
Abstract
The peak occurrence of Mycoplasma pneumoniae (M. pneumoniae) infections in childhood and haze episodes is concurrent. Together, the prevalence of macrolide-resistant M. pneumoniae varies among countries might also be related to the concentration of ambient fine particulate mass (aerodynamic diameter ≤2.5 μm, PM2.5). Numerous cohort studies have identified consistent associations between ambient PM2.5 and cardiorespiratory morbidity and mortality. PM2.5 is a carrier of the heavy metals. The relationship between PM2.5-associated metals and M. pneumoniae infections in childhood has been increasingly drawing public attention. First, we reviewed original articles and review papers in Pubmed and Web of Science regarding M. pneumoniae and PM2.5-associated metal and analyzed the structural basis of PM2.5-associated metal interaction with M. pneumoniae. Then, the possible mechanisms of action between them were conjectured. Mechanisms of oxidative stress induction and modulation of the host immune system and inflammatory responses via Toll-like receptors (TLRs) and/or the nuclear factor-kappa B (NF-κB) pathway are postulated to be the result of PM2.5-associated metal complex interaction with M. pneumoniae. In addition, a heavy metal effect on M. pneumoniae-expressed community-acquired respiratory distress syndrome (CARDS) toxin, and activation of the aryl hydrocarbon receptor (AhR) and TLRs to induce the differentiation of T helper (Th) cells are also regarded as important reasons for the influence of the heavy metals on the severity of M. pneumoniae pneumonia and the initial onset and exacerbation of M. pneumoniae associated asthma. PM2.5-associated metals via complex mechanisms can exert a great impact on the host through interaction with M. pneumoniae.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Mycoplasma pneumoniae (M. pneumoniae) infection is the dominant cause of pneumonia in childhood (Chiang et al. 2007; Atkinson et al. 2008; He et al. 2013). Although it has been nearly 70 years since M. pneumoniae was first isolated in tissue culture from the sputum of a patient with primary atypical pneumonia, the pathogenesis of M. pneumoniae infection is still not fully clear. This organism causes a variety of clinical presentations from self-limiting to life-threatening, from pulmonary to extrapulmonary, and can even cause community outbreaks similar to influenza. Macrolides are commonly recommended for treatment of microbiologically defined M. pneumoniae infection. However, there is a major concern that macrolide-resistant M. pneumoniae have increased locally and is spreading throughout the world. In East Asia, macrolide-resistant M. pneumoniae rapidly increases and will become the cause of the majority of clinically proven M. pneumoniae in both children and adults. For example, over 90 % of isolated M. pneumoniae in China is macrolide resistant, while no macrolide-resistent M. pneumoniae is found in the Netherlands. Generally, it becomes highly prevalent in East Asian countries including China, Japan, and South Korea, while being a medium or low prevalent M. pneumoniae in North America and Europe, respectively. Macrolide-resistant M. pneumoniae is reportedly more prevalent in children, and the predominant point mutation found is A2063G in domain V of 23S rRNA. The prevalence of macrolide-resistant M. pneumoniae varies among countries and age groups (Table 1) (Averbuch et al. 2011; Akaike et al. 2012; Miyashita et al. 2012; Spuesens et al. 2012; Uldum et al. 2012; Yamada et al. 2012; Yoo et al. 2012; Dumke et al. 2013; Eshaghi et al. 2013; Pereyre et al. 2013; Wu et al. 2013; Zhao et al. 2013; Saraya et al. 2014).
The reasons for the regional differences in macrolide-resistant M. pneumoniae have not been elucidated. In our opinion, this might be related to the concentration of ambient fine particulate mass (aerodynamic diameter ≤2.5 μm; PM2.5). For example, the rural background concentrations of PM2.5 in Europe seem to be in general quite uniform at between 11 and 13 μg/m3, and considerably lower than urban background levels (around 15–20 μg/m3), which in turn are lower than PM2.5 annual averages at traffic sites (typical range 20–30 μg/m3) (data before 2005) (WHO 2006). According to the relevant literatures: Munich and Wesel (Germen) October 2008 to November 2009, Augsburg (Germany) 2011–2012, Dresden (Germany) 2011–2012, Ljubljana (Slovenia) 2012–2013, and Prague (Czech Republic) 2012–2013, the mean and standard deviation of the air pollutants for PM2.5 were 14.8 ± 2.2, 14.9 ± 9.8, 16.2 ± 13.8, 20.7 ± 14.3, and 16.2 ± 11.6 μg/m3, respectively (Liu et al. 2015; Lanzinger et al. 2015). The average PM2.5 concentrations in the USA were 12.5 μg/m3 in 2002, with 90 % of the sites having PM2.5 levels <16 μg/m3 (WHO 2006). During August 2000 to February 2004, daily PM2.5 levels in Connecticut/Massachusetts region (USA) averaged 14.0 μg/m3 (Bell et al. 2014). The mean and standard deviation of the acute (2-day moving average) PM2.5 and the chronic (1-year exposure) PM2.5 across the North East USA for 2000–2009 were 11.1 ± 6.8 and 12.9 ± 2.2 μg/m3, respectively (Kloog et al. 2015). However, fine particles are responsible for most visibility problems in Asia. Measurements in the center of Beijing show PM2.5 concentrations averaging just over 100 μg/m3. The monthly average concentrations varied between 61 and 139 μg/m3. During air pollution episodes, daily mean PM2.5 values can reach 300 μg/m3 (WHO 2006; Liang et al. 2014). Especially, the monitor showed the concentration of PM2.5 got to amazing 886 μg/m3 in 2013 (Yu et al. 2013).
Together, although M. pneumoniae is endemic throughout the year, the peak occurrence of these illnesses is in fall and winter (Foy 1993; Layani-Milon et al. 1999). Notably, haze episodes always appear concurrently. Numerous cohort studies have identified consistent associations between ambient PM2.5 and cardiorespiratory morbidity and mortality (WHO 2013; Alessandria et al. 2014; Cakmak et al. 2014; Sarnat et al. 2015; Traversi et al. 2015). PM2.5 is a carrier of the heavy metals, it is established that exposure to heavy metals is associated with lower lung function and higher prevalence of respiratory symptoms and diseases in local residents, especially children (Zheng et al. 2013, 2016; Zeng et al. 2016). From the data difference of the concentration of PM2.5-associated metals in Europe, North America, and China (Table 2) (Duan and Tan 2013; Cakmak et al. 2014; Fuertes et al. 2014), which is a surprising positive correlation with regional differences in macrolide-resistant M. pneumoniae. We speculate that PM2.5-associated metals play important role during child M. pneumoniae infections. In this review, we focus on the interaction of M. pneumoniae with 11 common PM2.5-associated metals, including iron (Fe), copper (Cu), chromium (Cr), vanadium (V), cadmium (Cd), arsenic (As) (although As is not a heavy metal, considering its health effect, it is discussed as a heavy metal (oid) in the context), lead (Pb), nickel (Ni), mercury (Hg), zinc (Zn), and manganese (Mn), and discuss the possible mechanisms of action.
