
Abstract
Ibuprofen is amongst the most worldwide consumed pharmaceuticals. The present work presents the first data in the occurrence of ibuprofen in Portuguese surface waters, focusing in the north area of the country, which is one of the most densely populated areas of Portugal. Analysis of ibuprofen is based on pre-concentration of the analyte with solid phase extraction and subsequent determination with liquid chromatography coupled to fluorescence detection. A total of 42 water samples, including surface waters, landfill leachates, Wastewater Treatment Plant (WWTP), and hospital effluents, were analyzed in order to evaluate the occurrence of ibuprofen in the north of Portugal. In general, the highest concentrations were found in the river mouths and in the estuarine zone. The maximum concentrations found were 48,720 ng L−1 in the landfill leachate, 3,868 ng L−1 in hospital effluent, 616 ng L−1 in WWTP effluent, and 723 ng L−1 in surface waters (Lima river). Environmental risk assessment was evaluated and at the measured concentrations only landfill leachates reveal potential ecotoxicological risk for aquatic organisms. Owing to a high consumption rate of ibuprofen among Portuguese population, as prescribed and non-prescribed medicine, the importance of hospitals, WWTPs, and landfills as sources of entrance of pharmaceuticals in the environment was pointed out. Landfill leachates showed the highest contribution for ibuprofen mass loading into surface waters. On the basis of our findings, more studies are needed as an attempt to assess more vulnerable areas.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
In the last years, pharmaceuticals have become a class of emerging contaminants in aquatic ecosystems which attracted an increasing concern (Richardson 2010). The presence of pharmaceuticals in the environment, even at sub-therapeutic concentrations (ng L−1–μg L−1), could represent a potential threat to public health (Daughton and Ternes 1999; Stackelberg et al. 2004). Excretion by humans and animals, disposal of unused medicines (out-of-date or unwanted) through the sink/toilet, hospital effluents, Wastewater Treatment Plants (WWTP), livestock, aquaculture, and pharmaceutical production facilities effluents have been pointed out as representative sources of continuous entrance of pharmaceuticals in the environment (Santos et al. 2010; USEPA 2006). In order to try to constrain the problem, European Union (EU) and U.S. Food and Drug Administration (FDA) authorities have established environmental risk assessment studies as a prerequisite to obtain marketing authorization for new medical products (Santos et al. 2010).
Ibuprofen, 2-(4-isobutylphenyl) propionic acid is a non-steroidal anti-inflammatory drug (NSAID) widely used when an inflammatory component is present and in the treatment of pain and fever (Méndez-Arriaga et al. 2008) due to its activity on the cyclooxygenase (COX) pathway. It has a large consumption rate, being the third most popular pharmaceutical in the world, with an annual global production reported in kilotons (Ali et al. 2009). Because of its wide usage, the worldwide occurrence of ibuprofen in the aquatic environment has been reported in several studies (Kim et al. 2007; Lin and Tsai 2009; Nakada et al. 2006; Pailler et al. 2009; Roberts and Thomas 2006; Thomas and Foster 2004; Verenitch et al. 2006; Weigel et al. 2004a). High contributions of hospital and WWTP effluents as contamination sources have been portrayed, with concentrations that could reach some hundreds of micrograms per liter (Hilton and Thomas 2003; Kosma et al. 2010; Lin et al. 2009; Verenitch et al. 2006). It is worth of mentioning that Spain reports one of the highest levels of contamination (Bueno et al. 2009; Gómez et al. 2007; Gómez et al. 2006; Hernando et al. 2006). Due to its high consumption rate combined with its high environmental detection and toxicity for aquatic organisms, given that the COX enzyme has a major role in the synthesis of eicosanoids, which are important regulators of reproduction in both vertebrates and invertebrates (Hayashi et al. 2008), it is expected that chronic exposure to ibuprofen in water environment could affect reproduction of aquatic animals (Flippin et al. 2007; Han et al. 2010). Therefore, in June 2010, the European Commission included ibuprofen in a shortlist of 19 possible new priority substances, and it is considering whether to set limits on the handful of this drug commonly found in aquatic ecosystems (SCHER 2011).
In what concern to Portugal, the increasing global consumption rate tendency has been followed and, according to the last available data of the Portuguese Medicine Regulatory Agency (INFARMED), ibuprofen consumption has been increasing during the last decade, moving from the 15th to 8th position in the sales ranking, with more than 2 millions of prescriptions in 2009 (INFARMED 2012). Besides medical prescription, ibuprofen can also be found in the Portuguese market as an over-the-counter (OTC) medicine, which increases even more its consumption at households. Up to now, there are just a few studies focused in environmental contamination by pharmaceuticals in Portugal, covering different water samples, namely hospital effluents (Pena et al. 2010; Seifrtova et al. 2008), WWTPs influents (Pena et al. 2010; Salgado et al. 2010; Seifrtova et al. 2008; Sousa et al. 2011; Teixeira et al. 2008) and effluents (Pena et al. 2010; Salgado et al. 2010; Seifrtova et al. 2008; Sousa et al. 2011), and river waters (Barreiro et al. 2010; Madureira et al. 2009; Madureira et al. 2010; Pena et al. 2007; Ribeiro et al. 2009a; Ribeiro et al. 2009b; Ribeiro et al. 2009c). Concerning ibuprofen, available data is very sparse and only embrace its occurrence in wastewaters (Salgado et al. 2010; Sousa et al. 2011).
