcv,” to estimate the associations between air pollutants and mortalities.
Using time series analysis, the daily mortality was linked to daily levels of SO2, NO2, O3, and PM10 on the previous days. Degree of freedom (df) for the time trend and meteorological variables in our model were assigned based on the previous studies (Lee et al. 2015, Lin et al. 2015, 2016b, Tian et al. 2015):
Log E (Yt) is the expected mortality count on day t, α is the model intercept, s() indicates the penalized smoothing splines, t represents the time series, Temp represents the temperature, Humidity represents the humidity, DOW represents the day of week, β1–β3 are the regression coefficients, and Influenza represents the outbreak of influenza.
The sensitivity was assessed in the smooth function of time trends (df = 6–9 per year) and meteorological variables (the previous 3–5 days’ moving average temperature, df = 3–6, and relative humidity, df = 3–6). According to the reference and our sensitivity analysis results, we adopt 7 df for calendar time, 3 df for average temperature, and 3 df for relative humidity to produce in the best model fitting. A dummy variable for day of the week was introduced to control the systematic variation over time. Also, air pollutants were added separately into lag models. We separately tested SO2, NO2, O3, and PM10 using same-day, 1–6-days lag. We also examined the effects of multi-day lags (the previous 1, 2, 3, and 4 days: lag 0–1, 0–2, 0–3, 0–4, 1–2, 2–3, 3–4, moving average lags, and excess risk (ER) using interquartile range (IQR) increases). Moreover, multi-pollutant models were applied to examine the independent effects of these pollutants. Furthermore, the association between air pollutants and deaths in different genders (male and female) and age groups (age 64 years and younger; age 65 years and older) were also investigated.
In our analyses, several sensitivity analyses were performed to explore the robustness of the models. The sensitivity of the variables was assessed in terms of the df of time trends (6–9), df of mean temperature (3–9), and df of relative humidity (3–7). We also investigated whether associations between one pollutant and mortality were sensitive after adjusting for other pollutants by performing two-pollutant adjusted models where pollutants were included simultaneously with the same lag structure (lag02). For example, in order to analyze the effects of NO2 on mortality without the confounding of O3, we control O3 in the model. The model is shown below:
Thus, the collinearity issue was taken into consideration and was solved in present study.
In addition, there are some data missing of death reports (27/1063, 2.5%) during September and October of 2012. Expectation-maximization was performed to estimate the missing value. After time series analysis, the results showed that there is no significant difference between this data missing and data filling. Thus, in order to maintain objectivity and facticity, original data were used in our manuscript.
All analyses were conducted in SPSS 20.0 and R 3.1.1.
This study was approved by the Ethics Committee of Shenzhen Center for Disease Control and Prevention, the permit number is No. 20161018.
Results
Study population and air pollution characteristics
The characteristics of study population, the meteorology, and air pollutant data were shown in Table 1. The number of total non-accidental mortality in Shenzhen was 35,261 in 2012–2014. Total non-accidental mortality, cardiovascular mortality, and respiratory mortality were all higher for males (20.28 ± 6.06, 7.23 ± 3.07, 1.74 ± 0.98, respectively) and for elder (age 65 years and older; 33.46 ± 7.45, 7.83 ± 3.25, 1.95 ± 1.12, respectively). It’s worth mentioning that from January 1, 2013 to December 31, 2014, there are 93.56% (683/730) days which the concentrations of daily PM2.5 in Shenzhen were below the Chinese national standard limit (0–35 μg/m3 for the first level, 35–75 μg/m3 for the second level (China 2012)). The daily meteorological condition and pollution status in Shenzhen were shown in Supplementary Fig. 1 and Supplementary Fig. 2. The time series analysis of daily levels of pollutants in Shenzhen suggested that GAM model was suitable for the present study.