Methods
The structural basis of PM2.5-associated metal interaction with M. pneumoniae
M. pneumoniae is a unique organism that lacks a cell wall. It attaches to ciliated respiratory epithelial cells at the base of the epithelia by interactive adhesins and accessory proteins clustered at the tip of the organelle. Specifically, M. pneumoniae attaches to the bronchial epithelial cells via P1 adhesin, P30, and other structures (high-molecular-weight protein 1 (HMW1), HMW2, HMW4, HMW5, P90, and P65). Cytadherence of M. pneumoniae in the respiratory tract is the initial event in infection. The infection process is associated with the release of a soluble hemolysin, hydrogen peroxide (H2O2), superoxide radicals (O2−•) and the pertussis-like community-acquired respiratory distress syndrome (CARDS) toxin which results in interference with the integrity of the respiratory epithelium. The surface-associated pyruvate dehydrogenase (PDH) subunits might also play a role by interaction with human plasminogen (Saraya et al. 2014; Gründel et al. 2015). Furthermore, because mycoplasmas lack cell walls, they do not contain known pathogen-associated molecular patterns (PAMPs) such as those corresponding to lipopolysaccharide (LPS), peptidoglycan (PGN), or lipoteichoic acid. These findings suggested that lipoproteins are key factors of M. pneumoniae-induced inflammatory responses and facilitate the development of pneumonia in humans (Shimizu et al. 2014). Pattern recognition receptors (PRR) are essential for innate immunity to invading pathogens. One of the best-characterized groups of PRR is the family of Toll-like receptors (TLRs). TLRs are expressed on many cell types, including professional antigen presenting cells (APCs), such as dendritic cells (DCs) and macrophages, as well as T cells, B cells, and airway epithelial cells, to recognize microorganisms and to induce innate immune responses and subsequent acquired immunity (Gururajan et al. 2007; Jin et al. 2012; Kawasaki and Kawai 2014). Among the reported TLR family members, TLR2, TLR4, TLR5, and TLR9 have been implicated in the recognition of different bacterial components. In particular, lipoprotein from various microorganisms is recognized by TLR2. These TLR family members have been also shown to activate nuclear factor-kappa B (NF-κB) via interleukin-1R (IL-1R)-associated signal molecules, including myeloid differentiation protein (MyD88), interleukin-1 receptor-activated kinase (IRAK), tumor necrosis factor (TNF) receptor-associated factor 6 (TRAF6), and NF-κB-inducing kinase (NIK) (Shimizu et al. 2014). It is well known that NF-κB induces transcription of a number of important genes. Many of the NF-κB-targeted genes are pivotal in mediating cell-to-cell interaction, intercellular communication, cell recruitment or transmigration, amplification or spreading of primary pathogenic signals, and initiation or acceleration of carcinogenesis (Chen and Shi 2002). Therefore, cytadherence of invading mycoplasmas to the respiratory epithelium, localized host cell injury, and overaggressive inappropriate immune responses appear to contribute to the pathogenesis of M. pneumoniae infection (Shimizu et al. 2014). PM2.5 has increasingly been shown to be more harmful to human health than larger particles, since the smaller particles have more potential to be deposited in the respiratory bronchioles, the alveoli and even penetrate the blood-gas barrier as a result of greater penetration (Gao et al. 2015). The respiratory tract provides necessary and sufficient conditions for PM2.5-associated metal interactions with resident M. pneumoniae. Compared to adults, children are a demographic of special concern, as they represent a population at increased risk for air pollution–related respiratory conditions because of their biologic characteristics (e.g., immature lungs and immune system, higher breathing rates) and behavior (e.g., more time spent outdoors) (Ostro et al. 2009). So PM2.5-associated metal interaction with M. pneumoniae can exert a greater impact on them.
Strategy, criteria, and procedures for the literature search
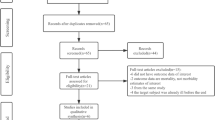
A systematic literature search was performed in Pubmed and ScienceDirect data base platforms. The search was extended to the last two decades (from August 1993 to June 2015). Indexing terms used for searching were M. pneumoniae and PM2.5-associated metals, including Fe, Cu, Cr, V, Cd, As, Pb, Ni, Hg, Zn, and Mn. We focused on the possible mechanisms of action between them. Inclusion criteria included the following: (1) M. pneumoniae produces a soluble hemolysin, H2O2 and O2 −•, which produce oxidative stress in the respiratory epithelium (Saraya et al. 2014). Correspondingly, the literatures involve in “metal” and “oxidative stress”. (2) M. pneumoniae modulates the host immune system and inflammatory responses via TLRs and/or the NF-κB pathway. Relatively, the studies relate to “metal”, “TLR”, and/or “NF-κB”. (3) M. pneumoniae synthesizes the pertussis-like CARDS toxin. The C-terminal domain of CARDS toxin interacts with the host protein annexin A2 (AnxA2), a member of the annexin family of proteins that is comprised of divalent calcium [Ca(II)]- and phospholipid-binding proteins (Somarajan et al. 2014). Comparatively, the reports refer to “metal”, “Ca(II) homeostasis”, and/or “Ca(II)-binding proteins”. (4) The differentiation of T helper (Th) cells could impact the severity of M. pneumoniae pneumonia and the initial onset and exacerbation of M. pneumoniae associated asthma (Wu et al. 2008; Saraya et al. 2014; Huang et al. 2015). Parallelly, the articles touch on “metal”, “Th”, “AhR”, and/or “TLR”. The rest were excluded.
Results and discussion
Through data analysis and synthesis of results above, we conjecture the possible mechanisms as follows:
-
(1)
Induction of oxidative stress
M. pneumoniae produces a soluble hemolysin, H2O2 and O2 −•, which produce oxidative stress in the respiratory epithelium, resulting in both structural and functional deterioration of cilia (Saraya et al. 2014).
