
Abstract
Objective
This study aims to evaluate differences in the morphological and morphometric features of hard tissue components of the temporomandibular joint (TMJ) in the cone beam computed tomography (CBCT) images of children with different skeletal models in the sagittal and vertical plane.
Methods
Condyle dimensions, horizontal condylar angle, the distance of the condyle center to the midsagittal plane, condyle position, eminence height, eminence inclination, condyle, and fossa shape and symmetry were evaluated in CBCT images in 190 TMJs in 95 pediatric patients. Patients were classified as Class 1–2–3 in the sagittal direction, as hypodivergent, normodivergent, and hyperdivergent in the vertical direction. Children were divided into 10–13 and 14–17 age groups.
Results
The left superior joint space in children with a different skeletal model in the sagittal plane was lower and found to be statistically significant in Class 3 children (p < 0.05). A statistically significant difference was found lower in the left articular eminence inclination and height in Class 3 children (p < 0.05). The most common oval fossa form was seen in Classes 2–3 children (p < 0.05). It was determined that the anterior joint space was lower in hyperdivergent children and the condyle was located more anteriorly. The mediolateral length of the condyle and the height of the articular eminence were positively correlated with age.
Conclusions
The results revealed that the difference in skeletal models seen in sagittal and vertical planes in children may cause morphological and morphometric changes in the hard tissue components of TMJ.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The craniofacial system is the integrity of different skeletal structures that function in harmony with each other. The structures in this system reach their ideal dimensions and positions in mutual interaction throughout the growth and development period [1, 2]. During the growth and development process, craniofacial structures change to create a balanced facial structure with the effect of genetic and environmental factors. These structures are in interaction and the growth difference in any of the structures affects other regions as well [1]. Articular structures also show an adaptation potential and reshape according to changing functional needs [3]. The temporomandibular joint (TMJ) is a ginglymoarthrodial joint located between the condylar process of the mandible and the mandibular fossa and articular eminence of the temporal bone. The morphological and morphometrical characteristics of the TMJ can be affected by various anatomical factors, such as growth patterns and pathological factors, like dental and skeletal malocclusion. Skeletal malocclusions may occur between the lower and upper jaws with deviations from the normal growth pattern [1, 2]. Since TMJ is exposed to different forces in individuals with different craniofacial morphologies, it is thought that the structural properties of the joint will also differ [4,5,6].
The radiological evaluation of TMJ is important to determine the normal variables and pathological conditions that need treatment in asymptomatic individuals and also guides in taking preventive measures, morphological and morphometric differences in TMJ structures with increasing age. In two-dimensional radiography techniques, the structure of the TMJ cannot be fully visualized due to the difficulty of positioning the X-rays correctly, the inability to obtain images in different sections and superimpositions [7, 8]. Today, the anatomical structures and morphology of the TMJ are evaluated with CBCT-provided three-dimensional cross-sectional imaging of the maxillofacial region without superposition from the surrounding tissues with lower radiation dose [8,9,10].
Some studies reported a relationship between TMJ morphology with different occlusion and face types, but some studies reported no relationship contrary to these results. Although there are studies in the literature evaluating the morphology and morphometric measurements of the TMJ in adults with different facial types and sagittal direction models, there are not enough studies in children [11,12,13,14]. Also, there are few studies evaluating the differences in TMJ morphology based on the interactive effects of both sagittal and vertical cephalometric relationships. In studies conducted in the literature, morphological and morphometric changes in temporomandibular joint structures were evaluated in different age groups, but there is no study in which all skeletal and occlusal differences were evaluated simultaneously in the same study. Therefore, this study aimed to evaluate the following null hypothesis: there are differences in the morphological and morphometric properties of the hard tissue components of the TMJ due to the exposure of the TMJ to different forces resulting from malocclusion in children with different sagittal and vertical craniofacial structures.
Materials and methods
Sample selection
The study was approved by the Clinical Research Ethics Committee of the University Hospital (Ethics committee approval number: 72867572-050.01.04-737). A hundred and ninety TMJs of 95 adolescents (45 boys and 50 girls) who had taken cone beam computed tomography with dental reasons (e.g., impacted teeth, cyst and tumor etc.), age range 10–17 years were evaluated in the present study. The exclusion criteria were the presence of congenital deformities or syndromes, such as Crouzon syndrome, Pierre Robin syndrome, cleft lip and palate, maxillofacial bone fractures or surgeries in the TMJ area, and TMJ hypoplasia, hyperplasia or tumors, a history of trauma, previous orthodontic treatment, and any systemic diseases, which may affect joint morphology such as rheumatoid arthritis.
