
Abstract
Objectives
To develop a 3D cone-beam computed tomography (CBCT) method (CBCT method) for determining tooth sizes and arch dimensions and to compare the accuracy and reproducibility of that method with those of a previously described 3D segmented CBCT method (CBCT seg. method) and a 2D digital method.
Methods
Plaster study models and CBCT images were available for 34 patients. For the first method, the plaster study casts were digitalized and measured using the 2D digital method. For the second method, CBCT seg. method, the CBCT images were sent in DICOM format to InVivoDental® Company for segmentation and conversion into three-dimensional images of the models. For the third method, CBCT method, axial cuts were performed on the CBCT images, and tooth sizes and arch dimensions were measured using Anatomage® software.
Results
Significant differences were found between the tooth size measurements obtained with the 3D CBCT method and the 2D digital method, but not for the intercanine width, intermolar width, and arch length. There were no significant differences between the measurements obtained with the CBCT seg. method and the 2D digital method.
Conclusions
A 3D CBCT method has been developed. It presented good accuracy for the intercanine width, intermolar width, and arch length, but not for the mesiodistal tooth sizes. Model segmentation will be necessary for measurements of tooth size.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Cone-beam computed tomography (CBCT) represents a great advance for orthodontic diagnosis. However, because of the high radiation associated with conventional tomography (CT), it has never been used for orthodontic diagnosis in our clinical practice. In addition, two-dimensional (2D) radiographs cannot provide us with the same information as CBCT scans. With CBCT we can not only obtain three-dimensional (3D) craniofacial images, but also 3D images of teeth that can then be measured.
Craniofacial parameter measurements obtained by CBCT have already been reported in the literature. Some authors found differences between the parameters measured using conventional radiographs and those measured using CBCT, although the differences were not clinically significant [1–4]. Periago et al. [5] found that the differences between CBCT and 2D radiographs in the skull were <2 mm in most cases. Their results are similar to the findings of Lagravere et al. [6] and Ballrick et al. [7], who found differences of <1 and 0.1 mm, respectively.
In studies comparing CBCT with direct measurements on real skulls, Damstra et al. [8] found no differences, while Baumgaertel et al. [9] observed a slight underestimation. Another study compared CBCT images with periapical radiographs and found differences between these modalities, although CBCT scans were at least as accurate and reliable as periapical radiographs [10].
Two previous studies have been undertaken on patients to compare measurements on CBCT images using the InVivoDental® program (segmentations from images) with digital plaster models, and found no significant differences for tooth measurements [11, 12]. The only disadvantage of the InVivoDental® program, which provides segmentations from CBCT images to obtain 3D digital models, is that it involves a high cost for clinicians.
The aims of this study were (1) to develop a 3D CBCT method for determining mesiodistal tooth sizes, intercanine width, intermolar width, and arch length; (2) to compare the accuracy and reproducibility of this method and the 3D segmented CBCT method (CBCT seg. method) with a 2D digital method; and (3) to assess the need for making segmentations from CBCT images to obtain 3D digital models.
Materials and methods
This study was approved by the Ethics Committee on Human Research of the University of Valencia, Spain. Thirty-four patients at the Orthodontics Department of the Faculty of Dentistry (University of Valencia, Valencia, Spain) were randomly selected (age range 10.6–51.4 years). A CBCT scan and plaster study models were available for all of these patients as part of their orthodontic records.
The inclusion criteria were as follows: (1) permanent dentition from the first permanent molar; (2) absence of anomalies in the number, size, and dental shape; (3) good quality of study models; and (4) absence of large restorations or presence of prostheses.
The observers were blinded to any information of identity, medical history, and sample group for each subject evaluated. Points were located by the observers, who had extensive experience in interpreting CBCT scans and dental images, using the same standardized method.
2D digital method
A 2D digital method, designed at the University of Valencia, Spain, was used as a gold standard, because its accuracy and reproducibility for measuring plaster study models have previously been confirmed by several studies [13–16]. Through this method, using a conventional scanner and conventional plaster models, we obtained a 2D image of each dental arch. The 2D images were stored in a computer and analyzed using measurement software (Ortodig; University of Valencia, Valencia, Spain) (Fig. 1). The software helped us to mark the points for the mesiodistal sizes of each tooth, intercanine width, intermolar width, and arch length, on the images of the casts. Finally, the software designed for this purpose automatically determined the dental sizes in millimeters from these data.

