
Abstract
The intelligent bed, a mechanical hospital bed equipped with several electronic sensor functions, is an assistive healthcare solution intended to reduce the manual workload of health professionals by providing valuable real-time and non-vital information about patients. Implementation of the intelligent bed in the Chinese health care context has not been fully studied. The aim of this study was to explore the experiences of Chinese health professionals during a 12-month implementation period of the intelligent bed in a rehabilitation department at a large tertiary hospital in Guangzhou. A documentary study was carried out 3 months prior to implementation. Participant observation totalling 35 h and qualitative semi-structured interviews with 9 h and 50 min were conducted over a 12-month testing period. Findings in this study highlighted the improved working ergonomics of the intelligent bed in comparison with regular hospital mechanical beds. The bed’s other advanced functions, however, were either not used by the staff, quickly abandoned after a month, or never fully implemented. Barriers to full implementation of the bed’s functions were the Chinese hierarchical organizational culture, inadequate training of the health professionals on the implementation of the intelligent bed, lack of user-friendliness, and insufficient technical support.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
Today, long working hours, low wages, relatively low social status and escalating violence against healthcare staff have drastically reduced the willingness of Chinese people to become healthcare professionals (HP)s [1–3]. A recent national investigation showed that only 6.83 % of doctors supported their children pursuing the same career [4]. Another study found that only 13.5 % of nurses from the study hospital felt the same way [5]. On the other hand, it is estimated that by the year 2020, two-hundred and forty-eight million Chinese citizens will be over age 60, equivalent to 17.17 % of the population [6]. This massive elderly sub-population will require an unprecedented amount of healthcare resources. Hence, it is urgent to identify new reliable, automated and effective health technologies to meet this challenge. The intelligent bed (IB) was proposed by its designers as a potential solution to this demographic transition. The IB uses the frame of a standard mechanical hospital bed and is equipped with a number of sensors inside.
Previous studies of the IB in China focused on its technical design. The majority of the healthcare products were imitations from various Western countries [7]. Most of the studies were limited to a laboratory environment [8, 9]. None of these studies were implemented in Chinese healthcare facilities, and none considered the context relevant to Chinese frontline HPs. The attitudes and perceptions of HPs with respect to new health care technologies are considered critical to successful implementation [10–12]. Hence, it is important to evaluate IB implementation in China from the perspective of the Chinese frontline HPs who are going to operate it.
The aim of this study was to explore the experiences of Chinese HPs during a 12-month implementation period of the IB in a rehabilitation department at a major hospital in Guangzhou.
2 Methods and Materials
2.1 The Context of the Study
Guangdong Provincial Hospital of Chinese Medicine (GPHCM), Guangzhou University town branch is a tier 3 hospital opened in 2007. Tier 3 is the highest level in terms of clinical services capability in the Chinese hospital scoring system. The capacity of the rehabilitation department is 43 beds, although at times occupancy exceeds 50 beds. The patients suffer from a variety of diseases, including heart failure, stroke, spinal cord injury, hypertension and diabetes. In addition, some patients have cognitive or physical disabilities. Each patient is usually accompanied by a relative or a care assistant hired by the family, who watches over the individual throughout the day. That person’s job is to provide basic care (tooth brushing, bathing, etc.) on a daily basis, monitor the patient’s status and assist the nurses with manual labour (moving patients, repositioning, adjusting the height of the bed, etc.). The department has 16 trained nurses who work in three clinical shifts. Their level of work experience in healthcare services ranges from one to 18 years. There are also exchange nurses from other hospitals. The number in this group varies from month to month. Both Chinese and Western medicine are provided by the HPs. Prior to this study, the department used only ordinary mechanical hospital beds.
2.2 The Concept of the Evaluation
The conceptual framework of the evaluation was discussed in a previous study [13] (Fig. 1). The evaluation of the use of the intelligent bed used a “before”, “during” and “after” approach. This design enabled us to compare the healthcare service provided by the HPs before the deployment of the IBs and after their implementation in the rehabilitation ward. The experience of the Chinese HPs at the implementation phase were presented as part of the “during” phase. In the “after” phase, a technology acceptance model (TAM) was applied to determine whether the IB had been accepted by the HPs [14–17].

The conceptual framework of the evaluation
2.3 The IB
2.3.1 Selection of Functions for the IB
The IBs evaluated in this study were invented in Denmark. We assumed that there are differences between China and the Scandinavian countries in terms of user customs, technological capabilities and local technical infrastructure. Prior to the actual test period, two workshops were organised at the hospital before the onset of the test-period. Each workshop lasted a maximum of 3 h. The purpose was to ensure that the functions of the bed could be accommodated and adapted to in the environment of the Chinese ward. The first workshop was conducted with the participation of the head nurse, the director of the rehabilitation department and the first author of this study. In this workshop, the HPs expressed their expectations about the functions of the IB. The summary of the first workshop was then discussed with the Danish supplier and the first author in order to adapt the IB to meet the HPs’ functional expectations. In the second workshop, held 3 months later, the Danish supplier introduced same participants from the first workshop were introduced to the bed’s available functions (n = 10). The functionalities were then presented and discussed, and eight functions were selected which were deemed relevant by consensus. The whole study lasted for 12 months, from December 2013 to November 2014.
2.3.2 Description of the Functions in the IB
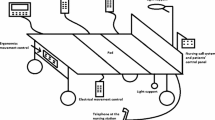
Once the HPs’ expectations had been met, five IBs were deployed with eight functions installed. Two types of beds were provided with the ratio of 4–1, since certain functions are mutually exclusive for technical reasons. The type 1 bed was equipped with all the features except electronic movement control. The type 2 bed had electronic movement control but lacked the electrical brake. The functionalities of the bed are depicted in Fig. 2.

