
Abstract
Links between environmental chemicals and human health have emerged, but the effects on self-rated health were less studied. Therefore, it was aimed to study the relationships of different sets of urinary environmental chemicals and the self-rated health in a national and population-based study in recent years. Data was retrieved from the US National Health and Nutrition Examination Surveys, 2011–2012, including demographics, serum measurements, lifestyle factors, self-rated health (with two grouping approaches) and urinary environmental chemical concentrations. T test and survey-weighted logistic regression modeling were performed. Among American adults aged 12–80 (n = 6833), 5892 people had reported their general health condition. Two thousand three hundred sixty-nine (40.2 %) people reported their general health condition as excellent or very good while 3523 (59.8 %) reported good, fair, or poor. People who reported their general health condition as good, fair, or poor had higher levels of urinary arsenic, heavy metals (including cadmium, cobalt, manganese, molybdenum, lead, antimony, strontium, tungsten and uranium), phthalates, pesticides and polyaromatic hydrocarbons but lower levels of benzophenone-3 and triclosan. There were no associations with urinary parabens, perchlorate, nitrate, thiocyanate or polyfluorinated compounds. However, only urinary cadmium, benzophenone-3, triclosan, and 2-hydroxynaphthalene remained significant when comparing between “good to excellent” and “poor to fair.” This is the first time observing risk associations of urinary arsenic, heavy metal, phthalate, pesticide, and hydrocarbon concentrations and self-rated health in people aged 12–80, although the causality cannot be established. Further elimination of these environmental chemicals in humans might need to be considered in health and environmental policies.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Links between environmental chemicals and human health including hypertension, cardiovascular diseases, food allergy, lung diseases, cancer and vision, remembering condition, hearing and balancing impairments and even emotional needs in American adults have emerged (Shiue 2013a, b, c, 2014a, b, 2015a, b), but the effects on self-rated health, an important risk predictor for human health conditions including both physical and mental domains (Mavaddat et al. 2014; Euteneuer 2014; Quon and McGrath 2014), have not been studied. In this context, therefore, the present study was aimed to examine the relationships of different sets of urinary environmental chemical concentrations and self-rated health in a national and population-based setting.
Methods
Study sample
As described elsewhere (Centers for Disease Control and Prevention CDC 2012), the US National Health and Nutrition Examination Surveys (NHANES) has been a national, population-based, multi-year, cross-sectional study since the 1980s. The study sample is representative of the civilian, noninstitutionalized US population. Information on demographics, serum measurements, lifestyle factors, self-rated health and urinary environmental chemical concentrations was obtained by household interview. In the current analysis, the 2011–2012 cohort as the most recent study cohort with the available information mentioned above was selected for statistical analysis. Informed consents were obtained from participants by the NHANES researchers.
Biomonitoring
Urines were only collected in a subsample, being one third of the whole cohort (still representative), to measure environmental chemical concentrations in urines among people aged 6 and above. Urine specimens were processed, stored under appropriate frozen (−20 °C) conditions, and shipped to the Division of Environmental Health Laboratory Sciences, National Center for Environmental Health, Centers for Disease Control and Prevention for analysis. According to the NHANES website (more details via: http://wwwn.cdc.gov/nchs/nhanes/2011-2012/PERNT_G.htm), ion chromatography coupled with electrospray tandem mass spectrometry was used to detect and measure the amount. Chromatographic separation is achieved using an IonPac AS16 column with sodium hydroxide as the eluent. The eluent from the column is ionized using an electrospray interface to generate and transmit negative ions into the mass spectrometer. Comparison of relative response factors (ratio of native analyte to stable-isotope-labeled internal standard) with known standard concentrations yields individual analyte concentrations. For statistical analysis purpose in the present study, urinary environmental chemical concentrations were all log transformed since they were highly skewed to one side.
Statistical analysis
People aged 12–80 were included in the current statistical analysis because self-rated health was asked in such age group (for more details please refer to: http://wwwn.cdc.gov/nchs/nhanes/2011-2012/HSQ_G.htm). Associations of different sets of urinary environmental chemical concentrations and self-rated health (question: Would you say your health in general is…? Answer: excellent, very good, good, fair, or poor) were examined separately by t test and survey-weighted logistic regression modeling to present odds ratios (OR) and 95 % confidence intervals (more details via: http://www.cdc.gov/Nchs/tutorials/environmental/orientation/sample_design/index.htm), with P < 0.05 considered statistically significant (Fig. 1). Self-rated health was treated as binary. There were two grouping approaches employed. In the first instance, being excellent and very good were grouped together (reference group) while being good, fair, and poor were grouped together. In the second instance, being excellent, very good, and good were grouped together (reference group) while being fair and poor were grouped together. Results following different grouping strategies were shown accordingly. Covariates including urinary creatinine, age, sex, ratio of family income to poverty (proxy of socioeconomic status), body mass index (BMI), serum cotinine (biomarker of smoking status), alcohol habit and physical activity level were adjusted.

Distribution of self-rated health condition
In addition, upon significant associations presented in the results, a subsequent analysis was initiated by treating the outcome variable as continuous. Survey-weighted general linear regression modeling was carried out to present betas (B) with 95 % confidence interval (CI). Statistical software STATA version 13.0 (STATA, College Station, TX, USA) was used to perform all the analyses. Since the present study is employing secondary data analyses without personal information identified, no further ethics approval was required.