The variabilities of daily total non-accidental mortality and cardiovascular mortality by years using the time series were presented in Supplementary Fig. 3A and B. The variability of daily respiratory mortality could not be shown as line graph for the limited number of subjects, thus it was shown in Supplementary Fig. 3C. Supplementary Fig. 4 exhibited an increasing trend of mortalities during the 2012–2014 periods.
Spearman rank correlation analysis
Spearman rank correlation analysis was performed to analyze the relationship among the air pollutants and the meteorological factor (Table 2). The air pollutants were significantly negatively associated with temperature and humidity (comparing with temperature, r SO2 = −0.163, r NO2 = −0.404, r PM10 = −0.348; comparing with humidity, r SO2 = −0.504, r NO2 = −0.063, r O3 = −0.548, r PM10 = −0.568). SO2 was positively associated with NO2 (r = 0.618), O3 (r = 0.315) and PM10 (r = 0.738). PM10 was significantly positively associated with NO2 (r = 0.599) and O3 (r = 0.573).
Regression results
Single-pollutant models
Using a single model, adjusted ER (95% CI) of mortality and SO2, NO2, O3, and PM10 IQR increases for lag periods (lag0–lag6, lag01–lag04, lag12, lag23, lag34) were presented in Fig. 2. Among the lag day analyses, the maximum effects and the most significant results were both considered as the criteria for further analysis. Finally, the lag02 day was found to have the most model fit (Supplement Table 1).

Risk estimates were expressed as excess risk (ER) with 95% CI per IQR increase of daily mean concentration of SO2, NO2, O3, and PM10 with different lag days (single lags for the current day (lag0) to 6 days before the current day (lag6); 1 day before the current day to 2 days before the current day (lag12), lag23, lag34, and multi-day lags for the current day and prior 1 day before (lag01), 2 days (lag02), 3 days (lag03), and 4 days (lag04))
The results showed that SO2, NO2, and PM10 were significantly associated with total non-accidental mortality, with the maximum effects observed at lag02 day (3-day moving average), and the corresponding ER for per IQR increase was 2.84 (95% confidence interval (CI) 0.33%, 5.41%), 6.05 (95% CI 3.38%, 8.78%), and 4.36% (95% CI 1.12%, 7.70%), respectively (P < 0.05). O3 was significantly associated with total non-accidental mortality only at lag4 day, the corresponding ER for per IQR increase was 2.48% (95% CI 0.04%, 4.97%) (P < 0.05). SO2 was significantly associated with cardiovascular mortality, with the maximum effects observed at lag5 day, the corresponding ER for per IQR increase was 3.83% (95% CI 1.28%, 6.45%) (P < 0.01).
NO2 and PM10 were significantly associated with cardiovascular mortality, with the maximum effects observed at lag02 day (3-day moving average), and the corresponding ER for per IQR increase was 6.88 (95% confidence interval (CI) 2.98%, 10.93%) and 6.51% (95% CI 1.70%, 11.55%), respectively (P < 0.05). However, there were no significant effects observed among the respiratory mortality and SO2, NO2, PM10, and O3.
The analyses between SO2, NO2, PM10, O3, and subgroups of mortality were shown in Table 3. In single lag model (lag02), once the concentration of PM10 is increased per IQR, total non-accidental mortality of all ages is all significantly increased. Once the concentration of NO2 is increased per IQR, significantly higher ERs of total non-accidental mortality will affect men than women (P < 0.05). Furthermore, once the concentration of PM10 is increased per IQR, total non-accidental mortality of all ages is all significantly increased. Once the concentrations of SO2/NO2/PM10 are increased per IQR, significantly higher ERs of cardiovascular mortality will affect men than women (P < 0.05). Similarly, once the concentrations of SO2/NO2/PM10 are increased per IQR, significantly higher ERs of cardiovascular mortality will affect the elderly (65 years and older) than younger (64 years and younger) (P < 0.05).
In single lag model (lag4), the total non-accidental mortality for men showed a significantly higher ER with PM10 and NO2 in both increase types. Moreover, the total non-accidental mortality for the elder (65 years and older) showed a significantly higher ER with PM10 and O3 in IQR increase type.