The overview of the IB
The weight scale, wet sensor, out-of-bed sensor, electrical movement control, and ergonomic control have separate control panels for the nurses to use. In addition to these features, a patient control panel was installed for the functions of calling the nurse and elevating the bed. The signals from the nurse call feature and the out-of-bed sensor were sent to the telephone at the nursing station through a fixed landline. A detailed description of the functions of the IB is presented below (Fig. 3).

The functions of the IB based on wireless technology
Weight scale This function provides a body mass measurement of the patients. It consists of a control panel and a sensor system connected to the IB. The patient’s weight is shown on the panel screen. When the patient wants to remain in bed or is unable to be moved to an external weight scale, the HPs can press the buttons on the panel by following a few steps. The first step should be done before the patient uses the bed. This step generates the start value, i.e. the bed’s weight without the patient. The second step is when the patient is in the bed, and the patient’s weight can be calculated automatically by using current the bed’s weight value minus the start value. The patient’s weight can then be viewed on the screen without moving the patient out of the bed.
Wet sensor This function alerts nurses when the bed becomes wet due to urine or sweat. It consists of a cloth that contains moisture sensors located under the sheet but above the mattress. Based on the patient’s clinical need, the level of acceptable moisture can be adjusted through the particular panel. When the moisture content of the cloth reaches the designated level, indicating too much patients’ urine on the mattress, the wet sensor in the IB will detect incidents and sound an alarm in order to notify the caring relatives or HPs by the bedside.
Electronic ergonomics control This function adjusts the IB’s positions to meet patient’s need for care. The panel for this function has six buttons that control elevations of upper body, lower body, and overall bed. For some situations, such as taking meals, patients need to sit up in the bed. Relatives or the HPs can use the electronic ergonomic control panel and adjust the bed to a proper position for patients, especially for those with back issues. This function can also be utilized to facilitate certain clinical tasks, such as repositioning of patients.
Out-of-bed sensor This sensor detects absence of patients beyond a certain time setting. Four time-setting options available: 5 s, 5, 20, and 30 min. These options can be set through the out-of-bed sensor control panel. Some patients may have to go to the toilet at night alone, with a risk of falling down. If the time out-of-bed sensor exceeds the setting in minutes, an alarm will ring to notify the HPs through the telephone at the nursing station.
Electrical movement control This control provides additional physical assistance for transporting patients to other areas of the hospital for treatments such as physical therapy, etc. Its purpose is to reduce the risk of patients being injured when they are moved from the bed onto another transportation device. With this function, patients can be transported on the bed itself. Users can operate an electrical movement control and choose two speed settings from the panel, pressing buttons to move forward or backward.
Electrical brake This function is to ensure the stationary position of the bed. When the bed is transported to a new position for parking, like a new ward, this function prevents the wheels from rolling.
Nurse call This device provides instant voice communication between patients and nurses. Patients in need of assistance need only to press the button on the ‘nurse call’ button. The communication will then be established between patient and the HPs at the nursing station. This function was set up so that patients can easily speak to the HPs when necessary.
Bed light This feature provides light both above and under the bed at night. The HPs can turn on the light through the patient’s control panel. The function provides convenience to the users without disturbing neighbouring patients at night. In addition, when patients leave the bed, the sensors will detect the patients’ absence and the light will automatically turn on. This function can also be controlled manually in situations where, for example, the patient wants to read in bed.
2.3.3 Wireless Infrastructure
The functionality of the IB is based upon wireless technology. In the initial design phase, the information from the IB was supposed to be read from an iPad using wireless technology. However, the existing wireless network in the hospital at the time did not function properly and was unable to provide internet access to the iPad. Under these conditions, the research team was compelled to establish its own communication system by installing wireless routers in the corridor. However, Chinese hospital regulations required that the team submit an application to the administration board before any technical installation or construction could be implemented inside the hospital. This bureaucratic process was overly long and complicated and ended up exceeded the time permit of this study. As an interim solution, use of the iPad was replaced by a telephone using a fixed landline. The application of wireless technology is still achievable and can be used in the future implementation of the IB. As an evidence of capable to use wireless technology in the IB, our study in Denmark has utilized a personal digital assistant and backup phones to receive notifications from the IB wirelessly [18].
2.4 The Workshop
During the week when the IB arrived, there was a 2-h workshop to train the nurses how to operate these functions (Fig. 4). The functions were first described in a PowerPoint presentation. The nurses were then shown how to operate the bed in a hands-on approach. Two nurses received extra training to become expert users. The Chinese guidelines on how to use the bed were attached at the end of each bed as depicted in Fig. 3.

Training workshop for nurses learning to operate the IB functions
2.5 Design of the Study
The case study approach used was inspired by Yin et al. [19, 20]. The strength of a case study approach is that it provides a comprehensive and insightful exploration of the designated topic. Data triangulation techniques were applied to improve the reliability and validity of the study [21, 22]. The data collection techniques in this study included documentary study, qualitative semi-structured interviews and participant-observation.
Documentary study [23] We began reviewing the documents 3 months prior to implementation of the IB. We searched for local demographic and socio-economic data about the region, news reports on using telemedicine technology and policies and regulations in the local healthcare system. The goal was to obtain a first impression of the local context to the extent that it was pertinent to the study’s aims. The first and second author conducted the documentation study.
Participant-observation [24] Observation guidelines were developed before the test was initiated. Observations were conducted before, during and after the implementations of the IB. The following occasions were observed: implementation of the bed by the nurses; meetings with the HPs and administration board; and conversations among the patients, relatives and HPs in relation to the IB. The purpose was to obtain a basic understanding of the workflow, organisational learning and innovation culture, the attitudes of the HPs toward new technologies and their internal relations. Participant-observation was conducted by the first and second author over a total of 35 h.