Imaging procedures
The cone beam images were performed using Planmeca ProMax 3D Mid (Planmeca Oy, Helsinki, Finland) flat panel-based CBCT machine. The maximum output of the scanner was 90 kV, 10 mA, 27 s and with 0.4 mm3 voxel size. The exposure field was 200 mm in diameter and 170 mm in height. The patient was placed in a horizontal position so that the Frankfort horizontal plane was perpendicular to the table, with their head within the circular gantry housing of the X-ray tube to obtain a consistent orientation of sagittal images. The X-ray tube detector system performed a 360° rotation around the head of the patient, and the scanning time was 27 s. The Planmeca Romexis Viewer® (Romexis 3.2.0, Helsinki, Finland) software program was used for analyses. In this program, lateral cephalometric radiography (LSR) images were obtained from the CBCT images of the patients with the feature of creating LSR.
Cephalometric analyses were performed on LSR images of patients. The subjects were divided into three groups according to the ANB angle to determine the sagittal jaw relationship: Class 1 (0° < ANB < 4°), Class 2 (ANB > 4°), and Class 3 (ANB < 0°) [15]. Each group formed was divided into three groups according to the Jarabak ratio to determine the vertical facial pattern: hypodivergent (Jarabak ratio > 63%), normodivergent (Jarabak ratio = 59–63%), and hyperdivergent (Jarabak ratio < 59%) groups [16].
Measurements on CBCT images were assessed by one dentomaxillofacial radiologist (four years of experience).
Measurements
Condylar dimensions
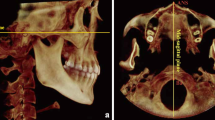
In the measurement of mandibular condyle dimensions, the section in which the side to be examined was seen the widest was determined on the axial images. The length of the condyle head in the mediolateral and anteroposterior directions was measured in this section (Fig. 1).

a The length of the condyle head in the mediolateral and anteroposterior directions. b The measurement of the horizontal condylar angle. c The vertical distance of the geometric center of the condyle to the midsagittal plane
Horizontal condylar angle and distance of condyle centers to midsagittal plane
The horizontal condylar angle, defined as the angle between the long axis of the condyle (mediolateral) and the coronal plane in the axial view, was measured (Fig. 1). The vertical distance of the geometric center of the condyle to the midsagittal plane was recorded in the same section (Fig. 1).
Evaluation of the position of the condyle in the mandibular fossa
The position of the mandibular condyle was evaluated by measuring the superior, anterior, and posterior joint spaces on the sagittal section corresponding to the condyle center in the axial section where the condyle is seen at its widest.
Superior joint space length It is the shortest distance between the highest point of the condyle and the highest point of the mandibular fossa.
Anterior joint space length It is the shortest distance between the most anterior point of the condyle and the posterior wall of the articular tubercle.
Posterior joint space length It is measured as the shortest distance between the most posterior point of the condyle and the posterior wall of the mandibular fossa.
Measurement articular eminence inclination and height
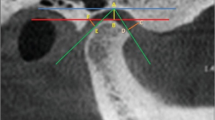
Measurement inclination of articular eminence Two different methods were used to measure the sagittal section, which corresponds to the center of the condyle, in the axial section where the condyle is seen the widest.
-
Top-roof line method Angle between Frankfurt horizontal plane and Etr plane (Fig. 2).
-
Best-fit line method Angle between Frankfurt horizontal plane and Ebf plane (Fig. 2).

a Measurement with top-roof line method of articular eminence inclination. b Measurement with best-fit line method of articular eminence inclination. c Measurement of articular eminence height
Measurement Height of Articular Eminence It is the vertical distance between the lowest point of the articular eminence and the deepest point of the mandibular fossa (Fig. 2).
Evaluation of mandibular condyle and glenoid fossa shapes
The shapes of the mandibular condyle and glenoid fossa were evaluated in the axial section where the condyle is seen at its widest size, in the coronal section that cuts the long axis of the condyle perpendicularly and passes through the center of the condyle and in the sagittal section that passes through the center of the condyle.
Condyle shapes were examined in the central coronal section by dividing them into 4 groups round (a), oval (b), flat (c), and angled (d) (Fig. 3).