In this context, ibuprofen monitoring studies in Portuguese aquatic environment are required, entailing different types of environmental samples. Since no data are available for surface waters, hospital effluent, and landfill leachate, particular attention needs to be paid to these types of samples. The aim of the present work was to develop an analytical methodology to evaluate the presence of ibuprofen in the aquatic environment in order to provide a first overview of the occurrence of ibuprofen in surface waters in north of Portugal. Douro river was used as a case study to understand how WWTP and hospital effluents, and landfill leachate contribute to the introduction of ibuprofen into surface waters.
Material and methods
Reagents, solvents, and materials
Acetonitrile, acetone, and methanol HPLC grade, formic acid (purity ≥98.0 %) were obtained from Merck (Darmstadt, Germany), glacial acetic acid (purity ≥99.7 %) and hydrochloric acid 37 % were obtained from Carlo Erba (Rodano, Italy), and sodium hydroxide (purity ≥98.0 %) was obtained from Panreac (Barcelona, Spain). Ibuprofen was purchased from Sigma-Aldrich (Steinheim, Germany).
Ultrapure water (18.2 MΩ cm; Millipore, Molsheim, France) was used for solid phase extraction (SPE) procedure and to prepare mobile phase in liquid chromatography.
A stock standard solution of ibuprofen was prepared by dissolving 2.3 mg of the powder in 10 mL of acetonitrile and stored at −20 °C. Working standard solutions were daily prepared from the stock standard solution using acetonitrile as solvent and kept at 4 °C prior to analysis. Amber glassware was used to prevent light degradation of ibuprofen.
All standard solutions and sample extracts were filtered through a 0.20-μm PTFE syringe filter (Teknokroma, Barcelona, Spain) and homogenized using a vortex mixer (Nahita 681/5, Navarra, Spain). All chromatographic solvents were filtered through a 0.20-μm nylon membrane filter (Supelco, Bellefonte, PA, USA) using a vacuum pump (Dinko D-95, Barcelona, Spain) and degassed for 15 min in an ultrasonic bath (Raypa® Trade, Terrassa, Spain).
Geographical characterization and sample collection
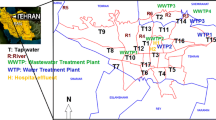
Twelve rivers, one stream, and one estuarine zone from north of Portugal (Fig. 1) were studied and they were characterized in Table 1.

Map of the study area and sample site localizations in the north of Portugal. R i river, T i Douro river tributaries, E Ria de Aveiro estuary, ET i Ria de Aveiro estuary tributaries, WWTP i wastewater treatment plant
Douro, Ave, Lima, Minho, and Leça rivers flow into the Atlantic Ocean nearby the cities of Porto/Vila Nova de Gaia, Vila de Conde, Viana do Castelo, Caminha, and Matosinhos, respectively. All these rivers pass through different regions that include densely populated areas, industrial poles, and large agricultural fields, which, as a whole, contribute to their pollution. Ria de Aveiro is an estuarine system in the northwest of Portugal formed by a complex system of channels and wide intertidal areas. It is connected to the Atlantic Ocean by an artificial inlet at the west side. The whole estuary is heavily influenced by human activities, including tourism, fishery and aquaculture, commercial harbors, agriculture, and industry. Rabaçal, Tinhela, Cabrum, Tâmega, and Uíma rivers are tributaries from Douro river. The first three tributaries are mainly located in rural areas crossing agricultural fields. Oppositely Tâmega and Uíma rivers pass through urban areas receiving discharges from industries and WWTP effluents. Ul, Moscoso, and Caima rivers are tributaries from Ria de Aveiro estuarine zone. Douro river was used as a case study to understand how ibuprofen is introduced in surface water and to identify critical points. For that, effluents of three WWTPs located along its extension, which cover rural and urban areas, were collected. Their characterization is described in Table 1. The effluents of four hospitals of the metropolitan area of Porto were also studied as well as the landfill leachate from a landfill located near to Porto, which serves a population of 464,000 inhabitants, and discharges an average leachate volume of 260 m3 day−1 directly into Douro river, after treatment. Ibuprofen mass loading from WWTP effluents and landfill leachates was calculated multiplying the ibuprofen concentration by the flow rate of wastewater, while for calculating the hospitals contribution the estimated water consumption data provided by the hospitals was used (Table 1).
