
Abstract
Objectives
The purpose of the present study was to determine the inclination and height of the articular eminence with respect to the condylar bone changes, condyle shape, fossa shape and condylar movements in patients with and without temporomandibular joint (TMJ) dysfunction using cone-beam computed tomography (CBCT).
Methods
The associations between the eminence inclination and the condylar bone changes, condylar movements, condylar shape and fossa shape were evaluated in patients with TMJ disorders and control patients without TMJ disorders. The measurements of the articular eminence inclination were established on central sagittal slices of the TMJ. The central coronal slices were used to determine the condyle and fossa shapes. The types of movements of the condyles were determined on open-mouth images, and mandibular hypermobility or hypomobility was noted for each joint.
Results
There were no significant differences in the eminence inclination and height with respect to the condylar bone changes and condylar movements in the TMJ disorder group. However, there was a significant association between the eminence inclination and the fossa shape in the TMJ disorder group and significant associations between the eminence inclination and both the condyle and fossa shapes in the control group. The articular eminence inclination was steeper in the control group than in the TMJ disorder group.
Conclusions
The eminence inclination was steeper in the control patients than in the patients with TMJ disorders, and was not correlated with the condylar bone changes or condylar movements.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The articular eminence is a part of the temporal bone on which the mandibular condyle slides during mandibular movements. The inclination of the articular eminence varies among individuals, and dictates the path of the condylar movements as well as the degree of rotation of the disk over the condyle [1]. As the steepness of the articular eminence increases, the movements of the disc and the condylar process also increase. The associations between temporomandibular joint (TMJ) disorders and the inclination of the articular eminence have been investigated by various authors. While some authors found a correlation between the inclination of the eminence and internal derangements [2, 3], others found no association [4].
Several changes may occur in the subarticular surfaces of the condyle and fossa during TMJ disorders. Erosions appear as pitted and irregular contours of the bony surfaces. In some instances, the bony surfaces become flattened, a condition called an osteophyte is created, and small bone projections may form. In other instances, there may be a relationship between the condylar bone changes and the eminence inclination. It has been noted that the eminences in joints with osteoarthritic changes were flatter than those in joints with normal bone structures [3].
Many methods have been used to examine the inclination of the articular eminence, such as measurements on dry skulls [5–7], conventional radiography [8], conventional tomography [1, 9], magnetic resonance imaging (MRI) [10–13] and computed tomography (CT) [3, 4, 14]. Cone-beam CT (CBCT) has recently been developed as an alternative to conventional CT for dental and maxillofacial osseous diagnostic tasks. CBCT, which was used in the present study, allows for a shorter scanning time and a lower radiation dose than conventional CT [15].
The purpose of the present study was to determine the inclination and height of the articular eminence with respect to the condylar bone changes, condyle shape, fossa shape and movements of the condylar process in patients with and without TMJ dysfunction by CBCT.
Materials and methods
Patients
The measurements were performed retrospectively on the CBCT records of 104 joints in 52 patients with TMJ dysfunction and 82 joints in 41 patients without TMJ dysfunction symptoms who were previously referred to our clinic. All of the patients in the first group had clinical signs and symptoms of TMJ dysfunction, such as TMJ noise, pain, hypomobility or hypermobility. The exclusion criteria were the presence of congenital craniofacial abnormalities and any systemic conditions that may affect the TMJ, such as rheumatoid arthritis. We did not perform new CBCT scans for the symptom-free control group. We chose our control group from patients for whom CBCT examinations were performed for reasons other than TMJ dysfunction.
Imaging procedures
The CBCT images were taken with a NewTom 3G (Quantitative Radiology, Verona, Italy) flat panel-based CBCT device. The scanner operated with a maximum output of 110 kV, 15 mAs, 0.16-mm voxel size and typical exposure time of 5.4 s. The patient was placed in a horizontal position, so that the Frankfort horizontal plane was perpendicular to the table, with their head within the circular gantry housing the X-ray tube to obtain consistent orientation of the sagittal images. The X-ray tube-detector system performed a 360° rotation around the head of the patient, and the scanning time was 36 s. A second scan of the patients with TMJ dysfunction was performed with each patient’s mouth open for detection of the range and type of the condylar movements. After the completion of the second scan, the patient left the examination room, and the clinician performed the primary reconstruction. The QR-NNT version 2.21 (Quantitative Radiology, Verona, Italy) software program was used for analyses.