a Round, b oval, c flat and d angled condyle shapes in the central coronal section
Mandibular fossa shapes were evaluated in the central sagittal section by dividing them into 4 groups oval (a), triangular (b), angular (c) and trapezoidal (d) (Fig. 4).

Mandibular fossa shapes in the central sagittal section; a oval, b triangular, c angular and d trapezoidal
Statistical analysis
The sample size was calculated using G*power (version 3.1.9.2) software based on the preliminary information obtained from the literature (power of 80%, α = 0.05 and effect size of 0.79). The minimum sample size for each group was found to be 7. The data were evaluated using the statistical package program (SPSS, Version 17.0).
The normal distribution of data was examined with the Kolmogorov–Smirnov test, and Levene’s test was used to test for homogeneity of variances. Categorical variables were given as numbers and percentages, and continuous (quantitative and quantitative) variables were given as mean and standard deviation. One-factor analysis of variance and LSD (Least Significant Difference) which are multiple comparison tests were used to compare the difference of means. Pearson correlation analysis was used to determine the significance and direction of linear relationships between variables.
The intra-observer agreement for the categorical variables was assessed using k statistics and interpreted as follows: A k-value greater than 0.81–1.00 corresponded to an excellent agreement, a k-value of 0.61 to 0.80 corresponded to a very good intra-observer agreement, a k-value of 0.41 to 0.60 corresponded to a good intra-observer agreement and a k-value of 0.21 to 0.40 corresponded to a moderate inter-observer agreement. Intra-observer agreement for numerical variables was evaluated with Cronbach's alpha coefficient test. These values are α ≥ 0.9 excellent, 0.7 ≤ α < 0.9 good, 0.6 ≤ α < 0.7 acceptable, 0.5 ≤ α < 0.6 poor, α < 0.5 unacceptable evaluated [17].
Results
In this study, 95 pediatric patients with a mean age of 13.63 ± 2.18 years (45 boys—mean age 13.38 ± 2.13, 50 girls—mean age 13.86 ± 2.23) were included. The sagittal direction jaw relations according to the ANB angle values and the vertical direction jaw relations according to the Jarabak ratio in the lateral cephalometric radiograph images of the study group were shown in Table 1.
The ML length of the condyle on both the right and left sides was longer in boys than in girls. A statistically significant difference was found between the genders in the ML length measurements of the right (p = 0.008) and left (p = 0.000) condyles. There was no statistically significant difference between the genders in the mean AP length of the right and left condyles (p > 0.05).
The mean of ML and AP measurements of the right and left condyles in children with different models of jaw relationship in both sagittal and vertical directions had approximately the same values in all three classes. There was no statistically significant difference between the ML and AP length values measured in the groups (p > 0.05) (Table 2).
In the study group, the mean value of the right horizontal condylar angle was 19.8 ± 2.66° (min. 14.34° and max. 26.1°), while the mean value of the left horizontal condylar angle was 20.07 ± 2.7° (min. 14.07° and max. 26.59°). There was no statistically significant difference between the genders in the mean values of the right and left horizontal condylar angle and the distance of the right–left condyle center to the midsagittal plane (p > 0.05).
No statistically significant difference was found between the right and left horizontal condylar angle measurement values in the groups of children with different models of sagittal and vertical jaw relationship (p > 0.05).
The distance measurement values of the condyle center to the midsagittal plane on the right (p = 0.01) and left sides (p = 0.04) were higher in individuals with hypodivergent face type than in other groups. There was no statistically significant difference between the groups in the distance measurement values of the condyle center to the midsagittal plane in children with a different model of the jaw relationship in the sagittal direction (p > 0.05) (Table 3).
Right and left upper, posterior and anterior joint space length measurements were higher in boys than girls. A statistically significant difference was found between the genders in the mean values of the right (p = 0.01) and left (p = 0.00) upper and left anterior (p = 0.00) joint space lengths.
In children with a different jaw relationship in the sagittal direction, the left upper joint space length was longer in Class 1 patients than in other class patients (p = 0.02). Right upper joint space length, right and left anterior joint space length, right and left posterior joint space length measurements had approximately the same values in all three classes (p > 0.05).
The mean values of right (p = 0.03) and left (p = 0.02) anterior joint space length in children with vertically different models of jaw relation were found to be statistically significant between the groups. In hyperdivergent patients, it was determined that the anterior joint space length was less and the condyle was located more anteriorly (Table 4).