Oxidative stress is also thought to be an important mechanism through which particulate air pollution contributes to adverse health effects. The metal content of PM2.5 is a logical candidate in exploring specific components that contribute to cardiorespiratory morbidity (Cakmak et al. 2014). Generally, heavy metals can induce oxidative stress by increasing the production of reactive oxygen species (ROS) and depletion of antioxidant reserves (Chen et al. 2011). Detailed studies in the past two decades have shown that redox-active metals such as Fe, Cu, Cr, V, cobalt (Co), titanium (Ti), and other metals undergo redox cycling reactions and possess the ability to produce reactive radicals such as O2 −• and nitric oxide (NO•) in biological systems. Disruption of such metal ion homeostasis may involve formation of the O2 −•, hydroxyl radical (OH•) (mainly via Fenton reaction) and other ROS. On the other hand, redox inactive metals, such as Cd, As, Pb, Ni, and Hg, exert their toxic effects via bonding to sulfhydryl groups in proteins and depletion of glutathione (Valko et al 2005; Ani et al. 2007; Jomova and Valko 2011). Interestingly, for As, the oxidation of trivalent arsenic [As(III)] to pentavalent arsenic [As(V)], under physiological conditions, also results in the formation of H2O2 (a source of damaging OH•) (Jomova and Valko 2011). Other redox inactive metals, such as Cd, are unable to generate free radicals directly. However, indirect formation of ROS and reactive nitrogen species (RNS), involving O2 −•, OH•, and NO•, has been reported (Waisberg et al 2003). An interesting mechanism explaining the indirect role of Cd in free radical generation was presented, in which it was proposed that Cd can replace Fe and Cu in various cytoplasmic and membrane proteins (e.g., ferritin, apoferritin), thus increasing the amount of unbound free or poorly chelated Cu and Fe ions participating in oxidative stress via Fenton reactions (Price and Joshi 1983). Most intriguingly, Zn is generally regarded as a redox inert metal and does not participate in oxidation-reduction reactions. Zn’s function as an antioxidant involves two different mechanisms: (i) the protection of sulfhydryl groups of proteins against free radical attack and (ii) reduction of free radical formation through prevention mechanisms involving antagonism of redox-active transition metals, such as Fe and Cu (Bray and Bettger 1990). Together, divalent zinc [Zn(II)] is also an important co-factor of superoxide dismutase (SOD), which plays an important role in the degradation of pro-inflammatory ROS (Stafford et al. 2013). However, despite the fact that Zn is an essential nutrient and vital to many physiological processes, exposure of human airway epithelial cells (HAECs) to Zn(II) leads to multiple oxidative effects that are exerted through H2O2-dependent and -independent mechanisms (Wages et al. 2014). Like Zn, Mn is an essential element. It actively participates in important enzymatic reactions for cellular function. As a SOD metal co-factor, Mn ion also involves catalytic conversion of O2 −• and H2O2. Nevertheless, continuous exposure to high concentrations of this metal, mainly through inhalation, may produce alterations in the central nervous system (Riojas-Rodríguez et al. 2010; Kim et al. 2014). It is feasible that manganese can generate oxidative products when exposed within the cell to potential oxidizing agents, such as dopamine or Fe. This could be a mechanism for manganese neurotoxicity (Zheng et al. 2013). In addition, with respect to the particular species, metal oxides are substances traditionally considered to be relatively inert chemically, but despite this, in very small (ultrafine) size ranges, these particles have been linked with significant oxidative stress-mediated toxicity. Some metals, such as Zn oxide, will dissolve in the body (Cassee et al. 2013). Notably, phagocytosis-induced ROS is an immediate response occurring within the first 30 min of particle uptake, whereas TLR signaling promotes a slower accumulation of ROS, which is derived from the mitochondria (Stafford et al. 2013). Furthermore, aryl hydrocarbon receptor (AhR) ligands have been shown to increase ROS production, perhaps as the consequence of increased expression of AhR target genes, cytochrome P4501A1 (CYP1A1), and a member of the membrane nicotinamide adenine dinucleotide phosphate (NADPH) oxidase complex, p40phox, while divalent cadmium [Cd(II)], As(III), hexavalent chromium [Cr(VI)], and divalent lead [Pb(II)] can interact with the metal ligation function of the AhR (Hemdan et al. 2013; Huang et al. 2015).
Therefore, PM2.5-associated metals can increase production of ROS and deplete of antioxidant reserves by multiple pathways. The overwhelming of body antioxidant mechanisms by increased ROS production may lead to oxidative stress and subsequently induce DNA damage, lipid peroxidation, protein modification, and other effects, all symptomatic of numerous diseases involving cancer, cardiovascular disease, diabetes, atherosclerosis, neurological disorders (Alzheimer’s disease, Parkinson’s disease), chronic inflammation, and others (Jomova and Valko 2011).
In a word, the PM2.5-associated metals and M. pneumoniae could produce synergistic effects for oxidative stress induction.
-
(2)
Modulation of the host immune system and inflammatory responses via TLRs and/or the NF-κB pathway
Lipoproteins from various Mycoplasma species have potent inflammatory properties. Three lipoproteins/lipopeptides of M. pneumoniae origin, macrophage-activating lipopeptide-2 (MALP-2), P48, and M161Ag (identical to MALP-404), reportedly modulate the host immune system via TLR2/TLR6 signaling. Shimizu et al. reported that the mycoplasma-derived lipoproteins NF-κB-activating lipoprotein 1 (N-ALP1)/N-ALP2 and F0F1-ATPase activate NF-κB via TLR1, 2 and TLR1, 2, 6 signaling, respectively. Stimulation of these TLRs has been shown to produce chemokines that promote lymphocyte and neutrophil trafficking and inflammation in the lung (Saraya et al. 2014). Shimizu et al. (2014) reported cytadherence of M. pneumoniae induces inflammatory responses through TLR4 and autophagy. Saraya et al. (2014) also demonstrated that the severity of the M. pneumoniae pneumonia depends on host innate immunity to M. pneumoniae, which might be accelerated by antecedent M. pneumoniae exposure (re-exposure or latent respiratory infection) through upregulation of TLR2 expression on bronchial epithelial cells and alveolar macrophages.
Meanwhile, in mice, instillation of PM2.5, in a dose-dependent manner, induces a Th1/Th2 cells shift in inflammatory responses and upregulates TLR2 and TLR4 on alveolar macrophages (Zhao et al. 2012). ROS also stimulate TLR2 and TLR4 through MyD88-dependent pathways, inducing cellular damage and elevated levels of damage-associated molecular patterns (DAMPs) (Hansel and Barnes 2009). Dagher et al. (2007) reported that the transition metals (i.e., Fe, aluminum (Al), Pb, Mn, Zn) and organic compounds (i.e., volatile organic compounds (VOC), polycyclic aromatic hydrocarbons (PAH)) present in PM2.5 can be involved in the induction of several physiopathological processes (i.e., oxidative stress, gene expression, and protein secretion of inflammatory mediators and apoptotic events) through activation of the NF-κB/inhibitory kappa B (IκB) complex in lung target cells. The metal content of PM2.5 is also regarded as a logical target in exploring these effects. Metal ions can activate TLR signaling similar to bacteria-derived PAMPs. Likewise, metal ions can function as haptens activating the adaptive immune system similar to bacterial derived antigens (Pajarinen et al. 2014). Schmidt et al. (2010) reported that divalent nickel [Ni(II)] triggers an inflammatory response by directly activating human TLR4. Ni(II)-induced TLR4 activation is species-specific; studies with mutant TLR4 proteins revealed that the non-conserved histidines 456 and 458 of human TLR4 are required for activation by Ni(II). Balbi et al. (2014) reported that in mussels (at least 15 mussels in quadruplicate for each condition) exposed for 96 h to either nanosized titanium dioxide (n-TiO2) (100 μg/L nominal concentration levels, corresponding to 60 μg/L Ti on a mass basis), or Cd(II) (100 μg/L) and to both n-TiO2 and Cd(II) at the same concentrations, neither contaminant alone affected mRNA levels for the toll-like receptor isoform (TLR-i), whereas a dramatic decrease was observed with the mixture (−80 % with respect to controls). A much more substantial literature has documented effects of Zn on signaling and inflammatory output in immune cells. Such effects are likely to be an important component of Zn-mediated host defense. Zn regulates inflammatory gene expression through multiple pathways, including protein tyrosine phosphorylation, mitogen-activated protein kinases (MAPKs), protein kinase C (PKC), phosphodiesterases (PDEs), and NF-κB, many of which lie downstream of TLRs. A reoccurring theme in Zn signaling is that Zn concentrations are critical; while low concentrations may be required for the activation of a specific pro-inflammatory signaling pathway, high concentrations can suppress the same pathway (Stafford et al. 2013). Following 10 weeks of exposure to Hg via drinking water, Assefa et al. (2012) found that Hg exposure significantly enhances the expression of TLR4 and activates p38 MAPK and NF-κB pathways in vole livers. Zelnikar et al. (2014) demonstrated that V potentiates TLR4 activity by increasing hepatocyte growth factor-regulated tyrosine kinase substrate (Hrs) phosphorylation status, reducing the size of Hrs/TLR4-positive endosomes and impacting TLR4 degradation, thus contributing to the detrimental effects of air pollutants on human health.