Qualitative semi-structured interview [25] The interviews were conducted in the HPs’ native language, Chinese and were recorded in a face-to-face manner. An interview guide was developed beforehand. Data saturation was considered the key criterion to be achieved [26]. The first round of interviews (n = 14) was initiated within a week after the arrival of the IB. One more interview was finished 4 months later, after the arrival of the beds, due to a job transfer. The purpose was to obtain a first impression from the HPs on their use of the IB. The second round (n = 5) took place 5 months later. It was carried out to collect timely feedback during implementation. The third round of interviews (n = 10) was conducted at the end of the study. The goal was to gain a better understanding of how the IB had operated. The first author was present at all the interviews. They were recorded with a digital device and then transcribed by the first and third author. Being a local and native speaker, the third author was assigned to check the transcriptions in an effort to avoid misunderstandings due to dialects. The transcription was then translated into English by the first author for the non-Chinese speaking researchers in the group. We were aware of the loss of meaning during the translation. Hence, the English version was carefully, retrospectively compared to the Chinese originals. The back translation work was conducted by the first author.
Transferability of the study was achieved in two ways. First, the article provides an adequate description of the testing environment. Second, the study was constructed based on well-recognised theories including the TAM, and Rogers’ diffusion of innovation theory [27].
2.6 Ethical Considerations
The research protocol was approved by the local ethical committee of GPHCM. It was also submitted to the Danish National Ethical Committee for review. The study was conducted in accordance with the Helsinki Declaration. Oral informed consent was obtained before the interviews began. In this paper the respondents, all of whom native Chinese, are anonymised using Anglicized pseudonyms such as ‘Sophia’, ‘Amy’, etc. [28, 29].
2.7 Participants of the Study
The inclusion criteria for HPs as participants were:
-
Employed full-time in this hospital.
-
Minimum 3 years’ experience in using a digital device such as a smart phone.
Six HPs had left the rehabilitation department or went on a leave of absence during the study due to personal reasons or a transfer. All the participants were female. Their ages were in the range of 28 ± 8, apart from the director. In total, 9 h and 50 min of interviews were recorded and transcribed. For the 9 HPs participating over a continuous 8-month implementation period, interviews were recorded over 7 h and 20 min, averaging 49 min per person (Table 1).
2.8 Data Analysis
Data analysis was inspired by Kvale et al. and on our previous studies [28, 30, 31]. The interview data was analysed using NVivo software, version 10.0. The following steps were followed:
-
Five interviews were reviewed and coded initially in order to obtain an initial impression of the data. Interviews were carried out with the director, the head nurse and three of the frontline nurses who had continuously used the IB for 8 months. This process was repeated several times until all the data had been fully reviewed and interpreted.
-
A code tree was then developed from dialogues among the first three listed authors. It consisted of nodes, affiliated child nodes and relevant descriptions. The code tree was constructed based on the conceptual framework of the evaluation and the five coded interviews. Where there was disagreement, the other authors were invited to facilitate the analysis process.
-
The next step was a rough coding of all the transcriptions using NVivo 10.0. After this rough coding, the structure of the code tree was adjusted and refined by reviewing all the coded materials. The purpose was to identify relevant patterns and topics and to develop themes and sub themes that were pertinent to the research aim. The interpretation of the interviews was further broadened according to the participant observation and documentations.
-
The conceptual framework was utilized to facilitate comprehension on how the IB affects delivery of healthcare in the Chinese ward. It was also used to understand whether the IB was adopted by the Chinese HPs.
-
In the final step, several hypotheses in relation to the research aim were formulated to challenge the existing code tree. The purpose was to expand visions of the analysis by comparing the analysis to conventional ways of thinking on interpreting the results. The research group then discussed its design in order to validate and condense the data.
The data analysis was conducted by the first, second, third and last author. The first and third authors are Chinese and have engineering training. The other two are Danish, with backgrounds in nursing, psychology and organisational behaviour. The diverse areas of expertise of the authors helped avoid bias and ensure the comprehensiveness of the results both from interdisciplinary and transcultural perspectives.
The use of software can create distance between the data and the researchers. It increases the possibility of decontextualisation of the data. In addition, the NVivo software program 10.0 has provided a standard procedure for analysis and hence entails a risk of homogeneity.
3 Results
Experiences by the Chinese HPs using the IB are presented in this section.
3.1 Cultural Tendencies and Hierarchical Structure
The first feedback concerns the cultural and hierarchical structure of the Chinese healthcare system. At the initial meetings to decide on the functions of the IB, subordinate HPs such as frontline nurses were excluded from the decision-making process. In other words, not all the stakeholders of the IB were represented in the workshop for selecting the relevant functions. One of the nurses, Cecelia explained this shortcoming in the decision-making process: ‘Actually [those] like us, the ordinary nurses, do not have… the right to speak.’
In addition, it was found that not all the frontline nurses felt confident enough to express their opinions on the IB. Some of them were also reluctant to articulate their user experiences, especially when they felt that their opinions might conflict with the views of their superiors from the administration. Furthermore, there were practical challenges in summing up all the HPs’ views from one workshop. When the researchers asked the hospital administration board about the possibility of involving all the nurses in the workshop, the proposal was rejected as not being feasible. The lack of feasibility refers to the fact that the HPs work in three shifts, such that involving all the nurses in a single workshop would affect their ordinary clinical shifts. However, based on the data from the participant-observation and understanding of Chinese culture in the hospital setting, it is also possible that the board might have had concerns about their authority being undermined by the presence of subordinate staffs.
3.2 Education Program
The second barrier is education program for learning how to operate the IB did not match the needs of the clinical staff. During the study, nurses left the rehabilitation department for other jobs or went on leave of absence due to transfer or for personal reasons.