Both right and left articular eminence inclination and eminence height were measured more in boys than in girls. While the measurement of the right articular eminence inclination with the top-roof line method was not statistically significant between the genders (p > 0.05), a statistically significant difference was found in the mean measurement of the left articular eminence inclination using the top-roof line method (p = 0.01).
There was no statistically significant difference between the values of the right articular eminence inclination measured by the best-fit line method in children with a different model of the jaw relationship in the sagittal direction. There was no statistically significant difference between the measurements made with the top-roof line method on both the right and left sides (p > 0.05).
In children with different models of jaw relation in both sagittal (p = 0.03) and vertical (p = 0.01) directions, eminence inclination values measured by the best-fit line method on the left side were statistically significantly different between the groups (Table 5).
The most common mandibular condyle was observed on the right (44.2%) and left (41.1%) sides in the study group. While the most common form of the round condyle was observed in the right condyle in Class 1 and Class 2 patients in children with a different jaw relationship in the sagittal direction, the oval condyle form was most common in Class 3 patients (p = 0.09). On the left condyle, oval condyle form was most common in Class 1 patients, while round condyle form was most common in Class 2 and Class 3 children (p = 0.3). Condyle shape symmetry was most common in Class 1 children (46.9%), while condyle shape symmetry was least observed in Class 2 children (41.2%) (p = 0.89).
The right condyle shape was most frequently observed in the round form in all groups of children with jaw relationships with a different pattern in the vertical direction (p = 0.58). The left condyle shape was observed most frequently as an oval and round form in hyperdivergent children, while the round form was determined most frequently in normodivergent and hypodivergent children (p = 0.39). Condyle shape symmetry was most common in hypodivergent children (44.4%) (p = 0.99).
Oval and trapezoidal fossa forms were observed most frequently in Class 1 patients in the right fossa in children with a different jaw relationship in the sagittal direction. Oval fossa form was most common in Class 2 and Class 3 children and it was found to be statistically significant (p = 0.02). In the left fossa, the most common oval fossa form was observed in Class 1, Class 2, Class 3 children and was found to be statistically significant (p = 0.004). Fossa shape symmetry was most common in Class 3 children (69%), while condyle shape symmetry was least observed in Class 1 children (46.9%) (p = 0.44).
In this study, Cronbach's alpha coefficient values in the intraobserver agreement assessment of morphometric measurements of the TMJ ranged from 0.57 (poor) to 0.99 (excellent). In the evaluation of their morphological characteristics, the intraobserver agreement kappa test coefficient values were between 0.54 and 1. In other words, values ranging from moderate agreement to very good agreement were observed.
Discussion
In this study, the morphological and morphometric features of the hard tissue components of the TMJ were evaluated on CBCT images in children with sagittal and vertically different craniofacial features. The TMJ is one of the most important and most complex joints in the human body, in which the right and left joints vary morphologically and morphometrically from person to person and in the same person [18]. Determining whether the TMJ and surrounding bone structures differ in individuals with different craniofacial features at an early age is important for the prevention and early diagnosis of TMJ-related pathologies.
Although there are studies in the literature evaluating TMJ morphology and morphometric measurements in adults with different facial types or sagittal direction models, this study was planned because there are not enough studies on this subject in pediatric patients [11,12,13,14]. However, in these studies, one or more of the morphological or morphometric measurements were evaluated in TMJ structures. In our study, many parameters were examined simultaneously in the TMJs of children aged 10–17 years with different sagittal and vertical craniofacial features. Both morphological (mandibular condyle and glenoid fossa shapes) and morphometric (length of the condyle head, horizontal condylar angle, distance of condyle centers to midsagittal plane, superior-anterior–posterior joint space length, articular eminence inclination, and height) features of temporomandibular joint structures were evaluated.
Zhang et al. examined the accuracy of CBCT in the assessment of TMJ dimensions and reported that the measurements of the joint spaces were very similar to the actual joint spaces [19]. In this study, images of patients who underwent CBCT, which is an imaging method that is effective in showing the bone structures of the joint and provides a three-dimensional examination in different planes, were used to examine the morphological and morphometric features of TMJ [9].
