
Abstract
Epidemiological studies have widely demonstrated association between ambient ozone and mortality, though controversy remains, and most of them only use a certain metric to assess ozone levels. However, in China, few studies have investigated the acute effects of ambient ozone, and rare studies have compared health effects of multiple daily metrics of ozone. The present analysis aimed to explore variability of estimated health effects by using multiple temporal ozone metrics. Six metrics of ozone, 1-h maximum, maximum 8-h average, 24-h average, daytime average, nighttime average, and commute average, were used in a time-series study to investigate acute mortality associated with ambient ozone pollution in Guangzhou, China, using 3 years of daily data (2006–2008). We used generalized linear models with Poisson regression incorporating natural spline functions to analyze the mortality, ozone, and covariate data. We also examined the association by season. Daily 1- and 8-h maximum, 24-h average, and daytime average concentrations yielded statistically significant associations with mortality. An interquartile range (IQR) of O3 metric increase of each ozone metric (lag 2) corresponds to 2.92 % (95 % confidence interval (CI) 0.24 to 5.66), 3.60 % (95 % CI, 0.92 to 8.49), 3.03 % (95 % CI, 0.57 to 15.8), and 3.31 % (95 % CI, 0.69 to 10.4) increase in daily non-accidental mortality, respectively. Nighttime and commute metrics were weakly associated with increased mortality rate. The associations between ozone and mortality appeared to be more evident during cool season than in the warm season. Results were robust to adjustment for co-pollutants, weather, and time trend. In conclusion, these results indicated that ozone, as a widespread pollutant, adversely affects mortality in Guangzhou.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Plenty of epidemiological studies, especially in USA and Europe, have demonstrated significant association between ambient ozone (O3) and mortality, including non-accidental mortality and mortality caused by cardiovascular disease and respiratory disease (Katsouyanni et al. 2001; Thurston and Ito 2001; Bell et al. 2004, 2005; Gryparis et al. 2004; Huang et al. 2005; Bell and Dominici 2008). A variety of concentration metrics for the time frame were used in these studies which analyzed O3’s acute effects on mortality and morbidity, including 1-h maximum, maximum 8-h average, and 24-h average (Bell et al. 2004; Zhang et al. 2006; Yang et al. 2012). The choice of temporal metrics could likewise affect risk estimates observed in these studies. So, standard ratios were used to convert among multiple metrics; however, it would introduce uncertainty (Anderson and Bell 2008), making it difficult and imprecise to combine or compare results using different metrics. Few studies, both in developed countries (Abbey and Burchette 1996; Bell et al. 2004; Darrow et al. 2011) and developing countries (Yang et al. 2012), have estimated the effects of multiple O3 metrics on human health.
When investigating the association between ambient air pollution and population health effects by ecological research method, ambient pollutant measurements from the Environmental Monitoring Center are used to assess the exposure levels of population. So, it is possible that the optimal temporal metric for an epidemiological study is determined by both the diurnal pattern of pollutant concentration and the time-activity pattern of population. The former reflects that which time frame is the most biologically relevant one. For example, peak concentration (1-h maximum) or average concentration metric would be chosen based on whether the health outcome is triggered by a higher, shorter dose or by a lower, relatively steady dose for several hours. The latter shows when the population is most likely to be exposed to ambient air because people generally spend most of their time indoors. A recent study (Chen et al. 2012) examined whether variation in O3 mortality coefficients might be partly explained by differences in total ozone exposure (from both outdoor and indoor exposures) based on 18 cities that had been included in the National Morbidity and Mortality Air Pollution Study (NMMAPS). Take 8-h O3 as an example, they found strong association between O3 exposure coefficients and O3 mortality coefficients (R 2 = 0.56, p < 0.001), suggesting that differences in total ozone exposure partially led to differences in O3 mortality coefficients. We assume that people are more likely to be exposed to ambient air during the daytime, especially during heavy commuting hours, and less likely to be exposed directly to ambient air in the evening. Therefore, exposure measurement error may be introduced according to exposure metric used. Previously, rare studies have reported effects of O3 exposure for multiple metrics simultaneously.
