
Abstract
Stroke rates were found to have seasonal variations. However, previous studies using air temperature, humidity, or air pressure separately were not adequate, and the study catchment was not clearly drawn. Therefore, here we proposed to use a thermal index called physiologically equivalent temperature (PET) that incorporates air temperature, humidity, wind speed, cloud cover, air pressure and radiation flux from a biometeorological approach to estimate the effect of weather as physiologically equivalent on ischemic stroke onsets in an Austrian population. Eight thousand four hundred eleven stroke events in Vienna registered within the Austrian Stroke Unit Register from January 1, 2004 to December 31, 2010 were included and were correlated with the weather data, obtained from the Central Institute for Meteorology and Geodynamics in the same area and study time period and calculated as PET (°C). Statistical analysis involved Poisson regression modeling. The median age was 74 years, and men made up 49 % of the entire population. Eighty percent had hypertension while 25.4 % were current smokers. Of note, 26.5 % had diabetes mellitus, 28.9 % had pre-stroke, and 11.5 % had pre-myocardial infarction. We have observed that onsets were higher on the weekdays than on the weekend. However, we did not find any significant association between PETs and ischemic stroke onsets by subtypes in Vienna. We did not observe any significant associations between PETs and ischemic stroke onsets by subtypes in Vienna. Hospital admission peaks on the weekdays might be due to hospital administration reasons.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Environmental factors have been central to many human chronic diseases, and the weather is no exception. The effect of the weather has been noted in scientific literature since the 1930s as increased hospital admissions due to coronary occlusion and heart failure were observed in correlation with low temperature that has prompted the concern on the influence of the seasonality effect (Bean and Mills 1938). The hypothesized mechanism was that an acute change in environmental temperature, being too cold or too hot (Bhaskaran, et al. 2009), tends to increase myocardial oxygen consumption and may induce cardiac arrhythmias or an anginal attack (Ansari and Burch 1969; Epstein, et al. 1969; Milo-Cotter, et al. 2006). In addition, activation of the sympathetic nervous system and secretion of catecholamine could increase in response to low temperature that could be observed by the increased heart rate and peripheral vascular resistance (Hanna 1999). However, overall across the globe, conflicting results on the effect of the weather on human health outcomes have been presented in the literature. While there are complex interactions between the weather and human health outcomes that have been observed, methodological concerns on the risk assessment from previous research have been brought up recently (Modesti 2013). Seemingly, correlating air temperature and human health outcomes might not be adequate since there has been difference between air temperature and the weather as biometeorological incorporating relevant meteorological parameters (Shiue and Matzarakis 2011). Therefore, following this context, we aimed to first investigate the monthly variations of hospital admissions of ischemic stroke and then to correlate the weather as biometeorological and hospital admissions of ischemic stroke by subtypes in a city-wide setting in recent years.
Methods
Study sample
As described previously (Ferrari, et al. 2010), between 1 January, 2004 and December 31, 2010, 41,901 prospectively registered hospital onsets with acute stroke in the Austrian Stroke Unit Registry were entered into the database. The number of patients registered over years is shown in Fig. 1. The Austrian Stroke Unit Registry is a comprehensive and high-quality nationwide database concerning the treatment and care of patients in stroke units that are located across the whole country. The number of documented ischemic stroke patients has increased from about 1400 in 2003 to more than 9000 in 2010. The reason for that is the growing number of participating centers in this time period. Ischemic stroke subtypes in the current analysis were identified according to TOAST classification (Adams, et al. 1993), namely, large-artery atherosclerosis, cardioembolism, small-vessel occlusion, stroke of other determined etiology, and stroke of undetermined etiology. Data that were collected included characteristics, management and outcome of all stroke patients and were performed by experienced stroke neurologists using standardized definitions and scores. All aspects of data entry, data protection, administration and scientific analysis were regulated by law (Federal Law on Quality in Health, Federal Law on GesundheitÖsterreich GmbH § 15a, and Stroke Unit Registry Act), and therefore, every involved clinician would have to follow the such strict procedure. For the weather data, we obtained daily air temperature, air humidity, wind speed and cloud cover from Central Institute for Meteorology and Geodynamics for three Vienna weather stations, namely, Hohe Warte, Groß Enzersdorf and Schwechat (see Fig. 2).