By obtaining 2-dimensional cephalograms from three-dimensional CBCT images, it is possible to simulate lateral and posteroanterior cephalometric radiographs and compare these films with existing films [20]. In this study, 2D lateral cephalometric radiograph images obtained from CBCT images were used to determine the sagittal and vertical jaw relationships of the patients. Kumar et al. reported that in the presence of CBCT images, more accurate evaluations can be made compared to conventional radiographs, since lateral cephalometric radiograph images obtained from CBCT prevent the patient from receiving additional radiation, and cephalometric points are marked more accurately by reducing the cost of shooting [21].
Biting force and chewing muscle activity were found to be high in hypodivergent individuals and low in hyperdivergent individuals [22, 23]. It has also been suggested that while normodivergent children develop more jaw strength as they grow, hyperdivergent children somehow stop gaining strength in their mandibular elevator muscles [24]. It has been found that bi-zygomatic width is higher in those who are fed a hard diet and have high chewing forces [25]. In our study, the distance values of the condyle centers of both sides to the midsagittal plane were found to be less in hyperdivergent patients in children with different face types. Since the development of bone components is related to muscle function, the reason why the bicondylar distance was found to be narrower in hyperdivergent patients in this study may be that these individuals have fewer chewing forces.
The relationship between craniofacial morphology and condyle position is controversial. While some researchers did not detect any relationship between condyle position and facial morphology, some researchers reported a significant relationship between condyle position and different skeletal models [26, 27]. In addition to studies reporting that the condyles are positioned significantly anteriorly in Class 3 patients, some studies found no significant difference in terms of condyle position in Class 1 and Class 2 groups [28, 29]. However, it has been reported that the posterior joint space length is shorter in adults than in children and the condyles are located more posteriorly [29]. In this study, no significant difference was found between the groups in the length measurements of the joint spaces on the right and left sides in children with different jaw relationships in the sagittal direction. Left upper joint space was found to be less in Class 3 children. However, no significant age-related difference was found in joint space length measurements and condyle position. The difference between the groups in terms of the left upper joint space may be because conditions such as parafunctional habits and unilateral chewing affect the chewing dynamics and therefore the TMJ in the children included in the study.
Burke et al. reported that the upper joint space increased in individuals with hypodivergent face type in children with Class 2 jaw relationship and there was no significant relationship between anterior and posterior joint space values and facial morphology [5]. Paknahad and Shahidi stated that in adults, the condyles are located more anteriorly in patients with hyperdivergent face type and they did not detect a significant difference in condyle position in normodivergent and hypodivergent patients [13]. In our study, it was found that the anterior joint space length was shorter and the condyle was located more anteriorly in hyperdivergent patients. This may be due to posterior rotation of the mandible as a result of increased anterior facial height in hyperdivergent patients.
Articular eminence is a small bone structure located in the anterior part of the mandibular fossa, exposed to functional forces together with other structures forming the TMJ and its posterior surface inclination differs between individuals [30]. The most commonly used methods for measuring the articular eminence inclination are the top-roof line and best-fit line methods, there is no definitively accepted method [27, 31]. While the best-fit line method shows the movement path of the condyle, the top-roof line method shows the articular eminence development and morphology better [31, 32]. In this study, both best-fit line and top-roof line methods were used in the measurement of articular eminence inclination, using the Frankfurt horizontal plane as the reference plane. In the literature, it has been reported that the eminence inclination is less in children and adults with Class 3 jaw relationship similar to our study [33, 34]. In our study, while the eminence inclination was found to be lower in both measurement methods in class 3 patients, a significant difference was found only in the measurement of the left eminence slope with the best-fit line method. Some studies about correlating the skeletal sagittal class and articular eminence inclination had found no significant difference between Classes 1, 2, and 3, but the Class 3 group had lower angles compared to Class I and Class II similar to our study [35,36,37].
It was reported that articular eminence development and inclination are affected more by function than skull base characteristics and genetics. Junli Ma et al. reported that the eminence in the chewing preferred side was steeper than that in the unpreferred side among the healthy subjects with chewing side preference [38]. Therefore unilateral chewing habit or parafunctional activities in children may have caused remodeling of the eminence structure.
Park et al. reported that there was no significant difference in the right and left articular eminence inclination between the groups in adult patients with vertically different craniofacial models, similar to our study [14]. Thus, it can be concluded that the articular eminence inclination is not affected by the vertical face morphology. In our study, while there was no difference between the groups in the mean of right articular eminence height, a significant difference was found between the groups in the mean of left articular eminence height. The difference between the results on the right and left, it may have been caused not by the different face types, but by the fact that the lack of teeth in the study group was frequently seen on the right side, unilateral chewing, and parafunctional habits.