So far, limited published epidemiological studies focus on Chinese cities (Zhang et al. 2006; Wong et al. 2008; Tao et al. 2011; Liu et al. 2012). Along with the rapid economic growth comes increasingly serious air pollution in this biggest developing country, China (Kan et al. 2009, 2012), and O3 is now recognized as an important air pollutant that could increase health risk (Tao et al. 2011; Kan et al. 2012). So, it is difficult to compare region-specific results with findings in the developed areas and also hard to inform local regulatory policy (Fann et al. 2011). Guangzhou is the core city of Pearl River Delta (PRD), an area with the fastest economic growth and urbanization and severe photochemical pollution (Chan and Yao 2008; Zhang et al. 2008). And, Guangzhou is a typical megacity of China that can represent the cities that have urgent issues of public health caused by air pollution in China, and it has a sound quality of data. So, we think that Guangzhou is a unique site for evaluating health effects of O3 pollution.
In the present study, we used generalized linear model (GLM) to conduct a time-series study in Guangzhou to explore short-term effects of O3 on daily mortality. In particular, various metrics of O3 were used, including 1-h maximum, maximum 8-h average, 24-h average, daytime average, nighttime average, and average of commute hours, in order to explore whether alternative temporal metrics would yield different relationships than a priori metrics, which are commonly used in air pollution research, and describe the variability of epidemiological results attributed to the use of different temporal metrics. Our findings might provide clues, or serve as evidence for further study on effects of ambient O3 on daily mortality, and ultimately provide useful information for environmental regulatory policies in China.
Material and methods
Guangzhou is located in the southern part of China with high population density. It has a total area of 7,434 km2 and a population of 12.7 million according to the national census in 2010. Guangzhou has a typical subtropical humid monsoon climate with an average annual temperature of 22 °C and relative humidity of 68 %. We chose Yuexiu district (a district is a subdivision of a municipality or a prefecture-level city) (see Supplemental Fig. 1) in this study because (1) this district is in the central area of Guangzhou and has a total area of 33.80 km2 with an ozone monitoring station, reflecting the pollution of central urban area, (2) this district has an average total population of 1.16 million during 2006 to 2008 and has the highest population density among all the districts, which is more than 34,000 per km2, and (3) this district has homogeneous characteristics of residents and a sound quality of mortality data.
Data collection
Daily mortality data in Yuexiu district of Guangzhou from January 1 2006 to December 31 2008 were obtained from the Guangzhou Provincial Center for Disease Control and Prevention (GDCDC). These data are comparable to data collected by the public security station. The causes of death were coded according to the International Classification of Diseases, Tenth Revision [ICD-10]. Only non-accidental mortality data (ICD-10: A00-R99) was analyzed in the present study.
Daily meteorological data were collected from the Guangzhou Meteorological Bureau. The daily mean temperature, relative humidity (RH), and dew point were used in the present study to adjust the effect of weather on mortality.
We obtained hourly ambient concentrations of O3, NO2, SO2, and PM10 from one monitoring station conducted by the Guangdong Environmental Monitoring Center. The monitoring station is located in the central city Park Luhu, reflecting the general background urban air pollution level in Guangzhou. The monitors sample air at about 9 m above ground level. We abstracted daily 24-h average concentrations of PM10, NO2, and SO2 to control for the confounding effects.
We created the following temporal metrics of daily O3 concentrations (Darrow et al. 2011): a daily 1-h maximum, a daily maximum 8-h average, a 24-h average, a daytime average (“daytime”, 0800–1900 h), a nighttime average (“nighttime”, 2400–0600 h), and an average of commute hours (“commute”, 0700–1000 and 1600–1900 h). For the calculation of 24-h average concentrations of O3, it is required to have at least 75 % of the 1-h values on that particular day. For the maximum 8-h average of O3, at least six hourly values have to be available. We provided effect estimates of O3 for the three most commonly used metrics and three alternative metrics in order to (1) examine whether the choice of metrics affects the direction of association, (2) compare the magnitude of association for multiple metrics, (3) and explore the implications of choice of exposure time frame on health risk estimates.
Statistical analysis
Because daily death counts typically follow a Poisson distribution, the core analysis was a GLM with log link and Poisson error that account for smooth fluctuations in daily mortality. We used the GLM to analyze the mortality, O3 pollution levels, and covariate data from 2006 to 2008 in Guangzhou, with natural cubic spline for filtering out seasonal patterns and long-term trends (Bell et al. 2004; Wong et al. 2008). Smoothed spline functions of time and weather conditions were first incorporated in the basic model, and Akaike’s information criterion (AIC) was used to determine the degree of freedom (df) of the natural spline smoothers (Hurvich et al. 1998). The previous studies have tested 1 to 21 df per year of data for time trend and 3 or 4 df for weather variable (Bell et al. 2004; Zhang et al. 2006). Based on the minimized AIC, we chose 8 df per year and 3 df for daily temperature, dew point, and RH. Day of the week (DOW) was included as dummy variable in the models. Then, we introduced the pollutant variables into the models and analyzed the effects on mortality.
