
Abstract
The objectives of this study were to survey elementary school students regarding the environmental conditions of their elementary schools and to assess the relationship between air pollution and allergic disease using the International Study of Asthma and Allergies in Childhood (ISAAC) questionnaire. Therefore, this study was designed as a cross-sectional study. In this study, seven elementary schools were selected and they were classified into three categories. The selection included one school with no traffic-related or other pollutants, three with traffic-related pollutants, and three with traffic-related and other pollutants from industrial and filling station sources. The ISAAC questionnaire survey was given to all of the students except to those in the 1st grade who were presumed to be less likely to be exposed to the school environment than the remainder of the students attending those seven schools. The assessment of allergic disease was conducted on a total of 4,545 students. Three school zones with critical exposure were selected within each school and they were evaluated based on the levels of black carbon (BC), PM10, SO2, NO2, and O3. There was a significant increase in the risks based on the odds ratios of treatment experiences (within 1 year) for allergy-related diseases such as asthma and allergic rhinitis (a) in the school group with traffic-related pollutants and the school group with complex pollutants were 2.12 (1.41–3.19) and 1.59 (1.06–2.37), respectively, in comparison to the school groups with no exposure to pollutants. This was determined based on the odds ratio of symptoms and treatment experiences for allergy-related diseases by group based on the home town zone as a reference. Also, in the case of atopic dermatitis, the odds ratio of treatment experiences (within 1 year) was 1.42 (1.02–1.97), which indicated elevated risks compared to the students in the S1 school. A regression analysis was used to assess the relationship between the substances and the symptomatic experiences within the last year. There were significant increases in the odds ratio of the symptoms associated with allergic rhinitis and the BC and SO2 in the complex pollution areas. The results of the assessment of the relationship between atopic dermatitis-associated symptoms and O3 showed that the odds ratio increased with statistical significance.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
An elementary school is an important public place for children and it is where they spend most of their days (Canha et al. 2011; Leickly 2003). Previous studies have reported that the indoor and outdoor air quality of schools and traffic-related pollution were related to the health of children (Carlisle and Sharp 2001; Dockery et al. 1996; Heindrich et al. 2005; Hirsch et al. 1999; McConnell et al. 2010; Venn et al. 2000), although some studies have also reported inconsistent results (McConnell et al. 1999; Peters et al. 1999). The varying results are likely due to differences in methods, air pollution concentrations, measurement locations, participant groups, and differences in pollutant classification (Annesi-Maesano et al. 2007).
In general, indoor air quality has a direct association with outdoor air quality (Godish 2004) and some previous studies (Koponen et al. 2001; Sawant et al. 2004) have evaluated the degree of contribution by the inflow of particulate matter from outdoor sources (Jones 1999). Similarly, exposure to the ambient environment surrounding schools, including vehicles, industry complexes, gas/oil stations, and commercial facilities, is a very important factor in the health of elementary students. In particular, traffic-related pollutants are critical contributors to the atmospheric pollution of urban areas (Keuken et al. 2005). Generally, the duration of the elementary school day ranges between 5 and 8 h (INCA 2009). In addition to 2 to 3 h spent on the school grounds and on the roads (Leickly 2003; Cleland et al. 2009).
Recently, a published report found that children who lived near roads where traffic jams frequently occurred were more likely to develop asthma (HEI 2010). In addition, previous studies have also consistently reported that black carbon (BC), which is recognized as a vehicular pollutant, has a positive relationship with respiratory diseases (Brauer et al. 2007; Wichmann et al. 2005). Previous studies have identified that vehicular combustion compounds cause serious health risks and children experience more harmful health effects than adults even if they are exposed to an equal level of atmospheric pollution (Kulkarni and Grigg 2008; WHO 2005). In addition, school buses in the USA produce exhaust pollutants such as diesel particulate matter (DPM) and BC, both of which have been identified as potential causes of asthma in sensitive children (Richmond-Bryant et al. 2009, 2011). Previous studies have also categorized local atmospheric quality into traffic-related pollutants and other unidentifiable pollutants (English et al. 1999; Lin et al. 2002).
Most studies make assessments based on the actual prevalence of allergic diseases using International Study of Asthma and Allergies in Childhood (ISAAC) questionnaires (Strachan et al. 1997; Suh et al. 2011). These questionnaires enable the identification of past and current state of diseases such as atopy, asthma, rhinitis, and conjunctivitis. They also help to identify the association between hereditary factors and environmental factors (Mutius et al. 1995), and are utilized in studies that assess the relationship between allergic diseases and indoor/outdoor environmental pollution (Ho et al. 2007; Zhao et al. 2008).
In this study, we categorized schools into those exposed to environmental traffic pollutants, those located in residential areas, and those exposed to complex pollution (traffic + others) based on an assessment of the surrounding environment. We then identified the current status of allergic diseases in children who commute to and from the schools using ISAAC questionnaires.
Materials and methods
Monitoring overview
This study was designed as a cross-sectional study centred on elementary schools and school zones in the four cities of Seoul, Daejeon, Incheon, and Siheung by classifying the around-school characteristics in order to study the association between environmental pollution and allergic diseases.
Seoul is the capital of the Republic of Korea with a population of 10,530,000 people and it is the center of the Korean economy, culture, and politics. Daejeon is a metropolitan city located in the middle of Korea, with a population of about approximately 1,500,000 people and it represents the provincial headquarters. Incheon is a city neighbouring Seoul and is a Sudogwon (sub-capital region) metropolitan city located in the mid-west region of Korea with a population of approximately 2,500,000 and with outer ports housing machinery- and metal-based industrial complexes. Siheung is a complex industrial city with a population of approximately 400,000that contains the Sihwa National Industrial Hub.
The following pollutants were evaluated in this study: BC, PM10, SO2, NO2, CO, and O3, which have also been evaluated in previous studies on allergic diseases (Raysoni et al. 2011; Zhao et al. 2008). For individual allergic disease and family factors of children, information was collected from individual questionnaires.
In addition, this study used three categories based on prior traffic counts for the classification of schools according to the surrounding characteristics. The detailed classifications were as follows: S1 is the school with no traffic-related or other pollutant sources; S2 is the school located in front of a bus exclusive lane; S3 is the Seoul inner ring road and vehicle-only road; S4 is the school near highways and IC and it also has complex pollutant sources; S5 is the school near an industrial complex (green belt is not included); S6 is the school near an industrial complex (green belt is included); and S7 is the school with complex pollution caused by traffic-related and topical pollutants.