Since the form of skeletal structures is closely related to function, TMJ morphology is affected by functional forces. It is thought that there will be a change in the shape of the condyle and fossa in individuals with different dentofacial morphologies since the mandible and TMJ are exposed to varying forces in different malocclusions [3]. Condyle shape classification is a controversial issue in studies conducted for many years and has been developed day by day [39,40,41,42]. In addition, there are few studies in the literature describing fossa shapes and suggesting a classification [39]. Merigue et al. found the most common convex condyle form in adolescent and adult patients with different skeletal models in the sagittal direction and reported that there was no significant difference between the groups [42]. In our study, different condyle shapes were determined on the right and left sides. In the right condyle, the round condyle form was most common in Class 1 and Class 2 patients, while the oval condyle form was most common in Class 3 patients. On the left side, the oval condyle form was most common in Class 1 patients, while the round condyle form was most common in Class 2 and Class 3 children. The reason for this may be that the TMJ region is exposed to different chewing forces due to the malocclusion present in the patients. In addition, the higher incidence of missing teeth in Class 1 patients in the study group may be the reason for the formation of different condyle forms.
Park et al. reported that round condyle shapes in hyperdivergent individuals and oval condyle shapes in hypodivergent individuals were the most common [14]. Burke et al. stated that they did not find a significant relationship between vertical facial morphology and condyle shape [5]. In our study, the right condyle shape was most frequently observed in the round form in all groups of children with a different jaw relationship in the vertical direction. The most common condyle shape in the left condyle was oval and round form in hyperdivergent children, the most common round form was determined in normodivergent and hypodivergent children.
Katsavrias reported the most common condyle and fossa form as oval in children and adults with Class 2 Division 2 sagittal jaw relation [43]. In this study, oval and trapezoidal fossa forms were observed most frequently in Class 1 patients on the right side, equally. Oval fossa form was most common in Class 2 and Class 3 patients. On the left side, the oval fossa form was most common in Class 1, Class 2 and Class 3 children. In the studies conducted, there is no standard classification in evaluating the condyle and fossa form, but different classifications have been used. Therefore, the convex shape accepted in one study may be included in the round or oval group in another study. Similarly, the condyle shape, which is considered angular, can be included in a different group depending on the section examined in another study. Differences in study results may be due to this situation.
The limitations of this study are that the sample size is limited because it was planned for pediatric patients. In addition, only radiographic features were evaluated; clinical features affecting TMJ morphology and morphometric features, such as bruxism, chewing habits, and parafunctional habits, were not evaluated.
Conclusion
According to the results of this study, the distance values of the condyle centers of both sides to the midsagittal plane were found to be less in hyperdivergent children compared to the other groups. In addition, it was determined that the anterior joint space width was reduced in hyperdivergent children and the condyle was located more anteriorly. However, changes were detected in some morphological and morphometric features of TMJ in children with different sagittal and vertical craniofacial morphology.
Data availability
The data sets used and analyzed during the current study are available from the corresponding author on reasonable request.
References
Enlow DH, Hans MG. Essentials of facial growth. Philadelphia: WB Saunders Company; 1996. p. 1–110.
Rakosi T, Jonas I, Graber TM. Color atlas of medicine: orthodontic-diagnosis. New York: Thieme Medical Publishers Inc.; 1993. p. 6–33.
Coşkuner HG, Kocadereli İ. Farklı malokluzyonlarda temporomandibular eklem pozisyonlarının değerlendirilmesi. Acta Odontol Turc. 2013;30(3):157–61.
Baccetti T, Antonini A, Franchi L, Tonti M, Tollaro I. Glenoid fossa position in different facial types: a cephalometric study. Br J Orthod. 1997;24(1):55–9.
Burke G, Major P, Glover K, Prasad N. Correlations between condylar characteristics and facial morphology in class II preadolescent patients. Am J Orthod Dentofac Orthop. 1998;114(3):328–36.
Ikai A, Sugisaki M, Young-Sung K, Tanabe H. Morphologic study of the mandibular fossa and the eminence of the temporomandibular joint in relation to the facial structures. Am J Orthod Dentofac Orthop. 1997;112(6):634–8.
