
Abstract
The purpose of this study was to compare the accuracy of digital dental casts from plaster cast scanning (PCS), impression scanning (IPS), intraoral scanning (IOS), and cone-beam computed tomography (CBCT) scanning (CCS) methods. The maxillary and mandibular dental casts of 15 patients who needed CBCT scans for oral examination or treatment were digitized via four methods. 12 linear distance measurements of all digital dental casts were selected and acquired with software and compared to those of the reference plaster cast to evaluate the dimensional accuracy. Three-dimensional deviation analysis of the IPS, IOS and CCS groups with respect to the reference PCS group was performed to evaluate the morphological accuracy. The discrepancy in linear distances between the digital dental casts and reference plaster casts was statistically significant (p < 0.01). The dimensional accuracies of the PCS (0.06 ± 0.12 mm) and IPS (0.03 ± 0.05 mm) casts were better than those of the IOS (0.37 ± 0.30 mm) and CCS (0.54 ± 0.40 mm) casts. The one-sample t test showed that there were statistically significant differences between the discrepancies in 8 of the linear distances for the PCS group and 9 of the linear distances for the IPS group between the digital dental casts and reference plaster casts, with an ideal error of 0.00 (p < 0.05). The sequence of morphological accuracy from good to poor was maxillary and mandibular IPS, mandibular IOS; maxillary IOS; and maxillary and mandibular CCS. The accuracy of the digital dental casts from the PCS and IPS methods was greater than that of IOS and CCS methods. Although accuracy of the digital dental cast from IOS was low, it satisfied the clinical requirements for fixed restorations in small units. The accuracy of the digital dental cast from CCS was poorest and could only be used for procedures with lower accuracy requirements.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Dental casts, whether acquired from either conventional impression methods or digital scanning methods, can be used for treatment planning, restoration designing and manufacturing in several disciplines, such as prosthodontics, oral implantology and orthodontics [1]. The traditional method of acquiring dental casts is to pour a plaster cast after making an impression. Developments in digital technology have led to the widespread use of digital dental casts, which form the basis of digital design and manufacturing, in dental treatment, as they are more environmentally friendly and occupy less space than plaster casts [2]. Methods for acquiring digital dental casts included plaster cast scanning, impression scanning, and intraoral scanning techniques and cone-beam computed tomography (CBCT) reconstruction [3,4,5,6,7,8].
Many studies have compared the different levels of accuracy in the digital dental casts acquired from these different methods, most of which have used the plaster casts measured with Vernier calipers as a reference, while others have used the digital dental casts derived from plaster cast scanning methods [4, 5, 7,8,9,10,11,12,13,14]. Two studies evaluated the morphological accuracy of digital dental casts acquired from CBCT reconstruction with respect to plaster casts and showed that the CBCT dental casts had large errors [7, 8]. One study evaluated the accuracy of digital dental casts acquired from plaster cast and impression scanning methods using the same CBCT device with respect to plaster casts measured by Vernier calipers [4]. One study evaluated the accuracy of digital dental casts acquired from plaster cast scanning and CBCT reconstruction methods with respect to plaster casts measured by Verner calipers [5]. A similar study evaluated the morphological accuracy of digital dental casts acquired from intraoral scanning and CBCT reconstruction methods with respect to the digital casts acquired from scanning plaster casts [10]. However, these previous studies did not clearly compare the dimensional and morphological accuracies of the digital dental casts in terms of the healthy and complete dentition derived from plaster cast scanning, impression scanning, intraoral scanning and CBCT scanning methods at the same time.
Therefore, the aim of this study was to compare and evaluate the dimensional and morphological accuracies of digital dental casts acquired from plaster cast scanning (PCS), impression scanning (IPS), intraoral scanning (IOS) and CBCT scanning (CCS) methods using healthy and complete dentition in vivo as research objects. The null hypothesis was that no significant differences would exist in terms of the dimensional and morphological accuracies among the different digital dental casts and that no significant differences would exist between the discrepancies in the linear distances measured for each digital dental cast and an ideal error of 0.00.