Field site selection
Prior traffic counts were performed for classification of the schools near residential areas. For the mean in-use vehicle counts inside school zones, the day volume proportions (proportion of 12 h daytime against 24 h traffic counts) were investigated. The traffic counts were performed from 8:00 a.m. to 7:00 p.m. using video cameras. This study conducted traffic counts at 15 min intervals and the results were presented in an hourly manner. The types of vehicles subjected to traffic counts by each measuring point were investigated and classified into eight different types according to their purpose, external size, riding/loading capacity, and function/structure.
Study locations
Hometown zone (S1)
This zone includes schools located to the north of downtown Seoul surrounded by residential areas and green belts situated at the rear of the school (Fig. 1a). It has lower traffic volume because there are no vehicle-only roads within 500 m (Table 1). Environmental contamination was measured at three different points: the main access for children, the school grounds, and one major school route for children.

The location of the target elementary school. a Home town zone (S1). b Traffic related zones (S2, S3, S4). c Related complex source zones (S5, S6, S7)
Traffic-related zones (S2, S3, S4)
The S2 category elementary schools are located among the traffic-related pollution areas, including schools located at the north side of downtown Seoul, where six-lane, two-way roads and side streets exist near the school with the co-existence of commercial business facilities and residential areas (Fig. 1b). The bus exclusive lanes and vehicle-only roads in front of the main gates of the schools cause frequent traffic and vehicular idling. Environmental contamination was measured at three different points: the main access for children, the school grounds, and one major school route for children.
The S3 category elementary school is located at the north side of downtown Seoul, where a beltway exists together with a six-lane, two-way road, commercial business facilities, and a residential area under the beltway (Fig. 1b). The street in front of the school’s main gate is very narrow, and thus, is very crowded during the school rush with frequent traffic and vehicular idling. The overhead beltway in front of the school’s rear gate has a high traffic volume with frequent traffic and vehicular idling. Environmental contamination was measured at three different measuring points: the main access for children, the school grounds, and one major school route for children.
The S4 elementary school is located near Daejeon IC in the Chung Cheong Nam-Do (Province) where the Gyeongbu express highway is present at the rear of the school and where public bus garages and a residential area are located (Fig. 1b). The street in front of the school’s main gate is narrow; however, traffic volume is moderate except during the school rush, resulting in less exposure to pollution. Nevertheless, the S4 school has characteristics associated with traffic-related pollution as has an express highway with IC nearby. Environmental contamination was measured at three different points: the main access for children, the school grounds, and one major school route for children.
Related complex source zones (S5, S6, S7)
The S5 school is among the complex pollution areas located at the south-east side of the city of Incheon within the capital region and the Nam-dong industrial complex is within 100 m. There are six-lane, two-way roads and side streets that are located near commercial business facilities and residential areas (Fig. 1c). There is a vehicle exclusive road in front of the school’s main gate, but the traffic volume is only moderate. Environmental contamination was measured at three different measuring points: the main access for children, the school grounds, and one major school route for children.
The S6 school is located in the city of Siheung city in Gyeoggi-do within Sudogwon (the Capital Region) and the Sihwa Industrial Complex is within 300 m. There are a six-lane, two-way road and side streets that are located near commercial business facilities and residential areas. The difference between the S6 and S5 zones is the existence of a green belt between the industrial complex and the school (Fig. 1c). There is a vehicle exclusive road in front of the school’s main gate, but the traffic volume is only moderate. Environmental contamination was measured at three different measuring points: the main access for children, the school grounds, and one major school-route for children.
The S7 school is located at the north side of downtown Seoul where small-scale steel and manufacturing facilities are within 100 m. There is a six-lane, two-way road within 300 m of the school with co-existence of commercial business facilities and residential area (Fig. 1c). The street in front of the school’s main gate is narrow; however, traffic volume is low except during school, so exposure to traffic-related pollution is insignificant. Environmental contamination was measured at three different points: the main access for children, school grounds, and one major school-route of children.
Experimental methods
Environmental contamination was measured by real-time monitoring from June 8, 2011 to October 6, 2011, over a 12-h period (07:30 to 19:30) at 21 locations inside the seven school zones. The sampling periods in the school main entrance and school zones were 3 days (1 site/day) per school. The pollutants of interest were PM10, SO2, NO2, CO, O3 (average of minutely measurements), and BC (average of minutely measurements) and were measured at each measuring point using the on-site automatic test method as prescribed by the Standard Methods for the Examination of Air Pollution. The concentrations of the pollutants were analyzed.
The β-ray absorption method (TAPI, Beta-Attenuation Mass Monitor, Model BAM1020) was used as a measuring method of PM10, which collected airborne nanoparticles ≤ 10 μm on a filter over a period of 12 h. β-Rays were then passed through the filter in order to calculate the mass concentration of nanoparticles. A pulse UV fluorescence method (TAPI, UV Fluorescence Analyzer, Model 100E) was used in order to measure the real-time SO2 concentration in the atmosphere. Chemiluminescence was used to measure NO2 (TAPI, Chemiluminescence Analyzer, Model 200E). This measurement occurs by analyzing the light created when NO2 is generated from the reaction with ozone after NO2 is converted in the air to NO. UV absorption was used to measure BC concentrations, which indicated the real-time concentration of ozone (O3; TAPI, UV Absorption Analyzer, Model 400E) in the environmental atmosphere by measuring the variation in the volume of UV absorption near 254 nm. A portable aethalometer (Magee Scientific, Model AE42-7-ER-MC; Kanaya et al. 2008; Latha and Badarinath 2003; Richmond-Bryant et al. 2009, 2011) was used to measure the BC concentrations, which converted the attenuation degree of seven different wavelengths (370, 470, 520, 590, 660, 880, and 950 nm) into the mass concentration per wavelength according to the particles collected on a quartz filter (Richmond-Bryant et al. 2009; 2011). The measurements were performed for 11 h (08:00 to 19:00) after ensuring that the preliminary operation was performed sufficiently.
