
Abstract
Background
Psoriasis is a chronic inflammatory skin disease which can cause sleep disturbances due to the disease itself or due to its complications. In this study, we aimed to analyze the array of sleep disturbances caused by psoriasis and to evaluate the interaction between the quality of sleep and the duration and severity of psoriasis.
Methods
Study subjects included 60 patients with plaque psoriasis and 60 sex- and age-matched controls. The Psoriasis Area and Severity Index (PASI) was used to evaluate severity of disease. Body mass index (BMI), medication usage, and duration of disease were recorded. All subjects completed the Epworth Sleepiness Scale (EES), Pittsburgh Sleep Quality Index (PSQI), insomnia severity index (ISI), Berlin-sleep apnea questionnaire, and questions based on criteria of the International Restless Legs Syndrome Study Group indicating the presence of restless legs syndrome (RLS).
Results
There were statistically significant and clinically relevant differences between the patients and controls regarding day-time sleepiness (ESS 5.3 vs 4.1, p = 0.037), sleep quality (PSQI 14.4 vs 4.9, p < 0.001), insomnia (ISI 19.7 vs 14.4, p < 0.001), sleep apnea (high risk 30% vs 7%, p = 0.01), and RLS (high risk 32% vs 0%, p < 0.001).
Conclusions
Patients with psoriasis experience poor sleep quality and are at markedly increased risk for insomnia, obstructive sleep apnea, and restless legs syndrome. These findings suggest the importance of evaluating patients with psoriasis for conditions that affect sleep. The study results further suggest that simple screening tools may be useful for this task.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Sleep is one of the most important factors in the maintenance of health, affecting both psychological and physiological well-being [1]. Sleep quality and daytime sleepiness are clinically important parameters in the sleep-wake cycle, with low sleep quality and insomnia triggering various psychiatric disorders, resulting also in deterioration in health status and work efficiency. Along with an objective sleep evaluation based on polysomnography (PSG) and multiple sleep latency testing, questionnaires that facilitate subjective self-assessment are widely used, with the Pittsburgh Sleep Quality Index (PSQI) and Epworth Sleepiness Scale (ESS) being the most common [2,3,4].
Psoriasis is a prevalent chronic inflammatory skin disease that affects some 2–3% of the population [5]. Aside from being a multisystem disease, it can also lead to sleep disorders through secondary causes such as depression, pain, restless leg syndrome (RLS), and poor sleep quality. Psoriasis can also lead to an increased incidence of sleep apnea and snoring by triggering obesity and metabolic syndrome [6, 7]. Obstructive sleep apnea syndrome (OSAS) plays a role in the pathogenesis of psoriasis by bringing about changes in the microvascular structure through inflammatory activation, and as a result, interactions between these two chronic conditions may worsen the pathogenic course of each disease [8]. Furthermore, meta-analyses have shown that little or excessive sleep can increase the mortality and morbidity associated with chronic diseases [9].
Studies evaluating sleep disorders related to psoriasis have indicated increased frequency of sleep apnea and insomnia due to pruritus, pain, and psychiatric disorders such as depression. Increased skin temperatures resulting from pruritus and inflammation may trigger sleep disorders by affecting circadian rhythm [10].
The present study examined the array of sleep disorders in psoriasis and sought to evaluate possible interactions between sleep quality and disease duration and severity.
Methods
The design was a cross-sectional, questionnaire-based, case-controlled study including clinical assessment of disease severity. The ethics committee gave its approval prior to initiation of the study. The study was conducted according to the principles of the Declaration of Helsinki.
After obtaining written informed consent, 60 patients with plaque psoriasis and 60 sex- and age-matched healthy controls were enrolled. All subjects were at least 18 years old. Exclusion criteria included prescribed neuroleptics, calcium channel blockers, dopamine antagonists, antidepressants, and anti-epileptics. Other exclusions included patients with renal disease, infectious disease, rheumatologic disease, lumbosacral radiculopathy, chronic obstructive lung disease, thyroid disease, anemia, peripheral vascular disease, depression-anxiety disorders, malignant disease, alcoholism, and pregnancy.
Body weight and height to calculate body mass index (BMI), neck circumference, and clinical examination results of patients with psoriasis presenting at dermatology outpatient clinics were recorded, along with medication usage and disease duration. The severity of psoriasis was evaluated using the Psoriasis Area and Severity Index (PASI), while the factors that may cause sleep disorders were investigated in detail by a neurologist. Neurological examinations were performed and underwent a brief neuropsychiatric interview for mental state and psychiatric illness assessment.