Materials and methods
Ethical approval was granted by the Peking University School and Hospital of Stomatology (PKUSSIRB‑202162027), and all patients provided informed consent.
Fifteen patients (9 females and 6 males; mean age 25.46 years) who needed CBCT scan for oral examination or treatment were selected for this study. The inclusion criteria were as follows: complete maxillary and mandibular dentition; and no maxillofacial tumors or deformities. The exclusion criteria were as follows: ongoing orthodontic treatment; metal restorations in the maxillary or mandibular dentition; and no independent behavioral or presentational disabilities. The sample size was calculated with a statistical software program (PASS 15.0; NCSS) based on the discrepancy in the linear distances between the digital dental casts and reference plaster casts and the root mean square (RMS) of the digital dental casts obtained in a pilot experiment according to 1-way analysis of variance (ANOVA) and a power value of 0.8, resulting in 8 and 12 participants, respectively. Based on the results of this calculation and similar studies reported previously [10], a 15-participant sample size was used.
Acquisition of four kinds of digital dental cast
The digitization devices used in this study included a desktop optical scanner with a 0.005 mm voxel size (OS) (D2000, 3Shape A/S, Copenhagen, Denmark), an intraoral scanner with a 0.02 mm voxel size (Trios 3, 3Shape A/S, Copenhagen, Denmark) and a CBCT scanning device with a 0.3 mm voxel size (i-CAT System, Imaging Sciences International, Hatfield, USA).
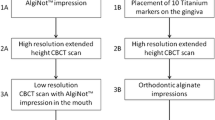
Maxillary and mandibular impressions were taken by addition silicone (Variotime Light Flow and Variotime Monophase, Gussa Dental, Hanau, Germany) using a double-mixing method and scanned with an OS device after disinfection using a UV disinfection cabinet and properly trimmed to obtain the digital dental casts from IPS. At the same time, the maxillary and mandibular dentitions of the patients were scanned by an IOS device; the scanning protocol was based on the manufacturer’s instructions and is described as follows. Each arch’s occlusal surface was scanned with a smooth movement, starting at the last tooth on the left. The scanner head was then turned 45° to scan the palatal surfaces and turned 45° again in the opposite direction to scan the buccal surfaces, finally yielding the IOS-based digital dental casts. Then, the plaster cast was poured with die stone (Dento–Stone, Dentona, Dortmund, Germany) and scanned with the OS device, yielding the PCS-based digital dental casts. Maxillofacial CBCT scanning was performed with the maxillary and mandibular dentition separated using a yarn roll under the following conditions: 120 kV; 5 mA; exposure time 3708 ms. The CBCT scanning casts were stored in DICOM file format and processed in the Mimics software program (Mimics 21.0, Materialise NV, Leuven, Belgium), in which the digital dental casts were obtained by segmentation with the enamel and dentin thresholds and reconstruction with the recommended “optimal” quality parameter. All digital dental casts were saved and exported in standard tessellation language (STL) file format (Fig. 1).

Four kinds of digital dental casts. A Plaster cast scanning (PCS). B Impression scanning (IPS). C Intraoral scanning (IOS). D CBCT scanning (CCS)
Linear distance measurements
Six anatomical landmarks of the maxillary teeth and six of the mandibular teeth were selected, allowing the measurement of 12 linear distances (Table 1). These linear distances for all digital dental casts were measured in the Geomagic software program (Geomagic studio 2014, 3D Systems, NC, USA). The corresponding linear distances for the plaster cast were directly measured with a Vernier caliper to serve as the reference due to the inability to directly measure these distances with the Vernier caliper in the mouth. For each linear measurement, the mean of the three separate measurements was calculated by the same person. The absolute value of the linear distance of each digital dental cast minus the linear distance of the plaster cast was taken as the discrepancy in the linear distance between the digital dental casts and plaster cast as a control, which was performed to evaluate the dimensional accuracy of the casts.