Number of registered ischemic stroke patients from 2004 to 2010

Distribution of the included stroke units and weather stations in Vienna
Statistical analysis
We first incorporated air temperature, air humidity, wind speed and cloud cover into an integrated thermal index, which is called physically equivalent temperature (PET) with a widely known unit, °C, in the present analysis (see Fig. 3). PET has been used to consider a heat balance of the human body under the standard conditions in an outdoor setting (Höppe 1999; Matzarakis, et al. 2007). In short, it is initially created to characterize and evaluate the thermal bioclimate in a physiologically significant manner. The application of PET assessment can be carried out by a RayMan model.9

Relationship of daily air temperature and PET between Jan 1, 2010 and December 31 in 2010 in Vienna
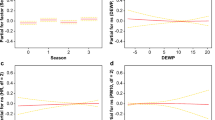
Since the target variable, stroke onsets, was Poisson distributed, a Poisson regression model was fitted and the effects were reported with 95 % confidence intervals (CIs). Specifically, for model specification, the bidirectional stepwise variable selection procedure was executed, optimizing the Akaike information criterion (AIC). The following variables were allowed as potentially explanatory variables in the selection process: day of the week; sinusoidal annual oscillations with maximum at the 1st, …, 365th day of the year; the 7 a.m.-, and 2 and 7 p.m.-PET; and several features derived from the PET—the n-day change 2 p.m.PETi–2 p.m.PETi-n for n = 1, …, 5; the k-day-mean for k = 1, …, 7; the warming 2 p.m.PET–7 a.m.PET; and a categorized PET with the levels (−Inf,4), (4,8), (8,18), (18,29), (29,35), (35,41), (41,Inf). In addition to the intercept, the final model contained the variables day of the week and an annual oscillation with its maximum at April 9 and minimum at October 9. None of the PET-related variables was included in the final model that is none of these features could improve the model according to the used Akaike information criterion.
All statistical analyses were performed in R, version 2.15.2 (R Core Team 2012) statistical software package. Since this is only a secondary data analysis, no further ethnical approval was required.
Results
Between 1 January, 2004 and 31 December, 2010, there were 8411 ischemic stroke patients from all 10 Stroke Units in Vienna identified for the current analysis. Patient demographics, clinical characteristics, and classical cardiovascular risk factors are shown in Table 1. The mean age was 74, and men made up 49 % of the study sample. Eighty percent of patients had hypertension while 25.4 % were current smokers. Of note, 26.5 % had diabetes mellitus, 28.9 % had pre-stroke, and 11.5 % had pre-myocardial infarction. Daily ischemic stroke onsets by day of the week were displayed in Fig. 4. Apparently, ischemic stroke onsets were significantly lower over the weekend than during the week (p = 0.028, chi-square test of independence). However, we did not find any association between ischemic stroke onsets and PET. We also modeled to see PET at different times including 7 a.m., and 2 and 7 p.m., mean value of the day and changes in the previous days. Still, no clear associations were found.

Ischemic stroke onset variations by day of the week between January 1, 2004 and December 31, 2010
Discussion
To our knowledge, this is the first study analyzing the relationship of PETs and ischemic stroke onsets by subtypes in Vienna over 7 years. The present study showed that the PET was not linked with ischemic stroke onsets. In other words, the daily (and perhaps monthly) variations in ischemic stroke onsets in Vienna cannot be explained solely by the weather. We have noted that there were fewer onsets on the weekend than on the weekdays. One reason could be that patients with mild deficit could have neglected their symptoms and believed to get well in a short time. Moreover, the impression for the general public is that the medical facility is more readily on the weekdays than the weekend. Therefore, we hypothesized that they might have waited for 1 or 2 days before urgently reaching the ambulance or outpatient clinics.