Singh M, Chakrabarty A. Anatomical variations in condylar shape and symmetry: study of 100 patients. Int J Sci Res. 2015;4(12):933–5.
Yasa Y, Akgül HM. Comparative cone-beam computed tomography evaluation of the osseous morphology of the temporomandibular joint in temporomandibular dysfunction patients and asymptomatic individuals. Oral Radiol. 2018;34(1):31–9.
White SC, Pharoah MJ. Other imaging modalities. In: White SC, Pharoah MJ, editors. Oral Radiology: principles and ınterpretation. 7th ed. St Louis: Elsevier Health Sciences; 2014.
Harorlı A, Akgül M, Dağıstan S (2012) Diş Hekimliği Radyolojisi Kitabı, Erzurum: Eser Ofset Matbaacılık 80–150.
Al-koshas M, Nambiar P, John J. Assessment of the condyle and glenoid fossa morphology using CBCT in South-East Asians. PLoS ONE. 2015;10(3): e0121682.
Krisjane Z, Urtane I, Krumina G, Zepa K. Three-dimensional evaluation of TMJ parameters in Class II and Class III patients. Stomatologija. 2009;11(1):32–6.
Paknahad M, Shahidi S. Association between condylar position and vertical skeletal craniofacial morphology: a cone beam computed tomography study. Int Orthod. 2017;15(4):740–51.
Park I-Y, Kim J-H, Park Y-H. Three-dimensional cone beam computed tomography-based comparison of condylar position and morphology according to the vertical skeletal pattern. Korean J Orthodont. 2015;45(2):66–73.
McNamara JA. Components of Class II malocclusion in children 8–10 years of age. Angle Orthod. 1981;51(3):177–202.
Siriwat PP, Jarabak JR. Malocclusion and facial morphology is there a relationship? An epidemiologic study. Angle Orthodont. 1985;55(2):127–38.
George D, Mallery P. SPSS for windows step by step: a simple guide and reference. 11.0 update. 4th ed. Boston: Allyn & Bacon; 2003.
Odabaş B, Arslan SG. Temporomandibular eklem anatomisi ve rahatsızlıkları. Dicle Tıp Dergisi. 2008;35(1):77–85.
Zhang ZL, Cheng JG, Li G, Zhang JZ, Zhang ZY, Ma XC. Measurement accuracy of temporomandibular joint space in Promax 3-dimensional cone-beam computerized tomography images. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012;114:112–7.
Büyük S, Halıcıoğlu K, Çelikoğlu M, Şekerci A, Ünal T, Kilkiş D. Konik Işınlı Bilgisayarlı Tomografi Kullanılarak Elde Edilen İki Ve Üç Boyutlu Lateral Sefalometrik Analizlerin Karşılaştırılması. Atatürk Üniversitesi Diş Hekimliği Fakültesi Dergisi. 2014;24(2):213–8.
Kumar V, Ludlow J, Soares, Cevidanes LH, Mol A. In vivo comparison of conventional and cone beam CT synthesized cephalograms. Angle Orthod. 2008;78:873–9.
Ueda HM, Ishizuka Y, Mıyamoto K, Morımoto N, Tanne K. Relationship between masticatory muscle activity and vertical craniofacial morphology. Angle Orthod. 1998;68:233–8.
Ueda HM, Mıyamoto K, Saıfuddın M, Ishızuka Y, Tanne K. Masticatory muscle activity in children and adults with different facial types. Am J Orthod Dentofacial Orthop. 2000;118:63–8.
Proffit WR, Fields HW. Occlusal forces in normal-and long-face children. J Dent Res. 1983;62(5):571–4.
He T, Olsson S, Daugaard JR, Kılıarıdıs S. Functional influence of masticatory muscles on the fiber characteristics and capillary distribution in growing ferrets (Mustela putonusfuro): a histochemical analysis. Arch Oral Biol. 2004;49:983–9.
Rodrigues AF, Fraga MR, Vitral RWF. Computed tomography evaluation of the temporomandibular joint in Class II Division 1 and Class III malocclusion patients: condylar symmetry and condyle-fossa relationship. Am J Orthod Dentofac Orthop. 2009;136(2):199–206.
Vitral RWF, de Souza TC. Computed tomography evaluation of temporomandibular joint alterations in class II Division 1 subdivision patients: condylar symmetry. Am J Orthod Dentofac Orthop. 2002;121(4):369–75.