Surface water samples (2.5 L) were collected from different sampling points in order to cover the north of Portugal, as shown in Fig. 1. Samples (2.5 L) from WWTP effluents, hospital effluents, and landfill leachates were also collected (Table 1). Sampling campaigns were performed between March 2010 and September 2011. Sample collection, preservation, and storage were done according to the US EPA Method Guideline (USEPA 2007). River samples were collected on the river side and all samples were collected in amber glass bottles and kept refrigerated (±4 °C) during the transport to the laboratory. All water samples were vacuum filtered through 1.2-μm glass microfiber filters (GF/C, Whatman, UK), followed by 0.20-μm nylon membrane filters (Supelco, Bellefonte, PA, USA) and stored at −20 °C, until extraction. Prior analysis, the samples’ pH was adjusted with hydrochloric acid (2 M).
Analytical procedure
The analytical procedure described in this section was optimized with respect to conditions of pre-concentration and liquid chromatography.
Analysis of ibuprofen was based on pre-concentration of the samples prior to chromatographic analysis by SPE using LiChrolut EN/RP-18 cartridges (Merck, Poland), which gave the best recoveries, and a vacuum manifold system (Phenomenex, USA). The SPE procedure was adapted from Kot-Wasik et al. (2006). Summarily, SPE cartridges were conditioned with 5 mL of acetone followed by 5 mL of methanol and 5 mL of water (pH 2.2) at a flow rate of 3 mL min−1. Aliquots of 600 mL of water sample (pH adjusted to 2.2) were loaded at 8 mL min−1, rinsed with 5 mL of water at 5 mL min−1 and dried with vacuum during 1 h. Elution of ibuprofen was performed ten times with 1 mL of methanol. The extract obtained was evaporated to dryness under a gentle stream of nitrogen and reconstituted in 1 mL of acetonitrile for further analysis. The optimum conditions for ibuprofen extraction, regarding sample pH adjustment prior extraction and sample volume, were found using a 22 factorial design. Best recoveries were obtained combining a sample pH of 2.2 and a sample volume of 600 mL.
Chromatographic separation was performed using a Shimadzu LC system (Shimadzu Corporation, Kyoto, Japan) equipped with a LC 20AB pump, a DGU-20A5 degasser, a SIL 20A autosampler and a RF-10AXL fluorescence detector (FLD). A Luna C18 column (5 μm, 4.6 × 150 mm, Phenomenex, USA) with a security guard column (4.0 × 3.0 mm, Phenomenex, USA) was used. Optimum chromatographic performance was obtained for the following conditions: isocratic elution at 0.8 mL min−1 using water (pH 3, adjusted with acetic acid) as eluent A and acetonitrile as eluent B in a mixture 50:50 (v/v). The injection volume was 20 μL and analysis was made at room temperature (20 ± 1 °C). Fluorescence detection was carried out at an excitation/emission wavelength pair of 220/290 nm. LCsolution software version 2.1 (Shimadzu Corporation, Kyoto, Japan) was used for control and data processing. Using the described experimental conditions, ibuprofen retention time was 18.68 min. Identification of ibuprofen was based on its retention time, the excitation/emission pair wavelength and in the standard addition method, which allows the identification and quantification of ibuprofen in the samples and simultaneously overcome the negative effects of matrix.
Method validation
The validation of the developed analytical methodology was done for river water, hospital and WWTP effluent and landfill leachate and comprised the determination of linearity, limit of detection (MDL), limit of quantification (MQL), recovery, precision, and matrix effects. Calibration curves generated using linear regression analysis and over the established concentration range (50–1,800 μg L−1) gave good fits (r 2 > 0.999). A nine point calibration curve was daily performed, and the possible fluctuation in signal intensity was checked by injecting a standard solution at two concentration levels after each eight injections. Detailed analytical quality assurance data is shown in Table 2. Extraction recoveries, determined for the different matrices at three final concentration levels (0.33, 0.67, and 1.50 μg L−1), ranged from 98 % to 103 %. SPE procedure allowed a pre-concentration factor of 600 in samples, which gave MDL and MQL ranging from 6 to 261 and 23 to 872 ng L−1, respectively, for all matrices. To ensure a correct quantification, instrumental and method precision were studied through the analysis of five replicates of a 900 μg L−1 standard and seven replicates of a 330 ng L−1 spiking level in river water. Results showed a precision of 0.50 % and 1.73 % for standard and 1.46 % and 2.05 % spiked river water from intra- and inter-day precision, respectively.