Psoriasis Area and Severity Index (PASI)
Measurements for the PASI include mean redness, thickness, and desquamation of lesions (0–4°), weighted by the area of involvement, with the total score ranging from 0 (disease free) to 72 (maximal disease) [11].
Epworth Sleepiness Scale (ESS)
This self-administered questionnaire is used to assess daytime sleepiness. The ESS is an 8-item scale that assesses likelihood of dozing (0 to 3) while performing certain activities with a range of possible points from 0 to 24. An ESS score > 10 is indicative of excessive daytime sleepiness [12].
Pittsburgh Sleep Quality Index (PSQI)
This questionnaire allows subjective assessment of sleep quality in the preceding month. The questionnaire consists of 19 questions based on various sleep habits. The questions yield “component” scores, each ranging from 0 to 3 points with more points indicating greater difficulties. The seven component scores sum to a total score ranging from 0 to 21 points. A total score of ≥ 5 denotes poor sleep quality with good reliability and validity [13].
Insomnia Severity Index (ISI)
The ISI consists of seven questions about the perceived effect of sleep disturbance on the individual during the preceding 2 weeks. The total score ranges from 0 to 28. Scores < 7 are normal, 8–14 subclinical insomnia, 15–21 clinical insomnia, and 22–28 severe insomnia [14].
The Berlin Questionnaire for Sleep Apnea
This screening survey assesses risk for OSAS using ten items divided into three categories. Positive scores in two or more categories indicate high risk for OSAS [15].
Questions for RLS Criteria
Criteria of the International Restless Legs Syndrome Study Group (IRLSSG) are determined through clinical interviews or questionnaires [16].
Statistical analysis
All statistical analyses were performed using the Statistical Package for Social Sciences 20.0 (IBM Corp.; Armonk, NY, USA) software package program. The Shapiro-Wilk test was used to confirm the normal distribution of all data in the present study. The continuous variables were expressed as means ± SD, and Student’s t tests were used to compare the means between two groups. For categorical variables, the Chi-square test was used to test the differences between groups. Bivariate logistic regression was applied to identify significant associations with poor sleep. Unless otherwise stated, p < 0.05 was set as the level of significance.
Results
For the 60 patients with psoriasis and 60 control subjects, there were no differences in age, sex, or BMI. See Table 1. The mean duration of the disease of psoriasis was 11.8 ± 8.1 years (range 1–30 years). Mean PASI was 10.1 ± 9.7 (range 1–41) in the psoriatic patient. Forty-five patients (75%) received topical treatment, 10 patients (16.6%) had systemic treatment, and 5 patients (8.4%) had topical and systemic treatment.
Daytime sleepiness and sleep questionnaire results are shown in Table 2. Specific responses to the PSQI by component scores are shown in Table 3. Statistically significant differences were found in scores for daytime sleepiness, sleep quality, insomnia severity, risk for sleep apnea, and risk for RLS. Furthermore, 54 (90%) of the patients with psoriasis experienced poor sleep quality, compared to 22 (33%) in the control group. Likewise, among patients with psoriasis, 23 (38%) achieved an insomnia severity score that was clinically suggestive of insomnia while only two patients (3%) in the control group had scores consistent with insomnia. Five patients (8.33%) and four control subjects (6.66%) had ESS scores > 10, indicating daytime sleepiness (p = 0.556). While the difference between these proportions was not statistically significant, comparison of the mean values between the two groups was statistically significant (p = 0.037).
Multivariate regression analysis showed that the model used in the present study was weak (Nagelkerke R2 = 0.068). There was no strongly significant relationship identified between poor sleep quality and sex, age, BMI, duration of disease, or PASI score (Table 4).
Discussion
The present study identified increased poor sleep quality and sleep disturbances in patients with psoriasis compared to controls. The study also identified with standardized and valid scales increased incidences of insomnia, OSAS, and RLS among the patients with psoriasis.
Previous studies have shown that psoriasis can lead to poor sleep quality and fragmented sleep, although there is a paucity of studies investigating the classification of sleep disorders [17,18,19]. Psoriasis can lead directly to sleep disorders in that the skin plays a primary role in the way circadian rhythm regulates body temperature. A small decrease in body temperature is of importance for the induction and maintenance of sleep [18]. Psoriasis impairs thermoregulation and heat transmission irregularities disrupt the induction and maintenance of sleep [18]. Pruritus and pain both increase in intensity in the evening hours along with a decrease in cortisol levels, as both are controlled by the circadian rhythm. These factors can lead to sleep disorders [19]. Sleep disorders may often be related to secondary causes (such as obesity, medication, depression, etc.) and not solely to the disease itself [20].