Accumulating evidence suggests that many metals are able to affect the activation or activity of the NF-κB transcription factor. To date, the results are not straightforward. Both activation and inhibition of NF-κB by metals have been reported. In the human bronchial epithelial cell line BEAS-2B, Chen et al. observed that the activation of NF-κB by As(III) occurred in a very narrow dose range. A 5- to 6-fold induction of NF-κB-dependent reporter gene activity was observed by As(III) at concentrations of 6–12 μM. In contrast, a substantial inhibition of NF-κB by As(III) was observed at concentrations higher than 25 μM. Obviously, at physiologically relevant dose ranges, As(III) is not an inhibitor but rather an activator for NF-κB. In airway epithelial cells, studies by Jaspers et al. indicated that As(III) activated NF-κB through an alternative mechanism that did not require the inducible degradation of IκBα and the nuclear translocation of NF-κB proteins. Mechanistic studies, using wild-type and sek1 [stress-activated protein kinase (SAPK)/extracellular-signal-regulated kinase (ERK) kinase] gene knockout mouse embryo stem cells, suggested that As(III)-mediated activation of NF-κB occurs through a signaling pathway that involves SEK1 (MKK4)-c-Jun N-terminal kinase (JNK). Neither ERK nor p38 is required for As(III)-induced NF-κB activation. In contrast to these studies, several reports suggest that As(III) inhibits NF-κB by either interfering with DNA binding of NF-κB or directly inactivating IκB kinase (IKK). Pentavalent vanadium [V(V)] activates NF-κB in virtually all types of cells. Studies by Schieven et al. indicated that the activation of NF-κB by V(V) might be tyrosine kinase-dependent. Studies by Imbert et al. indicated that the activation of NF-κB by V(V) occurs independently of IκBα degradation. However, several other studies suggest that V(V) does induce degradation of IκBα after the phosphorylation of serine or tyrosine. Cr(VI) is able to activate NF-κB at lower concentrations (<50 μM) in T cells, macrophages, and bronchial epithelial cells. The final concentration of Cr(VI) is critical for this metal to induce or inhibit NF-κB. The inhibitory effect of Cr(VI) at higher concentrations (>50 mM) on NF-κB may be due to cytotoxic effects on cells or interference with the DNA binding activity of NF-κB. Chen et al. demonstrated that Cr(VI) activated NF-κB at 5–10 μM in human bronchial epithelial cells cultured at a relatively high cell density, possibly through activating IKK. Chen et al. further showed that activation of NF-κB protects cells from Cr(VI)-induced cytotoxicity (Chen and Shi 2002). Many of Pb’s effects on the immune system might be explained through activation of the transcription factor, NF-κB. It was shown that Pb at physiologically relevant concentrations activates NF-κB in primary human CD4+ T lymphocytes. Pb-induced activation of NF-κB is blocked by antibodies for p65 and p50 subunits, but not by cRel, indicating that the p65:p50 heterodimer (NF-κB) is involved (Kudrin 2000). Chen et al. (2014) reported high levels (20 or 30 μM) of Cd exposure on normal human bronchial BEAS-2B cells can significantly upregulate the protein levels of eukaryotic translation initiation factor 5A1 (eIF5A1) and redox-sensitive transcription factor NF-κB p65. Moreno et al. (2008) reported direct stimulation of cyclic guanosine monophosphate (cGMP) synthesis and activation of mitogen-activated protein (MAP) kinase signaling pathways underlies the capacity of Mn to augment NF-κB-dependent gene expression in astrocytes. Shionome et al. (2013) reported Ni(II) ions can reduce NF-κB activity. The inhibitory effect of Ni(II) ions is attributed to the prevention of p50 subunit accumulation to the nucleus. The direct requirement for Zn in activating NF-κB has been demonstrated in T cells. However, an extensive literature has also documented inhibitory effects of Zn on NF-κB activation, both in vitro and in vivo. In the latter case, this also correlated with reduced TNF expression and liver injury, an effect that was metallothionein (MT)-independent. Others have also reported that Zn exerts protective effects in vivo by limiting NF-κB activation during innate immune responses. Multiple mechanisms of NF-κB inhibition have been identified. Direct inhibition of IKKβ by Zn has been reported, while others have also shown that Zn indirectly inhibits IKKβ via cGMP-dependent activation of protein kinase A (PKA) (Stafford et al. 2013). Kenneth et al. (2014) demonstrated that elevated Cu is a general inhibitor of NF-κB activity induced by multiple stimuli, with both canonical and non-canonical NF-κB blocked by excess Cu levels.
Furthermore, heavy metals can also modulate NF-κB by ROS. General, ROS seem to play a dual role in participating NF-κB activation cascade. On one hand, a number of reports suggest that NF-κB can be activated by a variety of ROS that causes oxidative stress. It has been realized for decades that oxidative stress is the major effect of toxic metals on cellular events (Chen and Shi 2002). Gius et al. (1999) summarize the available research evidences suggest that ROS act as a common second messenger following cellular exposure to agents that induce NF-κB activation. However, Kenneth et al. (2014) demonstrated elevated intracellular Cu blocks NF-κB gene transcription by increasing the production of intracellular ROS that results in the inhibition of IKK-dependent phosphorylation of IκBα.
In sum, both M. pneumoniae and heavy metals could modulate the host immune system and inflammatory response via TLRs and/or the NF-κB pathway.
-
(3)
Impact of the heavy metals on CARDS toxin
M. pneumoniae synthesizes an ADP-ribosyltransferase, similar to pertussis toxin, known as the CARDS toxin, which binds to surfactant protein A and enters host cells by clathrin-mediated endocytosis. CARDS toxin produces ciliostasis and nuclear fragmentation, and stimulates production of proinflammatory cytokines to cause an acute cellular inflammatory reaction, leading to airway damage (Atkinson and Waites 2014). Somarajan et al. (2014) recently showed that the C-terminal domain of CARDS toxin interacts with the host protein AnxA2, a member of the annexin family of proteins that is comprised of Ca(II)- and phospholipid-binding proteins that exhibit many signaling functions. The interaction between CARDS toxin and AnxA2 likely plays an important role in the observed localized and disseminated inflammation and tissue pathologies associated with M. pneumoniae infections. Exposure to the heavy metals Cd(II), Pb(II), or methylmercury (MeHg) results in neurotoxicity in both humans and laboratory animals, while developing organisms are generally more susceptible than adults to the neurotoxic effects of these metals. The mechanisms of neurotoxicity of these metals have not been elucidated. However, each of these metals disrupts neuronal function by altering the function of multiple cellular proteins and Ca(II) homeostatic mechanisms (Shafer 1998). Furthermore, intake of Cd and Pb modulates the activity or deregulates the expression of Ca(II)-binding proteins (Zhang et al. 2011). In addition, it is well established that accumulation of ROS lead to cytosolic Ca overload (Temsah et al. 1999; Gen et al. 2001; Viste et al. 2005; Song et al. 2006; Wagner et al. 2011). ROS can also impair the function of Ca-regulatory protein. The mechanisms, however, are incompletely understood but involve direct modification of target proteins (i.e., ion channels and transporters) and activation of serine/threonine kinases (i.e., cAMP-dependent protein kinase A (PKA), PKC, and Ca/calmodulin-dependent protein kinase II (CaMKII)) (Wagner et al. 2013). While oxidative stress induction is the major effect of the heavy metals contributes to negative health consequences, which we have sufficiently discussed above. Thus, PM2.5-associated metals might impact the effect of CARDS toxin on the host through regulating dynamic equilibrium of calcium ion.