ISAAC questionnaire
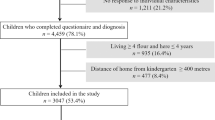
For the assessment of asthma and allergic diseases, we utilized the ISAAC questionnaire (Lee et al. 2005; Zhao et al. 2008) based on question items that were verified for reliability and feasibility. It was requested that all of the questionnaires be answered by students and parents together. The survey was performed during the period from June to October 2011. In total, 6,031 students in grades 2–6 at the seven chosen schools participated and 4,793 students responded to the questionnaire (retrieval rate 79.5 %). The first grade students were excluded from the evaluation since they had a relatively short exposure time due to their school route and living activities. Finally, the results of the questionnaire in regards to the prevalence of asthma, allergic rhinitis, and atopic dermatitis were classified into lifetime symptoms, symptoms, diagnosis, and status in the past 12 months by each disease.
Statistical methods
The relationships between allergic diseases and air pollution concentrations were assessed by using single-pollutant models. Each of the lifetime symptoms, symptoms in the previous 12 months, and treatment experiences in the previous 12 months identified by the questionnaire in connection with asthma, allergic rhinitis, and atopic dermatitis was designated as a dependent variable. The independent variables included pollution concentrations. Individual characteristics and known risk factors for allergic diseases were designated as potential confounder (age, gender, household income, exposure to indirect smoking, housing type, construction year, and presence/absence of water leakage).We obtained the odds ratios (ORs) relating allergic diseases to air pollution, after adjusting for individual-level risk factors. ORs with 95 % confidence interval (95 % CIs) were applied. We calculated adjusted OR s for a change in measured pollution concentration equal to the interquartile ranges of the pollution distribution (Kim et al. 2004). Predictive Analytics Software (PASW) version 20.0 was used for all statistical analyses. Statistically significance was provided by a p value < 0.05.
Results
Prior traffic counts
For the major streets adjacent to the elementary schools that were studied and for those schools with no facilities that presented a concern for environmental contamination, the vehicular running volume along the main school route was measured from 8:00 a.m. until 7:00 p.m. The measured data were classified by hour as presented in Table 1.
When analyzing the traffic counts by hour (8:00 and 9:00) when school and work rush hours overlapped, passenger vehicles were identified as the most common vehicle. However, the hour at which school ends was slightly different and was dependent on grade, but the passenger vehicle was still the most common vehicle between 1:00–3:00 p.m. In the case of the S4 school (express highway and IC), the traffic counts were measured on the street in front of the main gate of the school as well as on the nearby streets. The measured traffic count on the express highway was determined to be 75,435 vehicles based on the results of the annual average 24-h road traffic count survey by The Ministry of Land, Transport, and Maritime Affairs in 2010.
Air pollution measurements
The degrees of atmospheric pollution of the school routes around the schools (school zone) that were investigated in this study were presented in Table 2. The concentration of PM10 was the highest at 67.9 μg/m3 at the S2 location (bus exclusive road), where traffic-related pollutant sources were present. The highest level of BC was identified at S6 (School inside industrial complex and residential area) with a mean concentration of 10.98 μg/m3, followed by S5 (school near industrial complex) with a concentration of 6.91 μg/m3. Therefore, the contamination levels at the schools located near industrial complex areas were determined to be higher than the schools with the traffic-related pollutant sources (i.e., S2, S3, and S4). In addition, the S1 school with no traffic-related or other pollutant sources showed very low traffic count compared to the other six school zones. However, between the school and work rush hours of 8:00 a.m. and 9:00 p.m., the actual measurement indicated a concentration of 13.58 μg/m3 (Fig. 2). The mean levels of SO2, NO2, CO, and O3 were determined to be 0.005, 0.031, 0.28, and 0.035 ppm, respectively, but no clear difference based on the contamination source was observed.


Black carbon (BC) concentration (ng/m3) for all series sampling times. a S1 the school with no traffic-related or other pollutant sources. b S2 school located in front of a bus exclusive lane. c S3 Seoul inner ring road and vehicle-only road. d S4 school near to highways and I.C. and with complex pollutant sources. e S5 school near an industrial complex (green belt is not included). f S6 school near an industrial complex (green belt is included). g S7 school with complex pollution caused by traffic-related and topical pollutants
Questionnaire data
The survey was completed by 4,793 students from 7 schools and the final analysis results from 4,545 students, excluding 248 students whose survey results were ambiguous, were presented in Table 3.
The general characteristics of the participants indicated that 51.1 % were girls and those living in apartment and terraced houses represented 65.1 % and 26.7 % of the total sample, respectively. In addition, 24.9 % of the children had experienced exposure to indoor, indirect smoking. The age of currently occupied housing was between 10 and 20 years (55.9 %), between 5 and 10 years (20.0 %), and 6.7 % of the children resided in newly constructed housing. Those who experienced water leakage in their residence within the last 3 years were determined to be 15.3 %. The incidence of lifetime symptoms of asthma, allergic rhinitis, and atopic dermatitis was11.1 %, 37.8 %, and 22.3 %, respectively.
Associations between air pollution and allergic diseases
A regression analysis was performed in order to identify the association between atmospheric pollution levels based on the characteristics around schools and symptoms of asthma, allergic rhinitis, and atopic dermatitis. Corrections were made for the age, gender, household income, exposure to indirect smoking, housing type, construction year, and presence/absence of water leakage (Tables 4, 5, and 6).
The major outcomes associated with symptoms of asthma are presented in Table 4. Although none of the atmospheric pollutants showed a statistically significant correlation with incidence of asthma symptoms or its treatment during the previous year, the odds ratios of the concentrations of pollutants were as follows: 1.15 (95 % CI, 0.96–1.39) per increase of 15.0 μg/m3 for PM10, 1.04 (95 % CI, 0.92–1.17) per increase of 2.8 μg/m3 for BC, and 1.05 (95 % CI, 0.89–1.29) per increase of 0.002 ppm for SO2, which all indicated positive correlations. NO2 and O3 did not show any significant odds ratios of symptomatic experiences as the mean concentrations of both had increased. Although there was no statistically significant association, the pattern in the odds ratios of PM10 (1.17, 95 % CI 0.90–1.53) and NO2 (1.06, 95 % CI 0.90–1.24) was due to exposure to vehicle-related pollution and in the odds ratio of NO2 (1.05, 95 % CI 0.74–1.50) was due to exposure to complex pollution. Regarding the incidence of asthma-induced treatment in the last year, BC (1.10, 95 % CI 0.94–1.28), SO2 (1.11 95 % CI 0.86–1.44), and NO2 (1.04, 95 % CI 0.90–1.21) showed positive correlations. In the case of NO2, its odds ratio increased both for the area exposed to vehicle-related pollution and the area exposed to complex pollution.