Matrix effects in the fluorescence signal were evaluated by preparing different calibration curves in river, hospital effluent, WWTP effluent, and landfill leachate extract, and comparing them with one achieved for the standards prepared in acetonitrile. Blanks (samples with no addition of the standard) were assayed simultaneously in order to subtract the levels of ibuprofen present in the sample. Calibration curves obtained in solvent and in river and WWTP effluent extract exhibited similar slopes and Y-intercept, indicating a negligible matrix effect. On the other hand, for hospital effluent and landfill leachate, higher slopes, and Y-intercepts were found, indicating a pronounced matrix effect (data not shown). These results justify the use of the standard addition method, in order to reduce the matrix effects.
Environmental risk assessment
Environmental risk assessment posed by ibuprofen on aquatic ecosystems was estimated by calculating the risk quotient (RQ), using three different representative trophic levels of the ecosystem, namely algae, daphnids, and fish. RQs were determined as the ratio between measured concentrations of ibuprofen (MEC) and its predicted non-effect concentration (PNEC). Concentrations measured during this monitoring study were used as MEC values, while PNEC values were estimated from the lowest ecotoxicological data found in literature (effective concentration—EC50) for acute toxicity studies carried out with species belonging to the different trophic levels evaluated and applying an assessment factor of 1,000, which allows to account for extrapolation from intra- and inter-species variability in sensitivity (Sanderson et al. 2003). If RQ is equal or above to 1, there is a potential environmental risk; whereas, RQ lower than 1 indicates no risk (Ginebreda et al. 2010).
Results and discussion
Occurrence of ibuprofen in Portuguese surface waters
The developed method was applied to identify hot spots of contamination by the anti-inflammatory drug ibuprofen in surface waters of north of Portugal, namely 12 rivers, 1 stream, and 1 estuarine zone. Sampling sites were distributed between urban and rural areas, having a special focus in the northwest coast, where there are a higher population density and distinct contamination sources, such as industry, WWTP and hospital effluents. River water was also collected downstream of three WWTPs and other vulnerable sites, according to the demographic distribution. Due to Douro river extension, which passes through densely populated areas, industrial parks and large agricultural fields, sampling was made in order to cover all its extension and some of its tributaries to understand their contribution in the introduction of ibuprofen in the aquatic environment. Table 3 summarizes ibuprofen concentration range in surface waters from north of Portugal.
It is noticeable that ibuprofen was detected in all main rivers (Douro, Minho, Ave, Lima, and Leça), in Ria de Aveiro estuarine zone and one of its tributaries, and in two Douro river tributaries with concentrations that can reach 723 ng L−1. In general, higher concentrations of ibuprofen were detected in the coast area near to the river mouths, which run through large cities. Five of the studied rivers flow into the Atlantic Ocean in the northwest coast. These results suggest that the presence of this pharmaceutical could be related to human influence, such as the input of WWTP and hospital effluents. In fact in one sampling site of Lima river (R17), the negative impact of human activity is very clear, since it is possible to see an untreated sewage discharge entering directly into the river. This sample showed the highest ibuprofen concentration detected in the analyzed surface waters. Ria de Aveiro estuary findings can be justified due to the location of the estuary in an urban area, affected by human activities. Additionally, three tributaries of this estuarine zone were also analyzed, and ibuprofen was only detected at the sampling site of Moscoso stream (ET2; Table 3), reporting the resembling levels of contamination (229 ng L−1).
Regarding Douro river, sampling was done along the river, starting in Pocinho—Vila Nova de Foz Côa (R1; 30 km after the river enter in Portugal) and samples were collected approximately each 30 km downstream to the river mouth. The possible impact of WWTP effluents of urban and rural areas, which cover different population densities, in the Douro receiving waters was also evaluated. For instance, a low level of ibuprofen (46 ng L−1) was detected in the effluent of a WWTP located in a rural area (WWTP1); but in the Douro receiving water (R2), it was not possible to detect this, probably due to the dilution effect. On the other hand, ibuprofen was not detected near the discharge point of a small WWTP (WWTP2) located in an urban area. These results are in agreement with literature that described variations in the ibuprofen removal rate between 75 % and more than 98 % (Zorita et al. 2009), depending on the efficiency of the treatments used in the WWTP as well as the seasonal conditions (Ziylan and Ince 2011). Higher levels of ibuprofen in WWTP effluents in Portugal have been previously reported (Salgado et al. 2010; Sousa et al. 2011). During its course, Douro river receives several tributaries. Some of them were analyzed, showing the presence of ibuprofen in Tâmega and Uíma rivers, at concentrations that can reach 359 and 173 ng L−1, respectively, although it could not be detected after they met Douro river. It should be noticed that in Uíma river, ibuprofen was only detected in one sampling site (T5) located downstream of a WWTP (WWTP3), which had an estimated daily mass loading of 589 mg day−1 (Table 3). Non-detection of ibuprofen in some of the tributaries may be attributed to dilution by river water or to their location in rural areas. The presence of ibuprofen was only detected in the samples collected near to the Douro river mouth, where it crosses the city centre of Porto and Vila Nova de Gaia, at levels between 138 and 232 ng L−1. This could be explained by the presence of two of the largest WWTPs, which serve Porto city (approximately 370,000 inhabitants) and discharge their effluents into Douro river (Madureira et al. 2010). These results are in agreement with previously published data that showed the presence of other pharmaceuticals in the lower part of Douro river (Madureira et al. 2009; Madureira et al. 2010; Ribeiro et al. 2009c).