It was found in the present study that the patient group had a high risk of sleep apnea according to the Berlin questionnaire. A recent systematic review of the literature on psoriasis and sleep disorders revealed the reported prevalence of OSA in patients with psoriasis ranging from 36 to 81% [21]. Gabryelska et al. found in their polysomnographic study of psoriatic patients that elevated body mass index was an independent risk factor for OSA [7]. It is known that obesity is common in patients with psoriasis and that an increased BMI is a trigger for inflammation [6,7,8]. However, in agreement with studies by Duffin et al. and Bicici et al. [6, 22], we were not able to show an effect of obesity on sleep disorders.
Male gender, obesity, and neck circumference are associated with higher risk of sleep apnea [23]. However, in the current study, balanced groups were formed in an attempt to clarify the effect of the disease on sleep. According to the literature, the inflammatory activity of the disease itself may increase the risk of OSA and other sleep disturbances [23]. We theorize that the pathophysiology of inflammation in psoriasis may be responsible for a higher risk of OSA. Because most of the patients in the current study received local treatment and systemic treatment was given to only a limited number of patients, it was not possible to demonstrate a protective effect of psoriasis therapy. Thaci et al. have shown that treatment with etanercept significantly improved sleep. In particular, obese patients with OSA experienced a marked decrease in sleepiness after treatment with etanercept [24]. Several studies have shown that sleepiness is affected by medications that neutralize TNFa, such as thalidomide, etanercept, and infliximab [25].
Since the pathophysiologies of OSA and psoriasis are associated with inflammation, the interaction between the two diseases has been discussed in the literature [23]. According to the results of previous research, increased levels of pro-inflammatory cytokines are among the factors implicated as causes of OSAS and insomnia [26, 27]. The alteration or dysregulation of cytokines may lead to sleep dysfunction. Studies have shown that the circadian rhythm of TNFa release was previously found to be significantly disturbed in patients with OSA. It has been proposed that psoriasis and OSA are linked bidirectionally via inflammatory pathways [27]. In a prospective study including an 11-year follow-up period, the association of OSAS was investigated as a cause of psoriasis. This study showed a two-fold greater prevalence of psoriasis among patients diagnosed with OSAS [8]. A cross-sectional survey published in 2017 emphasized that sleep quality could be improved through the treatment of accompanying diseases and that factors such as pruritus and pain are detrimental to quality of life [28].
An evaluation of the increased prevalence of insomnia and poor sleep quality among the PSQI component scores revealed that sleep latency was increased and the normal waking time was not concordant with the circadian rhythm. The patients went to sleep late and woke up late in the morning, and as a result, these patients subjectively rated their sleep quality as poor. In studies using sleep-deprived psoriatic animal models, metabolic, endocrine, and sympathetic nervous system activity changed as a result of the release of inflammatory cytokines, and consequently, both sleep quality and the severity of psoriasis may be unfavorably affected [1]. It should be emphasized that the current study showed that though the patient group frequently experienced sleepiness, neither the patient group nor the control group scored high on the Epworth Sleepiness score (mean ESS < 10). The patient group suffered with insomnia with an abnormal circadian rhythm. The PSQI and ESS are only weakly related to each other [2]. The PSQI was more strongly related to self-reported measures of psychological symptoms and stress compared to the ESS [2].
Our findings of increased risk for RLS in patients with psoriasis agree with a systematic review by Gupta et al. which found that the risk of RLS is higher in patients with psoriasis than in the normal population [21]. In particular, the exclusion of depressive mood and inadequate protection of local treatments from systemic complications are the most important causes of poor sleep and RLS. It is emphasized that locally acting therapies cannot control the inflammatory process and provide an ineffective treatment for the sleep disorders [22].
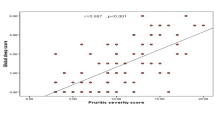
The present study identified no significant correlation between sleep disorders and disease severity and duration. This lack of correlation may be attributable to the small number of patients and low disease severity in the study. In a study of a large patient series (n = 152) using biological and systemic agents, Strober et al. identified PASI score as an important predictor of sleep quality and daytime sleepiness, while another study (n = 73) reporting similar results to those in the present study showed no significant relationship between PASI scores and sleep quality [6, 27].