The major outcomes associated with the symptoms of allergic rhinitis are presented in Table 5. When symptoms were experienced within the previous year, there were significant differences in the levels of BC, SO2, and O3, while there was a significant difference in the level of O3 for treatment experiences. Among them, the odds ratio of symptomatic experiences per increase of 0.01 ppm of O3 was 1.09 (95 % CI, 1.03–1.15), while the odds ratio of treatment experiences was 1.23 (95 % CI, 1.16–1.30), indicating that the odds ratio increased with statistical significance. In the case of treatment experiences for allergic rhinitis in participants from the area exposed to complex pollution in the previous year, the odds ratios of BC (1.29, 95 % CI 1.16–1.43) and SO2 (1.30, 95 % CI 1.09–1.56) increased with statistical significance.
The major outcomes associated with symptoms of atopic dermatitis are presented in Table 6. It was determined that the odds ratio of symptomatic experiences per increase of 0.01 ppm of O3 was 1.10 (95 % CI, 1.02–1.18), which supports previous findings. The participants from the areas exposed to vehicle-related pollution had increased odds ratios in both symptomatic and treatment experiences for atopic dermatitis from PM10, BC, and O3 within 1 year. However, no statistically significant difference was noted. The participants from the area exposed to complex pollution had increased odds ratios for both symptomatic and treatment experiences for 1 year based on the levels of BC and SO2.
The odds ratios of the symptomatic and treatment experiences in connection with the allergy-related diseases by group were compared based on the hometown zone (S1; Fig. 3). In the case of asthma (a), based on the school with no traffic-related and other pollutant sources (S1), the odds ratios of treatment experiences (within 1 year) in the school group with traffic-related pollutant sources (S2, S3, and S4), as well as the schools with complex pollutant sources (S5, S6, and S7) were 2.12 (1.41–3.19) and 1.59 (1.06–2.37), respectively. These results indicate that the risk was raised in comparison to the students in S1. In the case of allergic rhinitis (b), based on the school with no traffic-related and other pollutant sources (S1), the odds ratios of treatment experiences (within 1 year) in the school group with traffic-related pollutant sources (S2, S3, and S4) and the school group with complex pollutant sources (S5, S6, and S7) were 1.30 (1.11–1.52) and 1.72 (1.46–2.02), respectively. These results indicated that the risk was raised in comparison to the students in S1. In the case of atopic dermatitis (b), based on the school with no traffic-related and other pollutant sources (S1), the odds ratios of treatment experiences (within 1 year) in the school group with complex-polluted sources (S5, S6, and S7) was 1.42 (1.02–1.97). These results indicated that the risk was raised in comparison to the students of S1.

The odds ratios of symptomatic and treatment experiences in connection to the allergy-related diseases by group were compared based on home town zone. a Asthma. b Allergic rhinitis. c Atopic dermatitis
Discussion
The US Environmental Protection Agency (EPA 2010) recommends standard levels of CO, ozone, SO2, NO2, PM10, and PM2.5 in its national air quality standards. Existing studies related to the school environment and traffic (Brunekreef et al. 1997; Guo et al. 2008; Peacock et al. 2003; Rijnders et al. 2001; Van Roosbroeck et al. 2008) have also reviewed the association between the degree of contamination and allergies, as well as the connection between respiratory diseases and CO, ozone, SO2, NO2, and PM. In addition, the World Health Organization (WHO 2005) suggests the same air quality guideline values.
The mean concentration of PM10 around schools as determined in this study was 70.6 μg/m3, which is lower than Korean atmosphere environmental standard (24 h, 100 μg/m3) and the EPA standard value (24 h, 150 μg/m3), but it exceeded the standard value suggested by WHO (AQG value; 24 h, 50 μg/m3). The PM10 concentration of this study was higher than that reported in a study conducted in France, which was 40.6 μg/m3 (Penard-Morand et al. 2005), but lower than the concentration reported in a study conducted in Greece, which was 166 μg/m3. The mean concentration of NO2 was 0.031 ppm (31 ppb), which was lower than Korean atmosphere environmental standard (1 h, 100 ppb) and the EPA standard value (1 h, 100 ppb, 188 μg/m3) and that suggested by the WHO (AQG value; 1 h, 200 μg/m3). This was slightly higher than the 16.5 ppb reported by Peacock et al. (2003), and the 19.0 and 26.0 ppb reported by Singer et al. (2004), but similar to the results of a study conducted in China that reported between 53 and 73 μg/m3. The mean concentration of ozone was 0.035 ppm (35 ppb), which was lower than the Korean, EPA, and WHO standard values (8 h, 0.06 ppm; 8 h, 0.075 ppm; AQG value, 8 h, 100 ug/m3, respectively). This result was slightly higher than the results from the study conducted in England, which were between 17.1 and 19.2 ppb (Peacock et al. 2003), but was lower than the results from the study conducted in the USA (Rundell et al. 2006) at 0.33 ppm. The mean concentration of CO was 0.28 ppm (280 ppb), which was lower than Korean atmosphere environmental standard (8 h 9 ppm) and the EPA standard value (8 h, 9 ppm, 10 mg/m3). This result was slightly higher than that of the study conducted in the USA, which was <100 ppb (Rundell et al. 2006), but lower than the results of the study conducted in Pakistan (Ali and Athar 2008) at 0.33 ppm. The mean concentration of SO2 was 0.005 ppm, which was lower than the EPA standard value (24 h, 0.14 ppm) and the standard suggested by the WHO (AQG value, 20 μg/m3/24 h).
In this study, the symptomatic experiences within the last year in connection with the symptoms of allergic rhinitis were identified as having significant differences from BC, SO2, and O3, while the treatment experiences were identified as having significant differences from O3 only. In particular, the odds ratios of BC and SO2 were identified as having statistically significant increases for the treatment experiences of participants during the previous year from the area with complex pollution in connection with allergic rhinitis. The large scale research of Annesi-Maesano et al. (2007) had identified that, in the case of primary school children, the level of PM2.5 was 1.09 (0.93, 1.27) and the level of NO2 was 1.08 (0.92, 1.27) for lifetime allergic rhinitis and suggested the possible association with the disease, although the findings were not statistically significant.
For the association with the symptoms of atopic dermatitis, the odds ratio for the symptomatic experiences in connection with O3 was increased, which was statistically significant. Nevertheless, Annesi-Maesano et al. (2007) reported that atopic dermatitis had no association with PM2.5 or NO2. Variations in findings might be due to exposure misclassification in these studies (Annesi-Maesano et al. 2007) and the cross-sectional study design limits the possibility of results based on causal relationships (Zhao et al. 2008).