As explained by Amy: ‘It is already more than half, many of the staff have been replaced… [or] transferred to other departments.’ And from Lydia: ‘Yes, [they] left their job or some went to other departments… and then some became pregnant.’
3.3 Complex Functionality of the Bed
The third barrier concerns the functionality of the IB. The technical components did not fit the end users’ needs. Amy: ‘Maybe … some functions are not necessary for our department’ And from Hilary: ‘It is indeed [the case that] we did not use all the functions.’
In addition, an excess of functions caused frustrations among the HPs in utilizing the IB. According to Sophia: ‘Too many functions make [the IB] hard to use.’
As a result, the HPs ended up disconnecting most of the functions after just one month of implementation.
3.4 Technical Support
The technical support for the bed was not organised well. Communication regarding bed maintenance between users and suppliers was not efficient. As Jennie explained: ‘We made calls to the maintenance service, and the process is complex…, we don’t know why.’ In addition, the Chinese nurses do not habitually use e-mail for communication. Rather, they preferred to call for support by telephone, and complained that it was difficult to reach the supplier.
In the end, no training was given to the technical staff of the hospital. The need for such training was clear. Amy confirmed: ‘Of course training the technical department is definitely necessary.’ And from Cathy: ‘Yes, here we use [the IB], we also need people who know how to fix it.’ There were also difficulties with arranging a visit from the supplier due to scheduling and geographical distance. As Amy commented: ‘the company is in Shenzhen [but the bed is in Guangzhou]… and about the engineer, we need to book his time.’ Another complaint from Kate: ‘We ask for maintenance [of the IB], [but] it takes a long time to repair.’
3.5 Benefits to the HPs
It was found that the HPs appreciated the elevation function. It provided better ergonomic positions for the HPs and others who had to lift the bed, relieving them from some manually exhausting labour. As evidenced from the participant-observation, when adjusting the height of the old mechanical bed, the nurses had to bend down or squat to rotate the handles, requiring much strength, with the risk of back strain. The new IB achieved this function by simply pressing the button on the control panel. Comments from five HPs praised the benefits:
Jennie: ‘We [spent] a lot of time rotating the handles. Now it’s just about pressing the button, very convenient.’
Lydia: ‘[The IB] can reduce the [number of] times [we] bend our backs.’
Amy: ‘When doing the repositioning, it can save nurses’ backs.’
Sophia: ‘This is good, so that we can spend more time on the professional clinical tasks instead of [manual] labour.’
Cathy: ‘[The IB] saves a lot of energy.’
Technical barriers and usability of the IB are described in the following paragraphs.
3.5.1 Overall Technical Setup
The out-of-bed sensor and nurse call were connected to the telephone at the nursing station through a fixed landline that unfortunately, did not fit into the workflow of the rehabilitation department. Every morning, patients were transported to the rehabilitation exercise centre in a separate location. HPs then had to physically disconnect the line if they wanted to move the IBs. Furthermore, the types of events that set off alarms were not perceived as emergencies by the HPs. The out-of-bed sensor was connected to the telephone at the nursing station. The ringing from this telephone was traditionally perceived as an emergency. During the implementation, however, the alarm set off by the out-of-bed sensor was not considered by the nurses as an emergency. Its inaccuracy brought extra work and frustration to the nurses, especially at night. As Lilly comments: ‘Too many [alarms from the out-of-bed sensor] are… and very annoying.’
3.5.2 Weight Scale
In terms of the weight scale, according to the primary goal of treatment and patients’ health situation, the body mass was not critical data but still had to be measured. As Cecelia commented: ‘In our department, we only care [about the patients’ weight] from a nutrition perspective… the weight is not [what] matters.’ According to Susanna, ‘the patients in our department are relatively stable…so we rarely have those special medicines [the medicine that is strictly controlled based on the weight].’ And from Hilary: ‘For the stroke patients, we still have requirements as to body mass… the bed with the weight measurement is a… very good function that we need to keep.’
3.5.3 Wet Sensor
For the wet sensor, only one pad per bed was provided, and the nurses worried about its replacement, both in the short and long run. As Susana comments: ‘Only one pad, and then what to do if it is not working… our patients used 10 or 20 diapers per day.’ From Cecelia: ‘like in our department, every day the pad is wet, if washed and dried on a daily basis, within less than half a year… even the best quality [pad] cannot sustain [that] for half a year.’ Furthermore, the Chinese HPs questioned whose responsibility it was to clean the pad. As Cecelia explains: ‘Like if there is no relative, does that require [that] our doctors and nurses to wash [the pad]? We are already very busy.’ It was also necessary to wash the pads separately from other sheets so that they would not get lost. This was seen as extra work by the HPs. In addition, there were frequent visits by nurses to check the moisture level. The patients, relatives and care assistants also facilitated the work. As Cecelia comments: ‘[every] two hours [we] will definitely have one check [from the nurses on the moisture level], and also the care assistant, the relatives check even more frequently.’ Eventually, the sheet and mattress all had to be replaced if urine or sweat had reached the pad. This is perceived as heavy work by nurses. As Amy complained: ‘the point is that if you wait until the pad is wet, it then tells us that the sheets [and] mattress of the bed are already… wet… If it is this kind of wet situation, we need to change them all.’
3.5.4 Electrical Ergonomics Control
The nurses used the electrical ergonomics control on a daily basis, and they liked it. As Clare commented: ‘Every day we use [the electrical ergonomics control] to lift him/her up and down.’ Hilary also praised this function: ‘Yes. The electrical ergonomics control is great, and we used it quite often.’
3.5.5 Out-of-Bed Sensor
The out-of-bed sensor was not used after its initial utilization. The patients who use the IB have limited ability to move, and this function was not seen as necessary. As explained by Cathy: ‘We abandoned this function because our patients, those ones using the IB, can move or get out of the bed only if there is assistance, so we did not set up this alarm.’ And also from Kate: ‘Our patients here are all… disabled and stay in bed.’ Moreover, the relatives and care assistants were generally present on a 24-h basis. The nurses also visited patients every 2 h. Cathy explained: ‘Yes, we check [the patients] frequently, and so [do] the care assistants and relatives.’