Three-dimensional deviation analysis
The STL files of the PCS, IPS, IOS and CCS-based casts were imported into the Geomagic software program. The dentitions of all digital dental casts were selected along the gingival margin using the “selected bounded components” function, trimming all nonessential data such as soft tissue and areas outside the gingivobuccal regions. Next, registration using the “best-fit alignment” function and 3D deviation analysis of the digital dental casts from the IPS, IOS and CCS methods with respect to the reference digital dental cast from the PCS method, recorded as the root mean square (RMS), were performed to evaluate the morphological accuracy of the casts.
Statistical analysis
In SPSS software (SPSS Statistics 23.0, IBM, New York, USA), the Shapiro‒Wilk test was used to confirm the normality of the distribution of the data. One-way ANOVA was used to compare the discrepancy in the linear distances and the RMS among the digital dental casts. The one-sample t test was used to compare the discrepancy in the linear distances between the digital dental casts and the ideal error of 0.00 (α = 0.05).
Results
Compared with the control group, the discrepancy in the linear distances among the digital dental casts was statistically significant (p < 0.01) (Table 2). The discrepancy in the linear distances of the PCS and IPS casts was statistically smaller than that of the IOS and CCS casts, respectively (p < 0.01). There was no statistically significant difference in terms of the discrepancy in linear distances between the PCS and IPS casts or between the IOS and CCS casts (p > 0.05). The dimensional accuracies of the PCS (0.06 ± 0.12 mm) and IPS casts (0.03 ± 0.05 mm) were better than those of the IOS (0.37 ± 0.30 mm) and CCS casts (0.54 ± 0.40 mm).
The one-sample t test showed that there were statistically significant differences for 8 of the linear distances for the PCS group and 9 linear distances for the IPS group in terms of the discrepancy between the digital dental casts and the ideal error of 0.00 (p < 0.05). Furthermore, there were statistically significant differences in the discrepancies of all linear distances for the IOS group and the CCS group between the digital dental casts and the ideal error of 0.00 (p < 0.01) (Tables 3, 4).
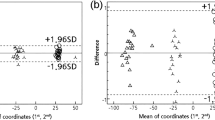
The RMS value was significantly different among the IPS, IOS and CCS groups with respect to the PCS group (p < 0.01) (Table 5). Compared with those of the reference PCS group, the distances, ranked from smallest to largest RMS values, were the maxillary and mandibular distances of the IPS group, the mandibular distances of the IOS group, the maxillary distances of the IOS group, and the maxillary and mandibular distances of the CCS group (Fig. 2).

Three-dimensional deviation analysis for 3 kinds of digital dental casts with respect to the reference PCS group. A, B Maxillary and mandibular IPS. C, D Maxillary and mandibular IOS. E, F Maxillary and mandibular CCS
Discussion
Based on the findings, the null hypothesis that no significant differences existed in terms of dimensional and morphological accuracies among the different digital dental casts and that no significant differences existed in terms of the discrepancy in the linear distances between each digital dental cast and the ideal error of 0.00 were rejected.
Digital dental casts are the basis of digital diagnosis and treatment, the accuracy of which can directly influence the effect of restoration. Most studies that evaluated the accuracy of digital dental casts only used either the dimensional accuracy or the morphological accuracy as the evaluation indicator [6, 15, 16]. The dimensional accuracy mostly refers to the discrepancy in the linear distances between digital dental casts and plaster casts measured with a Vernier caliper as a control group [15, 16]. Morphological accuracy mostly refers to the morphological discrepancy between digital dental casts derived from IPS and IOS and casts derived from PCS [6, 17].
The linear distances of the plaster casts, measured with a Vernier caliper, were used as the control group when evaluating the dimensional accuracy of digital dental casts in this study, consistent with previous studies [5, 7, 11]. The digital dental cast derived from PCS was used as the control group while evaluating the morphological accuracy of the digital dental casts in this study, consistent with similar studies [10, 16].
The absolute value of the discrepancies in the linear distances from the digital dental casts with respect to the plaster casts was used as the discrepancy value of the digital dental casts when evaluating the dimensional accuracy of the digital dental casts, because the discrepancies in the linear distances between the digital dental casts and reference plaster cast were the mainly focus of this study, regardless of whether the discrepancies were positive or negative, consistent with similar studies [18, 19].