On the other hand, there was no atmospheric pollutant substance that presented a statistically significant correlation with symptomatic or treatment experiences within the last year in connection with asthma in this study, but the study showed that there were positive correlations with PM10, BC, and SO2. Kim et al. (2004) studied the respiratory system of children near traffic on a busy road and reported that the odds ratios associated with PM10, BC, and NO2 in all of the participants were 1.06 (0.97, 1.16), 1.07 (0.98, 1.17), and 1.06 (0.99, 1.13), although those values were not statistically significant. Such results were consistent with the results of this study in connection with PM10 and BC. However, Zhao et al. (2008) reported that asthmatic symptoms were associated with indoor air pollutants rather than the outdoor atmosphere.
The results obtained by different studies can be differ depending on the scale of the study, its design, the measured substances, the measuring time, the monitoring locations, and the study methods. A number of previous studies have reported positive associations of traffic-related pollutants with various respiratory and pulmonary symptoms (Janssen et al. 2003; Kramer et al. 2000; Lin et al. 2002; Weiland et al. 1994). From the results of this study, when assessing the symptomatic experiences for allergic rhinitis and atopic dermatitis, BC was identified as having an association, although it was not a statistically significant.
BC is a component of the exhaust from the incomplete combustion of diesel fuel (Raysoni et al. 2011; Sarnat et al. 2010). Diesel particles have been shown to enhance inflammatory reactions and sensitization (Mastrangelo et al. 2003). In the present study, the mean concentration of BC was 5.78 (3.21–11.48), which was higher than the value of 2.4 μg/m3 measured in close proximity to a school by Patel et al. (2009) and the values between 3.8 and 4.9 μg/m3 (n/a-8.4) measured by Richmond-Bryant et al. (2009).
However, there were some limits to our study as the previous studies by Richmond-Bryant et al. (2009 and 2011) were the result of continuous measurement for 2 months, while this study measured pollutants during a short period (3 days) of time. Such a limitation was significant inverse associations between air pollution and allergic diseases. The hourly exposure characteristics of BC by school indicated that S1 had less traffic on a daily basis than the other school zones (S2–7; Table 1). However, between the hours of 8:00 a.m. and 9:00 a.m., which were the school and work rush hours, the maximum BC concentration was 13.58 μg/m3. S2 and S3 were in school zones with traffic-related pollutant sources, at which the level of BC had increased steadily regardless of the hour due to bus exclusive lanes as well as vehicle-only roads. Nevertheless, among those school zones with traffic-related pollutant sources, S4, which was located near the Express Highway had a BC level of 4.40 (1.18–11.07) μg/m3, which was not the expected level, but it was a similar concentration (4.52 μg/m3) and matched the hour range-specific characteristics (Fig. 3). Patel et al. (2009) reported that their result exceeded 2.4 μg/m3, which was measured near a large highway, but Richmond-Bryant et al. (2009) reported that a school zone in their study had a maximum BC value of 8.4 μg/m3 (average 4.9 μg/m3). The BC particulate pollutants were identified as being associated with a broader range of traffic and industrial sources (John et al. 2007). In this study, S5 and S6 were located in an industrial region and, due to the locality characteristics, it was determined that the degree of contamination was induced by diesel vehicles related to industrial activity and such traffic-related pollution reflecting mobile contamination sources could not be controlled by the green belt of S6.
The USA has been trying to reduce the emission of harmful substances such as NO2 and particulate matter by installing new engine ventilation devices and filters on school buses starting in 2003 (Richmond-Bryant et al. 2009). All the schools included in this study were public elementary schools established by the government and the students were residing in nearby residential areas from where they could walk. Therefore, there was no additional exposure caused by school buses. In Korea, only some of the private elementary schools operate school buses.
Also based on the results of the survey in this study, it was determined that 24.9 % of all participants had experienced exposure to indirect smoking and such exposure had an effect on the incidence of allergic disease. Zhao et al. (2008) pointed out that environmental tobacco smoke (ETS) is a critical risk factor that has effects on the respiratory symptoms of children, while a number of other studies report a similar association (Hugg et al. 2007; Tanaka et al. 2007). The OR estimates for asthma in children from families in which either parent smoked compared with children of non-smoking parents were consistently above 1 (Perter et al. 1996; Lam et al. 1999). Smoke-free home rules and other home smoking restrictions may be implemented for a variety of reasons, including to protect children in the household from second-hand smoke exposure (CDC 2006). The American Legacy Foundation also launced a media initiative in 2005 to promote smoke-free homes and vehicles (American Legacy Foundation 2005).
In this study, we came to the partial conclusion that the risk of allergic disease in children can be increased by exposure to complex pollution, including traffic-related pollutant sources and the existence of industrial complexes. Although the results of this study differed somewhat from previous studies in terms of the associations between individual symptoms, as well as diseases and substances, it carries significance as a large-scale study. The prevalence of “wheeze, last 12 months” was 3.6 % and the prevalence of “allergic rhinitis, last 12 months” was 31.9 % in this study. Suh et al. (2011), which utilized the same methods to our study formulated by the ISAAC study, were conducted on elementary schools located in Seoul and major cities in Korea (427 elementary schools, 31,026 subjects). The prevalence in boys and girls was mostly similar (“wheeze, last 12 months” was 4.8 % and the prevalence of “allergic rhinitis, last 12 months” was 32.9 %).
Variation measurement of the representative air quality for each school is very important in the scale of this study (Mejia et al. 2007). The data from the automatic monitoring system installed to applicable schools is not representative of all of the schools because the data were obtained by remote monitoring. Therefore, although the results were derived from three locations selected as representative locations, our study findings are limited to the short measuring times (3 days/school), measuring periods and sample sizes per school. At least, should have performed longer sampling periods and used a fixed between-site effect to correct the temporal variability due to the fact that sampling was performed simultaneously at all locations. Because of the relationships between allergic diseases and air pollution, concentrations were assessed by using single pollutant models in this study.
Also, since children do not stay in one place while at school, but instead they move around to different places including the school-route, grounds, classrooms, and laboratories, this study could not perform individual exposure assessments using school indoor contamination data (Diapouli et al. 2008; Mi et al. 2006; Zhao et al. 2008) or personal exposure monitors (PEMs) (Buthbumrung et al. 2008; Van Roosbroeck et al. 2006). A more extensive study would be required in order to make those assessments through a more evolved study design.