3.5.6 Electrical Movement Control
The electrical movement control function was abandoned after the first few times of operation because the bed was considered too difficult to manoeuvre. The nurses complained that the bed was too heavy to move and change direction, even with this component. As Lily explained, ‘The most important [thing] is that this bed is too heavy.’
3.5.7 Electrical Brake
The electrical brake is the function automatically locks the bed within one minute, which requires additional use of the panels to unlock the brake. This design was considered by the HPs as not user-friendly. As Kate explained: ‘[the bed] is just very hard to unlock… if after a little while not using it, [when] we go to move other stuff, it will be locked again.’ Cited from Lily: ‘Even [after] we have unlocked the bed, it is still not very easy to control.’
3.5.8 Nurse Call System
The nurse call system from the IB, when compared to the previous one in the ward, was perceived as less user-friendly. As Helen commented: ‘Because in our department there are some patients [who] are elderly, and then it is not very convenient for them, even … lifting up the hands was difficult… they have to figure out where the panel is. Pressing the button is not easy, but with [the previous nurse call], he could just grab and press [the button].’ What is more, the patients were being attended to by relatives or care assistants day and night. As Lily explained: ‘Our department is a bit special, basically all [the patients] have care assistants, and relatives will also be there.’
3.5.9 Bed Light
The bed light function did not fit into the environment of the Chinese rehabilitation ward, and there was already enough light. As Susana states: ‘In every ward, we already have light under the bed [before the arrival of the IB]…and we do not use the light above the bed, very often.’ And also from Cecelia: ‘Patients would not go to the toilet [at night]’. Furthermore, according to the regulations of the hospital, the main room light should be on when doing treatment at night. In addition, the design of the light above the bed was not considered user-friendly. As cited from Kate: ‘Sometimes the light above the bed, [its handle] is not fixed, and [it] sometimes hits the patients.’ And from Mary: ‘The light above the bed, its handle is not very user-friendly.’
The outcome using the evaluation model from Fig. 1 is presented below.
Figure 5 illustrates the experience of the Chinese HPs during the study by using a timeline. The figure is the application of the evaluation model shown in Fig. 1.

Results using the evaluation model in the implementation phase
As presented above, a number of organisational and technical barriers related to the operations arose during implementation. Most functions were ignored or disconnected during the trial, resulting in inadequate evaluation. While the electrical ergonomics controls were highly valued by the HPs for reducing manual workload, the more advanced functions were perceived as unreliable, complex, time-consuming and/or irrelevant by the HPs. Lack of training and insufficient communication regarding maintenance were also highlighted.
4 Discussion
The aim of this study was to explore the experiences of Chinese HPs during a 12-month implementation period of the IB in a rehabilitation department at a major hospital in Guangzhou. Unlike previous studies on this subject, our study pioneered the investigation of the implementation of the IB, a European technology, in a real Chinese healthcare context [32, 33].
4.1 Discussions of Experiences by the Chinese HPs Using the IB
4.1.1 Cultural Tendencies and Hierarchical Structure
Cultural traditions and hierarchical healthcare organisation structure play a major role in the decision-making process in the Chinese health care system. It was considered the job of administrative staff to make decisions. The frontline HPs, especially the young nurses in this case, were perceived as subordinate in relation to the decision-making process. This finding is similar to that of Cooke et al.’s study [34]. This form of decision-making distanced the actual users of the technology from its supplier. In addition, this decision-making process may have had a negative impact on the usefulness of the functions selected.
4.1.2 Education Program
The nurses stated that the training program on how to use the IB was inadequate. This was due to the fact that the nurses were frequently transferred to other departments or went on leave of absence for other reasons. When the nurses were not using the technology on a daily basis, there was a risk that they would not have the technology integrated into their workflows, which made implementation of the IB more difficult. This finding highlights the importance of educating the HPs with consistency and potentially including follow-up sessions to ensure that HPs are still familiar with the IB functions. Similar results have been reported in other studies [35, 36]. The expert users trained in the workshop did not provide any feedback in this study. This suggests that at least in the Chinese context, training expert users was not effective.
4.1.3 Complex Functionality of the Bed
It was found that the intelligent components were disconnected after 1 month of implementation. The HPs reported that the functions did not meet their needs and were too complex. This indicated that the functions did not suit the environment of the Chinese rehabilitation department. The HPs thus chose to refuse to use most of the functions. The feedback from the HPs can also be categorised as pertaining to the usability of the IB and its ease of use. In terms of usability, this study highlights the importance of acquiring adequate information from the HPs on their expectations about the technology. Additionally, we recommend considering the idea of modular design. The bed could be designed so that the most useful or preferred sensors could be easily installed and others removed. This idea was originally intended to meet the needs of different types of patients as well as their changing health situation. This recommendation would also improve the flexibility of implementation. As for ease of use, we advise that in tests of the IB as well as other health care technologies, the number of functions should be controlled to avoid the risk of technophobia.
4.1.4 Technical Support
According to the HPs, maintenance of the IB was not performed well. Several related issues were cited, including insufficient communication, shortage of training for technicians and difficulties arranging visits from suppliers. Each of these issues has the potential to undermine the successful implementation of the IB. In particular, without an established communication method, the HPs were unable to reach the suppliers and arrange repairs on time. If the IB was not operating properly for a prolonged period, the HPs would become frustrated. Poor operation would eventually affect the attitudes of the HPs toward the use of the IB. Furthermore, training hospital technicians to maintain or repair the IB was needed, as this would have effectively ensured timely maintenance of the machines, avoiding delays due to the distance between the hospital and suppliers. This recommendation is supported by Brewer [37]. These issues certainly support the necessity to develop a streamlined maintenance plan involving HPs, technical staff and suppliers. A thorough consideration and discussion of these issues would be necessary prior to deployment of the IB. This finding is similar to that of Broens’s study [38].
