
Abstract
This article has presented a conceptual framework for the effect evaluation of the intelligent bed. The overall study is inspired by the case study design. Different functions with wireless sensor technology have been tested in Denmark and China. We have included technical aspects concerning on how different hardware have been operated in the different contexts, and how these applications and standards affect the process of performing clinical tasks. We have also discussed how the cultural differences and barriers can be highlighted by the evaluation system in the test of the intelligent bed. We concluded that it is important to realize the difference on the local social–cultural, economic context as well as the technical infrastructures. A process perspective should bear in mind when adopting new technology. It is also important to involve all the stakeholders including patients, healthcare professionals and researchers, etc., as a good way to facilitate the process of accepting of the technology.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Background
The intelligent bed is a nursing bed applied with different sensor technologies inside. The design purpose is to improve the feeling of security of patients, decrease workload for Health Professionals (HP), and ultimately improve quality of care. However, evidences suggest the proclaimed benefits are not robust. One of the reasons is due to the immaturity of the technology. But most importantly, a comprehensive and rigid effect evaluation framework is missing.
By reviewing the previous studies, most of the research focuses on developing specific technical features and tests in a limited laboratory environment. It has suspicious to simplify the surrounding circumstances and hence lack of considerations on the local economic, social and cultural factors [1]. Furthermore, the in-depth views of the users are not considered seriously [2]. This is due to their opinions on the use of the technology is sometimes biased as unprofessional, individual based and also involved the feeling of resistance to change [3]. Finally, the western health science has a long tradition of quantitative evidence based, there is a strong tendency to apply Randomized Controlled Trails (RCT) in the research. This may results a shortage of insight views on the implementation of technology from the users’ perspectives [4]. Except the publication bias, these barriers above can partly explain why most of the published results in the recent years are positive, but the application of the technology is still not widespread [5].
The aim of this paper is to develop a new conceptual framework on the effect evaluation of the intelligent bed.
2 Materials and Methods
2.1 Design Phase in China
The intelligent bed was tested in a rehabilitation ward at a prestigious hospital in the country which applying both western and Chinese medicine in the treatment. Before the delivery of the intelligent bed, we have initiated two workshops to decide what functions to be included in the test in relevant to the context. Each workshop lasted maximum 3 h. The first work shop was held 8 months before the delivery of the intelligent bed to get a general picture on the necessity of the patients and the HPs there. The participants included the chief doctor of the department, the leading nurse and one researcher. The summary of the workshop was then presented and discussed with the Danish vendors afterwards. The second workshop was held 5 months before the implementation to finalize the choice of the functions and ensure its technical feasibility. The participants include the chief doctor, the leading nurse, one researcher, one engineer and two employees from the company. During the workshop, we also visited and talked with the patients, relatives and care assistants in the ward, to get a closer look on what function was really necessary.
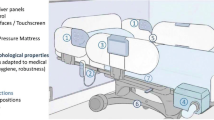
The functions of the intelligent bed tested in China include: weight scale, out of bed detector, light support both above and under the bed, nursing call system, wet sensor, ergonomics movement control and electrical movement control (Fig. 1).

The design of the intelligent bed in China
The measurement on the weight of the patients can be illustrated on the weight scale panel. The moist level of the mattress was monitored by the pad in the bed and alarmed from the wet sensor panel. There was light support both above and under the bed to facilitate the life of the patients, for instance, preventing falls when patients are going to the toilet at night. Ergonomics movement control was placed at the end of the bed, it can adjust the elevation of the bed and block the functions in the patients’ control panel when it is necessary. Electrical movement control was to move the bed both forward and backwards, lock the bed when it is in the ward. Signals from the out of bed sensor and nursing call system were connected to the telephone at the nursing station through the cables on the wall (Fig. 2).

The workshop for training the Chinese HPs
At the first arrival week of the intelligent bed, the researchers and the vendors have conducted a 2-h workshop to teach the HPs on how to use the functions of the intelligent bed. The HPs were taught hand by hand around the bed. Two nurses were given extra training to become the key users.