Results
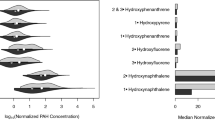
Among American adults aged 12–80 (n = 6833), 5892 people had reported their general health condition. 2369 (40.2 %) people reported their general health condition as excellent or very good while 3523 (59.8 %) reported good, fair or poor (see Table 1). People who reported their general health condition good, fair or poor had higher levels of urinary arsenic, heavy metals (including cadmium, cobalt, manganese, molybdenum, lead, antimony, strontium, tungsten and uranium), phthalates, pesticides and polyaromatic hydrocarbons but lower levels of benzophenone-3 and triclosan. There were no associations with urinary parabens, perchlorate, nitrate, thiocyanate or polyfluorinated compounds. However, only cadmium (OR 1.28, 95 % CI 1.09–1.50, P = 0.004), benzophenone-3 (OR 0.89, 95 % CI 0.82–0.96, P = 0.007), triclosan (OR 0.87, 95 % CI 0.80–0.96, P = 0.007) and 2-hydroxynaphthalene (OR 1.18, 95 % CI 1.00–1.40, P = 0.050) remained significant risk effects on self-rated health when comparing between “good to excellent” and “poor to fair” (data not shown).
Discussion
There are strengths in designing this study. First, this study was conducted in a large and nationally representative human sample with mixed socioeconomic status. Second, this is the first time examining the risk associations of urinary arsenic, heavy metals, phthalates, pesticides, phenols, polyaromatic hydrocarbons, parabens, perchlorate, nitrate, thiocyanate and polyfluorinated compounds and self-rated health in both adolescents and adults aged 12–80. Therefore, no previous studies from literature with the same or similar topics could be compared and discussed here. However, there are also some limitations that cannot be ignored. First, there could still be other emerging chemicals from the living environments that we might not yet know and would need future research to further identify and examine. Second, the causality cannot be established in the present study due to the cross-sectional study design in nature. Therefore, future studies with a longitudinal or experimental study design to confirm or refute the current observations and, if at all, to understand the persisting risk effects along the life course from those mentioned above environmental chemicals would be suggested.
Conclusion
In sum, American adults who reported their general health condition good, fair or poor had higher levels of urinary arsenic, heavy metals (including cadmium, cobalt, manganese, molybdenum, lead, antimony, strontium, tungsten and uranium), phthalates, pesticides and polyaromatic hydrocarbons but lower levels of benzophenone-3 and triclosan, compared to those reported their health conditions excellent or very good. There were no associations with urinary parabens, perchlorate, nitrate, thiocyanate or polyfluorinated compounds. Further elimination of these environmental chemicals in humans might need to be considered in future health and environmental policies.
References
Centers for Disease Control and Prevention (CDC) (2012) National Center for Health Statistics (NCHS). National Health and Nutrition Examination Survey Data. Hyattsville, MD: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, [http://www.cdc.gov/nchs/nhanes.htm]
Euteneuer F (2014) Subjective social status and health. Curr Opin Psychiatry 27:337–343
Mavaddat N, Parker RA, Sanderson S, Mant J, Kinmonth AL (2014) Relationship of self-rated health with fatal and non-fatal outcomes in cardiovascular disease: a systematic review and meta-analysis. PLoS One 9:e103509
Quon EC, McGrath JJ (2014) Subjective socioeconomic status and adolescent health: a meta-analysis. Health Psychol 33:433–447
Shiue I (2013a) Urine phthalate concentrations are higher in people with stroke: United States National Health and Nutrition Examination Surveys (NHANES), 2001–2004. Eur J Neurol 20:728–731
Shiue I (2013b) Association of urinary arsenic, heavy metal, and phthalate concentrations with food allergy in adults: National Health and Nutrition Examination Survey, 2005–2006. Ann Allergy Asthma Immunol 111:421–423
Shiue I (2013c) Urinary environmental chemical concentrations and vitamin D are associated with vision, hearing, and balance disorders in the elderly. Environ Int 53:41–46
Shiue I (2014a) Urinary thiocyanate concentrations are associated with adult cancer and lung problems: US NHANES, 2009–2012. Environ Sci Pollut Res Int. doi:10.1007/s11356-014-3777-8
Shiue I (2014b) Higher urinary heavy metal, phthalate, and arsenic but not parabens concentrations in people with high blood pressure, U.S. NHANES, 2011–2012. Int J Environ Res Public Health 11:5989–5999
Shiue I (2015a) Arsenic, heavy metals, phthalates, pesticides, hydrocarbons and polyfluorinated compounds but not parabens or phenols are associated with adult remembering condition: US NHANES, 2011–2012. Environ Sci Pollut Res Int 22:6381–6386
Shiue I (2015b) Urinary parabens and polyaromatic hydrocarbons independent of health conditions are associated with adult emotional support needs: USA NHANES, 2005-2008. Environ Sci Pollut Res Int. doi:10.1007/s11356-015-4561-0
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
Responsible editor: Philippe Garrigues
Rights and permissions
About this article

Cite this article
Shiue, I. Urinary arsenic, heavy metals, phthalates, pesticides, polyaromatic hydrocarbons but not parabens, polyfluorinated compounds are associated with self-rated health: USA NHANES, 2011–2012. Environ Sci Pollut Res 22, 9570–9574 (2015). https://doi.org/10.1007/s11356-015-4604-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-015-4604-6