4.1.5 Benefits to the HPs
We have found that the elevation function brought benefits to the HPs. This was the only function that the HPs used on the daily basis. Their positive feedback on this function warrants its further application on a wider scale. There may be a paradigm shift in the workflow of the HPs when the numbers of the beds reaches a certain tipping point. Furthermore, this function can provide a better ergonomic position by decreasing the number of times HPs must bend their backs in each work routine. We believe that this benefit would decrease the risk of back injuries resulting from the undesirable working position [39, 40]. It would ultimately improve the health situation of HPs over the long term. Interviews and participant-observation revealed that the HPs spent many hours per shift elevating beds manually. This work assignment, with its risk of back injury, could be changed if the IB were introduced on a larger scale. As the nurses are professional health providers, most of them spend years receiving clinical education; distributing this amount of labour to clinical staff is arguably not economical for the hospital. Furthermore, most of them were young females, as stated previously. They have physical limitations when it comes to carrying out heavy physical labour, such as frequently moving patients. If the Chinese nurses have to carry out this amount of manual labour on the daily basis, there would be negative effect on their morale and ultimately, their willingness to continue in this career. It can be argued that focusing on decreasing the amount of heavy physical labour tasks is critically important to improving the performance of HPs [41]. HPs would then be able to spend more time focusing on clinical practice. This goal is advocated by Kocher [42]. It might also be a good way to bypass the risk of malpractice due to the exhaustion of HPs, and to increase the quality of care at the same time. We further believe that it is a practical solution for many developing countries applying healthcare technology, especially in cases where the technical infrastructure has not reached a European level.
4.2 Discussion of Technical Barriers and Usability of the IB
The overall technical set up did not fit into the work routines of the rehabilitation department during the implementation of the IB. These findings were the result of four factors: patients’ health situations, the environment of the ward, work routines and user-friendliness. Starting from the first factor, the health situations of patients determine their medical needs. These types of needs are related to the usability of the technology [43–45]. We therefore suggest that a full investigation of patients’ health situations would be important when implementing IBs. Moreover, ongoing changes in the patient’s health status should also be taken into consideration. The improvement or worsening of patients’ health would require different types of technology. The Chinese ward environment was different from what we have observed in Europe. Relatively underdeveloped infrastructure (size of the ward, number of electrical outlets, etc.) and the 24/7 accompaniment of relatives and care assistants make up the most important differences. These non-professional caregivers can perform the task of monitoring the status of the patients, which is why functions like the wet sensor and out-of-bed sensor were found to be superfluous and not used. These differences suggest that the primary mission of the IB should not be that of patient monitoring. The nurses visited the patients at least every 2 h, a work routine that enabled frequent visits from the HPs. The occasions when the nurses appeared were not based on the alarm sent from the IB, but on the arrangements made by administrative staff. This indicated a low level of confidence in the health care technology at the administration level. This feeling deepened when the timely maintenance of the IBs proved problematic. User-friendliness was critical in the implementation [46, 47]. We recommend that in the initial phase of a larger implementation study in the future, trainers being by introducing a few simple and easy-to-handle technological features in order to build users’ trust in the device, and then introduce more advanced features only later. User-friendliness problems arose with different functions, such as electrical movement control, electrical brake, bed light and nurse call. This indicates the need for further adjustments to these functions so as to better adapt to the Chinese ward environment.
The feedback discussed above has implications for future studies. This can be referred to explore what managerial, operational and social-cultural factors that might affect implementation of Western healthcare technology in China [48]. The Chinese frontline nurses were not actively involved in the choice of the technical functions. This disadvantage in the design phase has arguably distanced the technology from its daily users. In our implementation process, the functions of the intelligent bed were not fully utilized in the Chinese rehabilitation department. This indicates that it is necessary to include all the users of technology even it is in the design phase so as to ensure that the technology can provide maximum benefits to match local healthcare context. It is necessary to fully understand the Chinese hierarchical structure and cultural traditions as expressed in the Chinese workplaces. This need does not apply solely to the arena of healthcare technology, of course. It is necessary for all implementation studies in China. It is critical to develop a new implementation strategy that can identify and then avoid, or at least limit, conflicts due to social-cultural differences. In this study, there is a need to include all the subordinate HPs in the decision-making process without offending the administration board. Ultimately, communication about technical assistance, education and training of the staff is also important in any successful implementation of technologies [49].
In summary, although the elevation functions have generated benefits to the HPs on a daily basis, the bed’s advanced features remained unused due to a combination of inadequate training for the HPs and hospital technicians, poor user-interface experience and insufficient communication and maintenance obstacles. Furthermore, in the initial selection of the IB’s functions, factors including patients’ health situations, the environment of the ward and the structure of existing work routines were not taken into consideration.
5 Conclusions
The IB provided better working ergonomic positions to HPs, but its other advanced functions were disregarded or not fully utilized after 1 month of implementation. Barriers to full implementation were the Chinese hierarchical organizational culture, inadequate training of the HPs on the implementation of the IB, lack of user-friendliness, and insufficient technical support. We found that when transferring Danish healthcare technology into a Chinese context, the implementation process is complex, as the functionality of the Danish IB was not adjusted to Chinese culture and the Chinese care system. This led the Chinese HPs to avoid using, or simply reject the functionalities of the Danish IB.
References
Li, J. (2010). Research on work satisfaction and willing of leaving jobs of nursing staffs. Shanghai Nursing, 10(2), 83–87.