2.2 Implementation Phase in China
Five intelligent beds were deployed in the Chinese rehabilitation department. The beds were allocated to the patients who had stroke or disability. Most of the patients spent at least 2 years in the hospital, an extreme case were 8 years. The final decision on who to use the bed was made by the director. The beds were located within 20 m from the nursing station. This was due to the cautious attitudes on the new technology in case that the functions were not working. In the morning at 7:00, by using the ergonomics movement control, the patients were elevated to receive the basic nursing (tooth brushed, etc.) and then had breakfast. Afterwards, the patients were transported to the exercise center by using the electrical movement control. In the noon, the patients were back from the center and had their lunch. Then at 14:00, some of the patients were back to the center again to finish the rest of the trainings. Others continued with the medical treatment. During this period, the HPs came to measure the weight of the patients by using the weight scale. The patients may talked to the HPs through the nursing call system. The light was off at 23:00. During the night shift, the out of bed sensor and wet sensor were on to inform the relatives or HPs.
2.3 Design Phase in Denmark
The intelligent bed was tested both in homecare and district nursing home. Several workshops were held to enable the HPs discuss how to integrate the functions of the intelligent bed on the daily basis. Each workshop lasts from 1.5 to 3 h. The participants consisted of patients, HPs including occupational therapists, nurses, caregivers with researchers from the university and company engineers. The HPs were also invited to present their work content to better facilitate the understanding on their daily work routines. Due to the fact that not all the HPs have participated the workshop, we have trained the key users to operate the bed in the first 3 weeks. It has also given the opportunity for other HPs to be more familiar about the technology and better use the functions.
The functions of the intelligent bed tested in Denmark including: ergonomics movement control, brake not locked detector, bed in unsafe exit high position detector, bed rails in unsafe position detector, no power to the bed detector, out of bed detector, wet sensor, catheter bag detector, light support, and nursing call system. Most of the functions were identical comparing to the test in China. Minor changes were existed due to the differences of the test environment. Catheter bag detector was to inform the HPs when the level of urine in the bag required to be replaced (Fig. 3).

The design of the intelligent bed in Denmark
The intelligent bed was placed at the patients’ dwellings. The signals from the bed were sent to the server. The server then distributes the information accordingly. HPs can receive the data through their smart phones and computers. They then decide if it is in need of taking a visit to the patients in addition to the normal work routines. Company staff can monitor the status of the intelligent bed, provide technical assistance if it is necessary.
2.4 Implementation Phase in Denmark
Over 50 intelligent beds were tested in the Danish homecare and district nursing home. The beds were distributed to the patients who had various type of physical and mental disability. Most of the patients spent as long years as possible to stay at home and then moved into the district nursing home. The distance from the patients’ residence to the HPs’ office varies from approximately 100 m to maximum 20 km. Most of the work routines and the characteristics were similar to the classical homecare service or district nursing in Europe [6]. But the HPs can receive the alarms from the intelligent beds in their smart phones. There was a response team with 1–3 caregivers standing by equipped with cars when the alarm was sent from the distant intelligent bed.
2.5 Data Collection and Analysis
The overall design is inspired by the case study approach [7]. It facilitates to obtain a deep insight on how the intelligent bed has been implemented in pertinent within its unique context [8]. A process perspective is adopted for the researchers to understand how the intelligent bed has influenced consecutively, for instance, the working culture of the organization and the attitude of the individuals on the new technology. The data collection is built upon the chain of evidences including documentary study, participant observation and qualitative interviews.