-
(4)
Effect of the heavy metals via AhR and TLRs on the differentiation of Th cells
The AhR is a ligand-activated member of the Per-Arnt-Sim (PAS) family of basic helix-loop-helix (HLH) transcription factors. The AhR is activated in many immune cell types, including T cells, B cells, natural killer (NK) cells, macrophages, and DCs, as well as in epithelial cells, Langerhans cells, innate lymphoid cells, intraepithelial lymphocytes, and microglia. The AhR mediates cellular responses to toxins or its ligands (Nguyen et al. 2014). Through metal ligation of the AhR, heavy metal ions, such as Cd(II), As(III), Cr(VI), and Pb(II) can activate the AhR (Hemdan et al. 2013). The AhR plays an important role in the control of the adaptive immune response. In particular, Quintana and Sherr (2013) found that the AhR controls the differentiation and activity of specific T cell subpopulations, while the differentiation of Th cells could impact the severity of M. pneumoniae pneumonia and the initial onset and exacerbation of M. pneumoniae-associated asthma.
In mouse models for M. pneumoniae pneumonia, Saraya et al. found that enhanced host immune responses against M. pneumoniae antigen are required for persistent inflammation in the lung, as well as Th2 characteristics causing plasma cell infiltration into the peri-bronchovascular areas (PBVAs), but not Th1 characteristics. Th2 characteristics might be required to generate typical M. pneumoniae pneumonia, even in humans. Other studies also showed that the histopathological score of M. pneumoniae pneumonia is significantly higher in infected BALB/c mice (Th2 predominant) than in C57BL/6 mice (Th1 predominant) through the late phase, suggesting differences in host reactions against intranasally inoculated live M. pneumoniae. Tanaka et al. described the different pathological findings in a Mycoplasma pulmonis (M. pulmonis)-infected mouse model involving treatment with IL-2 (Th1 upregulated) vs. cyclosporine A (Th1 downregulated). So the severity of M. pneumoniae pneumonia seems to depend on polarization toward Th1 or Th2 predominance (Saraya et al. 2014). In addition, M. pneumoniae has been recognized as a contributing factor in both stable asthma and asthma exacerbations (Wu et al. 2008). Asthma is a phenotypically heterogeneous chronic disease of the airways, characterized by either predominant eosinophilic or neutrophilic, or even mixed eosinophilic/neutrophilic inflammatory patterns. Eosinophilic inflammation can be associated with the whole spectrum of asthma severity, ranging from mild-to-moderate to severe uncontrolled disease, whereas neutrophilic inflammation occurs mostly in more severe asthma. Eosinophilic asthma includes either allergic or nonallergic phenotypes underlying immune responses mediated by Th2 cell-derived cytokines, while neutrophilic asthma is mostly dependent on Th17 cell-induced mechanisms. These immune-inflammatory profiles develop as a consequence of a functional impairment of T regulatory (Treg) lymphocytes, which promotes the activation of DCs directing the differentiation of distinct Th cell subsets (Pelaia et al. 2015).
At the same time, AhR and TLR signaling intersect and cross-regulate each other. TLR activation upregulates AhR expression, and AhR acts as a negative regulator of TLR signaling (Quintana and Sherr 2013). Traditionally, activation of TLRs in APCs will lead to the production of IFN-α, proinflammatory cytokines, such as TNF-α, IL-1 and IL-6, and the cytokines IL-12 and IL-18, which instruct Th1 to differentiate, whereas an increased Th2 response is observed in MyD88-deficient mice with impaired TLR signaling. The IL-12 and IL-23 secretions of DCs induced by TLR activation are enhanced by the chemokine CCL17 in an autocrine manner. Production of these cytokines is significantly reduced in CCL17-deficient DCs. Activation of TLR4 results in a MyD88-dependent Th17 response in memory CD4+ T cells in the absence of TIR domain-containing adaptor inducing interferon-β (TRIF). Activation of DCs via TLR2-MyD88 also induces Th1 and Th17 cell differentiation. Still, signaling of TLR2 can inhibit DCs to produce IL-12p70 by dampening the type 1 IFN amplification loop. This signaling also drives the immune response induced by synergistic combination of TLR4 and TLR7/8 agonists (both are potent inducers of Th1 responses) toward Th2 and Th17 responses in naive and memory T cell subpopulations (Jin et al. 2012). So TLRs could give rise to the AhR-like effect by these mechanisms.
Conclusions
Metal ions are essential life elements that regulate numerous biological and biochemical functions to every living cell. However, overwhelming exposure to heavy metals in a variety of environmental settings is highly toxic to eukaryotic cells (Chen and Shi 2002). Particularly in regard to children with M. pneumoniae infections, based on the discussion above, PM2.5-associated metals via complex mechanisms can exert a great impact on the host through interaction with M. pneumoniae, which might be an important reason that the peak occurrence of M. pneumoniae infections in childhood and haze episodes are concurrent. Together, which might also be account for the prevalence of macrolide-resistant M. pneumoniae varies among countries. In view of this, it is necessary to increase public awareness about the effects of exposure to inhalational toxic heavy metals and arouse local government interest in public health and safety, so that a more comprehensive National Ambient Air Quality Standard (NAAQS) can be established. More important, reduction of the heavy metal loading might employ the treatment of M. pneumoniae infection in childhood more effectively.