In addition, this study cannot determine causal relationships because it was cross-sectional in design and failed to perform a comprehensive assessment of multiple confounding variables (exposure to indoor smoking, duration of residence, genetic effects, mould, pests, climate, diet, food product and social-cultural factors) that are known to be related to allergic diseases (Annesi-Maesano et al. 2007; Kim et al. 2004; Zhao et al. 2008).
In school zones in Korea, people are encouraged to drive less than 30 km/h on the roads located within 500 m of schools. In addition, a policy has been established for designation of a school environment and hygiene purification district in order to prevent any environmental contamination resulting from facilities being located around a school, but the policy is not followed completely. Baldauf et al. (2009) state that near-road concentrations of traffic-generated pollutants generally return to background levels within 200–500 m from the source. Therefore, the school zone requires reinforcement not only in terms of safety from traffic accidents, but also in terms of the protection of children’s health and the control of environmental contamination for a school zone as a major space where children are present.
Conclusions
The objectives of this study were to perform an ISAAC Questionnaire Survey among elementary school students applicable depending on the environmental conditions of the elementary schools and to make assessments on a relationship between air pollution and allergic diseases, as designed as a cross-sectional study.In this study, seven elementary schools were selected and they were classified into three categories. The schools selected included one school with no traffic-related and other pollutants, three with traffic-related pollutants, and three with traffic-related and complex pollutants.
There were significant association in the risks as determined by the odds ratios of treatment experiences (within 1 year) for allergy-related diseases such as asthma and allergic rhinitis in the school group with traffic-related pollutants and the school group with complex pollutants. These results were determined by comparing the odds ratios of symptoms and treatment experiences for allergy-related diseases by group based on the hometown zone (S1) as a reference. Also, in case of atopic dermatitis, the odds ratio of treatment experiences (within 1 year), which indicated an elevation in the risks in comparison with the students in the S1 school. The BC and SO2 of the complex pollution areas (industrial pollution + traffic-related pollution) showed a significant increase in the odds ratio based on the results of the regression analysis of the relationship between the substances and symptomatic experiences associated with allergic rhinitis for the last year. The odds ratio of the O3 increased with statistical significance based on the result of the assessment of its relationship with atopic dermatitis-associated symptoms. Both particulate pollution including BC and well known pollutants from traffic-related exhaust from tailpipes emissions as well as SO2, NO2, and O3, were found to be associated with allergic diseases in children.
Not only particulate pollutions including BC, well-known traffic-related exhaustion pollutant but also SO2, NO2, and O3, which were the pollutants emitted from industrial sources, directly or indirectly, had association with allergic diseases in children. Thus, it requires strategies and actions to be taken for protecting childhood health in school zones.
References
Ali M, Athar M (2008) Air pollution due to traffic, air quality monitoring along three sections of National Highway N-5. Pakistan. Environ Monit Assess 136:219–226
American Legacy Foundation (2005) More than 13 million American children regularly breathing secondhand smoke in their homes, cars: American Legacy Foundation and Ad Council launch first campaign to call attention to and educate public about dangers of secondhand smoke (press release). American Legacy Foundation, Washington, January 11
Annesi-Maesano I, Moreau D, Caillaud D, Lavaud F, Moullec YL, Taytard A, Pauli G, Charpin D (2007) Residential proximity fine particles related to allergic sensitisation and asthma in primary school children. Respir med 101:1721–1729
Baldauf R, Watkins N, Heist D, Bailey C, Rowley P, Shores R (2009) Near-road air quality monitoring: factors affecting network design and interpretation of data. Air Qual Atmos Health 2:1–9
Brauer M, Hoek G, Smit HA, de Jongste JC, Gerritsen J, Postma DS, Kerkhof M, Brunekreef B (2007) Air pollution and development of asthma, allergy and infections in a birth cohort. Eur Respir J 29:879–888
Brunekreef B, Janssen NAH, de Hartog J, Harssema H, Knape M, van Vliet P (1997) Air pollution from truck traffic and lung function in children living near motorways. Epidemiology 8:298–303
Buthbumrung N, Mahidol C, Navasumrit P, Promvijit J, Hunsonti P, Autrup H, Ruchirawat M (2008) Oxidative DNA damage and influence of genetic polymorphisms among urban and rural schoolchildren exposed to benzene. Chem Biol Interact 172:185–194
Canha N, Almeida M, Freitas MDC, Almeida SM, Wolterbeek H, Wolterbeek T (2011) Seasonal variation of total particulate matter and children respiratory diseases at Lisbon primary schools using passive methods. Procedia Environ Sci 4:170–183
Carlisle AJ, Sharp NCC (2001) Exercise and outdoor ambient air pollution. Br J Sports Med 35:214–222
CDC (Centers for Disease Control and Prevention) (2006) The health consequences of involuntary exposure to tobacco smoke: a report of the Surgeon General. U.S. Dept. of Health and Humans Services, Centers for Diseases Control and Prevention, Coordinating Center for Health Promotion, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, Atlanta, Available: http://www.surgeongeneral.gov/library/secondhandsmoke/
Cleland V, Timperio A, Salmon J, Hume C, Baur LA, Crawford D (2009) Predictors of time spent outdoors among children: 5-year longitudinal findings. J Epidemiol Community Health. doi:10.1136/jech.2009.087460