Yang, T., & Zhang, X. (2011). Investigation and analysis on nurses’ feeling of accomplishments in China. Work Secures the World, (1), 53–55.
Hesketh, T., Wu, D., Mao, L., & Ma, N. (2012). Violence against doctors in China. BMJ, 345, e5730. doi:10.1136/bmj.e5730.
Chinese Medical Doctor Association. (2011). The fourth time inquiry on the careers of doctors. http://www.cmda.net/gongzuodongtai/zhinengbumen/2011-08-08/9778.html. Accessed April 18, 2016.
Yang, J., & Gao, L. (2015). The investigation on health care staffs’ attitudes towards their children choosing nursing as a career. Education Teaching Forum (3), 73–74.
The National Office on Elders. (2006). The prediction of aging population trend in China. http://news.xinhuanet.com/video/2006-10/11/content_5467909.htm. Accessed April 17, 2016.
Liao, Y. (2013). The development and trend of the intelligent bed. Medical Equipment, 2(10), 5–7.
Ge, X. (2014). Developments on smart home intelligent bed and health status monitoring system based on the internet of things. Management and Technology of Small and Medium Size Enterprise, (9), 241–242.
Pu, W., Li, M., Yu, H., Shen, L., Chen, R., & Ding, H. (2007). Design of an intelligent nursing bed with fall-proof function. Journal of Clinical Rehabilitative Tissue Engineering Research, 11(48), 9765–9767.
MacNeill, V., Sanders, C., Fitzpatrick, R., Hendy, J., Barlow, J., Knapp, M., et al. (2014). Experiences of front-line health professionals in the delivery of telehealth: A qualitative study. The British Journal of General Practice: The Journal of the Royal College of General Practitioners, 64(624), e401–e407. doi:10.3399/bjgp14X680485.
Hu, P. J., Chau, P. Y. K., Sheng, O. R. L., & Tam, K. Y. (1999). Examining the technology acceptance model using physician acceptance of telemedicine technology. Journal of Management Information Systems, 16(2), 91–112. doi:10.2307/40398433.
Menachemi, N., Burke, D., & Ayers, D. (2004). Factors affecting the adoption of telemedicine—A multiple adopter perspective. Journal of Medical Systems, 28(6), 617–632. doi:10.1023/B:JOMS.0000044964.49821.df.
Cai, H., Toft, E., & Dinesen, B. (2015). A conceptual framework for the effect evaluation of the intelligent bed. Wireless Personal Communications, 80(4), 1405–1414. doi:10.1007/s11277-014-2090-7.
Venkatesh, V., & Davis, F. D. (2000). A theoretical extension of the technology acceptance model: Four longitudinal field studies. Management Science, 46(2), 186–204. doi:10.1287/mnsc.46.2.186.11926.
Davis, F. D., Bagozzi, R. P., & Warshaw, P. R. (1989). User acceptance of computer technology: A comparison of two theoretical models. Management Science, 35(8), 982–1003. doi:10.1287/mnsc.35.8.982.
Davis, F. D., & Venkatesh, V. (1996). A critical assessment of potential measurement biases in the technology acceptance model: Three experiments. International Journal of Human–Computer Studies, 45(1), 19–45. doi:10.1006/ijhc.1996.0040.
Davis, F. D. (1989). Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Quarterly, 13(3), 319. doi:10.2307/249008.
Cai, H., Toft, E., Hejlesen, O., Hansen, J., Oestergaard, C., & Dinesen, B. (2015). Health Professionals’ User Experience of the intelligent bed in patients’ homes. International Journal of Technology Assessment in Health Care, First View,. doi:10.1017/S0266462315000380.
Yin, R. K. (2013). Case study research-design and methods (5th ed.). Los Angeles: SAGE Publications.
Yin, R. K. (1999). Enhancing the quality of case studies in health services research. Health Services Research, 34(5 Pt 2), 1209–1224.
Mays, N., & Pope, C. (2000). Qualitative research in health care. Assessing Quality in Qualitative Research. BMJ, 320(7226), 50–52. doi:10.1136/bmj.320.7226.50.
Ammenwerth, E., Iller, C., & Mansmann, U. (2003). Can evaluation studies benefit from triangulation? A case study. International Journal of Medical Informatics, 70(2–3), 237–248. doi:10.1016/S1386-5056(03)00059-5.
Noor, K. B. M. (2008). Case study: A strategic research methodology. American Journal of Applied Sciences, 5(11), 1602–1604. doi:10.3844/ajassp.2008.1602.1604.
Patton, M. Q. (1999). Enhancing the quality and credibility of qualitative analysis. Health Services Research, 34(5 Pt 2), 1189–1208.
Britten, N. (1995). Qualitative research: Qualitative interviews in medical research. BMJ, 311(6999), 251–253. doi:10.1136/bmj.311.6999.251.
Cleary, M., Horsfall, J., & Hayter, M. (2014). Data collection and sampling in qualitative research: Does size matter? Journal of Advanced Nursing, 70(3), 473–475. doi:10.1111/jan.12163.
Rogers, E. M. (2003). Diffusion of innovations (5th ed.). New York: Free Press.
Brinkmann, S., & Kvale, S. (2014). Interviews: Learning the craft of qualitative research interviewing (3rd ed.). Los Angeles: SAGE Publications.
DiCicco-Bloom, B., & Crabtree, B. F. (2006). The qualitative research interview. Medical Education, 40(4), 314–321. doi:10.1111/j.1365-2929.2006.02418.x.
Dinesen, B., & Toft, E. (2009). Telehomecare challenge collaboration among healthcare professionals. Wireless Personal Communications, 51(4), 711–724. doi:10.1007/s11277-009-9767-3.