Seren E, Akan H, Toller MO, Akyar S. An evaluation of the condylar position of the temporomandibular joint by computerized tomography in Class III malocclusions: a preliminary study. Am J Orthod Dentofac Orthop. 1994;105(5):483–8.
Cohlmia JT, Ghosh J, Sinha PK, Nanda RS, Currier GF. Tomographic assessment of temporomandibular joints in patients with malocclusion. Angle Orthod. 1996;66(1):27–36.
O’Ryan F, Epker BN. Temporomandibular joint function and morphology: observations on the spectra of normalcy. Oral Surg Oral Med Oral Pathol. 1984;58(3):272–9.
Çağlayan F, Sümbüllü MA, Akgül HM. Associations between the articular eminence inclination and condylar bone changes, condylar movements, and condyle and fossa shapes. Oral Radiol. 2013;30(1):84–91.
Katsavrias EG. Changes in articular eminence inclination during the craniofacial growth period. Angle Orthod. 2002;72(3):258–64.
Katsavrias EG, Halazonetis DJ. Condyle and fossa shape in Class II and Class III skeletal patterns: a morphometric tomographic study. Am J Orthod Dentofac Orthop. 2005;128(3):337–46.
Akahane Y, Deguchi T, Hunt NP. Morphology of the temporomandibular joint in skeletal class iii symmetrical and asymmetrical cases: a study by cephalometric laminography. J Orthod. 2001;28(2):119–28.
Lobo F, Tolentino ES, Iwaki LCV, Walewski LÂ, Takeshita WM, Chicarelli M. Imaginology tridimensional study of temporomandibular joint osseous components according to sagittal skeletal relationship, sex, and age. J Craniofac Surg. 2019;30:1462–5.
Arieta-Miranda JM, Silva-Valencia M, Flores-Mir C, Paredes-Sampen NA, Arriola-Guillen LE. Spatial analysis of condyle position according to sagittal skeletal relationship, assessed by cone beam computed tomography. Prog Orthod. 2013;14:36.
Moscagiuri F, Caroccia F, Lopes C, Di Carlo B, Di Maria E, Festa F, Dattilio M. Evaluation of articular eminence inclination in normo-divergent subjects with different skeletal classes through CBCT. Int J Environm Res Public Health. 2021;18(11):5992.
Jiang H, Li C, Wang Z, Cao J, Shi X, Ma J, Liu H. Assessment of osseous morphology of temporomandibular joint in asymptomatic participants with chewing-side preference. J Oral Rehabil. 2015;42(2):105–12.
Raustia AM, Pyhtinen J. Morphology of the condyles and mandibular fossa as seen by computed tomography. J Prosthet Dent. 1990;63(1):77–82.
Pandis N, Karpac J, Trevino R, Williams B. A radiographic study of condyle position at various depths of cut in dry skulls with axially corrected lateral tomograms. Am J Orthod Dentofac Orthop. 1991;100(2):116–22.
Yale SH, Allison BD, Hauptfuehrer JD. An epidemiological assessment of mandibular condyle morphology. Oral Surg Oral Med Oral Pathol. 1966;21(2):169–77.
Merigue LF, Conti ACDCF, Oltramari-Navarro PVP, Navarro RDL, Almeıda MRD. Tomographic evaluation of the temporomandibular joint in malocclusion subjects: condylar morphology and position. Braz Oral Res. 2016;30(1):e17.
Katsavrias EG. Morphology of the temporomandibular joint in subjects with Class II Division 2 malocclusions. Am J Orthod Dentofac Orthop. 2006;129(4):470–8.
Acknowledgements
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article. ‘This article does not contain any studies with human or animal subjects performed by any of the authors.’
Funding
Not applicable.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The author(s) declare no competing interests.
Ethical approval
The study was approved by the Clinical Research Ethics Committee of the University Hospital (Ethics committee approval number: 72867572-050.01.04-737). All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5). Informed consent was obtained from all patients for being included in the study.
Informed consent
Informed consent form was not obtained as it was a retrospective study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Sırlı Yılmazturk, S., Bozdemir, E., Orhan, K. et al. Evaluation of morphological and morphometric characteristics of the temporomandibular joint in children with different skeletal models in the sagittal and vertical direction. Oral Radiol 40, 178–187 (2024). https://doi.org/10.1007/s11282-023-00718-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11282-023-00718-2