The 10-μg/m3 increasing type was also made in lag models in the present study. The results were consistent with the IQR increasing type (Supplement Table 1).
Sensitivity analysis results
Multi-pollutant adjusted analysis
The air pollutants models which showed significant differences in lag02 day were further analyzed in two-pollutant adjusted models. The results of lag02 in two-pollutant adjusted models were shown in Table 4. The adverse effects for NO2 remained significantly associated with both total non-accidental mortality and cardiovascular mortality after adjusting for all other pollutants in IQR increase type. However, the adverse effects for PM10/SO2 remained significantly associated with both total non-accidental mortality and cardiovascular mortality only after adjusting for O3 in IQR increase type. Meanwhile, there were no significant associations between PM10/SO2 and mortality after adjusting for other pollutants. Moreover, there were no significant associations between SO2, NO2, PM10, and respiratory mortality after adjusting for other pollutants.
Season analysis
The significant association between NO2 and total non-accidental mortality was observed in hot season but not in warm season in lag02 days (Table 5). The significance appeared to be larger after adjusting for other pollutants. A significant seasonal pattern with increased counts in hot season and lower counts in warm season was observed between NO2 and total non-accidental mortality in lag02 days, due to moderate seasonal variability. Meanwhile, the significant association between NO2 and cardiovascular mortality was observed in hot season but not in warm season in lag02 days. The counts were significant and appeared to be larger after adjusting for SO2, O3, and PM10. There were no significant associations between SO2, PM10, total non-accidental mortality, and cardiovascular mortality in either warm season or hot season. There were no significant associations between SO2, NO2, PM10, and respiratory mortality in either warm season or hot season.
Exposure-response analysis
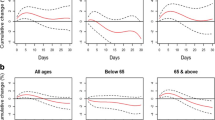
Fig. 3A plotted the exposure-response relationships between air pollutants (SO2, NO2, PM10, and O3) and total non-accidental mortality. The 25–75% ambient pollutant concentrations were considered as reasonable and credible ranges. The shapes of SO2 and PM10 curves were similar and approximate linear at the 25–75% ambient levels. There was an inflection point in the shape of NO2 curve at the ambient NO2 levels, and then the shape of NO2 curve tends to become linear at higher ambient concentrations.

Exposure-response curves for daily mean concentration of air pollutants (SO2, NO2 PM10, and O3) at distributed lag02 days and its association with total non-accidental mortality and cardiovascular mortality in single-pollutant model, after adjusting for the time trend, seasonality, meteorological factors, DOW effect, and influenza epidemics. X axis represents the concentration of air pollutants (μg/m3). The 25–75% ambient pollutant concentrations were considered as reasonable and credible ranges. The solid line represents the effect estimates; the gray area represents the 95% confidence intervals (CI)
Fig. 3B plotted the exposure-response relationships between air pollutants (SO2, NO2, and PM10) and cardiovascular mortality. The shapes of SO2 and PM10 curves were similar and approximate linear at the 25–75% ambient levels. The 25–75% ambient levels of NO2 are 33.47–74.36 μg/m3. The shapes of NO2 curve were approximate linear at the 33.4–40.91-μg/m3 NO2 levels. There was a peak in the shape of NO2 curve at 40.92-μg/m3 NO2 levels, and then the shape of NO2 curve tended to become a horizontal line at 40.93–74.36-μg/m3 NO2 levels.
Discussion
In this time series study, we demonstrated positive correlations between ambient NO2 and mortality outcomes (total non-accidental mortality and cardiovascular mortality). The association became stronger when the co-pollutants (SO2, O3, and PM10) were adjusted in two-pollutant adjusted models. Men and subjects age 65 years and older appeared to be more sensitive to ambient NO2. Ambient SO2 and PM10 were also positively associated with daily mortality, but the associations were not always significant after different lag analyses or adjusting for co-pollutants. The significant associations between effects of SO2 and PM10 on total non-accidental mortality and cardiovascular mortality on lag02 day were observed in single-pollutant model. Meanwhile, co-pollutant analysis showed that the significant associations were not confounded by O3.