References
Akaike H, Miyashita N, Kubo M, Kawai Y, Tanaka T, Ogita S, Kawasaki K, Nakano T, Terada K, Ouchi K, Atypical Pathogen Study Group (2012) In vitro activities of 11 antimicrobial agents against macrolide-resistant Mycoplasma pneumoniae isolates from pediatric patients: results from a multicenter surveillance study. Jpn J Infect Dis 65:535–538
Alessandria L, Schilirò T, Degan R, Traversi D, Gilli G (2014) Cytotoxic response in human lung epithelial cells and ion characteristics of urban-air particles from Torino, a northern Italian city. Environ Sci Pollut Res Int 21:5554–5564
Ani M, Moshtaghie AA, Ahmadvand H (2007) Comparative effects of copper, iron, vanadium and titanium on low density lipoprotein oxidation in vitro. Iran Biomed J 11:113–118
Assefa S, Curtis JT, Sethi S, Davis RL, Chen Y, Kaul R (2012) Inorganic mercury exposure in prairie voles (Microtus ochrogaster) alters the expression of toll-like receptor 4 and activates inflammatory pathways in the liver in a sex-specific manner. Hum Exp Toxicol 31:376–386
Atkinson TP, Waites KB (2014) Mycoplasma pneumoniae infections in childhood. Pediatr Infect Dis J 33:92–94
Atkinson TP, Balish MF, Waites KB (2008) Epidemiology, clinical manifestations, pathogenesis and laboratory detection of Mycoplasma pneumoniae infections. FEMS Microbiol Rev 32:956–973
Averbuch D, Hidalgo-Grass C, Moses AE, Engelhard D, Nir-Paz R (2011) Macrolide resistance in Mycoplasma pneumoniae, Israel, 2010. Emerg Infect Dis 17:1079–1082
Balbi T, Smerilli A, Fabbri R, Ciacci C, Montagna M, Grasselli E, Brunelli A, Pojana G, Marcomini A, Gallo G, Canesi L (2014) Co-exposure to n-TiO2 and Cd2+ results in interactive effects on biomarker responses but not in increased toxicity in the marine bivalve M. galloprovincialis. Sci Total Environ 493:355–364
Bell ML, Ebisu K, Leaderer BP, Gent JF, Lee HJ, Koutrakis P, Wang Y, Dominici F, Peng RD (2014) Associations of PM2.5 constituents and sources with hospital admissions: analysis of four counties in Connecticut and Massachusetts (USA) for persons ≥ 65 years of age. Environ Health Perspect 122:138–144
Bray TM, Bettger WJ (1990) The physiological role of zinc as an antioxidant. Free Radic Biol Med 8:281–291
Cakmak S, Dales R, Kauri LM, Mahmud M, Van Ryswyk K, Vanos J, Liu L, Kumarathasan P, Thomson E, Vincent R, Weichenthal S (2014) Metal composition of fine particulate air pollution and acute changes in cardiorespiratory physiology. Environ Pollut 189:208–214
Cassee FR, Héroux ME, Gerlofs-Nijland ME, Kelly FJ (2013) Particulate matter beyond mass: recent health evidence on the role of fractions, chemical constituents and sources of emission. Inhal Toxicol 25:802–812
Chen F, Shi X (2002) Signaling from toxic metals to NF-kappaB and beyond: not just a matter of reactive oxygen species. Environ Health Perspect 110(Suppl 5):807–811
Chen A, Dietrich KN, Huo X, Ho SM (2011) Developmental neurotoxicants in e-waste: an emerging health concern. Environ Health Perspect 119:431–438
Chen DJ, Xu YM, Du JY, Huang DY, Lau AT (2014) Cadmium induces cytotoxicity in human bronchial epithelial cells through upregulation of eIF5A1 and NF-kappaB. Biochem Biophys Res Commun 445:95–99
Chiang WC, Teoh OH, Chong CY, Goh A, Tang JP, Chay OM (2007) Epidemiology, clinical characteristics and antimicrobial resistance patterns of community-acquired pneumonia in 1702 hospitalized children in Singapore. Respirology 12:254–261
Dagher Z, Garcon G, Billet S, Verdin A, Ledoux F, Courcot D, Aboukais A, Shirali P (2007) Role of nuclear factor-kappa B activation in the adverse effects induced by air pollution particulate matter (PM2.5) in human epithelial lung cells (L132) in culture. J Appl Toxicol 27:284–290
Duan J, Tan J (2013) Atmospheric heavy metals and arsenic in China: situation, sources and control policies. Atmos Environ 74:93–101
Dumke R, Lück C, Jacobs E (2013) Low rate of macrolide resistance in Mycoplasma pneumoniae strains in Germany between 2009 and 2012. Antimicrob Agents Chemother 57:3460
Eshaghi A, Memari N, Tang P, Olsha R, Farrell DJ, Low DE, Gubbay JB, Patel SN (2013) Macrolide-resistant Mycoplasma pneumoniae in humans, Ontario, Canada, 2010–2011. Emerg Infect Dis 19:1525–1527
Foy HM (1993) Infections caused by Mycoplasma pneumoniae and possible carrier state in different populations of patients. Clin Infect Dis 17(Suppl 1):S37–S46
Fuertes E, MacIntyre E, Agius R, Beelen R, Brunekreef B, Bucci S, Cesaroni G, Cirach M, Cyrys J, Forastiere F, Gehring U, Gruzieva O, Hoffmann B, Jedynska A, Keuken M, Klümper C, Kooter I, Korek M, Krämer U, Mölter A, Nieuwenhuijsen M, Pershagen G, Porta D, Postma DS, Simpson A, Smit HA, Sugiri D, Sunyer J, Wang M, Heinrich J (2014) Associations between particulate matter elements and early-life pneumonia in seven birth cohorts: results from the ESCAPE and TRANSPHORM projects. Int J Hyg Environ Health 217:819–829
Gao Y, Guo X, Li C, Ding H, Tang L, Ji H (2015) Characteristics of PM2.5 in Miyun, the northeastern suburb of Beijing: chemical composition and evaluation of health risk. Environ Sci Pollut Res Int 19:19
Gen W, Tani M, Takeshita J, Ebihara Y, Tamaki K (2001) Mechanisms of Ca2+ overload induced by extracellular H2O2 in quiescent isolated rat cardiomyocytes. Basic Res Cardiol 96:623–629
Gius D, Botero A, Shah S, Curry HA (1999) Intracellular oxidation/reduction status in the regulation of transcription factors NF-kappaB and AP-1. Toxicol Lett 106:93–106
Gründel A, Friedrich K, Pfeiffer M, Jacobs E, Dumke R (2015) Subunits of the pyruvate dehydrogenase cluster of Mycoplasma pneumoniae are surface-displayed proteins that bind and activate human plasminogen. PLoS One 10:e0126600
Gururajan M, Jacob J, Pulendran B (2007) Toll-like receptor expression and responsiveness of distinct murine splenic and mucosal B-cell subsets. PLoS One 2:e863
Hansel TT, Barnes PJ (2009) New drugs for exacerbations of chronic obstructive pulmonary disease. Lancet 374:744–755
He XY, Wang XB, Zhang R, Yuan ZJ, Tan JJ, Peng B, Huang Y, Liu EM, Fu Z, Bao LM, Zou L (2013) Investigation of Mycoplasma pneumoniae infection in pediatric population from 12,025 cases with respiratory infection. Diagn Microbiol Infect Dis 75:22–27
Hemdan NY, Abu El-Saad AM, Sack U (2013) The role of T helper (TH)17 cells as a double-edged sword in the interplay of infection and autoimmunity with a focus on xenobiotic-induced immunomodulation. Clin Dev Immunol 2013:374769