The present study revealed that the prevalence of sleep disorders in patients with psoriasis is considerably increased when compared to healthy controls. Limitation of the present study is that we were unable to perform polysomnography on the patients and control subjects, nor was it possible to measure body temperature, iron, or ferritin. Strengths of the present study are its homogeneous patient group excluding those with comorbid diseases and systemic drug use. Furthermore, sleep assessments were not based solely on questionnaires but were supported by neurological examination. In view of the important findings of the current study, the authors believe that all patients with psoriasis should be evaluated for sufficient sleep time and adequate sleep quality.
References
Jensen P, Zachariae C, Skov L, Zachariae R (2018) Sleep disturbance in psoriasis: acase-controlled study. Br J Dermatol 179:1376–1384. https://doi.org/10.1111/bjd.16702. [Epub ahead of print]
Buysse DJ, Hall ML, Strollo PJ, Kamarck TW, Owens J, Lee L, Reis SE, Matthews KA (2008) Relationships between the Pittsburgh sleep quality index (PSQI), Epworth sleepiness scale(ESS), and clinical/polysomnographic measures in a community sample. J Clin Sleep Med 4(6):563–571
Buysse DJ, Reynolds CF, Monk TH et al (1989) The Pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res 28:193–213
Johns MW (1991) A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep. 14:540–545
Rachakonda TD, Schupp CW, Armstrong AW (2014) Psoriasis prevalence among adults in the United States. J Am Acad Dermatol 70(3):512–516. https://doi.org/10.1016/j.jaad.2013.11.013 Epub 2014 Jan 2
Biçici F, Hayta SB, Akyol M, Özçelik S, Ziynet Çınar Z (2015) Evaluation of sleep quality in patients with psoriasis. Turkderm. 49:208–212
Gabryelska A, Sochal M, Wasik B, Białasiewicz P (2018) Patients with obstructive sleep apnea are over four times more likely to suffer from psoriasis than the general population. J Clin Sleep Med 14(1):153. https://doi.org/10.5664/jcsm.6908
Cohen JM, Jackson CL, Li TY, Wu S, Qureshi AA (2015) Sleep disordered breathing and the risk of psoriasis among US women. Arch Dermatol Res 307(5):433–438. https://doi.org/10.1007/s00403-015-1536-4 Epub 2015 Feb 13
Cappuccio FP, D’Elia L, Strazzullo P, Miller MA (2010) Sleep duration and all-cause mortality: a systematic review and meta-analysis of prospective studies. Sleep. 33:585–592
Henry AL, Kyle SD, Bhandari S, Chisholm A, Griffiths CE, Bundy C (2016) Measurement, classification and evaluation of sleep disturbance in psoriasis: a systematic review. PLoS One 11(6):e0157843. https://doi.org/10.1371/journal.pone.0157843
Armstrong AW, Parsi K, Schupp CW, Mease PJ, Duffin KC (2013) Standardizing training for psoriasis measures: effectiveness of an online training video on psoriasis area and severity index assessment by physician and patient raters. JAMA Dermatol. 149:577–582
Baumgartel KL, Terhorst L, Conley YP, Roberts JM (2013) Psychometric evaluation of the Epworth sleepiness scale in an obstetric population. Sleep Med 14(1):116–121. https://doi.org/10.1016/j.sleep.2012.10.007 Epub 2012 Dec 4
Dudysová D, Malá I, Mladá K, Saifutdinova E, Koprivova J, Sos P (2017) Structural and construct validity of the Czech version of the Pittsburgh sleep quality index in chronic insomnia. Neuro Endocrinol Lett 38(1):67–73
Chahoud M, Chahine R, Salameh P, Sauleau EA (2017) Reliability, factor analysis and internal consistency calculation of the insomnia severity index (ISI) in French and in English among Lebanese adolescents. eNeurologicalSci. 7:9–14. https://doi.org/10.1016/j.ensci.2017.03.003 eCollection 2017 Jun
Kashaninasab F, Alavi K, Farhadi M, Salehi M, Ghaleh Bandi MF (2017) A comparative study of four Persian versions of sleep questionnaires for screening obstructive sleep apnea syndrome (OSAS). Med J Islam Repub Iran 31:122. https://doi.org/10.14196/mjiri.31.122.eCollection