The area of interest was defined on axial slices of 0.5-mm thickness. The axial view from which the condyles were seen with their widest mediolateral extent was used as the reference view for the secondary reconstruction. The lateral slices of the TMJ were reconstructed perpendicular to the long axis of the condyle with a thickness of 1 mm, and the coronal slices were reconstructed parallel to the long axis of the condyle with a thickness of 1 mm on the selected axial image. The same procedure described above was performed for the open-mouth position.
Measurements
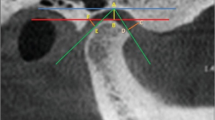
The measurements of the articular eminence were taken on the central sagittal slices of the TMJ described above. The points used for measurements in this study were as follows (Fig. 1):

Examples of the measurements, and the lines and angles used in the study. Bf eminence inclination best-fit line, Tr eminence inclination top-roof line, Eh eminence height
- Cu:
-
Highest point of the condylar process
- R:
-
Highest point of the fossa
- T:
-
Lowest point of the articular eminence
- Ce:
-
Point at which the F′ line cuts the posterior surface of the eminence
- Po:
-
Porion (highest point of the auditory meatus)
Using these points, the following planes were established:
- Ebf:
-
Best-fitting plane of the articular eminence inclination connecting the Ce
- Etr:
-
Plane passing through the points Cu and R
- F:
-
Frankfort horizontal
- F′:
-
Line parallel to F passing through the point Cu
- F′′:
-
Line parallel to F passing through the point R
Using these planes, the eminence inclination was measured in two ways. The first was the best-fit line method, which involved the angle between the Ebf and Frankfort horizontal planes, and the second was the top-roof line method, which used the angle between the Etr and Frankfort horizontal planes (Fig. 1) [9, 16]. The eminence height was established by measurement of the perpendicular distance between the lowest point of the articular eminence and the highest point of the fossa (Fig. 1).
The condylar bone changes were categorized according to previously reported definitions [3] as normal, erosion and osteophyte formation in a frontal view (Fig. 2). The basic shapes used for classification were round, oval, flattened and triangular for the condyles in a frontal view (Fig. 3) [17], and triangular, trapezoidal, oval and round for the fossa in a lateral view (Fig. 4) [16]. We used the central coronal slice to determine the condyle shape and the central sagittal slice to determine the fossa shape. The same procedure was used for all patients. Furthermore, the types of movements of the condyles were determined in the TMJ disorder group on the open-mouth images, and mandibular hypermobility or hypomobility was noted for each joint.

Condylar bone changes in a coronal view: normal (a), osteophyte (b), erosion (c)

Condyle shapes in a coronal view: triangular (a), oval (b), flattened (c), round (d)

Fossa shapes in a sagittal view: triangular (a), oval (b), trapezoidal (c), round (d)
Statistical analysis
Statistical analyses were conducted with SPSS software (SPSS 20.0 for Windows; SPSS Inc., Chicago, IL, USA). One-way ANOVA was used to determine differences in the eminence inclination and eminence height values according to the condylar bone changes, condylar movements, condyle shape and fossa shape. Further analyses were conducted with the least significant difference (LSD) test to highlight the significant differences between the groups. The Kruskal–Wallis test was used to determine the correlations of the condylar movements with the condyle and fossa shapes. The Chi square test was used to determine the differences among the condyle and fossa shapes in the TMJ disorder group and the control group. Finally, Student’s t-test was used to determine the differences in the eminence height and inclination between the TMJ disorder and control groups. Values of P < 0.05 were considered to indicate statistical significance.
Three observers chosen by the study organizer performed the measurements and categorizations. These three observers were oral and maxillofacial radiologists with experience of CBCT images for 5 years, and performed the measurements and categorizations after providing calibration for each other. The observers established the parametric measurements while being unaware of whether the patients belonged to the TMJ disorder group or the control group. The three observers established all of the parametric measurements, and the mean values were used to determine the reliability of the study. For the non-parametric categorizations, any conflicts in the decisions were resolved by consensus.
Results
The distributions of the condylar bone changes, condylar movements, and condyle and fossa shapes in the TMJ disorder group are shown in Table 1. Condylar bone changes were seen in 13 of the 104 joints, comprising 6 condyles with erosion and 7 condyles with osteophyte formation. The eminence inclination values were higher in the joints without condylar bone changes than in the joints with condylar bone changes, but the differences were not significant. In addition, there were no significant differences in the eminence inclination and height with respect to the condylar movements and condyle shape in the TMJ disorder group. The eminence inclination and height values were only associated with the fossa shape (Table 1).
The associations between the condylar movements and the condyle and fossa shapes were investigated, but no significant associations were found (P > 0.05; χ2 = 2.789 for condyle shape; χ2 = 2.011 for fossa shape).