The actual accuracy was inevitably lower than the ideal accuracy (an ideal error of 0.00) due to possible errors resulting from the impression [20], the plaster cast creation, the registration and the scanning processes.
The dimensional and morphological accuracies of the PCS group and IPS group were better than those of the IOS group and CCS group. The accuracy of the IPS casts could be affected by the presence of an undercut in the impression of the complete dentition, especially for dentitions with obvious gingival recession. However, the problem mentioned above would be avoided in scanning prepared teeth without undercuts, such as when preparing teeth for full-crown implants.
The average error in terms of the linear distance of the IOS group (0.37 ± 0.30 mm) was larger than that of the PCS group (0.06 ± 0.12 mm) and IPS group (0.03 ± 0.05 mm). The RMS of the mandibular IOS group (0.118 ± 0.034 mm) was smaller than that of the maxillary IOS group (0.217 ± 0.080 mm), which is consistent with a previous study [10]. Because the mandibular dentition was more clearly visualized and smaller than the maxillary dentition, which made it easier to perform the corresponding image processing and reconstruction, the accuracy of the mandibular dentition was higher than that of maxillary dentition [21]. The accuracy of the IOS cast decreases as the scanning range increasing, and thus IOS is recommended for use in the restoration of full-crown or fixed partial dentures with less than half an arch [22]. In addition, scanning in sections is recommended when IOS is used for multiple units of fixed restoration over half an arch [22].
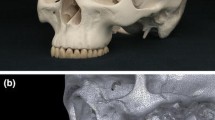
During the CBCT scanning procedure, the accuracy of the CCS cast is higher in the open-mouth position than in the closed-mouth position [23] but decreases if metal restorations are present [24]. As a result, to optimize the accuracy of the CCS casts in this study, subjects with metal restorations in the dentition were excluded, and the maxillary and mandibular dentitions were separated with a yarn roll, creating an open-mouth position. In addition, the quality parameter was set to “optimal” during the CBCT reconstruction process as recommended by the Mimics software program in this study. Under the above conditions, the average error in terms of the linear distance for the CCS group was the largest (0.54 ± 0.40 mm) among these 4 groups, which is consistent with most previous studies [5, 7, 8]. For morphological accuracy, the tooth morphology of the CCS group seemed larger than that of the actual teeth, and the RMS of the CCS group was the largest, with the main discrepancy mainly located in the occlusal surface of the posterior tooth, which is similar to one study [10]. Although the consensus on the discrepancy range of clinically acceptable dental casts was deficient, some researchers have recommended that the discrepancy range from 0.15 to 0.20 mm [25, 26], which is much smaller than the discrepancies of the CCS group in this study. Due to its poor accuracy, CCS should only be recommended for procedures requiring lower accuracy, such as digital orthodontic planning, model archiving [8] or individual trays [27], not for those with high accuracy requirements, such as full-crown or fixed partial dentures.
The limitation of this study was the use of plaster casts as a reference group. The gold standard for such comparisons would be a measurement of the intraoral distances, but this was unfeasible due to the inability to use the Vernier caliper in the mouth. The potential in this compromise, thus, needs to be recognized. Nevertheless, the credibility of the control that was used is in line with previous studies and can be considered acceptable [4, 5, 7,8,9,10,11,12,13].
Conclusion
Within the limitations of this current study, it was concluded that the accuracy of the digital dental casts based on plastic cast scanning and impression scanning was greater than that of the casts based on intraoral scanning and CBCT scanning. Although the accuracy of the digital dental casts based on intraoral scanning was low, it satisfied the clinical requirements. The accuracy of the digital dental casts based on CBCT scanning was poorest and should only be used for special procedures with lower accuracy requirements.
References
Walker MP, Rondeau M, Petrie C, Tasca A, Williams K. Surface quality and long-term dimensional stability of current elastomeric impression materials after disinfection. J Prosthodont. 2007;16(5):343–51. https://doi.org/10.1111/j.1532-849X.2007.00206.x.
Tomita Y, Uechi J, Konno M, Sasamoto S, Iijima M, Mizoguchi I. Accuracy of digital models generated by conventional impression/plaster-model methods and intraoral scanning. Dent Mater J. 2018;37(4):628–33. https://doi.org/10.4012/dmj.2017-208.