We calculated partial Spearman correlations between six metrics and between ozone and other pollutants. Corresponding p values, which are highly influenced by sample size and not unit dependent, were calculated to verify whether the estimated results were statistically significant for each metric.
Most studies in China reported results at lags 1 and 2 or moving average concentration at lags 01 and 12 after examining the lag structure (Zhang et al. 2006; Tao et al. 2011; Yang et al. 2012). According to prior research, single-day lag models might underestimate the cumulative association of O3 with mortality (Bell et al. 2004), so we also examined the associations with different lag structures to conduct sensitivity analyses, both by including a single-day (from lag 0 to lag 4) and multiday moving average lags (lag 01, lag 04, and lag 12). Therefore, we reported the estimated effects of mortality and its 95 % confidence interval (CI) associated with both a 10 μg/m3 increase, to compare with previous studies, and an interquartile range (IQR) increase in each metric to compare among metrics for the same relative degree of variability. Both single- and two-pollutant models were applied to estimate for confounding by other pollutants. Two-pollutant models were restricted to pollutants with partial Spearman correlations <0.6 to avoid collinearity.
Then, we stratified O3 concentration as concentrations during warm season (May through October) and cool season (November through April) by using 4-df spline to control for time trend for each period (Wong et al. 2001b; Darrow et al. 2011; Liu et al. 2012). We tested the statistical significance of differences between effect estimates of the strata of season by calculating the 95 % confidence interval (95 % CI) as \( \left({\widehat{Q}}_1-{\widehat{Q}}_2\right)\pm 1.96\sqrt{S{{\widehat{E}}_1}^2+S{{\widehat{E}}_2}^2} \), where \( {\widehat{Q}}_1 \) and \( {\widehat{Q}}_2 \) are the estimates for the warm season and cool season and SÊ 1 and SÊ 2 are their respective standard errors (Zeka et al. 2006).
Additional sensitivity analyses were examined for estimated effects of maximum 8-h average exposure (lag 2) on mortality with respect to (1) excluding days with daily concentrations of O3 above the 95th or below the 5th percentile; (2) excluding days with daily concentrations of O3 above 160 μg/m3, which is the regulatory standard value in People’s Republic of China Ambient Air Quality Standards (GB3095-2012); (3)adding temperature at lag 2, lag 1–2 days, and lag 4–6 days; and (4) varying the df in the smooth functions of time to control for seasonality and long-term trends, from 1 to 15 per year.
All the analyses were conducted by glm function in quantmod package of R 2.15.1 (R Development Core Team 2012). Statistical significant was defined as p < 0.05.
Results
Table 1 summarizes the non-accidental mortality data, pollutants data, and meteorological data for Guangzhou through 2006 to 2008. The average number of daily deaths in the Yuexiu district during the whole period was 17.7. The mean daily 1-h maximum, maximum 8-h average, 24-h average, daytime average, nighttime average, and commute average concentrations of O3 were 105.5, 74.3, 36.4, 55.4, 16.0, and 34.3 μg/m3, respectively. The mean daily average temperature, dew point, and relative humidity (RH) were 23.1 °C, 16.9 °C, and 72 %, respectively, reflecting the subtropical climate in the city.
For O3, many of the metrics were highly correlated with each other (r = 0.666–0.954), except the nighttime metric, which was extremely uncorrelated or weakly correlated with other metrics (Table 2). The more temporal overlap between two metrics, the higher the correlation observed between them. For example, the daytime was highly correlated with 24-h average and 8-h average. The weakest correlation among the O3 metrics was between 1-h maximum and nighttime, for O3 concentration was always high during the daytime with high temperature. All the metrics were negatively correlated or weakly correlated with PM10, NO2, and SO2.
Diurnal pattern of O3 was presented in Supplemental Fig. 2. O3 exhibited a typical diurnal trend, with peaks occurring in the mid to late afternoon and the minimum occurring during the night. Supplemental Fig. 3a–f present each metric concentration of O3 in each month. We observed an apparent seasonal trend for O3 concentrations; namely, O3 concentrations experienced a slight increase in summer and reached the maximum in autumn.