Allen RP, Picchietti DL, Garcia-Borreguero D, Ondo WG, Walters AS, Winkelman JW, Zucconi M, Ferri R, Trenkwalder C, Lee HB, International Restless Legs Syndrome Study Group (2014) Restless legs syndrome/Willis–Ekbom disease diagnostic criteria: updated international restless legs syndrome study group (IRLSSG) consensus criteria–history, rationale, description, and significance. Sleep Med 15:860–873
Gowda S, Goldblum OM, McCall WV, Feldman SR (2010) Factors affecting sleep quality in patients with psoriasis. J Am Acad Dermatol 63(1):114–123. https://doi.org/10.1016/j.jaad.2009.07.003 Epub 2009 Nov 26
Leibowitz E, Seidman DS, Laor A, Shapiro Y, Epstein Y (1991) Are psoriatic patients at risk of heat intolerance? Br J Dermatol 124:439–442
Smolensky MH, Portaluppi F, Manfredini R, Hermida RC, Tiseo R, SackettLundeen LL et al (2015) Diurnal and twenty-four hour patterning of human diseases: acute and chronic common and uncommon medical conditions. Sleep Med Rev 21:12e22
Armstrong AW, Harskamp CT, Armstrong EJ (2013) Psoriasis and the risk of diabetes mellitus: a systematic review and meta-analysis. JAMA Dermatol 149:84–91
Gupta MA, Simpson FC, Gupta AK (2016) Psoriasis and sleep disorders: a systematic review. Sleep Med Rev 29:63–75. https://doi.org/10.1016/j.smrv.2015.09.003 Epub 2015 Sep 21
Callis Duffin K, Wong B, Horn EJ, Krueger GG (2009) Psoriatic arthritis is a strong predictor of sleep interference in patients with psoriasis. J Am Acad Dermatol 60(4):604–608. https://doi.org/10.1016/j.jaad.2008.10.059 Epub 2009 Jan 24
Papadavid E, Dalamaga M, Vlami K, Koumaki D, Gyftopoulos S, Christodoulatos GS, Papiris S, Rigopoulos D (2017) Psoriasis is associated with risk of obstructive sleep apnea independently from metabolic parameters and other comorbidities: a large hospital-based case-control study. Sleep Breath 21(4):949–958. https://doi.org/10.1007/s11325-017-1507-4 Epub 2017 May 8
Thaci D, Galimberti R, Amaya-Guerra M et al (2014) Improvement in aspects of sleep with etanercept and optional adjunctive topical therapy in patients with moderate-to-severe psoriasis: results from the PRISTINE trial. J Eur Acad Dermatol Venereol 28:900–906
Shalom G, Dreiher J, Cohen A (2016) Psoriasis and obstructive sleep apnea. Int J Dermatol 55(11):e579–e584. https://doi.org/10.1111/ijd.13367
Shutty BG, West C, Huang KE, Landis E, Dabade T, Browder B, O'Neill J, Kinney MA, Feneran AN, Taylor S, Yentzer B, McCall WV, Fleischer AB Jr, Feldman SR (2013) Sleep disturbances in psoriasis. Dermatol Online J 19(1):1
Strober BE, Sobell JM, Duffin KC, Bao Y, Guérin A, Yang H, Goldblum O, Okun MM, Mulani PM (2012) Sleep quality and other patient-reported outcomes improve after patients with psoriasis with suboptimal response to other systemic therapies are switched to adalimumab: results from PROGRESS, an open-label phase IIIB trial. Br J Dermatol 167(6):1374–1381. https://doi.org/10.1111/bjd.12000.Epub2012Nov
Henry AL, Kyle SD, Chisholm A, Griffiths CB (2017) A cross-sectional survey of the nature and correlates of sleep disturbance in people with psoriasis. Br J Dermatol 177:899–900
Funding
This research received no external funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The ethics committee gave its approval prior to initiation of the study. The study was conducted according to the principles of the Declaration of Helsinki.
Conflicts of interest
The authors declare that they have no conflict of interest.
Additional information
Comments
Sleep in a component of the 24hour daily cycle that is often ignored in clinical assessments. The authors have reminded us in this study the physiological tie between the brain and skin and just how strong the relationship is between a chronic inflammatory skin disease and the brain's control over sleep. The authors observed a range of sleep disturbances in the adult participants who had psoriasis, at a level of significance that was higher compared to age matched controls.
Margot Skinner
Dunedin, New Zealand
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Saçmacı, H., Gürel, G. Sleep disorders in patients with psoriasis: a cross-sectional study using non-polysomnographical methods. Sleep Breath 23, 893–898 (2019). https://doi.org/10.1007/s11325-019-01820-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11325-019-01820-8