Going into the contribution of hospital effluents in surface waters contamination by ibuprofen, four hospitals (two general, a paediatric, and a maternity), which send their effluents to WWTPs located in Douro river area, were analyzed. Ibuprofen was found in all hospital effluents showing estimated daily mass loadings from 162 to 2,193 mg day−1 for maternity (H4) and general (H2) hospitals, respectively (Table 3). In view of the scarce data of landfill leachates as contamination sources of surface waters, a landfill located in Porto area, which leachates are discharged into the Douro river, was also pointed out in this study. Contamination levels from 9,761 to 48,720 ng L−1 were found, representing an estimated daily mass loading of ibuprofen to Douro river up to 12,681 mg day−1. These high concentrations of ibuprofen in landfills could be explained by its high consumption among Portuguese population, given that ibuprofen is in the top ten of the most prescribed pharmaceuticals in Portugal (INFARMED 2012) and unused medicines might be eliminated in household wastes. Ibuprofen concentrations in landfill leachates at micrograms per liter level were also reported by Eggen et al. (2010). In general, ibuprofen concentrations found in wastewaters (WWTP effluents and landfill leachates) represented median inputs varying from 23 to 12,681 mg day−1 into Portuguese surface waters, being the highest inputs attributed to landfill leachates. These findings highlight the pronounced contribution of landfill leachates in the entrance of ibuprofen into surface waters.
The results obtained are in agreement with some studies presented in the literature, where ibuprofen was reported in river waters of different countries, such as Sweden (10–220 ng L−1; Bendz et al. 2005; Daneshvar et al. 2010), Romania (<30–115.2 ng L−1; Moldovan 2006) and Germany (4.9–152 ng L−1; Hernando et al. 2006; Weigel et al. 2004b), contrarily to what happens in countries like UK (2,370 ng L−1; Roberts and Thomas 2006), Luxembourg (2,383 ng L−1; Pailler et al. 2009), and Spain (16,886 ng L−1; Valcárcel et al. 2011), where much higher concentrations were pointed out. The presence of ibuprofen in hospital effluents was also described in several studies, ranging from 90 ng L−1 in Norway (Weigel et al. 2004a) to 151,000 ng L−1 in Spain (Gómez et al. 2006), and in WWTP effluents with concentrations between 18 ng L−1 in USA (Thomas and Foster 2004) and 28,000 ng L−1 in Spain (Gómez et al. 2007). Once again, the results obtained for hospital and WWTP effluents are in accordance with data presented in literature.
Environmental risk assessment
Due to environmental concentrations of ibuprofen exceeded the 10 ng L−1 safety threshold established by European Medicines Agency (EMA) (Gros et al. 2010), ecotoxicological risk was evaluated in surface waters, WWTP effluents, and landfill leachates in order to assess the potential risk of ibuprofen for aquatic organisms.
Acute EC50 values of ibuprofen used in this study were collected from literature and are summarized in Table 4. As no experimental values were available for fish, an EC50 estimated with ECOSAR was used (Sanderson et al. 2003). According to the EU directive 93/67/EC, ibuprofen can be classified as toxic for the environment (1 < EC50 < 10 mg L−1; Sanderson et al. 2003). Table 5 shows the risk quotients obtained for fish, Daphnia, and algae in the river, WWTP effluents, and landfill leachates where ibuprofen was quantified. Ibuprofen showed RQ greater than 1 in landfill leachates, indicating a potential environmental risk for aquatic organisms. In rivers and WWTP effluents RQ were below 1, so it is assumed that there is no risk. When the three bioassays are compared, algae appear to be the most sensitive organisms, followed by fish and Daphnia. These results are in agreement with Ginebreda et al. (2010), who also reported a higher sensitivity of algae to pharmaceuticals.
However, this evaluation is only focused on the toxicity that an individual compound (ibuprofen) may cause to aquatic organisms, but in the aquatic environment, pharmaceuticals are present as mixtures of a great variety of different therapeutic classes, which may reveal synergic or additive effects, exhibiting higher toxicities than single compounds, even a lower concentrations, as was shown by Cleuvers (2003) for ibuprofen.