Measurement of mesiodistal tooth sizes (TS) using three methods: digital method, CBCT seg. method, and CBCT method
3D CBCT segmented method
The second method evaluated was the 3D CBCT seg. method. The CBCT scanner used was a Dental Picasso Master 3D® (EWOO Technology, Seoul, Republic of Korea). The patients were scanned in full occlusion to allow use of the images for cephalometric purposes. The slice thickness was 0.1 mm and the scanning angle covered was 360°, thus generating a large number of slice images. The voxel size was 0.4 mm, the tube voltage range was 40–90 kV, and the intensity range was 2–10 mA. The computer software used to analyze the 3D images was the InVivoDental® program (Anatomage®; InVivoDental® Company, San Jose, CA, USA). CBCT images in DICOM format were safely sent to the website of InVivoDental® Company for segmentation and conversion into three-dimensional images of the models (Fig. 1). This allowed use of the CBCT seg. method.
3D CBCT method
For the 3D CBCT method, axial cuts were performed on the CBCT images at the level of the incisal edges and occlusal surfaces of the maxillary and mandibular teeth (Fig. 1).
Measurements
We proceeded to undertake measurements using the three measurement methods (2D digital method, CBCT seg. method, and CBCT method). The measurements taken were as follows:
-
1.
Mesiodistal tooth sizes (TS): these sizes corresponded to the maximum width and distance between the mesial and distal anatomical contact points. The second and third molars, both upper and lower, were excluded.
-
2.
Intercanine width (ICW): this width was defined as the linear distance between the cusp tips of both canines or the center of wear facets, should they be present, in both the maxilla and the mandible.
-
3.
Intermolar width (IMW): this width was defined as the maximum distance between the vestibular surfaces of the first permanent molars on one or other side of the arch, both upper and lower.
-
4.
Arch length (AL): this length was defined as a line passing through the ideal points of contact of each tooth, and was obtained by joining the most mesial and distal points of each tooth selected, from the mesial side of the first molar to the mesial side of the contralateral molar, in the maxilla and the mandible. This measurement was based on a subjectively assessed ideal arch.
Statistical analysis
The reproducibility of the methods was analyzed by determining intraobserver and interobserver measurement errors, which were calculated as coefficients of variation (CVs). These CVs (CV = SD × 100/mean) were expressed as percentages (%). To estimate the measurement errors and assess intraobserver reproducibility, the principal observer made a second measurement using both methods on a subsample of 20 randomly selected CBCT images (600 measurements) at an interval of 1 week after the first measurement. To estimate interobserver reproducibility, a second observer made the same measurements on these 20 CBCT images at the same interval of 1 week after the first measurement. This second observer, who had the same extensive experience in interpreting CBCT scans and dental images as the main observer, performed the same procedures to calculate the errors of the three methods.
All data from the samples and for the three methods were checked using the Kolmogorov–Smirnov test to determine whether they followed a normal distribution, and the significance for each variable under analysis was obtained. The resulting data showed that all of the variables followed a normal distribution, with significance values ranging from 0.144 to 0.999.
To compare mean values, a paired Student’s t test was used. The correlations between the variables for the three methods were determined using Pearson’s correlation coefficients, with estimations of the slope and ordinate at the origin and their respective 95 % confidence intervals.
The discrepancies among the three methods were assessed by calculating the differences between the mean values of a measurement taken using the three methods, and expressed as percentages.
All statistical analyses were performed with a standard statistical software package (SPSS v.15.0; SPSS Inc., Armonk, NY, USA).
Results
The CVs for the intraobserver and interobserver errors for the digital method, CBCT seg. method, and CBCT method are shown in Table 1. The ANOVAs revealed differences between the three methods. Specifically, there were significant differences between the CBCT method and the digital method and between the CBCT method and CBCT seg. method. The ANOVA produced values of p < 0.005, with the CBCT method having clearly different mean values compared with the other two more homogeneous methods.
Table 2 shows the TS, ICW, IMW, and AL data as means and SDs, respectively, for the three methods, as well as comparisons of the CBCT method and CBCT seg. method with the digital method.
Table 3 shows the mean differences, SDs, discrepancies, and p values in the determination of the TS, ICW, IMW, and AL measurements between two methods: CBCT method vs. digital method and CBCT seg. method vs. digital method. Significant differences (p ≤ 0.05) are marked in grey.
Table 4 shows the slopes and ordinates at origin (95 % CI) and the correlation coefficients for the regression analysis in each group for the CBCT method and the CBCT seg. method relative to the 2D digital method, respectively. The measurements that included a 0 in the ordinate at the origin and a 1 in the slope are highlighted in grey.