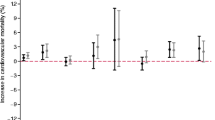
Most studies in China reported significant effects at lags 1 and 2 or moving average concentration at lags 01 and 12 (Thurston and Ito 2001; Zhang et al. 2006; Tao et al. 2011). Our results were consistent with these studies. We compared the statistical significance and the magnitudes of associations for multiple metrics at lag 2 (Table 3). The associations between total mortality and 1-h maximum, 8-h maximum, 24-h average, and daytime O3 metrics were statistically significant for both scales (a 10 μg/m3 and an IQR). Furthermore, when comparing the magnitudes of association, interpretation differed a lot according to how the regression coefficients were scaled: the same unit (10 μg/m3) or IQR. The estimate for 24-h average was highest when effects were scaled according to increase of the same unit, but the maximum 8-h average was highest when scaled to the IQR. However, using nighttime average and commute average, the associations were not significant. Figure 1 compares the percent increase of total mortality per 10 μg/m3 increase for each metric of O3 (lag 2), with and without adjustment for PM10, SO2, and NO2. We found that estimates for various metrics were mostly robust to the adjustment for co-pollutants.

Estimated effects of short-term O3 exposure on mortality, with and without adjustment for co-pollutants (A, B, C, D, E, and F represent 1-h maximum, 8-h maximum, 24-h average, average of daytime, nighttime, and commute, respectively)
We explored whether the associations between ozone and mortality were modified by seasons by performing a stratified analysis (Table 4). Some metrics of O3 were significantly associated with total mortality during cool season, and the magnitudes were higher than that of the year-round estimates. For warm season, we did not observe significant associations for any metrics that we used. However, the between-season difference was statistically insignificant.
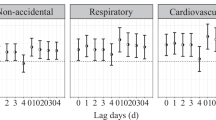
We performed sensitivity analysis of different lag structures of O3 exposure, including single-day lags and multiday lags (Fig. 2). For single-day lags, the effects of daily 1-, 8-, and 24-h and daytime O3 were maximal at lag day 2 and commute O3 average at lag 3. Multiday lags (lag 12) yielded similar effects compared with single-day lags. The effects of nighttime O3 concentration were not significant for all the lagged days that we examined.

Percent increase in daily mortality with 10 μg/m3 increase of O3
Additional sensitivity analysis indicated that the effect estimates of O3 (maximum 8-h average was used as an indicating metric to perform sensitivity analysis) were robust to different methods adopted (Table 5). Most of the O3 effect estimates did not deviate from the main analysis >20 %; however, we found stronger association when excluding days with higher O3 concentration. With smoothing of calendar time varying from 3 to 15, the estimates of the mortality increase associated with a 10 μg/m3 increase in the previous O3 concentrations ranged from 0.38 %(95 % CI, 0.03–0.72) to 0.62 % (95 % CI, 0.26–0.98) (see Supplemental Fig. 4), suggesting that our findings with regard to the effect of O3 on mortality outcomes were relatively robust.
Discussion
In this time-series study, we compared associations between multiple temporal metrics of O3 concentration and non-accidental mortality in Guangzhou. To our knowledge, this is one of the few studies to report the acute effect on daily mortality of ambient O3 exposure for multiple metrics simultaneously in China (Yang et al. 2012). Our results should contribute to the understanding of O3-related health effects in China.
Diurnal pattern of O3 concentrations led to variation among different metrics. Generally, temporal metrics including peak pollutant hours had higher exposure levels. For example, daytime average concentration (55.4 μg/m3) was higher than 24-h average concentration (36.4 μg/m3) during our study period, because the latter combined both day and night concentrations into one metric. Since we were not sure about individual’s time-activity pattern, we analyzed relationships between all these temporal metrics of O3 and mortality. In our study site Guangzhou, the O3 concentration was higher in warm season (89.0 μg/m3) than cool season (59.2 μg/m3). During the warm season (from May to October) and cool season (from November to April), O3 concentrations varied a lot from month to month, as the difference between higher O3 level and lower O3 levels months was around 29.9 μg/m3 during warm season, for example.