Conclusions
The occurrence of ibuprofen in surface waters of north of Portugal was reported, showing its presence in all the main rivers and in the estuarine zone, principally near the river mouths, at concentrations of some hundreds of nanograms per liter. Due to its high consumption rate among Portuguese population, hospitals, WWTPs, and landfills were identified as hot spots of contamination, contributing to the loading of ibuprofen into surface waters. Landfill leachates showed the highest contribution for the loading of ibuprofen into surface waters; therefore, more attention should be paid to these kinds of facilities. The information obtained represents an important base for further studies due to the highest concentrations observed in the northwest area, near to the coast. Environmental risk assessment was evaluated showing that there is no expected ecotoxicological risk for aquatic organisms due to the presence of ibuprofen in surface waters and WWTP effluents, while, after treatment, landfill leachates pose a potential risk for aquatic organisms. However, the environmental risk assessment carried out in this work has been focused in the individual toxicity of ibuprofen and the potential for synergic or additive effects should be also taken into account. As a consequence of the findings for ibuprofen in surfaces waters of north of Portugal, more studies are needed as an attempt to assess more vulnerable areas and to better understand its impact in public health and its risk for aquatic organisms.
References
Ali I, Singh P, Aboul-Enein HY, Sharma B (2009) Chiral analysis of ibuprofen residues in water and sediment. Anal Lett 42:1747–1760
Barreiro JC, Vanzolini KL, Madureira TV, Tiritan ME, Cass QB (2010) A column-switching method for quantification of the enantiomers of omeprazole in native matrices of waste and estuarine water samples. Talanta 82:384–391
Bendz D, Paxéus NA, Ginn TR, Loge FJ (2005) Occurrence and fate of pharmaceutically active compounds in the environment, a case study: Höje River in Sweden. J Hazard Mater 122:195–204
Bueno MJM, Agüera A, Hernando MD, Gómez MJ, Fernández-Alba AR (2009) Evaluation of various liquid chromatography-quadrupole-linear ion trap-mass spectrometry operation modes applied to the analysis of organic pollutants in wastewaters. J Chromatogr A 1216:5995–6002
Cleuvers M (2003) Aquatic ecotoxicity of pharmaceuticals including the assessment of combination effects. Toxicol Lett 142:185–194
Daneshvar A, Svanfelt J, Kronberg L, Weyhenmeyer GA (2010) Winter accumulation of acidic pharmaceuticals in a Swedish river. Environ Sci Pollut Res 17:908–916
Daughton CG, Ternes TA (1999) Pharmaceuticals and personal care products in the environment: agents of subtle change? Environ Health Perspect 107:907–938
Dave G, Herger G (2012) Determination of detoxification to Daphnia magna of four pharmaceuticals and seven surfactants by activated sludge. Chemosphere 88:459–466
Eggen T, Moeder M, Arukwe A (2010) Municipal landfill leachates: a significant source for new and emerging pollutants. Sci Total Environ 408:5147–5157
Flippin JL, Huggett D, Foran CM (2007) Changes in the timing of reproduction following chronic exposure to ibuprofen in Japanese medaka, Oryzias latipes. Aquat Toxicol 81:73–78
Ginebreda A, Muñoz I, de Alda ML, Brix R, López-Doval J, Barceló D (2010) Environmental risk assessment of pharmaceuticals in rivers: relationships between hazard indexes and aquatic macroinvertebrate diversity indexes in the Llobregat River (NE Spain). Environ Int 36:153–162
Gómez MJ, Petrović M, Fernández-Alba AR, Barceló D (2006) Determination of pharmaceuticals of various therapeutic classes by solid-phase extraction and liquid chromatography–tandem mass spectrometry analysis in hospital effluent wastewaters. J Chromatogr A 1114:224–233
Gómez MJ, Martínez Bueno MJ, Lacorte S, Fernández-Alba AR, Agüera A (2007) Pilot survey monitoring pharmaceuticals and related compounds in a sewage treatment plant located on the Mediterranean coast. Chemosphere 66:993–1002
Gros M, Petrovic M, Ginebreda A, Barcelo D (2010) Removal of pharmaceuticals during wastewater treatment and environmental risk assessment using hazard indexes. Environ Int 36:15–26
Han S, Choi K, Kim J, Ji K, Kim S, Ahn B, Yun J, Choi K, Khim JS, Zhang X, Giesy JP (2010) Endocrine disruption and consequences of chronic exposure to ibuprofen in Japanese medaka (Oryzias latipes) and freshwater cladocerans Daphnia magna and Moina macrocopa. Aquat Toxicol 98:256–264
Hayashi Y, Heckmann L-H, Callaghan A, Sibly RM (2008) Reproduction recovery of the crustacean Daphnia magna after chronic exposure to ibuprofen. Ecotoxicology 17:246–251
Hernando MD, Heath E, Petrovic M, Barcelo D (2006) Trace-level determination of pharmaceutical residues by LC-MS/MS in natural and treated waters. A pilot-survey study. Anal Bioanal Chem 385:985–991