Discussion
Both plaster and digital (2D) study models have been important diagnostic tools for drawing up a suitable treatment plan for a long time, while three-dimensional models have become valuable in recent years. The measurements that we normally carry out on these models were used in our study to check whether the measurements undertaken by the CBCT method and the CBCT seg. method were as reliable as those taken by the 2D digital method (gold standard).
The reproducibility of dental measurements in the CBCT seg. method has been proven, as the digital method and CBCT seg. method have similar CVs, with the CVs of the CBCT seg. method being slightly higher.
We found some studies in the literature that compared the CBCT seg. method with the digital method. Our results are consistent with the studies of Lagravere et al. [6], Ballrick et al. [7], Baumgaertel et al. [9], Tarazona et al. [12], and Liu et al. [17]. The CVs for the CBCT Method were slightly higher than those for the other two methods. The interobserver CVs were slightly higher than the intraobserver CVs in all of the measurements for both CBCT methods. These discrepancies possibly arose because the second observer was less experienced than the first observer, when it came to locating the different points.
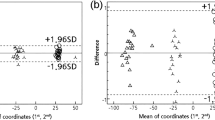
In our study, we checked the accuracy of dental measurements in humans. On comparing the measurements obtained by the CBCT seg. method and the same measurements obtained by the digital method, we observed that the measurements obtained with the two methods were equal, with significant differences only existing for the mesiodistal size of the first upper left molar size and for the upper IMW (Table 3). The adjustment line comparing these two methods (Fig. 2a) showed that all of the measurements analyzed were close to the bisection and that the estimated line perfectly overlapped the main diagonal. However, in addition to the individual measurements, we analyzed the confidence intervals of the slope and ordinate at the origin (Table 4). To consider that the two measurement methods are comparable, the correlation coefficients must be high and the confidence intervals of the slope and ordinate at the origin must contain 1 and 0, respectively. This ensures that there are no systemic differences in the measurements (which would occur if the confidence level of the ordinate did not contain 0) and that an increase in the size of the object measured would represent the same increase in the two measurement methods (which would not occur if the confidence level of the slope did not contain 1).

Dispersion diagram for all of the data: mesiodistal tooth sizes (TS; purple color), intercanine width (ICW; blue color), intermolar width (IMW; green color), and arch length (AL; yellow color). a Ordinates (digital method) vs. abscissae (CBCT segmented method). b Ordinates (digital method) vs. abscissae (CBCT method) (color figure online)
In this case, all of the measurements (TS, ICW, IMW, and AL) fulfilled the requirements for the above situation. Therefore, we can state that the CBCT seg. method is accurate for measuring TS, ICW, IMW, and AL. These results coincide with those of Tarazona et al. [12].
Second, on comparing the data obtained with the CBCT method and the digital method, we observed that in this case, there were more significant differences than in the previous case, because there were differences between the upper incisors (central and lateral) and upper and lower canines, and in the AL, lower ICW, and IMW (Table 3). The adjustment line comparing the CBCT method and the digital method (Fig. 2b) showed that all of the measurements analyzed were close to the bisection, but in a more dispersed way than before. The regression lines did not perfectly overlap the main diagonal of the quadrant, although the ordinate at the origin and the slope included 0 and 1 for all measurements (ICW, IMW, and AL) except for the TS (Table 4). Therefore, we can say that the CBCT method is not as accurate for measuring mesiodistal tooth sizes as the CBCT seg. method, perhaps because of the clearer visibility of the tooth outlines in the latter method compared with the former method.
Our results suggest that 3D CBCT seg. method measurements provide us with much more information than the 2D digital method. We can measure not only teeth that have already erupted, but also teeth that have not erupted at all. Moreover, we can more accurately measure cases with crowding teeth, and reliably measure all teeth. In conclusion:
-
1.
An easy and fast 3D CBCT method has been developed to determine mesiodistal tooth sizes, intercanine width, intermolar width, and arch length.
-
2.
This method presented good intraobserver and interobserver reproducibilities.
-
3.
The CBCT seg. method presented great accuracy regarding mesiodistal tooth sizes, intercanine width, intermolar width, and arch length compared with the 2D digital method, while the CBCT method presented good accuracy only for the intercanine width, intermolar width, and arch length, but not for the mesiodistal tooth sizes.
-
4.
Segmentation from the CBCT images is necessary for measuring tooth sizes, since the measurements on the axial cuts from the CBCT images (CBCT method) were not sufficiently accurate.