The distributions of the condylar bone changes and condyle and fossa shapes in the control group are shown in Table 2. In the control group, the eminence inclination and height values were associated with both the condyle and fossa shapes. There was only one case with condylar bone changes in the control group. Thus, statistical tests could not be performed to determine the relationship between the condylar bone changes and the eminence inclination in the control group. In addition, condylar movements could not be considered in the control group because of the absence of open-mouth scans.
The distributions of the condyle and fossa shapes are shown in Table 3. Significant differences were observed between the TMJ disorder and control groups. Although round-shaped condyles were observed most frequently in the TMJ disorder group, oval-shaped condyles were observed most frequently in the control group. Triangular-shaped condyles were observed less frequently in both the control and TMJ disorder groups. Regarding the fossa shapes, a round fossa was found most frequently, and a triangular fossa was found least frequently, in both the TMJ disorder and control groups.
There was a significant difference in the eminence inclination values between the TMJ disorder group and the control group (P < 0.05). The eminence inclination values for both the best-fit and top-roof line methods were lower in the TMJ disorder group than in the control group (Table 4).
Discussion
The articular eminence is a small bone situated in front of the glenoid fossa, and its posterior surface slope varies among the general population. Although the articular eminence is an anatomic structure belonging to the cranium, it is exposed to functional loads arising from chewing forces, and these loads influence its morphological shape [18].
Various methods have been used in previous studies to measure the inclination of the posterior slope of the articular eminence. It is very important to choose an appropriate method for true measurement of the eminence inclination. The TMJ is difficult to view with conventional techniques because of superimposition of the adjacent dense temporal bone. It has been shown that CBCT offers a low-dose and cost-effective alternative to conventional CT for diagnostic evaluation of osseous abnormalities of the TMJ [15, 19–21]. Hashimoto et al. [22] demonstrated that CBCT imaging performance was better than four-row multidetector medial CT. It is also expected that CBCT manufacturers will improve their reconstruction algorithms and post-processing imaging, thereby providing higher resolution to the images, while keeping the radiation exposure to the patient as low as possible. While the NewTom 3G scans patients over a 36-s period, the actual exposure takes place for only 5.4 s. The effective dose detriment of the currently available large field-of-view CBCT units is several to many times higher than that of conventional panoramic imaging, but several to many times lower than the reported doses for conventional CT [20].
CBCT also allows measurements of angles and distances with real dimensions and without superimposition or distortion. In particular, panoramic imaging and conventional tomography can yield disappointing results. Consequently, it has been noted that no slices can be made in studies performed with only a single slice or with transcranial or panoramic radiographic examinations, and therefore the results may not depict a true measurement of the eminence inclination [13]. The view of the eminence in the central slice reflects the steepest part of the eminence, and gives the best representation of the eminence inclination [23]. For this reason, we chose the central sagittal slice of the condyle for measurements.
Few studies in the literature have examined the association between condylar bone changes and the eminence inclination [3]. Recent studies in the literature have generally used MRI to determine the eminence inclination with respect to the position of the disc [10, 12, 13, 24]. Some of these studies used MRI together with tomography [24, 25], and some researchers used only CT [4] to compensate for the disadvantages of using MRI to diagnose bone structures. The present study also had limitations, since it could not examine the relationships between the soft tissues of the TMJ, such as discs and ligaments, and the eminence anatomy. However, CBCT was shown to be an appropriate tool for determining the condylar bone changes, eminence inclination and morphologies of the fossa and condylar processes.
In the present study, we observed condylar bone changes in only 13 of 104 joints in the TMJ disorder group, and did not find a significant association between condylar bone changes and the eminence inclination. Although the eminence inclination was slightly higher in the joints without condylar bone changes than in the joints with condylar bone changes, the differences were not significant. Yamada et al. [3] mentioned that the slope of the articular eminence decreased with an increase in the severity of condylar bone changes. In addition to condylar bone changes, flattening of the articular eminence may also be involved as a reaction to loading on the TMJ. Similarly, Ren et al. [26], Estomaguio et al. [4] and Kurita et al. [12] found differences in the eminence inclination between patients with and without condylar bone changes. Ren et al. [26], who used precise image diagnosis techniques to establish their control group, also reported that osseous condylar changes were more related to the inclination of the eminence than to the presence of disc displacement. However, Jasinevicius et al. [7] found that only degeneration of the eminence was associated with the eminence inclination in a study on dry skulls. Similar to the present study, they found no association between condylar bone changes and the eminence inclination.