Hilton MJ, Thomas KV (2003) Determination of selected human pharmaceutical compounds in effluent and surface water samples by high-performance liquid chromatography–electrospray tandem mass spectrometry. J Chromatogr A 1015:129–141
INFARMED (2012) Estatística do Medicamento. INFARMED. http://www.infarmed.pt/portal/page/portal/INFARMED/PUBLICACOES/TEMATICOS/ESTATISTICA_MEDICAMENTO. Accessed 1 February 2012 (in Portuguese)
Kim SD, Cho J, Kim IS, Vanderford BJ, Snyder SA (2007) Occurrence and removal of pharmaceuticals and endocrine disruptors in South Korean surface, drinking, and waste waters. Water Res 41:1013–1021
Kosma CI, Lambropoulou DA, Albanis TA (2010) Occurrence and removal of PPCPs in municipal and hospital wastewaters in Greece. J Hazard Mater 179:804–817
Kot-Wasik A, Debska J, Wasik A, Namiesnik J (2006) Determination of non-steroidal anti-inflammatory drugs in natural waters using off-line and on-line SPE followed by LC coupled with DAD-MS. Chromatographia 64:13–21
Lin AY-C, Tsai Y-T (2009) Occurrence of pharmaceuticals in Taiwan’s surface waters: impact of waste streams from hospitals and pharmaceutical production facilities. Sci Total Environ 407:3793–3802
Lin AY-C, Yu T-H, Lateef SK (2009) Removal of pharmaceuticals in secondary wastewater treatment processes in Taiwan. J Hazard Mater 167:1163–1169
Madureira TV, Barreiro JC, Rocha MJ, Cass QB, Tiritan ME (2009) Pharmaceutical trace analysis in aqueous environmental matrices by liquid chromatography-ion trap tandem mass spectrometry. J Chromatogr A 1216:7033–7042
Madureira TV, Barreiro JC, Rocha MJ, Rocha E, Cass QB, Tiritan ME (2010) Spatiotemporal distribution of pharmaceuticals in the Douro River estuary (Portugal). Sci Total Environ 408:5513–5520
Méndez-Arriaga F, Torres-Palma RA, Pétrier C, Esplugas S, Gimenez J, Pulgarin C (2008) Ultrasonic treatment of water contaminated with ibuprofen. Water Res 42:4243–4248
Moldovan Z (2006) Occurrences of pharmaceutical and personal care products as micropollutants in rivers from Romania. Chemosphere 64:1808–1817
Nakada N, Tanishima T, Shinohara H, Kiri K, Takada H (2006) Pharmaceutical chemicals and endocrine disrupters in municipal wastewater in Tokyo and their removal during activated sludge treatment. Water Res 40:3297–3303
Pailler JY, Krein A, Pfister L, Hoffmann L, Guignard C (2009) Solid phase extraction coupled to liquid chromatography-tandem mass spectrometry analysis of sulfonamides, tetracyclines, analgesics and hormones in surface water and wastewater in Luxembourg. Sci Total Environ 407:4736–4743
Pena A, Chmielova D, Lino CM, Solich P (2007) Determination of fluoroquino one antibiotics in surface waters from Mondego River by high performance liquid chromatography using a monolithic column. J Sep Sci 30:2924–2928
Pena A, Paulo M, Silva LJG, Seifrtova M, Lino CM, Solich P (2010) Tetracycline antibiotics in hospital and municipal wastewaters: a pilot study in Portugal. Anal Bioanal Chem 396:2929–2936
Pomati F, Netting AG, Calamari D, Neilan BA (2004) Effects of erythromycin, tetracycline and ibuprofen on the growth of Synechocystis sp and Lemna minor. Aquat Toxicol 67:387–396
Ribeiro C, Pardal MA, Martinho F, Margalho R, Tiritan ME, Rocha E, Rocha MJ (2009a) Distribution of endocrine disruptors in the Mondego River estuary, Portugal. Environ Monit Assess 149:183–193
Ribeiro C, Pardal MA, Tiritan ME, Rocha E, Margalho RM, Rocha MJ (2009b) Spatial distribution and quantification of endocrine-disrupting chemicals in Sado River estuary, Portugal. Environ Monit Assess 159:415–427
Ribeiro C, Tiritan ME, Rocha E, Rocha MJ (2009c) Seasonal and spatial distribution of several endocrine-disrupting compounds in the Douro River estuary, Portugal. Arch Environ Contam Toxicol 56:1–11
Richardson SD (2010) Environmental mass spectrometry: emerging contaminants and current issues. Anal Chem 82:4742–4774
Roberts PH, Thomas KV (2006) The occurrence of selected pharmaceuticals in wastewater effluent and surface waters of the lower Tyne catchment. Sci Total Environ 356:143–153
Salgado R, Noronha JP, Oehmen A, Carvalho G, Reis MAM (2010) Analysis of 65 pharmaceuticals and personal care products in 5 wastewater treatment plants in Portugal using a simplified analytical methodology. Water Sci Technol 62:2862–2871
Sanderson H, Johnson DJ, Wilson CJ, Brain RA, Solomon KR (2003) Probabilistic hazard assessment of environmentally occurring pharmaceuticals toxicity to fish, daphnids and algae by ECOSAR screening. Toxicol Lett 144:383–395
Santos LHMLM, Araújo AN, Fachini A, Pena A, Delerue-Matos C, Montenegro MCBSM (2010) Ecotoxicological aspects related to the presence of pharmaceuticals in the aquatic environment. J Hazard Mater 175:45–95
SCHER (2011) Opinion on draft environmental quality standards under the Water Framework Directive—Ibuprofen.