Diapouli E, Chaloulakou A, Mihalopoulos N, Spirellis N (2008) Indoor and outdoor PM mass and number concentrations at schools in the Athens area. Environ Monit Assess 136:13–20
Dockery DW, Cunningham J, Damokosh AI, Neas LM, Spengler JD, Koutrakis P, Ware JH, Raizenne M, Speizer FE (1996) Health effects of acid aerosols on North American children: respiratory symptoms. Environ Health Perspect 104:500–505
English P, Neutra R, Scalf R, Sullivan M, Waller L, Zhu L (1999) Examining associations between childhood asthma and traffic flow using a geographic information system. Environ Heal Perspect 107:761–767
EPA (Environmental Protection Agency) (2010) (Online) Available: http://www.epa.gov/air/criteria.html. Accessed 16 June 2010
Godish T (2004) Air quality, 4th edn. Lewis, Boca Raton
Guo H, Morawska L, He C, Gilbert D (2008) Impact of ventilation scenario on air exchange rates and on indoor particle number concentrations in an air-conditioned classroom. Atmos Environ 42:757–768
Health Effects Institute (2010) Traffic-related air pollution: a critical review of the literature on emissions, exposure, and health effects. Health Effects Institute, Boston
Heindrich J, Schwarze PE, Stilianakis N, Momas I, Medina S, Totlandsdal AI, van Bree L, Kuna-Dibbert B, Kryzanowski M (2005) Studies on health effects of transport-related pollution. In: Krzyzanowski M, Kuna-Dibbert B, Schneider J (eds) Health effects of transport-related pollution. Regional Office for Europe of the World Health Organization (WHO), Copenhagen, pp 125–126
Hirsch T, Weiland SK, von Mutius E, Safeca AF, Grafe H, Csaplovics E, Duhme H, Keil U, Leupold W (1999) Inner city air pollution and respiratory health and atopy in children. Eur Respir J 14:669–677
Ho WC, Hartley WR, Myers L, Lin MH, Lin YS, Lien CH, Lin RS (2007) Air pollution, weather, and associated risk factors related to asthma prevalence and attack rate. Environ Res 104:402–409
Hugg TT, Jaakkola MS, Ruotsalainen RO, Pushkarev VJ, Jaakkola JJ (2007) Parental smoking behaviour and effects of tobacco smoke on children’s health in Finland and Russia. Eur J Pub Health 8(1):55–62
INCA (2009) INCA comparative tables (Online). International Review of Curriculum and Assessment Framework Internet Archive (INCA), London, Available: http://www.inca.org.uk/INCA-comparative_tables_September_2009.pdf (accessed 11.06.10)
Janssen NA, Brunekreef B, van Vliet P, Aarts F, Meliefste K, Harssema H, Fischer P (2003) The relationship between air pollution from heavy traffic and allergic sensitization, bronchial hyperresponsiveness, and respiratory symptoms in Dutch schoolchildren. Environ Health Perspect 111:1512–1518
John K, Karnae S, Crist K, Kim M, Kulkarni A (2007) Analysis of trace elements and ions in ambient fine particulate matter at three elementary schools in Ohio. J Air Waste Manag Assoc 57:394–406
Jones AP (1999) Indoor air quality and health. Atmos Environ 33:4535–4564
Kanaya Y, Komazaki Y, Pochanart P, Liu Y, Akimoto H, Gao J, Wang T, Wang Z (2008) Mass concentrations of black carbon measured by four instruments in the middle of central east china in June 2006. Atmos Chem Phys 8:7637–7649
Keuken M, Sanderson E, Aalst R, Borken J, Schneider J (2005) Contribution of traffic to levels of ambient air pollution in Europe. In: Krzyzanowski M, Kuna-Dibbert B, Schneider J (eds) Health Effects of Transport-related Air Pollution. European Office of the World Health Organization (WHO), Copenhagen, pp 53–54
Kim JJ, Smorodinsky S, Lipsett M, Singer BC, Hodgson AT, Ostro B (2004) Traffic-related air pollution near busy roads. The East Bay Children’s Respiratory Health Study. Am J Respir Crit Care Med 170:520–526
Koponen IK, Asmi A, Keronen P, Puhto K, Kulmala M (2001) Indoor air measurement campaign in Helsinki. Finland 1999—the effect of outdoor air pollution on indoor air. Atmos Environ 35:1465–1477
Kramer U, Koch T, Ranft U, Ring J, Behrendt H (2000) Traffic-related air pollution is associated with atopy in children living in urban areas. Epidemiology 11:64–70
Kulkarni N, Grigg J (2008) Effect of air pollution on children. Paediatr Child Health 18:238–243
Lam TH, Hedley AJ, Chung SF, Macfarlane DJ (1999) Child Health and Activity Research Group (CHARG). Passive smoking and respiratory symptoms in primary school children in Hong Kong. Hum Exp Toxicol 18(4):218–223
Latha KM, Badarinath KVS (2003) Black carbon aerosols over tropical urban environment—a case study. Atmos Res 69:125–133
Lee YL, Lin YC, Hwang BF, Guo YL (2005) Changing prevalence of asthma in Taiwanese adolescents: two surveys 6 years apart. Pediatr Allergy Immunol 16:157–164
Leickly FE (2003) Children, their school environment, and asthma. Ann Allergy Asthma Immunol 90:3–5
Lin S, Munsie JP, Hwang SA, Fitzgerald E, Cayo MR (2002) Childhood asthma hospitalization and residential exposure to state route traffic. Environ Res 88:73–81
Mastrangelo G, Clonfero E, Pavznerllo S, Fedeli U, Fadda E, Turato A, Piccinni S, Montagnani R, Marcer G (2003) Exposure to diesel exhaust enhances total IgE in non-atopic dockers. Int Arch Occup Environ Heal 76:63–68
McConnell R, Berhane K, Gililand F, London SJ, Vora H, Avol E, Gauderman WJ, Margolis HG, Lurmann F, Thomas DC et al (1999) Air pollution and bronchitic symptoms in Southern California children with asthma. Environ Health Perspect 53:241–247
McConnell R, Islam T, Shankardass K, Jerrett M, Lurmann F, Gilliland F, Gauderman J, Avol E, Kuenzli N, Yao L, Peters J, Berhane K (2010) Childhood incident asthma and traffic-related air pollution at home and school. Environ Heal Perspect 118(7):1021–1026
Mejia JF, Wraith D, Mengersen K, Morawska L (2007) Trends in size classified particle number concentration in subtropical Brisbane, Australia, based on a 5 years study. Atmos Environ 41:1064–1079
Mi YH, Norback D, Tao J, Mi YL, Ferm M (2006) Current asthma and respiratory symptoms among pupils in Shanghai, China: influence of building ventilation, nitrogen dioxide, ozone, and formaldehyde in classrooms. Indoor Air 16:454–464
Mutius E, Sherrill DL, Fritzsch C, Martinez FD, Lebowitz MD (1995) Air pollution and upper respiratory symptom in children from East Germany. Eur Respir J 8:723–728