References
Hilgers ML, Scarfe WC, Scheetz JP, Farman AG. Accuracy of linear temporomandibular joint measurements with cone beam computed tomography and digital cephalometric radiography. Am J Orthod Dentofac Orthop. 2005;128:803–11.
Moshiri M, Scarfe WC, Hilgers ML, Scheetz JP, Silveira AM, Farman AG. Accuracy of linear measurements from imaging plate and lateral cephalometric images derived from cone-beam computed tomography. Am J Orthod Dentofac Orthop. 2007;132:550–60.
Hassan B, Van der Stelt P, Sanderink G. Accuracy of three-dimensional measurements obtained from cone beam computed tomography surface-rendered images for cephalometric analysis: influence of patient scanning position. Eur J Orthod. 2009;31:129–34.
Berco M, Rigali P, Miner M, Deluca S, Anderson N, Will L. Accuracy and reliability of linear cephalometric measurements from cone-beam computed tomography scans of a dry human skull. Am J Orthod Dentofac Ortho. 2009;136(17):e1–17.
Periago D, Scarfe W, Moshiri M, Scheetz J, Silveira A, Farman A. Linear accuracy and reliability of cone beam CT derived 3-dimensional images constructed using an orthodontic volumetric rendering program. Angle Orthod. 2008;78:387–95.
Lagravere MO, Carey J, Toogood RW, Major PW. Three-dimensional accuracy of measurements made with software on cone-beam computed tomography images. Am J Orthod Dentofac Orthop. 2008;134:112–6.
Ballrick JW, Palomo JM, Ruch E, Amberman BD, Hans MG. Image distortion and spatial resolution of a commercially available cone-beam computed tomography machine. Am J Orthod Dentofac Orthop. 2008;134:573–82.
Damstra J, Fourie Z, Huddleston Slater JJ, Ren Y. Accuracy of linear measurements from cone-beam computed tomography-derived surface models of different voxel sizes. Am J Orthod Dentofac Orthop. 2010;137(16):e1–6.
Baumgaertel S, Palomo JM, Palomo L, Hans MG. Reliability and accuracy of cone-beam computed tomography dental measurements. Am J Orthod Dentofac Orthop. 2009;136:19–28.
Sherrard JF, Rossouw PE, Benson BW, Carrillo R, Buschang PH. Accuracy and reliability of tooth and root lengths measured on cone-beam computed tomographs. Am J Orthod Dentofac Orthop. 2010;137:S100–18.
Kau CH, Littlefield J, Rayny N, Nguyen J, Creed B. Evaluation of CBCT digital models and traditional models using the little index. Angle Orthod. 2010;80:435–9.
Tarazona B, Llamas JM, Cibrian R, Gandia JL, Paredes V. A comparison between dental measurements taken from CBCT models and those taken from a digital method. Eur J Orthod. 2013;35:1–6.
Leifert MF, Leifert MM, Efstratiadis SS, Cangialosi TJ. Comparison of space analysis evaluations with digital models and plaster dental casts. Am J Orthod Dentofac Orthop. 2009;136(16):e1–4.
Bootvong K, Liu Z, McGrath C, Hägg U, Wong RW, Bendeus M, et al. Virtual model analysis as an alternative approach to plaster model analysis: reliability and validity. Eur J Orthod. 2010;32:589–95.
Paredes V, Gandía JL, Cibrián R. A new, accurate and fast digital method to predict unerupted tooth-size. Angle Orthod. 2006;76:14–9.
Paulino V, Paredes V, Gandía JL, Cibrián R. Prediction of arch length based on intercanine width. Eur J Orthod. 2008;30:295–8.
Liu Y, Olszewskib R, Alexandronic ES, Enciso R, Xue T, Mah JK. The validity of in vivo tooth volume determinations from cone-beam computed tomography. Angle Orthod. 2010;80:160–6.
Conflict of interest
Yanira Hernandez, Beatriz Tarazona, Natalia Zamora, Rosa Cibrian, Jose Luis Gandia, and Vanessa Paredes declare that they have no conflict of interest.
Human rights statement and informed consent
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and later versions. Informed consent was obtained from all patients for being included in the study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Hernandez, Y., Tarazona, B., Zamora, N. et al. Comparative study of reproducibility and accuracy in measuring mesiodistal tooth sizes using three different methods: 2D digital, 3D CBCT, and 3D CBCT segmented. Oral Radiol 31, 165–172 (2015). https://doi.org/10.1007/s11282-015-0204-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11282-015-0204-x