Seifrtova M, Pena A, Lino CM, Solich P (2008) Determination of fluoroquinolone antibiotics in hospital and municipal wastewaters in Coimbra by liquid chromatography with a monolithic column and fluorescence detection. Anal Bioanal Chem 391:799–805
Sousa MA, Goncalves C, Cunha E, Hajslova J, Alpendurada MF (2011) Cleanup strategies and advantages in the determination of several therapeutic classes of pharmaceuticals in wastewater samples by SPE-LC-MS/MS. Anal Bioanal Chem 399:807–822
Stackelberg PE, Furlong ET, Meyer MT, Zaugg SD, Henderson AK, Reissman DB (2004) Persistence of pharmaceutical compounds and other organic wastewater contaminants in a conventional drinking-water treatment plant. Sci Total Environ 329:99–113
Teixeira S, Delerue-Matos C, Alves A, Santos L (2008) Fast screening procedure for antibiotics in wastewaters by direct HPLC-DAD analysis. J Sep Sci 31:2924–2931
Thomas PM, Foster GD (2004) Determination of nonsteroidal anti-inflammatory drugs, caffeine, and triclosan in wastewater by gas chromatography–mass spectrometry. J Environ Sci Health A 39:1969–1978
USEPA (2006). http://www.epa.gov/ppcp/. Accessed 1 February 2012
USEPA (2007) Method 1694: Pharmaceuticals and personal care products in water, soil, sediment, and biosolids by HPLC/MS/MS. U.S. Environmental Protection Agency Office of Water Office of Science and Technology Engineering and Analysis Division, Washington, DC
Valcárcel Y, Alonso SG, Rodríguez-Gil JL, Maroto RR, Gil A, Catalá M (2011) Analysis of the presence of cardiovascular and analgesic/anti-inflammatory/antipyretic pharmaceuticals in river- and drinking-water of the Madrid Region in Spain. Chemosphere 82:1062–1071
Verenitch SS, Lowe CJ, Mazumder A (2006) Determination of acidic drugs and caffeine in municipal wastewaters and receiving waters by gas chromatography–ion trap tandem mass spectrometry. J Chromatogr A 1116:193–203
Weigel S, Berger U, Jensen E, Kallenborn R, Thoresen H, Hühnerfuss H (2004a) Determination of selected pharmaceuticals and caffeine in sewage and seawater from Tromsø/Norway with emphasis on ibuprofen and its metabolites. Chemosphere 56:583–592
Weigel S, Kallenborn R, Hühnerfuss H (2004b) Simultaneous solid-phase extraction of acidic, neutral and basic pharmaceuticals from aqueous samples at ambient (neutral) pH and their determination by gas chromatography–mass spectrometry. J Chromatogr A 1023:183–195
Ziylan A, Ince NH (2011) The occurrence and fate of anti-inflammatory and analgesic pharmaceuticals in sewage and fresh water: treatability by conventional and non-conventional processes. J Hazard Mater 187:24–36
Zorita S, Mårtensson L, Mathiasson L (2009) Occurrence and removal of pharmaceuticals in a municipal sewage treatment system in the south of Sweden. Sci Total Environ 407:2760–2770
Acknowledgments
The work has been supported by Fundação para a Ciência e a Tecnologia (FCT) through the grant no. PEst-C/EQB/LA0006/2011 and project PTDC/ECM/103141/2008. Lúcia H.M.L.M. Santos also thanks to FCT and FSE/POPH for her PhD grant (SFRH/BD/48168/2008). The authors are grateful to Autoridade Nacional do Medicamento e Produtos de Saúde (INFARMED), especially to the “Centro de Informação” and “Centro de Documentação Técnica e Científica,” for all the information given about ibuprofen consumption rates in Portugal. The authors also wish to acknowledge to the hospitals by providing the samples.
Author information
Authors and Affiliations
Corresponding author
Additional information
Responsible editor: Hongwen Sun
Paula Paíga and Lúcia H.M.L.M. Santos equally contributed to this work.
Rights and permissions
About this article
Cite this article
Paíga, P., Santos, L.H.M.L.M., Amorim, C.G. et al. Pilot monitoring study of ibuprofen in surface waters of north of Portugal. Environ Sci Pollut Res 20, 2410–2420 (2013). https://doi.org/10.1007/s11356-012-1128-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-012-1128-1