We examined the concentration-response relationship using a smoothing function; the result suggested an approximately linear relationship without an obvious threshold. Thus, we used the non-threshold model.
Shenzhen has undergone rapid economic growth through industrialization and urbanization, which could be characterized by extension of building and traffic density. Therefore, as one of the crucial constituent of traffic-related pollutants, an overload of NO2 in Shenzhen is not strange. In our study, the rise of NO2 significantly raised the total non-accidental mortality risk at lag0, lag1, lag2, lag3, lag4, lag01, lag02, lag03, lag04, lag12, lag23, and lag34; increasing NO2 significantly raised the cardiovascular mortality risk at lag0, lag1, lag01, lag02, lag03, lag04, and lag12, but not at lag5 and lag6 days; these results indicate rapid effect of short-term NO2 exposure on mortality outcomes.
In China, the air quality standards (24-h level, 8-h for O3) of SO2, NO2, O3, and PM10 should not exceed 50, 80, 100, and 70 μg/m3, respectively. Our results showed that concentrations of pollutants in Shenzhen were within these standards. But concentration of NO2 in Shenzhen was higher than the year mean standards (40 μg/m3). Therefore, our results might partly attribute to the higher median concentrations of NO2 (44.93 μg/m3). The results of strong relationship between ambient NO2 and total non-accidental mortality are consistent with the study in Nanjing, China (Lu et al. 2015). They reported that mortality risks were associated with ambient concentrations of NO2 (51.5 ± 19.8 μg/m3). Being consistent with the present results, Italian researchers also reported that there were significant effects of NO2 on natural, cardiac, and respiratory mortality in Italian cities (Chiusolo et al. 2011).
Ambient PM pollution has been considered as a potential risk factor for mortality (Brunekreef & Holgate 2002, Stafoggia et al. 2015). Some studies have reported the health effect of PM10 (Carreras et al. 2015, Lin et al. 2015, Nasser et al. 2015, Pinheiro Sde et al. 2014). One interesting study examined the effectiveness of the air pollution controlling measures during the 2010 Asian Games period in Guangzhou and found a significant reduction in PM10 concentration, followed by obvious mortality reduction (Hualiang Lin et al. 2014). Ting Wang et al. found that there were strong associations between daily cardiovascular and ambient PM10 exposure (10–503 μg/m3) in Tianjin Binhai New Area. Similarly, our results demonstrated that PM10 was associated with total non-accidental mortality and cardiovascular mortality in Shenzhen in lag02 days.
There were no significant associations between SO2, NO2, O3, PM10, and the respiratory mortality in present study. This may be partly due to the climate of Shenzhen. Some researchers observed significant inactiveness of some respiratory viruses under relatively higher temperature (Chan et al. 2015). Besides, another reason for these outcomes is that the air pollutions in Shenzhen are within the current air quality standards (Perez et al. 2015).
Meanwhile, the daily mean ambient O3 concentration in Shenzhen (32.24 μg/m3) is slightly higher than that in Korea (31.44 μg/m3) and Japan (29.04 μg/m3). Sanghyuk Bae et al. reported the non-linear concentration-response relationships between daily mean ambient O3 concentration and the daily number of non-accidental death in Japanese and Korean cities (Bae et al. 2015). Our result is consistent with their studies. However, there were no significant associations between O3 and the cardiovascular mortality and O3 and the respiratory mortality in the present study.
After two-pollutant adjusted model analyses, it should be noticed that the levels of O3 could significantly modify the effects of NO2, SO2, and PM10 on total non-accidental mortality and significantly modify the effects of NO2 and PM10 on cardiovascular mortality in the present study. Some studies argued that NO2 and O3 might act through similar biological pathways and increase mortality risks (Lang-Yona et al. 2016).