The present study has a number of strengths. First, our study is unique in terms of its size and the rigorous quality control in the Austrian Stroke Registry. Therefore, selection bias has been largely minimized. Second, we used weather data from three weather stations representative of Vienna that overcame the limitation of previous studies with single weather station to correlate with health data from a large geographic region. Third, we used 7 years of data in order to ensure that we could reach statistical power. However, there were still a few limitations worthy of being noted. First, three weather stations might not perfectly cover the entire Vienna region. Second, we did not include air pollution data to be adjusted since the air pollution level could have been reduced (more details via http://aqicn.org/map/austria/) in Austria. Therefore, the effect from air pollution would be minimal. From a meteorological point of view, when investigating the weather effect, it would make scientific sense to generate climatic variables into single index since they interact with each other at the same time and 1 °C in a cold climate would mean differently in a warm climate (Sabetghadam and Ahmadi-Givi 2014). There should also be indexes to be developed that could additionally incorporate air pollutants since they could influence each other at the same time. However, this might be methodologically difficult since the level of each pollutant could vary across each geographic region. Future studies keeping the strengths and overcoming the limitations would be warranted.
In conclusion, we did not observe any significant association between PET and ischemic stroke onsets by subtypes in Vienna between 2004 and 2010. Hospital admission peaks on the weekdays might be due to hospital administration reasons (e.g., people avoid weekend admissions, people lack awareness of primary symptoms, etc). Future research looking into these aspects would be suggested.
References
Adams HP Jr, Bendixen BH, Kappelle LJ, Biller J, Love BB, Gordon DL, Marsh EE 3rd (1993) Classification of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Rial of Org 10172 in acute stroke treatment. Stroke 24:35–41
Ansari A, Burch GE (1969) Influence of hot environments on the cardiovascular system: a clinical study of 23 cardiac patients at rest. Arch Intern Med 123:371–378
Bean WB, Mills CA (1938) Coronary occlusion, heart failure, and environmental temperatures. Am Heart J 16:701–713
Bhaskaran K, Hajat S, Haines A, Herrett E, Wilkinson P, Smeeth L (2009) Effects of ambient temperature on the incidence of myocardial infarction. Heart 95:1760–1769
Epstein SE, Stampfer M, Beiser D, Goldstein RE, Braunwald E (1969) Effects of a reduction in environmental temperature on the circulatory response to exercise in man—implications concerning angina pectoris. N Engl J Med 280:7–11
Ferrari J, Knoflach M, Kiechl S, Willeit J, Schnabl S, Seyfang L, Lang W, Austrian Stroke Unit Registry Collaborators (2010) Early clinical worsening in patients with TIA or minor stroke: the Austrian stroke unit registry. Neurology 74:136–141
Hanna JM (1999) Climate, altitude, and blood pressure. Hum Biol 71:553
Höppe P (1999) The physiological equivalent temperature - a universal index for the biometeorological assessment of the thermal environment. Int J Biometeorol 43:71–75
Matzarakis A, Rutz F, Mayer H (2007) Modelling radiation fluxes in simple and complex environments - application of the RayMan model. Int J Biometeorol 51:323–334
Milo-Cotter O, Setter I, Uriel N, Kaluski E, Vered Z, Golik A, Cotter G (2006) The daily incidence of acute heart failure is correlated with low minimal night temperature: cold immersion pulmonary edema revisited? J Card Fail 12:114–119
Modesti PA (2013) Season, temperature and blood pressure: a complex interaction. Eur J Intern Med 24:604–607
R Core Team (2012). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. http://www.R-project.org/
Sabetghadam S, Ahmadi-Givi F (2014) Relationship of extinction coefficient, air pollution, and meteorological parameters in an urban area during 2007 to 2009. Environ Sci Pollut Res Int 21:538–547
Shiue I, Matzarakis A (2011) When stroke epidemiology meets weather and climate: a heat exposure index from human biometeorology. Int J Stroke 6:176
Acknowledgments
IS was supported by University of Exeter Outward Mobility Fellowship when initiating the international research collaboration and is now supported by the Global Platform for Research Leaders scheme.