In general, similar estimates were observed across all the ozone metrics. Four metrics were strongly statistical significantly associated with increased mortality (1-h maximum, 8-h maximum, 24-h average, and daytime average) and yielded slightly similar magnitude associations with daily mortality. The other metrics (nighttime and commute average) were weakly associated with mortality. One time-series study used these same metrics to investigate relationships between ambient air pollution and respiratory emergency department (ED) visits in Atlanta. For O3, 8-h maximum, 1-h maximum, and daytime average yielded significantly positive associations with respiratory ED, and multiple metrics of ozone were slightly similar with overlapping 95 % CIs. Our results were consistent with the prior study. Also, we found that with an IQR increase in each metric concentration, 8-h maximum yielded the largest estimate, 3.60 % (95 % CI, 0.92 to 8.49) increase in daily mortality, followed by daytime, 24-h average, and 1-h maximum. One-hour maximum, which included peak hour of O3 concentrations (Supplemental Fig. 2), however, yielded the smallest estimate. In addition, our pollution data was collected from environmental monitoring station located in Park Luhu at the downtown, reflecting downtown pollution condition. Eight-hour maximum and daytime concentrations might correlate best with individual exposure levels because of influx of people into the city center during the day and exodus at night. And, the high ozone exposure during the 8-h maximum period and daytime in the city may cause more significant health effect compared with nighttime and commute time. So, it was suggested that health effects were more related with a short time exposure of a little higher O3 concentration, such as 8-h maximum and daytime concentration of O3, rather than a peak concentration, like the 1-h maximum. The addition of daily maximum 8-h average concentration for O3 into the People’s Republic of China Ambient Air Quality Standards in 2012 was partly supported by our analysis.
Nighttime average metric was less correlated with other metrics and negatively correlated with all the co-pollutants. When we controlled for PM10 and NO2 in two-pollutant models, estimated effects of nighttime O3 increased slightly (Fig. 1). What is more, people are likely to be in their homes during nighttime (Klepeis et al. 2001). So, the weak associations for nighttime O3 might also indicate that 24-h average metric would not be a proper exposure time frame, because it included nighttime O3 concentrations. A previous investigation (Darrow et al. 2011) in Atlanta, USA, also found variability of estimates across O3 metrics by examining associations between O3 metrics and respiratory ED visits. They observed that nighttime O3 metric was negatively associated with health outcome. Our findings were consistent with these previous studies to some extent.
We found weaker associations between mortality and commute metrics, when people are supposed to be more likely to be exposed to ambient air. And, the estimates were robust to adjustment by co-pollutants. The diurnal pattern (Supplemental Fig. 2) of O3 levels showed that the commute time included two periods in which O3 was forming and depleting and did not include hours when O3 levels are the highest, which partly explained that the health effects might not be obvious. In addition, the weak association observed for commute ozone indicated that O3 may be not the only pollutant related to mortality.
We compared percent increase in total mortality associated with 10 μg/m3 increase in maximum 8-h average O3 (lag 12) with a previous study (Tao et al. 2011) which was conducted in the same city. This recent study with the same metric and same lagged day (Tao et al. 2011) found 0.64 % (95 % CI, 0.42 to 0.86) increase in total mortality, which is roughly comparable to our analysis, indicating 0.50 % (95 % CI, 0.05 to 0.95). The slight difference of magnitude might be caused by that this recent study (Tao et al. 2011) used averaging O3 concentrations from two monitoring stations, one located in rural area and the other in urban area, while our study used data from one station in the central city. Besides, another important reason causing this difference may be due to the fact that the study of Tao (2011) used mortality data from more districts of Guangzhou city, which had an average of 83.2 daily non-accidental deaths compared with an average of 17.7 daily non-accidental deaths in our study, which may result in a relative risk value with narrower CIs than that of this study. The reason that we only chose one district of Guangzhou is that the data in this district is of high quality and availability.
Also, we compared our results with related studies worldwide from two aspects. First, prior studies mainly reported effects of ozone in regions with relative low exposure level, mostly in the USA and Europe. However, we conducted this study in Guangzhou where ozone is the primary pollutant and the level is quite high (Chan and Yao 2008). Based on a time-series study of 95 large US urban communities, a 15-ppb (≈30 μg/m3) increase in the previous week’s O3 (8-h max) was associated with a 0.64 % (95 % CI, 0.41–0.86 %) increase in daily total mortality (Bell et al. 2004). Consistent with previous studies in the USA, our analysis found that a 30 μg/m3 increase in the lag 2 O3 (8-h max) corresponds to 1.42 % (95 % CI, 0.33–2.52 %) increase in total mortality.