After seasonal analyses, the positive associations of NO2 with total non-accidental mortality were only found in hot seasons, but not in warm seasons, even after adjusting for other pollutants. Similarly, the positive associations of NO2 with cardiovascular mortality were only found in hot seasons, but not in warm seasons, even after adjusting for SO2, SO2 + O3, and SO2 + O3 + PM10. These seasonal trends are consistent with the previous study in Shenzhen (Dai et al. 2015). There were significant associations between SO2, PM10, and total non-accidental mortality or cardiovascular mortality in the whole year data, but no significant associations in either warm season data or hot season data. The possible reason is that the study power was reduced in subgroup analyses.
From the exposure-response curves, we observed approximate linear association between pollutants (SO2 and PM10) and total non-accidental mortality and association between pollutants (SO2 and PM10) and cardiovascular mortality. What is more, we observed significant increases in mortality risk even when the concentrations of air pollutants were within the current air quality standards. Therefore, we did not set any thresholds for this curve. Besides, we could see that the 95% CI in relationships between air pollutants (SO2, NO2, and PM10) and total non-accidental mortality was much narrower than that of between air pollutants (SO2, NO2, and PM10) and cardiovascular mortality. This result demonstrated that relationships between air pollutants and total non-accidental mortality are better than relationships between air pollutants and cardiovascular mortality with respect to the reliability of sample indexes to estimate the population parameter.
There are a few limitations in present study. Firstly, we only had 3-year completed and accurate data. We will keep collecting data, and long-term time series analyses will be completed in the near future. Moreover, modeling the associations between air pollutants and mortality outcomes, even after adjusting for covariates, cannot completely reflect the causal effects for other influence factors. Another limitation of this study was that we did not have access to ambient PM2.5 data, limiting our ability to control for its potential confounding effect. Though, one of the multi-city studies in China reported a significant mortality effect and burden associated with ambient PM2.5 in South China (Lin et al. 2016a). However, in view of the low concentration of PM2.5, there might also be hardly any confounding effects of PM2.5 to NO2 concentration in Shenzhen City.
Conclusions
In conclusion, the present study identified the adverse effects of NO2, SO2, and PM10 on the total non-accidental mortality and the cardiovascular mortality in Shenzhen, especially in men and elder subgroups in hot seasons. Our results suggested that the health risks caused by ambient NO2 in current concentrations would be greatest for citizens. Therefore, much more attention and efforts are urgently needed to protect residents from air pollutants. Moreover, controlling the amount of vehicles and alleviating vehicular emissions seem to be one of the effective ways to resolve the air pollution issue in Shenzhen.
References
Bae S, Lim YH, Kashima S, Yorifuji T, Honda Y, Kim H, Hong YC (2015) Non-linear concentration-response relationships between ambient ozone and daily mortality. PLoS One 10:e0129423
Brunekreef B, Holgate ST (2002) Air pollution and health. Lancet 360:1233–1242
Carreras H, Zanobetti A, Koutrakis P (2015) Effect of daily temperature range on respiratory health in Argentina and its modification by impaired socio-economic conditions and PM10 exposures. Environ Pollut 206:175–182