The qualitative interview is to gain an insight of the users to cover different aspects on the implementation of the bed. It is operated as semi-structured and lasts for 1–1.5 h, depends on the content of the interview and if the respondents think it is fully recorded and well understood by the researchers. The transcribed data will then be sent to respondents for verification [9]. Participant observation is implemented through the whole trial including meetings, training workshops and the implementation of the intelligent bed [10]. The purpose is to acquire the basic knowledge of the care delivery process, the working culture, the attitudes of the users towards the new technologies and the internal relations within its context. Documentary study is applied to obtain a first impression on the basic societal knowledge and the local health care system [11]. The data will be analyzed with the software Nvivo 10.0. The analysis will follow the steps inspired by Kvale [28]: designing the code tree, refining, developing the topics based on the research questions, deriving the effects from the theories onto the topics. The data from participant observation will be applied to investigate how these wireless applications have been implemented during the test, for instance, how frequent a specific technology has been used and in what ways the healthcare professionals combine it with the treatment? It also helps the researchers to draw out the pattern of how the intelligent bed has been used, and try to identify the impact on the health care delivering process as well as the influence on the internal learning culture. Furthermore, the data from qualitative interview will be used to get the feedback from the different users of the technologies. It has also provided a unique chance to see how these new wireless technologies gradually change the working atmosphere, etc. inside the health institutions. At last, several perspectives obtained from the theories will bear in mind to better elucidate the research questions.
2.6 Theoretical Framework
The conceptual framework is grounded on the technology acceptance model, diffusion of innovation and technical transformation theory. The integration of the theories can bring more validity and reliability onto the research.
The Technology Acceptance Model helps to understand how the perceived usefulness and ease of use influence the adoption of the new technology [12]. The model helps to explain what elements will affect the willingness on using the new technology. Furthermore, it helps to elucidate how these individuals overcome the technical and organizational barriers in pertinent with better using the functions of the intelligent bed and delivering a more effective health care. This perspective can also help the researchers to understand how the application of the intelligent bed changes the values of the users on Telehealth and the overall health care service, and how these changing values reshape the design of the intelligent bed.
Diffusion of innovation is the theory about how, why and on what speed the new technology is disseminated across different social and cultural context [13]. The theory helps to understand how the users of the intelligent bed, especially the senior ones accept this new technology and gradually adapted it on the daily basis. It is also relevant to explain why the intelligent bed technology can or can not be integrated into the local context. By observing the process of the diffusion, this perspective can throw light upon how the unique local context affects the speed of disseminating this new wireless technology.
Technical transformation theory will also be introduced [14]. As a matter of fact, the intelligent bed technology is developed and manufactured in Denmark. This implies that the design of the functions as well as its purpose is heavily influenced by the Danish values towards its own health care system. Hence, a gap may exist due to the evidently cultural, social and economic differences between Denmark and China. This perspective help to identify what factors from these differences may affect the application of this wireless technology from Denmark into China, and examine the inter-relations among these factors. It also illuminates the researchers on how to successfully translate a new wireless technology from a developed country to a developing country.

New data processing algorithms
3 Results and Discussion
Figure 5 has illustrated how the new technology is accepted by the individuals or the organizations. The steps have been divided using a timeline to differential. Technical and social–cultural aspects have been included in the model. These two aspects affect the perceived effectiveness and usability of the users on a one way direction. Bearing with the pre-occupied perceptions, the trial use is proceeded but with a possibility of rejection. This situation may circles several times and eventually moves into the adoption of the technology. By accepting the new technology, both technical and social–cultural aspects of the individuals or the organizations are influenced in a feedback loop.
Table 1 has descripted the content of technical and social–cultural aspects when adapting a new Telehealth technology. It has explicitly illustrated the definition of the two aspects, given the example respectively. It can also be regarded as the expansion of the left part of Fig. 4.
This article has brought a new approach onto the effect evaluation of the intelligent bed. The spectrum was expanded into an interdisciplinary arena containing technical, social–cultural and economic aspects. The major strengths of this framework lies on: (1) including social–cultural aspects into the study and considering it as a major challenge in the implementation of new Telehealth technology, (2) involving the frontline users to decide which function of the intelligent bed to be tested as well as to assess the technology, (3) using different source of evidence to provide a comprehensive picture of implementation (Fig. 5).