Furthermore, various O3 metrics were used as proxies for population exposure throughout the paper published. In a previous study of China, Yang et al. (Yang et al. 2012) examined effects of three exposure metrics of O3 (1-h max, max 8-h average, and 24-h average) on daily mortality in Suzhou. One-hour max and 8-h max were more strongly associated with increased mortality compared to 24-h average levels. A cohort study (Abbey and Burchette 1996) investigated long-term effects of alternative ambient O3 metrics on respiratory diseases and found that the metric with the greatest power for the most health outcomes was the 8-h average (9:00 am to 5:00 pm). We also suggested in the present study that it be inappropriate to use 24-h average as an exposure metric. However, a study of Prague (Hůnová et al. 2013) which used negative binomial model rather than Poisson regression reported that daily 24-h mean O3 concentration was more strongly associated with hospital admissions and mortality than maximum daily running 8-h mean, but it did not show an explanation for the result at that moment. According to a previous study (Smith et al. 2009), O3 mortality associations from time-series analyses of daily data for multiple cities revealed still unexplained inconsistencies and showed sensitivity to modeling choices and data selection.
Differences of pollutant’s effects between seasons were usually assessed by examining separate effects in the warm season and cool season in previous studies (Wong et al. 2001a; Zhang et al. 2006; Darrow et al. 2011; Yang et al. 2012). Guangzhou is a megacity with severe photochemical pollution and has a typical subtropical humid monsoon climate, so we examined effects both in warm season and cool season. The association between O3 and daily mortality appeared to be more evident in the cool season than in the warm season, though this difference was not statistically significant. The finding was consistent with previous studies in other Chinese cities (Zhang et al. 2006; Yang et al. 2012) but differed from western studies (Bell et al. 2004; Gryparis et al. 2004; Schwartz 2005). It could be partly explained by the subtropical monsoon climate of Guangzhou. Temperature and humidity are relatively high in warm season, and warm season includes flood season of Guangzhou from April to September, leading to unstable weather conditions. These factors might lead to common use of air conditioning and prevent people from being directly exposed to ambient air. By contrast, in cool season, with less variable weather condition, people tend to go outside and open the windows, so O3 penetrates well through open windows into indoor environment. Thus, for our study city, ambient O3 concentrations might be considered a fairly suitable surrogate for population exposure in cool season but definitely not in warm season.
In the single-day lag models, the estimated effects of daily 1-, 8-, and 24-h and daytime O3 on mortality outcomes reached a maximum at lag 2 (Fig. 2). Studies in Suzhou (Yang et al. 2012) and Shanghai (Zhang et al. 2006) both reported maximum estimates at lag days 1–2. Multiday exposure (lag 12) usually yielded a little larger effects than single-day exposure, which is consistent with previous study of the same city (Tao et al. 2011).
One critical concern is the extent to which effect estimates may be confounded by either co-pollutants or temperature. In this analysis, all the metrics were negatively correlated or weakly correlated with PM10, NO2, and SO2 (Table 2), and most estimates were robust to adjustment for these co-pollutants (Fig. 1). The lack of correlation and insensitivity of effects with inclusion of co-pollutants implied strong evidence against confounding of the effects of these co-pollutants, which was consistent with previous studies (Bell et al. 2004, 2007). The relationships between O3 and mortality did not appear to be confounded by temperature either, supported by sensitivity analysis adding temperature at diverse lag days (Table 5).
The current study had some limitations. First, the pollution data was obtained from one monitoring station, which may lead to measurement error. O3 is not a routinely monitored air pollutant in most Chinese cities, so available data of ambient O3 concentration has still been limited. Second, we used monitoring concentrations as the proxies of population exposure level of air pollution to conduct a time-series study. The pollutant measurements may differ from individual exposure levels, because of individuals’ different activity-time patterns and fast depletion of O3 in indoor environments. Therefore, further investigations are needed to help to explore this issue. Several factors might be taken into account, such as correlation between these metrics and measured individual exposure or average population exposure and time-activity pattern of the study population——the day length and commuting time vary according to different climate, geographic location, and lifestyle. Therefore, the used O3 exposure concentration or metric should be most closely related to individual exposure level when analyzing health effects of ambient O3 exposure.