Ho CT, Lin HH, Lo LJ. Intraoral scanning and setting up the digital final occlusion in three-dimensional planning of orthognathic surgery: its comparison with the dentalmodel approach. Plast Reconstr Surg. 2019;143(5):1027–36. https://doi.org/10.1097/PRS.0000000000005556.
Rangel FA, Maal TJ, Bronkhorst EM, Breuning KH, Schols JG, Bergé SJ, Kuijpers-Jagtman AM. Accuracy and reliability of a novel method for fusion of digital dental casts and cone beam computed tomography scans. PLoS ONE. 2013;8(3): e59130. https://doi.org/10.1371/journal.pone.0059130.
Kim J, Heo G, Lagravere MO. Accuracy of laser-scanned models compared to plaster models and cone-beam computed tomography. Angle Orthod. 2014;84(3):443–50. https://doi.org/10.2319/051213-365.1.
Kihara H, Hatakeyama W, Komine F, Takafuji K, Takahashi T, Yokota J, Oriso K, Kondo H. Accuracy and practicality of intraoral scanner in dentistry: a literature review. J Prosthodont Res. 2020;64(2):109–13. https://doi.org/10.1016/j.jpor.2019.07.010.
Akyalcin S, Dyer DJ, English JD, Sar C. Comparison of 3-dimensional dental models from different sources: diagnostic accuracy and surface registration analysis. Am J Orthod Dentofacial Orthop. 2013;144(6):831–7. https://doi.org/10.1016/j.ajodo.2013.08.014.
Becker K, Schmucker U, Schwarz F, Drescher D. Accuracy and eligibility of CBCT to digitize dental plaster casts. Clin Oral Investig. 2018;22(4):1817–23. https://doi.org/10.1007/s00784-017-2277-x.
De Luca CG, Pacheco-Pereira C, Lagravere MO, Flores-Mir C, Major PW. Intra- arch dimensional measurement validity of laser-scanned digital dental models compared with the original plaster models: a systematic review. Orthod Craniofac Res. 2015;18(2):65–76. https://doi.org/10.1111/ocr.12068.
Emara A, Sharma N, Halbeisen FS, Msallem B, Thieringer FM. Comparative evaluation of digitization of diagnostic dental cast (plaster) models using different scanning technologies. J Dent (Basel). 2020;8(3):79. https://doi.org/10.3390/dj8030079.
Grunheid T, Patel N, De Felippe NL, Wey A, Gaillard PR, Larson BE. Accuracy, reproducibility, and time efficiency of dental measurements using different technologies. Am J Orthod Dentofac Orthop. 2014;145(2):157–64. https://doi.org/10.1016/j.ajodo.2013.10.012.
Creed B, Kau CH, English JD, Xia JJ, Lee RP. A Comparison of the accuracy of linear measurements obtained from cone beam computerized tomography images and digital models. Semin Orthod. 2011;17(1):49–56. https://doi.org/10.1053/j.sodo.2010.08.010.
Im J, Cha JY, Lee KJ, Yu HS, Hwang CJ. Comparison of virtual and manual tooth setups with digital and plaster models in extraction cases. Am J Orthod Dentofac Orthop. 2014;145(4):434–42. https://doi.org/10.1016/j.ajodo.2013.12.014.
Leifert MF, Leifert MM, Efstratiadis SS, Cangialosi TJ. Comparison of space analysis evaluations with digital models and plaster dental casts. Am J Orthod Dentofac Orthop. 2009;136(1):16e11-14. https://doi.org/10.1016/j.ajodo.2008.11.019.
Yousef H, Harris BT, Elathamna EN, Morton D, Lin WS. Effect of additive manufacturing process and storage condition on the dimensional accuracy and stability of 3D-printed dental casts. J Prosthet Dent. 2021. https://doi.org/10.1016/j.prosdent.2021.02.028.
Joda T, Matthisson L, Zitzmann NU. Impact of aging on the accuracy of 3d-printed dental models: an in vitro investigation. J Clin Med. 2020;9(5):1436. https://doi.org/10.3390/jcm9051436.