The former theory on technology acceptance model is a general theory which lacks of focus on the Telehealth technology. The study has examined in detail on this area. By highlighting social–cultural aspects, the research has provided a new angle on the perspectives of individuals and organizations when introducing the new technology in different context. The necessity on this topic is supported by Ketikidis’s findings [15]. However, several issues have to be addressed. The first is the standardization of the definition on the aspects. Even though the article has provided some examples for interpreting the definitions, rigid and systematic variables are required. Certain connections among different variables are also relevant to be identified, either qualitative or quantitative. This is similar to Holden’s findings [16]. Some discussions on the choice of variables are already on the process, for instance, in Gagnon’s research, where they shows the critical importance of the organizational infrastructure [17]. It is argued that more concrete evidences are required, a more clear and systematic algorithm for identifying and weighting the variables are also in a great necessity.

New technology acceptance model with process perspective
In this study, the development of the new wireless technology has provided a new possibility to improve the health care quality and decrease the cost simultaneously. It may not always be promising as it is expected [18]. Sometimes this trend of spreading may be proved as a failure before it is commercialized. Hence, it requires more research on different perspectives as well as at different levels, which may help to facilitate the difficulty of implementing these new applications into the real context. From the former studies, it indicates that different users have different length of time to accept new technologies in terms of age, sexuality, etc [19]. But in most cases, the perceptions of users on the new health technologies are ignored by technical companies and policy makers. A misconception in these organizations are existed that the involvement of users will create too many target functions for the technologies to fulfill [3]. This point of view has limited the willingness of these organizations to include the users, especially the technical companies. Thereby, the suggestions from the users should be considered more than before for they are the individuals who are experiencing the real issues that the health technology is trying to solve [1]. Their opinions are also beneficial for the usability of the intelligent bed from a technical aspect in their respective context.
Unlike the traditional ways of diagnose and treatment, wireless technology has provided the Telehealth a possibility to be implemented distantly. This might has brought some disadvantages as stated in the Evans’s study that the applications of these new technology may decrease the face to face chances of the patients and healthcare professionals, and may had a negative effect on the patients’ treatment [20]. This concern is in pertinent with the technical aspects of the intelligent bed on how these wireless applications will be applied. Also, it might also has influenced on the clinical process of the health care institutions. Some arguments are also existed that these new wireless technologies will bring more benefits [21]. Other interesting opinions are like both the advantages and disadvantages brought by the technologies will be compromised when the healthcare professionals use it [22, 23]. The study hence provides a possibility to examine these arguments and tries to make discussions upon that, for instance, the different results might because of the types of the patients or the organizational culture, different settings of the political structure or maybe the pitfalls in the implementation of the project, etc. The result will be beneficial to the future design of the wireless applications on the new health care technology.
4 Conclusions
This paper has presented a new angle on the effect evaluation of the intelligent bed using wireless technology. It is critical to realize the importance of considering the local social–cultural and economic context as well as the technical infrastructures. A process perspective should bear in mind when adopting new technology. It is also important to involve all the stakeholders including patients, healthcare professionals and researchers, etc., as a good way to facilitate the process of accepting of the technology.
References
Kidholm, K., Ekeland, A. G., Jensen, L. K., Rasmussen, J., Pedersen, C. D., Bowes, A., et al. (2012). A model for assessment of telemedicine applications: Mast. International Journal of Technology Assessment in Health Care, 28(1), 44–51. doi:10.1017/S0266462311000638.
Bygholm, A., & Kanstrup, A. M. (2014). Learning from an Ambient Assisted Living Lab: The case of the intelligent bed. Studies in Health Technology and Informatics, 205, 318–322.
Kanstrup, A. M., & Bertelsen, P. (2011). User innovation management, a handbook. Aalborg: Aalborg University Press.