Conflict of interest
None.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
Responsible editor: Philippe Garrigues
Appendix Austrian Stroke-Unit-Registry Contributing Austrian Stroke-Unit-Registry Collaborators
Appendix Austrian Stroke-Unit-Registry Contributing Austrian Stroke-Unit-Registry Collaborators
Johannes Sebastian Mutzenbach, MD (Christian-Doppler-Clinic, Salzburg, local site investigator); Katharina Stadler, MD (Christian- Doppler-Clinic, Salzburg,local site investigator); Cornelia Rösler, MD (Christian-Doppler-Clinic, Salzburg, local site investigator); Regina Katzenschlager, MD (Donauspital, Vienna, local site investigator); Sabine Torma, MD (Donauspital, Vienna, local site investigator); Miroslav Krstic, MD (Donauspital, Vienna, local site investigator); Franz Gruber, MD (General Hospital, Linz, local site investigator); Milan R. Vosko, MD (General Hospital, Linz, local site investigator); Cornelia Brunner, MD (General Hospital, Linz, local site investigator), Michael Brainin, MD (Hospital Donauregion, Tulln, study coordinator); Karl Matz, MD (Hospital Donauregion, Tulln, local site investigator); Yvonne Teuschl, MD (Hospital Donauregion, Tulln, local site investigator); Omid Hosseiny, MD (Hospital Göttlicher Heiland,Vienna, local site investigator); Wolf Muellbacher, MD (Hospital Göttlicher Heiland,Vienna, local site investigator); Dietlind Resch, MD (Hospital Hietzing, Vienna, local site investigator); Martina Mayr, MD (Hospital Hietzing, Vienna, local site investigator) Robert Paur, MD (Hospital Hietzing, Vienna, local site investigator); Otto Berger, MD (Hospital Kaiser Franz-Josef, Vienna, local site investigator); Vera Nussgruber,MD (Hospital Kaiser Franz-Josef, Vienna, local site investigator); Wolfgang Grisold, MD (Hospital Kaiser Franz-Josef, Vienna, local site investigator); Joerg Weber, MD (Hospital Klagenfurt, local site investigator); Heinz Kohlfuerst, MD (Hospital Klagenfurt, local site investigator); Klaus Berek, MD (Hospital Kufstein, local site investigator); Markus Mayr, MD (Hospital Kufstein, local site investigator); Stefan Haaser, MD (Hospital Kufstein, local site investigator); Susanne Asenbaum-Nan, MD (Hospital Mostviertel, Amstetten, local site investigator); Dietmar Schafelner, MD (Hospital Mostviertel, Amstetten, local site investigator); Berthold Kepplinger, MD (Hospital Mostviertel, Amstetten, local site investigator); Alexandra Herbst, MD (Hospital Oberwart, local site investigator); Barbara Muellauer, MD (Hospital Oberwart, local site investigator); Eva Schubert-Vadon, MD (Hospital Oberwart, local site investigator); Christian Eggers, MD (Hospital of the Mercy Friars Linz, local site investigator); Christof Bocksrucker, MD (Hospital of the Mercy Friars Linz, local site investigator); Andrea Hackenbuchner, MD (Hospital Otto Wagner, Vienna, local site investigator); Martin Krichmayr, MD (Hospital Rudolfstiftung, Vienna, local site investigator); Peter Sommer, MD (Hospital Rudolfstiftung, Vienna, local site investigator); Elisabeth Fertl, MD (Hospital Rudolfstiftung, Vienna, local site investigator); Herbert Koller, MD (Hospital LSF Graz, local site investigator); Franz-Stefan Höger, MD (Hospital LSF, Graz, local site investigator); Julia Ferrari, MD (Hospital St. John of God Vienna, local site investigator); Marek Sykora (Hospital St. John of