Huang SK, Zhang Q, Qiu Z, Chung KF (2015) Mechanistic impact of outdoor air pollution on asthma and allergic diseases. J Thorac Dis 7:23–33
Jin B, Sun T, Yu XH, Yang YX, Yeo AE (2012) The effects of TLR activation on T-cell development and differentiation. Clin Dev Immunol 2012:836485
Jomova K, Valko M (2011) Advances in metal-induced oxidative stress and human disease. Toxicology 283:65–87
Kawasaki T, Kawai T (2014) Toll-like receptor signaling pathways. Front Immunol 5:461
Kenneth NS, Hucks GE Jr, Kocab AJ, McCollom AL, Duckett CS (2014) Copper is a potent inhibitor of both the canonical and non-canonical NF-kappaB pathways. Cell Cycle 13:1006–1014
Kim HM, Shin JH, Cho YB, Roe JH (2014) Inverse regulation of Fe- and Ni-containing SOD genes by a Fur family regulator Nur through small RNA processed from 3’UTR of the sodF mRNA. Nucleic Acids Res 42:2003–2014
Kloog I, Zanobetti A, Nordio F, Coull BA, Baccarelli AA, Schwartz J (2015) Effects of airborne fine particles (PM2.5) on deep vein thrombosis admissions in the northeastern United States. J Thromb Haemost 13:768–774
Kudrin AV (2000) Trace elements in regulation of NF-kappaB activity. J Trace Elem Med Biol 14:129–142
Lanzinger S, Schneider A, Breitner S, Stafoggia M, Erzen I, Dostal M, Pastorkova A, Bastian S, Cyrys J, Zscheppang A, Kolodnitska T, Peters A, UFIREG study group (2015) Associations between ultrafine and fine particles and mortality in five central European cities—results from the UFIREG study. Environ Int 88:44–52
Layani-Milon MP, Gras I, Valette M, Luciani J, Stagnara J, Aymard M, Lina B (1999) Incidence of upper respiratory tract Mycoplasma pneumoniae infections among outpatients in Rhone-Alpes, France, during five successive winter periods. J Clin Microbiol 37:1721–1726
Liang Y, Fang L, Pan H, Zhang K, Kan H, Brook JR, Sun Q (2014) PM2.5 in Beijing-temporal pattern and its association with influenza. Environ Health 13:102
Liu C, Fuertes E, Flexeder C, Hofbauer LC, Berdel D, Hoffmann B, Kratzsch J, von Berg A, Heinrich J, GINIplus Study Group, LISAplus Study Group (2015) Associations between ambient air pollution and bone turnover markers in 10-year old children: results from the GINIplus and LISAplus studies. Int J Hyg Environ Health 218:58–65
Miyashita N, Kawai Y, Akaike H, Ouchi K, Hayashi T, Kurihara T, Okimoto N, Atypical Pathogen Study Group (2012) Macrolide-resistant Mycoplasma pneumoniae in adolescents with community-acquired pneumonia. BMC Infect Dis 12:126
Moreno JA, Sullivan KA, Carbone DL, Hanneman WH, Tjalkens RB (2008) Manganese potentiates nuclear factor-kappaB-dependent expression of nitric oxide synthase 2 in astrocytes by activating soluble guanylate cyclase and extracellular responsive kinase signaling pathways. J Neurosci Res 86:2028–2038
Nguyen NT, Nakahama T, Le DH, Van Son L, Chu HH, Kishimoto T (2014) Aryl hydrocarbon receptor and kynurenine: recent advances in autoimmune disease research. Front Immunol 5:551
Ostro B, Roth L, Malig B, Marty M (2009) The effects of fine particle components on respiratory hospital admissions in children. Environ Health Perspect 117:475–480
Pajarinen J, Jamsen E, Konttinen YT, Goodman SB (2014) Innate immune reactions in septic and aseptic osteolysis around hip implants. J Long-Term Eff Med Implants 24:283–296
Pelaia G, Vatrella A, Busceti MT, Gallelli L, Calabrese C, Terracciano R, Maselli R (2015) Cellular mechanisms underlying eosinophilic and neutrophilic airway inflammation in asthma. Mediat Inflamm 2015:879783
Pereyre S, Touati A, Petitjean-Lecherbonnier J, Charron A, Vabret A, Bébéar C (2013) The increased incidence of Mycoplasma pneumoniae in France in 2011 was polyclonal, mainly involving M. pneumoniae type 1 strains. Clin Microbiol Infect 19:E212–E217
Price DJ, Joshi JG (1983) Ferritin. Binding of beryllium and other divalent metal ions. J Biol Chem 258:10873–10880
Quintana FJ, Sherr DH (2013) Aryl hydrocarbon receptor control of adaptive immunity. Pharmacol Rev 65:1148–1161
Riojas-Rodríguez H, Solís-Vivanco R, Schilmann A, Montes S, Rodríguez S, Ríos C, Rodríguez-Agudelo Y (2010) Intellectual function in Mexican children living in a mining area and environmentally exposed to manganese. Environ Health Perspect 118:1465–1470
Saraya T, Kurai D, Nakagaki K, Sasaki Y, Niwa S, Tsukagoshi H, Nunokawa H, Ohkuma K, Tsujimoto N, Hirao S, Wada H, Ishii H, Nakata K, Kimura H, Kozawa K, Takizawa H, Goto H (2014) Novel aspects on the pathogenesis of Mycoplasma pneumoniae pneumonia and therapeutic implications. Front Microbiol 5:410
Sarnat SE, Winquist A, Schauer JJ, Turner JR, Sarnat JA (2015) Fine particulate matter components and emergency department visits for cardiovascular and respiratory diseases in the St. Louis, Missouri-Illinois, Metropolitan Area. Environ Health Perspect 123:437–444
Schmidt M, Raghavan B, Müller V, Vogl T, Fejer G, Tchaptchet S, Keck S, Kalis C, Nielsen PJ, Galanos C, Roth J, Skerra A, Martin SF, Freudenberg MA, Goebeler M (2010) Crucial role for human Toll-like receptor 4 in the development of contact allergy to nickel. Nat Immunol 11:814–819
Shafer TJ (1998) Effects of Cd2+, Pb2+ and CH3Hg+ on high voltage-activated calcium currents in pheochromocytoma (PC12) cells: potency, reversibility, interactions with extracellular Ca2+ and mechanisms of block. Toxicol Lett 99:207–221
Shimizu T, Kimura Y, Kida Y, Kuwano K, Tachibana M, Hashino M, Watarai M (2014) Cytadherence of Mycoplasma pneumoniae induces inflammatory responses through autophagy and toll-like receptor 4. Infect Immun 82:3076–3086
Shionome T, Endo S, Omagari D, Asano M, Toyoma H, Ishigami T, Komiyama K (2013) Nickel ion inhibits nuclear factor-kappa B activity in human oral squamous cell carcinoma. PLoS One 8:e68257
Somarajan SR, Al-Asadi F, Ramasamy K, Pandranki L, Baseman JB, Kannan TR (2014) Annexin A2 mediates Mycoplasma pneumoniae community-acquired respiratory distress syndrome toxin binding to eukaryotic cells. MBio 5:e01497–14
Song Y, Shryock JC, Wagner S, Maier LS, Belardinelli L (2006) Blocking late sodium current reduces hydrogen peroxideinduced arrhythmogenic activity and contractile dysfunction. J Pharmacol Exp Ther 318:214–222