Saliba, V., Legido-Quigley, H., Hallik, R., Aaviksoo, A., Car, J., & McKee, M. (2012). Telemedicine across borders: A systematic review of factors that hinder or support implementation. International Journal of Medical Informatics, 81(12), 793–809. doi:10.1016/j.ijmedinf.2012.08.003.
Wootton, R. (2012). Twenty years of telemedicine in chronic disease management-an evidence synthesis. Journal of Telemedicine and Telecare, 18(4), 211–220. doi:10.1258/jtt.2012.120219.
World Health Organization. (2012). Home Care Across Europe, current structure and future challenges.
Yin, R. K. (2008). Case study research design and methods. London: SAGE.
Stake, R. E. (1995). The art of case study research. London: SAGE.
Rubin, H. J., & Rubin, I. S. (2011). Qualitative interviewing: The art of hearing data. London: SAGE.
Israel, A., Eng, E., Schulz, A. J., & Parker, E. A. (2012). Methods for community-based participatory research for health. San Francisco: Jossey-Bass.
Prior, L. (2003). Using documents in social research. London: SAGE.
Davis, F. D. (1989). Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Quarterly, 13(3), 319. doi:10.2307/249008.
Tidd, J., & Bessant, (2009). Managing innovation: Integrating technological, market and organizational change. London: Wiley.
Kuada, J. E. (2003). Culture and technological transformation in the South: Transfer or local innovation. Copenhagen: Samfundslitteratur.
Ketikidis, P., Dimitrovski, T., Lazuras, L., & Bath, P. A. (2012). Acceptance of health information technology in health professionals: An application of the revised technology acceptance model. Health Informatics Journal, 18(2), 124–134. doi:10.1177/1460458211435425.
Holden, R. J., & Karsh, B. T. (2010). The technology acceptance model: its past and its future in health care. Journal of Biomedical Informatics, 43(1), 159–172. doi:10.1016/j.jbi.2009.07.002.
Gagnon, M. P., Orruno, E., Asua, J., Abdeljelil, A. B., & Emparanza, J. (2012). Using a modified technology acceptance model to evaluate healthcare professionals’ adoption of a new telemonitoring system. Telemedicine and e-Health, 18(1), 54–59. doi:10.1089/tmj.2011.0066.
Sherer, S. A. (2010). Information systems and healthcare XXXIII: An institutional theory perspective on physician adoption of electronic health records. Communications of the Association for Information Systems, 26(7), 127.
Rogers, E. M. (2003). Diffusion of innovations. New York: Free Press.
Evans, H. H. (1993). High tech vs ‘high touch’: The impact of medical technology on patient care. In J. M. Clair, R. M. Allman (Eds.), Sociomedical perspectives on patient care (pp. 82–95). Lexington: The University Press of Kentucky.
Valero, M. A., Arredondo, M. T., Guillen, S., Traver, V., Fernandez, C., Basagoiti, I., et al. (2001). Impact of a broadband interactive televisit/teleconsultation service for residential and working environments. Proceedings of the AMIA Symposium, 721–725.
Kuszler, P. C. (1999). Telemedicine and integrated health care delivery: Compounding malpractice liability. American Journal of Law and Medicine, 25, 297–326.
Brigden, M., Minty, A., Pilatzke, S., Della, Vidov, L., Sherrington, L., et al. (2008). A survey of recipient client physician satisfaction with teleoncology services originating from thunder bay regional health sciences centre. Telemedicine and e-Health, 14(3), 250–254.
Kvale, S., & Brinkmann, S. (2008). Interviews: learning the craft of qualitative research interviewing (2nd ed.). Los Angeles: SAGE Publications Ltd.
Conflict of interest
No conflicted interests are existed in the research.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Cai, H., Toft, E. & Dinesen, B. A Conceptual Framework for the Effect Evaluation of the Intelligent Bed. Wireless Pers Commun 80, 1405–1414 (2015). https://doi.org/10.1007/s11277-014-2090-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11277-014-2090-7