God Vienna, local site investigator); Wilfried Lang, MD (Hospital St. John of God Vienna, study coordinator); Nenad Mitrovic, MD (Hospital Vöcklabruck, local site investigator); Thomas Salletmayr, MD (Hospital Vöcklabruck, local site investigator); Monika Grunenberg, MD (Hospital Vöcklabruck, local site investigator); Hanspeter Haring, MD (Hospital Wagner-Jauregg, Linz, local site investigator); Nakajima Takeshi, MD (Hospital Waldviertel Horn, local site investigator); Alexandra Rieseneder, MD (Hospital Waldviertel Horn, local site investigator); Martin Gabler (Hospital Waldviertel Horn, local site investigator); Andreas Doppelbauer, MD (Hospital Weinviertel Mistelbach, local site investigator); Stefan Pingitzer, MD (Hospital Weinviertel Mistelbach, local site investigator); Manfred Eder; MD (Hospital Weinviertel Mistelbach, local site investigator); Peter Schnider, MD (Hospital Wiener Neustadt, local site investigator),Isabelle Csmarich, MD (Hospital Wiener Neustadt, local site investigator); Andrea Hager-Seifert,MD (Hospital Wiener Neustadt, local site investigator); Franz Fazekas, MD (Medical University,Graz, local site investigator); Kurt Niederkorn, MD (Medical University,Graz,study coordinator), Thomas Gattringer, MD (Medical University,Graz,local site investigator); Johann Willeit, MD (Medical University, Innsbruck, local site investigator); Michael Knoflach, MD (Medical University, Innsbruck, local site investigator); Stefan Kiechl, MD (Medical University, Innsbruck, local site investigator); Claude Alf, MD (Neurological Center Rosenhügel, Hospital Hietzing Vienna - 1st Dept. of Neurology, local site investigator); Georg Dimitriadis, MD (Neurological Center Rosenhügel, Hospital Hietzing Vienna - 1st Dept. of Neurology, local site investigator); Manfred Schmidbauer, MD (Neurological Center Rosenhügel, Hospital Hietzing Vienna - 1st Dept. of Neurology, local site investigator); Elsa Fröschl, MD (Neurological Center Rosenhügel, Hospital Hietzing Vienna - 2nd Dept. of Neurology, local site investigator); Christoph Baumgartner, MD (Neurological Center Rosenhügel, Hospital Hietzing Vienna - 2nd Dept. of Neurology, local site investigator); Judith Stanek, MD (Wilhelminen Hospital, Vienna, local site investigator); Gerhard Daniel, MD (Wilhelminen Hospital, Vienna, local site investigator) Silvia Parigger, MD (Wilhelminen Hospital, Vienna, local site investigator); Josef Grossmann, MD (Hospital Lienz, local site investigator); Martin Kosco, MD (Hospital Lienz, local site investigator); Robert Perfler, MD (Hospital Lienz, local site investigator); Sylvia Promisch, MD (Hospital LKH Villach, local site investigator); Peter Kapeller, MD (Hospital LKH Villach, local site investigator); Magret Niederkorn-Duft, MD (Hospital LKH Knittelfeld,local site investigator); Philipp Werner, MD (LKH Feldkirch, local site investigator); Gesundheit Österreich GmbH/BIQG (M. Moritz, A. Gollmer,R. Kern, L. Seyfang), Steering Group at the GÖG/BIQG (Head: W. Lang)
Rights and permissions
About this article

Cite this article
Ferrari, J., Shiue, I., Seyfang, L. et al. Weather as physiologically equivalent was not associated with ischemic stroke onsets in Vienna, 2004–2010. Environ Sci Pollut Res 22, 8756–8762 (2015). https://doi.org/10.1007/s11356-015-4494-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-015-4494-7