Conclusions
We estimated significant associations between non-accidental mortality and multiple ozone metrics. The comparison of magnitudes for multiple ozone metrics implied possible exposure measurement error. The maximum 8-h average and daytime average of O3 might be more strongly related to mortality. World Health Organization (WHO) suggests that maximum 8-h average is a proper metrics for investigating health effects of ambient O3 exposure as well (WHO 2000). Our findings extended understanding of the acute effects of ozone on urban population and indicated that current level of O3 has an adverse effect on mortality in Guangzhou, China.
References
Abbey DE, Burchette RJ (1996) Relative power of alternative ambient air pollution metrics for detecting chronic health effects in epidemiological studies. Environmetrics 7:453–470
Anderson GB, Bell ML (2008) Does one size fit all? The suitability of standard ozone exposure metric conversion ratios and implications for epidemiology. J Expo Sci Environ Epidemiol 20:2–11
Bell ML, Dominici F (2008) Effect modification by community characteristics on the short-term effects of ozone exposure and mortality in 98 US communities. Am J Epidemiol 167:986–997
Bell ML, McDermott A, Zeger SL, Samet JM, Dominici F (2004) Ozone and short-term mortality in 95 US urban communities, 1987–2000. JAMA 292:2372–2378
Bell ML, Dominici F, Samet JM (2005) A meta-analysis of time-series studies of ozone and mortality with comparison to the national morbidity, mortality, and air pollution study. Epidemiology 16:436–445
Bell ML, Kim JY, Dominici F (2007) Potential confounding of particulate matter on the short-term association between ozone and mortality in multisite time-series studies. Environ Health Perspect 115:1591–1595
Chan CK, Yao X (2008) Air pollution in mega cities in China. Atmos Environ 42:1–42
Chen C, Zhao B, Weschler CJ (2012) Assessing the influence of indoor exposure to “outdoor ozone” on the relationship between ozone and short-term mortality in U.S. communities. Environ Health Perspect 120:235–240
Darrow LA, Klein M, Sarnat JA, Mulholland JA, Strickland MJ, Sarnat SE, Russell AG, Tolbert PE (2011) The use of alternative pollutant metrics in time-series studies of ambient air pollution and respiratory emergency department visits. J Expo Sci Environ Epidemiol 21:10–19
Fann N, Bell ML, Walker K, Hubbell B (2011) Improving the linkages between air pollution epidemiology and quantitative risk assessment. Environ Health Perspect 119:1671–1675
Gryparis A, Forsberg B, Katsouyanni K, Analitis A, Touloumi G, Schwartz J, Samoli E, Medina S, Anderson HR, Niciu EM, Wichmann HE, Kriz B, Kosnik M, Skorkovsky J, Vonk JM, Dörtbudak Z (2004) Acute effects of ozone on mortality from the air pollution and health. Am J Respir Crit Care Med 170:1080–1087
Huang Y, Dominici F, Bell ML (2005) Bayesian hierarchical distributed lag models for summer ozone exposure and cardio-respiratory mortality. Environmetrics 16:547–562
Hůnová I, Malý M, Řezáčová J, Braniš M (2013) Association between ambient ozone and health outcomes in Prague. Int Arch Occup Environ Health 86:89–97
Hurvich CM, Simonoff JS, Tsai CL (1998) Smoothing parameter selection in nonparametric regression using an improved Akaike information criterion. J R Stat Soc Ser B 60:271–293
Kan H, Chen B, Hong CJ (2009) Health impact of outdoor air pollution in China: current knowledge and future research needs. Environ Health Perspect 117:A187–A187
Kan H, Chen R, Tong S (2012) Ambient air pollution, climate change, and population health in China. Environ Int 42:10–19
Katsouyanni K, Touloumi G, Samoli E, Gryparis A, Le Tertre A, Monopolis Y, Rossi G, Zmirou D, Ballester F, Boumghar A, Anderson HR, Wojtyniak B, Paldy A, Braunstein R, Pekkanen J, Schindler C, Schwartz J (2001) Confounding and effect modification in the short-term effects of ambient particles on total mortality: results from 29 European cities within the APHEA2 project. Epidemiology 12:521–531