Patel MM, Chillrud SN, Correa JC, Feinberg M, Hazi Y, Deepti KC, Prakash S, Ross JM, Levy D, Kinney PL (2009) Spatial and temporal variations in traffic-related particulate matter at New York City High Schools. Atmos Environ 43:4975–4981
Peacock J, Symonds P, Jackson P, Bremmer SA, Scarlett JF, Strachan DP (2003) Acute effects of winter air pollution on respiratory function in schoolchildren in southern England. Occup Environ Med 60:82–89
Penard-Morand C, Charpin D, Raherison C, Kopferschmitt C, Caillaud D, Lavaud F, Annesi-Maesano I (2005) Long-term exposure to background air pollution related to respiratory and allergic health in schoolchildren. Clin Exp Allergy 35:1279–1287
Perter J, Hedley AJ, Wong CM, Lam TH, Ong SG, Liu J, Sepiegelhalter DJ (1996) Effets of an ambient air pollution intervention and environmental tobacco smoke on children’s respiratory health in Hong Kong. Int J Epidemiol 25(4):821–828
Peters JM, Avol E, Navidi W, London SJ, Gauderman WJ, Lurmann F, Linn WS, Margolis H, Rappaport E, Gong H, Thomas DC (1999) A study of twelve Southern California communities with differing levels and types of air pollution: I: prevalence of respiratory morbidity. Am J Respir Crit Care Med 159:760–767
Raysoni AU, Sarnat JA, Sarnat SE, Garcia JH, Holguin F, Luevano SF, Li WW (2011) Binational school-based monitoring of traffic-related air pollutions in El Paso, Texas (USA) and Ciudad Juarez, Chihuahua (Mexico). Environ Pollut 159:2476–2486
Richmond-Bryant J, Bukiewicz L, Kalin R, Galarraga C, Mirer F (2011) A multi-site analysis of the association between black carbon concentrations and vehicular idling, traffic, background pollution, and meteorology during school dismissals. Sci Total Environ 409:2085–2093
Richmond-Bryant J, Saganich C, Bukiewicz L, Kalin R (2009) Associations of PM2.5 and black carbon concentrations with traffic, idling, background pollution, and meteorology during school dismissals. Sci Total Environ 407:3357–3364
Rijnders E, Janssen NAH, van Vliet PHN, Brunekreef B (2001) Personal and outdoor nitrogen dioxide concentrations in relation to degree of urbanization and traffic density. Environ Heal Perspect 109(3):411–417
Rundell KW, Caviston R, Hollenbach AM, Murphy K (2006) Vehicular air pollution, playgrounds, and youth athletic fields. Inhal Toxicol 18:541–547
Sarnat JA, Moise T, Shpund J, Liu Y, Pachon JE, Qasrawi R, Abdeen Z, Brenner S, Nassar K, Schauer JJ (2010) Assessing the spatial and temporal variability of fine particulate matter components in Israeli, Jordanian, and Palestinian cities. Atmos Environ 44:2383–2392
Sawant AA, Na K, Zhu X, Cocker K, Butt S, Song C, Cocker DR III (2004) Characterization of PM2.5 and selected gas-phase compounds at multiple indoor and outdoor sites in Mira Loma, California. Atmos Environ 38:6269–6278
Singer BC, Hodgson AT, Hotchi T, Kim JJ (2004) Passive measurement of nitrogen oxides to assess traffic-related pollutant exposure for the East Bay Children’s Respiratory Health Study. Atmos Environ 38:393–403
Strachan D, Sibbald B, Weiland S, Ait-Khaled N, Anabwani G, Anderson HR, Asher MI, Beasley R, Biorksten B, Burr M, Clayton T, Crane J, Ellwood P, Keil U, Lai C, Mallol J, Martinez F, Mitchell E, Montefort S, Pearce N, Robertson C, Shah J, Stewart A, von Mutius E, Williams H (1997) Worldwide variations in prevalence of symptoms of allergic rhinoconjunctivitis in children: the International Study of Asthma and Allergies in Childhood (ISAAC). Pediatr Allergy Immunol 8(4):161–176
Suh MN, Kim HH, Sohn MH, Kim KE, Kim CS, Shin DC (2011) Prevalence of allergic diseases among Korean school-age children: a nationwide cross-sectional questionnaire study. J Korean Med Sci 26:332–338
Tanaka K, Miyake Y, Arakawa M, Sasaki S, Ohya Y (2007) Prevalence of asthma and wheeze in relation to passive smoking in Japanese children. Ann Epidemiol 17(12):1004–1010
Van Roosbroeck S, Li R, Hoek G, Lebret E, Brunekreef B, Spiegelman D (2008) Traffic-related outdoor air pollution and respiratory symptoms in children: the impact of adjustment for exposure measurement error. Epidemiology 19:409–416
Van Roosbroeck S, Wichmann J, Janssen NAH, Hoek G, van Wijnen JH, Lebret E, Brunekreef B (2006) Long-term personal exposure to traffic-related air pollution among school children, a validation study. Sci Total Environ 368:565–573
Venn A, Lewis S, Cooper M, Hubbard R, Hill I, Boddy R, Bell M, Britton J (2000) Local road traffic activity and the prevalence, severity, and persistence of wheeze in school children: combined cross sectional and longitudinal study. Occup Environ Med 57:152–158
Weiland SK, Mundt KA, Ruckmann A, Keil U (1994) Self-reported wheezing and allergic rhinitis in children and traffic density on street of residence. Ann Epidemiol 4:243–247
Wichmann J, Janssen NAH, van der Zee S, Brunekreef B (2005) Traffic-related differences in indoor and personal absorption coefficient measurements in Amsterdam, the Netherlands. Atmos Environ 39:7384–7392
World Health Organization (WHO) (2005) WHO air quality guidelines global update. Report on a working group meeting. Born, Germany, 18–20 October 2005
Zhao Z, Zheng Z, Wang Z, Ferm M, Liang Y, Norback D (2008) Asthmatics symptoms among pupils in relation to winter indoor and outdoor air pollution in schools in Taiyuan, China. Environ Heal Perspect 116(1):90–97
Acknowledgments
This work was carried out with the support of “Research of Air Pollution at School Zone (2011)” of the National Institute of Environmental Research, Ministry of Environment, Republic of Korea.
Author information
Authors and Affiliations
Corresponding author
Additional information
Responsible editor: Philippe Garrigues
Rights and permissions
About this article
Cite this article
Kim, HH., Lee, CS., Jeon, JM. et al. Analysis of the association between air pollution and allergic diseases exposure from nearby sources of ambient air pollution within elementary school zones in four Korean cities. Environ Sci Pollut Res 20, 4831–4846 (2013). https://doi.org/10.1007/s11356-012-1358-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-012-1358-2