Liczmanski K, Stamm T, Sauerland C, Blanck-Lubarsch M. Accuracy of intraoral scans in the mixed dentition: a prospective non-randomized comparative clinical trial. Head Face Med. 2020;16(1):11. https://doi.org/10.1186/s13005-020-00222-6.
Ye H, Lv L, Liu Y, Liu Y, Zhou Y. Evaluation of the accuracy, reliability, and reproducibility of two different 3d face-scanning systems. Int J Prosthodont. 2016;29(3):213–8.
Rosati R, De Menezes M, Rossetti A, Sforza C, Ferrario VF. Digital dental cast placement in 3-dimensional, full-face reconstruction: a technical evaluation. Am J Orthod Dentofac Orthop. 2010;138(1):84–8. https://doi.org/10.1016/j.ajodo.2009.10.035.
Hirota Y, Tawada Y, Komatsu S, Watanabe F. Effect of impression holding time and tray removal speed on the dimensional accuracy of impressions for artificial abutment tooth inclined. Odontology. 2021;109(1):157–67. https://doi.org/10.1007/s10266-020-00537-5.
Goracci C, Franchi L, Vichi A, Ferrari M. Accuracy, reliability, and efficiency of intraoral scanners for full-arch impressions: a systematic review of the clinical evidence. Eur J Orthod. 2016;38(4):422–8. https://doi.org/10.1093/ejo/cjv077.
Su TS, Sun J. Comparison of repeatability between intraoral digital scanner and extraoral digital scanner: an in-vitro study. J Prosthodont Res. 2015;59(4):236–42. https://doi.org/10.1016/j.jpor.2015.06.002.
Hassan B, Couto Souza P, Jacobs R, de Azambuja BS, van der Stelt P. Influence of scanning and reconstruction parameters on quality of three-dimensional surface models of the dental arches from cone beam computed tomography. Clin Oral Investig. 2010;14(3):303–10. https://doi.org/10.1007/s00784-009-0291-3.
Gamba TO, Oliveira ML, Flores IL, Cruz AD, Almeida SM, Haiter-Neto F, Lopes SL. Influence of cone-beam computed tomography image artifacts on the determination of dental arch measurements. Angle Orthod. 2014;84(2):274–8. https://doi.org/10.2319/040313-255.1.
Imburgia M, Logozzo S, Hauschild U, Veronesi G. Accuracy of four intraoral scanners in oral implantology: a comparative in vitro study. BMC Oral Health. 2017;17(1):92. https://doi.org/10.1186/s12903-017-0383-4.
Zhang F, Suh KJ, Lee KM. Validity of intraoral scans compared with plaster models: an in-vivo comparison of dental measurements and 3d surface analysis. PLoS ONE. 2016;11(6): e0157713. https://doi.org/10.1371/journal.pone.0157713.
Huang Z, Wang XZ, Hou YZ. Novel method of fabricating individual trays for maxillectomy patients by computer-aided design and rapid prototyping. J Prosthodont. 2015;24(2):115–20. https://doi.org/10.1111/jopr.12183.
Acknowledgements
This work was supported by the National Natural Science Foundation of China (81801015), the National Key R&D Program of China (2018YFB1106900), the Program for New Clinical Techniques and Therapies of PKUSS (PKUSSNCT-20B07) and the PKU‑Baidu Fund (2019BD021). The authors would like to express their gratitude to SpringerNature (https://authorservices.springernature.com/) for the expert linguistic services provided.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests in relation to the present study.
Ethical approval
This study included 15 patients (9 females and 6 males; mean age 25.46 years). All procedures performed in the present study involving human participants were in accordance with the Declaration of Helsinki. Ethical approval was granted by Peking University School and Hospital of Stomatology (PKUSSIRB‑202162027).
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Ye, J., Wang, S., Wang, Z. et al. Comparison of the dimensional and morphological accuracy of three-dimensional digital dental casts digitized using different methods. Odontology 111, 165–171 (2023). https://doi.org/10.1007/s10266-022-00736-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10266-022-00736-2