Spuesens EB, Meijer A, Bierschenk D, Hoogenboezem T, Donker GA, Hartwig NG, Koopmans MP, Vink C, van Rossum AM (2012) Macrolide resistance determination and molecular typing of Mycoplasma pneumoniae in respiratory specimens collected between 1997 and 2008 in the Netherlands. J Clin Microbiol 50:1999–2004
Stafford SL, Bokil NJ, Achard ME, Kapetanovic R, Schembri MA, McEwan AG, Sweet MJ (2013) Metal ions in macrophage antimicrobial pathways: emerging roles for zinc and copper. Biosci Rep 33:e00049
Temsah RM, Netticadan T, Chapman D, Takeda S, Mochizuki S, Dhalla NS (1999) Alterations in sarcoplasmic reticulum function and gene expression in ischemicreperfused rat heart. Am J Physiol 277:H584–H594
Traversi D, Cervella P, Gilli G (2015) Evaluating the genotoxicity of urban PM2.5 using PCR-based methods in human lung cells and the Salmonella TA98 reverse test. Environ Sci Pollut Res Int 22:1279–1289
Uldum SA, Bangsborg JM, Gahrn-Hansen B, Ljung R, Mølvadgaard M, Føns Petersen R, Wiid Svarrer C (2012) Epidemic of Mycoplasma pneumoniae infection in Denmark, 2010 and 2011. Euro Surveill 17:20073
Valko M, Morris H, Cronin MT (2005) Metals, toxicity and oxidative stress. Curr Med Chem 12:1161–1208
Viste K, Kopperud RK, Christensen AE, Døskeland SO (2005) Substrate enhances the sensitivity of type I protein kinase A to cAMP. J Biol Chem 280:13279–13284
Wages PA, Silbajoris R, Speen A, Brighton L, Henriquez A, Tong H, Bromberg PA, Simmons SO, Samet JM (2014) Role of H2O2 in the oxidative effects of zinc exposure in human airway epithelial cells. Redox Biol 3:47–55
Wagner S, Ruff HM, Weber SL, Bellmann S, Sowa T, Schulte T, Anderson ME, Grandi E, Bers DM, Backs J, Belardinelli L, Maier LS (2011) Reactive oxygen species-activated Ca/calmodulin kinase IIδ is required for late INa augmentation leading to cellular Na and Ca overload. Circ Res 108:555–565
Wagner S, Rokita AG, Anderson ME, Maier LS (2013) Redox regulation of sodium and calcium handling. Antioxid Redox Signal 18:1063–1077
Waisberg M, Joseph P, Hale B, Beyersmann D (2003) Molecular and cellular mechanisms of cadmium carcinogenesis. Toxicology 192:95–117
WHO (2006) WHO Europe Air quality guidelines for particulate matter, ozone, nitrogen dioxide and sulfur dioxide. Global Update 2005. World Health Organization. Available at: http://www.euro.who.int/document/e90038.pdf
WHO (2013) Review of evidence on health aspects of air pollution–REVIHAAP project technical report. WHO regional office for Europe, Copenhagen. http://www.euro.who.int/_data/assets/pdf_file/0004/193108/REVIHAAP-Final-technical-report-final-version.pdf?ua=1
Wu Q, Martin RJ, Lafasto S, Efaw BJ, Rino JG, Harbeck RJ, Chu HW (2008) Toll-like receptor 2 down-regulation in established mouse allergic lungs contributes to decreased mycoplasma clearance. Am J Respir Crit Care Med 177:720–729
Wu PS, Chang LY, Lin HC, Chi H, Hsieh YC, Huang YC, Liu CC, Huang YC, Huang LM (2013) Epidemiology and clinical manifestations of children with macrolide-resistant Mycoplasma pneumoniae pneumonia in Taiwan. Pediatr Pulmonol 48:904–911
Yamada M, Buller R, Bledsoe S, Storch GA (2012) Rising rates of macrolide-resistant Mycoplasma pneumoniae in the central United States. Pediatr Infect Dis J 31:409–410
Yoo SJ, Kim HB, Choi SH, Lee SO, Kim SH, Hong SB, Sung H, Kim MN (2012) Differences in the frequency of 23S rRNA gene mutations in Mycoplasma pneumoniae between children and adults with community-acquired pneumonia: clinical impact of mutations conferring macrolide resistance. Antimicrob Agents Chemother 56:6393–6396
Yu W, Liu C, Zhang C, Jiang X (2013) Monitoring air quality in China is becoming big business [N]. China daily 2013-02-08. Available at:http://europe.chinadaily.com.cn/business/2013-02/08/content_16215030.htm
Zelnikar M, Benčina, Jerala R, Manček-Keber M (2014) Vanadate from air pollutant inhibits hrs-dependent endosome fusion and augments responsiveness to toll-like receptors. PLoS One 9:e99287
Zeng X, Xu X, Zheng X, Reponen T, Chen A, Huo X (2016) Heavy metals in PM2.5 and in blood, and children’s respiratory symptoms and asthma from an e-waste recycling area. Environ Pollut 210:346–353
Zhang Q, Zhou T, Xu X, Guo Y, Zhao Z, Zhu M, Li W, Yi D, Huo X (2011) Downregulation of placental S100P is associated with cadmium exposure in Guiyu, an e-waste recycling town in China. Sci Total Environ 410–411:53–58
Zhao C, Liao J, Chu W, Wang S, Yang T, Tao Y, Wang G (2012) Involvement of TLR2 and TLR4 and Th1/Th2 shift in inflammatory responses induced by fine ambient particulate matter in mice. Inhal Toxicol 24:918–927
Zhao F, Liu G, Wu J, Cao B, Tao X, He L, Meng F, Zhu L, Lv M, Yin Y, Zhang J (2013) Surveillance of macrolide-resistant Mycoplasma pneumoniae in Beijing, China, from 2008 to 2012. Antimicrob Agents Chemother 57:1521–1523
Zheng G, Xu X, Li B, Wu K, Yekeen TA, Huo X (2013) Association between lung function in school children and exposure to three transition metals from an e-waste recycling area. J Expo Sci Environ Epidemiol 23:67–72
Zheng X, Xu X, Yekeen TA, Zhang Y, Chen A, Kim SS, Dietrich KN, Ho SM, Lee SA, Reponen T, Huo X (2016) Ambient air heavy metals in PM2.5 and potential human health risk assessment in an informal electronic-waste recycling site of China. Aerosol Air Qual Res 16:388–397
Acknowledgments
This work was supported by the Project of International Cooperation and Innovation Platform in Guangdong Universities (2013gjhz0007) and the Education Department of Guangdong Government under the Top-tier University Development Scheme for Research and Control of Infectious Diseases (2015038). We would like to thank Dr. Stanley Lin for his constructive comments and English language editing.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics statement
This manuscript is a review article and does not involve a research protocol requiring approval by the relevant institutional review board or ethics committee.
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Responsible editor: Philippe Garrigues
Rights and permissions
About this article

Cite this article
Hou, W., Xu, X., Lei, Y. et al. The role of the PM2.5-associated metals in pathogenesis of child Mycoplasma Pneumoniae infections: a systematic review. Environ Sci Pollut Res 23, 10604–10614 (2016). https://doi.org/10.1007/s11356-016-6535-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-016-6535-2