Chan PK, Tam WW, Lee TC, Hon KL, Lee N, Chan MC, Mok HY, Wong MC, Leung TF, Lai RW, Yeung AC, Ho WC, Nelson EA, Hui DS (2015) Hospitalization incidence, mortality, and seasonality of common respiratory viruses over a period of 15 years in a developed subtropical city. Medicine 94:e2024
Chen B, Hong C, Kan H (2004) Exposures and health outcomes from outdoor air pollutants in China. Toxicology 198:291–300
Chen L, Villeneuve PJ, Rowe BH, Liu L, Stieb DM (2014) The Air Quality Health Index as a predictor of emergency department visits for ischemic stroke in Edmonton, Canada. J Expo Sci Environl Epidemiol 24:358–364
Chiusolo M, Cadum E, Stafoggia M, Galassi C, Berti G, Faustini A, Bisanti L, Vigotti MA, Dessi MP, Cernigliaro A, Mallone S, Pacelli B, Minerba S, Simonato L, Forastiere F, EpiAir Collaborative G (2011) Short-term effects of nitrogen dioxide on mortality and susceptibility factors in 10 Italian cities: the EpiAir Study. Environ Health Perspect 119:1233–1238
Dai X, He X, Zhou Z, Chen J, Wei S, Chen R, Yang B, Feng W, Shan A, Wu T, Guo H (2015) Short-term effects of air pollution on out-of-hospital cardiac arrest in Shenzhen, China. Int J Cardiol 192:56–60
Ferrari J, Shiue I, Seyfang L, Matzarakis A, Lang W, Austrian Stroke Registry C (2015) Weather as physiologically equivalent was not associated with ischemic stroke onsets in Vienna, 2004–2010. Environ Sci Pollut Res Int 22:8756–8762
Gleason JA, Fagliano JA (2015) Associations of daily pediatric asthma emergency department visits with air pollution in Newark, NJ: utilizing time-series and case-crossover study designs. J Asthma: Off J Assoc Care Asthma 52:815–822
Lang-Yona N, Shuster-Meiseles T, Mazar Y, Yarden O, Rudich Y (2016) Impact of urban air pollution on the allergenicity of Aspergillus fumigatus conidia: outdoor exposure study supported by laboratory experiments. Sci Total Environ 541:365–371
Lee H, Honda Y, Hashizume M, Guo YL, Wu CF, Kan H, Jung K, Lim YH, Yi S, Kim H (2015) Short-term exposure to fine and coarse particles and mortality: a multicity time-series study in East Asia. Environ Pollut 207:43–51
Li H, Chen R, Meng X, Zhao Z, Cai J, Wang C, Yang C, Kan H (2015) Short-term exposure to ambient air pollution and coronary heart disease mortality in 8 Chinese cities. Int J Cardiol 197:265–270
Lin H, Zhang Y, Liu T, Xiao J, Xu Y, Xu X, Qian Z, Tong S, Luo Y, Zeng W, Ma W (2014) Mortality reduction following the air pollution control measures during the 2010 Asian Games. Atmos Environ 91:24–31
Lin H, Tao J, Du Y, Liu T, Qian Z, Tian L, Di Q, Rutherford S, Guo L, Zeng W, Xiao J, Li X, He Z, Xu Y, Ma W (2015) Particle size and chemical constituents of ambient particulate pollution associated with cardiovascular mortality in Guangzhou, China. Environ Pollut
Lin H, Liu T, Xiao J, Zeng W, Li X, Guo L, Zhang Y, Xu Y, Tao J, Xian H, Syberg KM, Qian ZM, Ma W (2016a) Mortality burden of ambient fine particulate air pollution in six Chinese cities: results from the Pearl River Delta Study. Environ Int 96:91–97
Lin H, Tao J, Du Y, Liu T, Qian Z, Tian L, Di Q, Rutherford S, Guo L, Zeng W, Xiao J, Li X, He Z, Xu Y, Ma W (2016b) Particle size and chemical constituents of ambient particulate pollution associated with cardiovascular mortality in Guangzhou, China. Environ Pollut 208:758–766
Liu T, Zhang YH, Xu YJ, Lin HL, Xu XJ, Luo Y, Xiao J, Zeng WL, Zhang WF, Chu C, Keogh K, Rutherford S, Qian Z, Du YD, Hu M, Ma WJ (2014) The effects of dust-haze on mortality are modified by seasons and individual characteristics in Guangzhou, China. Environ Pollut 187:116–123