Dinesen, B., Huniche, L., & Toft, E. (2013). Attitudes of COPD patients towards tele-rehabilitation: A cross-sector case study. International Journal of Environmental Research and Public Health, 10(11), 6184–6198. doi:10.3390/ijerph10116184.
Zhang, L. (2013). Invention of intelligent assistive devices in China: Today and future. Chinese Journal of Rehabilitation Theory and Practice, 19(5), 401–403. doi:10.3969/j.issn.1006-9771.2013.05.001.
Zhai, J., Xu, X., Liu, C., & Xie, C. (2010). Design study of a novel intelligent health care and monitoring bed. Journal of Machine Design, 27(8), 35–37, 82, doi:10.13841/j.cnki.jxsj.2010.08.022.
Cooke, F. L., & Zhan, C. (2013). Between market and bureaucracy: Public healthcare reforms in China and nurses’ terms and conditions. The International Journal of Human Resource Management, 24(16), 3178–3195. doi:10.1080/09585192.2013.775034.
Sirois, P., Fournier, H., Lebouthilier, A., Guerette-Daigle, L., Robichaud, S., Leblanc-Cormier, G., et al. (2013). Nurses’ perceptions and attitudes towards new ADU technology and use. Technology and Health Care, 21(1), 41–47. doi:10.3233/Thc-120708.
Gagnon, M. P., Orruno, E., Asua, J., Abdeljelil, A. B., & Emparanza, J. (2012). Using a modified technology acceptance model to evaluate healthcare professionals’ adoption of a new telemonitoring system. Telemedicine and e-Health, 18(1), 54–59. doi:10.1089/tmj.2011.0066.
Brewer, E., Demmer, M., Ho, M., Honicky, R. J., Pal, J., Plauche, M., et al. (2006). The challenges of technology research for developing regions. Pervasive Computing, IEEE, 5(2), 15–23. doi:10.1109/MPRV.2006.40.
Broens, T. H. F., Huis in’t Veld, R. M. H. A., Vollenbroek-Hutten, M. M. R., Hermens, H. J., van Halteren, A. T., & Nieuwenhuis, L. J. M. (2007). Determinants of successful telemedicine implementations: A literature study. Journal of Telemedicine and Telecare, 13(6), 303–309. doi:10.1258/135763307781644951.
Knibbe, J. J., & Friele, R. D. (1996). Prevalence of back pain and characteristics of the physical workload of community nurses. Ergonomics, 39(2), 186–198. doi:10.1080/00140139608964450.
Yip, Y. B. (2001). A study of work stress, patient handling activities and the risk of low back pain among nurses in Hong Kong. Journal of Advanced Nursing, 36(6), 794–804. doi:10.1046/j.1365-2648.2001.02037.x.
Rufo, R. (2011). Behind the scenes with integrated telemedicine. Nursing Management (Springhouse), 42, 6–9. doi:10.1097/01.numa.0000406582.33874.16.
Kocher, R., & Sahni, N. R. (2011). Rethinking Health Care Labor. New England Journal of Medicine, 365(15), 1370–1372. doi:10.1056/NEJMp1109649.
Kidholm, K., Ekeland, A. G., Jensen, L. K., Rasmussen, J., Pedersen, C. D., Bowes, A., et al. (2012). A model for assessment of telemedicine applications: Mast. International Journal of Technology Assessment in Health Care, 28(1), 44–51. doi:10.1017/S0266462311000638.
Karsh, B. T. (2004). Beyond usability: Designing effective technology implementation systems to promote patient safety. Quality and Safety in Health Care, 13(5), 388–394. doi:10.1136/qhc.13.5.388.
Aggelidis, V. P., & Chatzoglou, P. D. (2009). Using a modified technology acceptance model in hospitals. International Journal of Medical Informatics, 78(2), 115–126. doi:10.1016/j.ijmedinf.2008.06.006.
Stowe, S., & Harding, S. (2010). Telecare, telehealth and telemedicine. European Geriatric Medicine, 1(3), 193–197. doi:10.1016/j.eurger.2010.04.002.
Demiris, G., Charness, N., Krupinski, E., Ben-Arieh, D., Washington, K., Wu, J., et al. (2010). The role of human factors in telehealth. Telemedicine and e-Health, 16(4), 446–453. doi:10.1089/tmj.2009.0114.
Koumaditis, K., Themistocleous, M., & Cunha, P. R. D. (2013). SOA implementation critical success factors in healthcare. Journal of Enterprise Information Management, 26(4), 343–362. doi:10.1108/JEIM-06-2012-0036.
Yao, W., Chu, C. H., & Li, Z. (2012). The adoption and implementation of RFID technologies in healthcare: A literature review. Journal of Medical Systems, 36(6), 3507–3525. doi:10.1007/s10916-011-9789-8.
Acknowledgments
The authors would like to thank Mr. Hjalte Holm Andersen and Ms. Ida Munk Petersen for their comments on the article. We also wish to thank the Department of Health at Guangdong Province, the Royal Danish Consulate General in Guangzhou, and Guangdong Provincial Hospital of Chinese Medicine for their cooperation. We thank Linak A/S for providing five IBs to the study. We especially thank Mr. Ole Lindholm, Mr. Karsten Westermann, Mr. Simon Jenkinson, Ms. Grethe Koudal, Mr. Long Zhao, Mr. Xiang Gao, Mr. Shengwang Wan, Mr. Rongyuan Yang and the rest of staffs from the Chinese hospital for their support.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have nothing to disclose.
Rights and permissions
About this article

Cite this article
Cai, H., Krebs, H.J., Tao, Y. et al. A Qualitative Study on Implementation of the Intelligent Bed: Findings from a Rehabilitation Ward at a Large Chinese Tertiary Hospital. Wireless Pers Commun 90, 399–420 (2016). https://doi.org/10.1007/s11277-016-3375-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11277-016-3375-9