In the control group, we observed only one joint with condylar osteophyte formation. Essentially, we do not expect to see condylar bone changes in patients without TMJ dysfunction, as such changes are the long-term consequences of TMJ disorders. However, degenerative changes of the TMJ detected on radiologic examination can sometimes be incidental, and may not be responsible for facial pain symptoms or TMJ dysfunction.
In the present study, the condyle and fossa shapes were assessed morphologically from the coronal and sagittal slices in CBCT records, a method that is both simple and sophisticated. The articular eminence inclination was associated with the fossa shape in the TMJ disorder group and with both the condyle and fossa shapes in the control group. In a previous morphometric study, Katsavrias and Halazonetis [27] stated that, although the variability of the fossa shape was related to the eminence inclination, the variability of the condyle shape was mainly related to the condylar inclination.
A positive correlation was detected between a steeper eminence and the depth of the mandibular fossa in a previous clinical study by Quirch et al. [28]. Sülün et al. [13] found a significant correlation between the posterior slope of the articular eminence and the fossa depth. They also mentioned that both a steeper slope of the articular eminence and the depth of the fossa might have some relationship to internal derangements of the TMJ.
There were significant differences between the condyle and fossa shapes in our TMJ disorder and control groups. The prevalent condyle shapes were round in the TMJ disorder group and oval in the control group. However, it has been described that such morphological variations are a prerequisite for functional integrity [16]. Thus, the morphological features may be affected by the functions.
In the present study, we did not find a significant relationship between the condylar movements and the eminence inclination. Gökalp et al. [10] found a relationship between the condylar movements and the eminence inclination in patients with disc displacement without reduction. However, they found no relationship between the eminence inclination and the condylar movements in patients with disc displacement with reduction. We also did not find any association between the condylar movements and the shapes of the condyle and fossa. It should be mentioned that the movements of the condyle depend not only on the eminence inclination but also on other etiologic factors of mandibular hypomobility, such as ankylosis (fibrous or osseous), muscle contraction (myostatic or myofibrotic), capsular fibrosis or coronoid impedance.
It has been reported that a steep slope of the articular eminence predisposes patients to certain internal derangement disorders [10, 11, 13]. However, in the present study, we found that the eminence inclination was greater in patients without TMJ dysfunction than in patients with TMJ dysfunction. Similarly, Ren et al. [26] found that the eminence inclination was steeper in symptom-free volunteers than in patients with internal derangement. It has also been noted that flattening of the articular eminence was observed in patients with internal derangement [12].
Overall, the conclusions of the present study are as follows:
-
1.
The eminence inclination was not related to condylar bone changes or condylar movements.
-
2.
The condylar movement was not related to the eminence inclination or the condyle and fossa shapes.
-
3.
The eminence inclination was steeper in control patients than in patients with TMJ dysfunction, and may flatten over time in patients with TMJ disorders.
Additional studies are required to further understand the complex nature of the TMJ and its disorders.
References
Pandis N, Karpac J, Trevino R, Williams B. A radiographic study of condyle position at various depths of cut in dry skulls with axially corrected lateral tomograms. Am J Orthod Dentofacial Orthop. 1991;100:116–22.
Sato S, Kawamura H, Motegi K, Takahashi K. Morphology of the mandibular fossa and the articular eminence in temporomandibular joints with anterior disk displacement. Int J Oral Maxillofac Surg. 1996;25:236–68.
Yamada K, Tsuruta A, Hanada K, Hayashi T. Morphology of the articular eminence in temporomandibular joints and condylar bone change. J Oral Rehabil. 2004;31:438–44.
Estomaguio GA, Yamada K, Ochi K, Hayashi T, Hanada K. Craniofacial morphology and inclination of the posterior slope of the articular eminence in female patients with and without condylar bone change. Cranio. 2005;23:257–63.
Jasinevicius TR, Pyle MA, Lalumandier JA, Nelson S, Kohrs KJ, Sawyer DR. The angle of the articular eminence in modern dentate African-Americans and European-Americans. Cranio. 2005;23:249–56.
Jasinevicius TR, Pyle MA, Lalumandier JA, et al. Asymmetry of the articular eminence in dentate and partially edentulous populations. Cranio. 2006;24:85–94.
Jasinevicius TR, Pyle MA, Nelson S, Lalumandier JA, Kohrs KJ, Sawyer DR. Relationship of degenerative changes of the temporomandibular joint (TMJ) with the angle of eminentia. J Oral Rehabil. 2006;33:638–45.
Baccetti T, Antonini A, Franchi L, Tonti M, Tollaro I. Glenoid fossa position in different facial types: a cephalometric study. Br J Orthod. 1997;24:55–9.