Lu F, Zhou L, Xu Y, Zheng T, Guo Y, Wellenius GA, Bassig BA, Chen X, Wang H, Zheng X (2015) Short-term effects of air pollution on daily mortality and years of life lost in Nanjing, China. Sci Total Environ 536:123–129
Nasser Z, Salameh P, Nasser W, Abou Abbas L, Elias E, Leveque A (2015) Outdoor particulate matter (PM) and associated cardiovascular diseases in the Middle East. Int J Occup Med Environ Health 28:641–661
Perez L, Grize L, Infanger D, Kunzli N, Sommer H, Alt GM, Schindler C (2015) Associations of daily levels of PM10 and NO(2) with emergency hospital admissions and mortality in Switzerland: trends and missed prevention potential over the last decade. Environ Res 140:554–561
Pinheiro Sde L, Saldiva PH, Schwartz J, Zanobetti A (2014) Isolated and synergistic effects of PM10 and average temperature on cardiovascular and respiratory mortality. Rev Saude Publica 48:881–888
Rodopoulou S, Samoli E, Chalbot MC, Kavouras IG (2015) Air pollution and cardiovascular and respiratory emergency visits in Central Arkansas: a time-series analysis. Sci Total Environ 536:872–879
Samoli E, Peng R, Ramsay T, Pipikou M, Touloumi G, Dominici F, Burnett R, Cohen A, Krewski D, Samet J, Katsouyanni K (2008) Acute effects of ambient particulate matter on mortality in Europe and North America: results from the APHENA study. Environ Health Perspect 116:1480–1486
Scheers H, Jacobs L, Casas L, Nemery B, Nawrot TS (2015) Long-term exposure to particulate matter air pollution is a risk factor for stroke: meta-analytical evidence. Stroke 46:3058–3066
Shenzhen Statistics Bureau (2015) Statistics annual report in Shenzhen China
Shenzhen Traffic Management Bureau (2015) Transportation statistics annual report in Shenzhen, China
Silverman RA, Ito K (2010) Age-related association of fine particles and ozone with severe acute asthma in New York City. J Allergy Clin Immunol 125(367–373):e5
Stafoggia M et al (2015) Desert dust outbreaks in southern Europe: contribution to daily PM concentrations and short-term associations with mortality and hospital admissions. Environ Health Perspect
Tian L, Qiu H, Pun VC, Ho KF, Chan CS, Yu IT (2015) Carbon monoxide and stroke: a time series study of ambient air pollution and emergency hospitalizations. Int J Cardiol 201:4–9
Xie SH, Wu YS, Liu XJ, Fu YB, Li SS, Ma HW, Zou F, Cheng JQ (2016) Mortality from road traffic accidents in a rapidly urbanizing Chinese city: a 20-year analysis in Shenzhen, 1994–2013. Traffic Inj Prev 17:39–43
World Health Organization (2006) The international classification of diseases ICD-10, 2nd edn., vol 1
Acknowledgements
Authors thank the Shenzhen Environmental Monitoring Center and Meteorological Bureau of Shenzhen Municipality for supplying the air monitoring data. This work was supported by the National Natural Science Foundation of China (Grant No. 81573242) and China Postdoctoral Science Foundation funded project (Grant No. 2016M602537).
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
The authors’ declare that there is no conflict of interest.
Additional information
Responsible editor: Philippe Garrigues
Electronic supplementary material
Supplementary Fig. 1
(GIF 188 kb)
Supplementary Fig. 2
(GIF 385 kb)
Supplementary Fig. 3
(GIF 354 kb)
Supplementary Fig. 4
(GIF 43 kb)
Supplementary Table 1
(DOCX 18 kb)
Supplementary Table 2
(DOCX 18 kb)
Supplementary Table 3
(DOCX 15 kb)
Rights and permissions
About this article

Cite this article
Guo, Y., Ma, Y., Zhang, Y. et al. Time series analysis of ambient air pollution effects on daily mortality. Environ Sci Pollut Res 24, 20261–20272 (2017). https://doi.org/10.1007/s11356-017-9502-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-017-9502-7