Klepeis NE, Nelson WC, Ott WR, Robinson JP, Tsang AM, Switzer P, Behar JV, Hern SC, Engelmann WH (2001) The National Human Activity Pattern Survey (NHAPS): a resource for assessing exposure to environmental pollutants. J Expo Anal Environ Epidemiol 11:231–252
Liu T, Li TT, Zhang YH, Xu YJ, Lao XQ, Rutherford S, Chu C, Luo Y, Zhu Q, Xu XJ, Xie HY, Liu ZR, Ma WJ (2012) The short-term effect of ambient ozone on mortality is modified by temperature in Guangzhou, China. Atmos Environ 76:56–67
Schwartz J (2005) How sensitive is the association between ozone and daily deaths to control for temperature? Am J Respir Crit Care Med 171:627–631
Smith RL, Xu B, Switzer P (2009) Reassessing the relationship between ozone and short-term mortality in U.S. urban communities. Inhal Toxicol 21:37–61
Tao Y, Huang W, Huang X, Zhong L, Lu SE, Li Y, Dai L, Zhang Y, Zhu T (2011) Estimated acute effects of ambient ozone and nitrogen dioxide on mortality in the Pearl River Delta of southern China. Environ Health Perspect 120:393–398
Thurston GD, Ito K (2001) Epidemiological studies of acute ozone exposures and mortality. J Expo Anal Environ Epidemiol 11:286–294
WHO (2000) Air quality guidelines for Europe
Wong CM, Ma S, Anthony Johnson H, Lam TH (2001a) Effect of air pollution on daily mortality in Hong Kong. Environ Health Perspect 109:335–340
Wong CM, Ma S, Hedley AJ, Lam TH (2001b) Effect of air pollution on daily mortality in Hong Kong. Environ Health Perspect 109:335–340
Wong CM, Vichit-Vadakan N, Kan H, Qian Z (2008) Public Health and Air Pollution in Asia (PAPA): a multicity study of short-term effects of air pollution on mortality. Environ Health Perspect 116:1195–1202
Yang C, Yang H, Guo S, Wang Z, Xu X, Duan X, Kan H (2012) Alternative ozone metrics and daily mortality in Suzhou: the China Air Pollution and Health Effects Study (CAPES). Sci Total Environ 426:83–89
Zeka A, Zanobetti A, Schwartz J (2006) Individual-level modifiers of the effects of particulate matter on daily mortality. Am J Epidemiol 163:849–859
Zhang Y, Huang W, London SJ, Song G, Chen G, Jiang L, Zhao N, Chen B, Kan H (2006) Ozone and daily mortality in Shanghai, China. Environ Health Perspect 114:1227–1232
Zhang YH, Su H, Zhong LJ, Cheng YF, Zeng LM, Wang XS, Xiang YR, Wang JL, Gao DF, Shao M, Fan SJ, Liu SC (2008) Regional ozone pollution and observation-based approach for analyzing ozone–precursor relationship during the PRIDE-PRD2004 campaign. Atmos Environ 42:6203–6218
Acknowledgments
This work was supported by the National Natural Science Foundation of China (project numbers: 21277135, 40905069, 41205081), Beijing National Natural Science Foundation (project number: 8132048), China Environmental Protection Agency (EPA) Charity Special Fund (project number: 201009032), and Guangdong Province medical fund (project number: B2012072)
Compliance with ethical standards
We confirm that the manuscript has been read and approved by all named authors and that there are no other persons who satisfied the criteria for authorship but are not listed. We also confirm that there are no known conflicts of interest associated with this publication and there has been no significant financial support for this work that could have influenced its outcome.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding authors
Additional information
Responsible editor: Michael Matthies
Tiantian Li, Meilin Yan, and Wenjun Ma are co-first authors.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplemental Table 1A
(DOCX 13 kb)
Supplemental Table 2B
(DOCX 13 kb)
Supplemental Table 2
(DOCX 14 kb)
Supplemental Fig. 3
(DOCX 158 kb)
Supplemental Fig. 2
(DOCX 71 kb)
Supplemental Fig. 3A
(DOCX 41 kb)
Supplemental Fig. 3B
(DOCX 28 kb)
Supplemental Fig. 3C
(DOCX 37 kb)
Supplemental Fig. 3D
(DOCX 42 kb)
Supplemental Fig. 3E
(DOCX 38 kb)
Supplemental Fig. 3F
(DOCX 39 kb)
Supplemental Fig. 4
(DOCX 58 kb)
Rights and permissions
About this article

Cite this article
Li, T., Yan, M., Ma, W. et al. Short-term effects of multiple ozone metrics on daily mortality in a megacity of China. Environ Sci Pollut Res 22, 8738–8746 (2015). https://doi.org/10.1007/s11356-014-4055-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-014-4055-5