Katsavrias EG. The effect of mandibular protrusive (activator) appliances on articular eminence morphology. Angle Orthod. 2003;73:647–53.
Gökalp H, Türkkahraman H, Bzeizi N. Correlation between eminence steepness and condyle disc movements in temporomandibular joints with internal derangements on magnetic resonance imaging. Eur J Orthod. 2001;23:579–84.
Kurita H, Ohtsuka A, Kobayashi H, Kurashina K. Is the morphology of the articular eminence of the temporomandibular joint a predisposing factor for disc displacement? Dentomaxillofac Radiol. 2000;29:159–62.
Kurita H, Ohtsuka A, Kobayashi H, Kurashina K. Flattening of the articular eminence correlates with progressive internal derangement of the temporomandibular joint. Dentomaxillofac Radiol. 2000;29:277–9.
Sülün T, Cemgil T, Duc JM, Rammelsberg P, Jäger L, Gernet W. Morphology of the mandibular fossa and inclination of the articular eminence in patients with internal derangement and in symptom-free volunteers. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001;92:98–107.
Kikuchi K, Takeuchi S, Tanaka E, Shibaguchi T, Tanne K. Association between condylar position, joint morphology and craniofacial morphology in orthodontic patients without temporomandibular joint disorders. J Oral Rehabil. 2003;30:1070–5.
Hintze H, Wiese M, Wenzel A. Cone beam CT and conventional tomography for the detection of morphological temporomandibular joint changes. Dentomaxillofac Radiol. 2007;36:192–7.
Katsavrias EG. Morphology of the temporomandibular joint in subjects with Class II Division 2 malocclusions. Am J Orthod Dentofacial Orthop. 2006;129:470–8.
Bumann A, Lotzmann U. TMJ disorders and orofacial pain: the role of dentistry in a multidisciplinary diagnostic approach. Stuttgart: Georg Thieme Verlag; 2002. p. 19.
O’Ryan F, Epker BN. Temporomandibular joint function and morphology: observations on the spectra of normalcy. Oral Surg Oral Med Oral Pathol. 1984;58:272–9.
Baba R, Ueda K, Okabe M. Using a flat-panel detector in high resolution cone beam CT for dental imaging. Dentomaxillofac Radiol. 2004;33:285–90.
Ludlow JB, Davies-Ludlow LE, Brooks SL, Howerton WB. Dosimetry of 3 CBCT devices for oral and maxillofacial radiology: CB Mercuray, NewTom 3G and i-CAT. Dentomaxillofac Radiol. 2006;35:219–26.
White SC. Cone-beam imaging in dentistry. Health Phys. 2008;95:628–37.
Hashimoto K, Kawashima S, Araki M, Iwai K, Sawada K, Akiyama Y. Comparison of image performance between cone-beam computed tomography for dental use and four-row multi-detector helical CT. J Oral Sci. 2006;48:27–34.
Ichikawa J, Hara T, Tamatsu Y, Ide Y. Morphological changes in the internal structure of the articular eminence of the temporal bone during growth from deciduous to early mixed dentition. J Biomech. 2007;40:3541–7.
Galante G, Paesani D, Tallents RH, Hatala MA, Katzberg RW, Murphy W. Angle of the articular eminence in patients with temporomandibular joint dysfunction and asymptomatic volunteers. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995;80:242–9.
Major PW, Kinniburgh RD, Nebbe B, Prasad NG, Glover KE. Tomographic assessment of temporomandibular joint osseous articular surface contour and spatial relationships associated with disc displacement and disc length. Am J Orthod Dentofacial Orthop. 2002;121:152–61.
Ren YF, Isberg A, Westesson PL. Steepness of the articular eminence in the temporomandibular joint. Tomographic comparison between asymptomatic volunteers with normal disk position and patients with disk displacement. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995;80:258–66.
Katsavrias EG, Halazonetis DJ. Condyle and fossa shape in Class II and Class III skeletal patterns: a morphometric tomographic study. Am J Orthod Dentofacial Orthop. 2005;128:337–46.
Quirch JS, Carraro JJ, Itoiz ME. Correlation between articular eminentia and the depth of glenoid fossa. J Periodontal Res. 1966;1:227–32.
Conflict of interest
There are no financial or other relations that could lead to a conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Çağlayan, F., Sümbüllü, M.A. & Akgül, H.M. Associations between the articular eminence inclination and condylar bone changes, condylar movements, and condyle and fossa shapes. Oral Radiol 30, 84–91 (2014). https://doi.org/10.1007/s11282-013-0149-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11282-013-0149-x