
Abstract
Background
Our previous studies demonstrated that 2012 Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equations were inaccurate enough for estimating glomerular filtration rate in elderly Chinese. Thus, this study was constructed to modify these equations.
Methods
A total of 839 subjects (aged ≥60 years) from four hospitals in China between October 2009 and December 2014 were included. A random sample of 674 (80.3 %) subjects was used as a training sample set, and the remaining 165 (19.7 %) subjects as the verification set. The equations were modified using the hill-climbing algorithm.
Results
Compared with the original CKD-EPI equations, the accuracy assessment indexes (bias, precision, accuracy and misclassification) were obviously improved after modification. Bland–Altman analysis also demonstrated that this modification attempt gained success to some extent.
Conclusions
The modified 2012 CKD-EPI equations could be more accurate than the original equations for elderly Chinese individuals.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Chronic kidney disease (CKD) has been a major public health problem with an increasing prevalence [1, 2]. China also does not stay away from this global chronic disease. Timely and accurate evaluating renal function is important for the diagnosis of CKD. Glomerular filtration rate (GFR) has been regarded as the essential parameter of renal function. However, techniques, precisely measuring GFR, are complicated and expensive. Thus, equations based on renal biomarkers provide an available method for GFR evaluation (eGFR).
The simplified Modification of Diet in Renal Disease (MDRD) Study and the 2009 Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equations have been the most widely used methods for predicting eGFR in recent decades. These equations are based on serum creatinine (sCr). However, sCr concentration is influenced by several factors, including muscle mass, distal tubule secretion and inflammation [3]. The above influences tend to exist more often in the elderly. In addition, differences in race, physical fitness, diet and living habits also influence sCr [4]. What is more, previous studies indicated that none of the sCr-based equations predicted satisfactory eGFR in elderly Chinese [5, 6].
Kidney Disease: Improving Global Outcomes (KDIGO) 2012 Clinical Practice Guidelines for the Evaluation and Management of CKD recognized the limitations of sCr and then recommended additional confirmatory tests: serum cystatin C (sCys) and equations based on sCys (2012 CKD-EPI equations). However, our previous validation studies demonstrated that the 2012 CKD-EPIscr–cys equation was inaccurate for elderly CKD 3–5 stage patients, while the 2012 CKD-EPIcys equation performed no better than the other included equations [7].
According to the research background mentioned earlier, a modification study on the basis of 2012 CKD-EPI equations was subsequently conducted for elderly Chinese [8].
Methods
Subjects
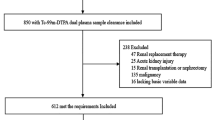
A total of 839 elderly Chinese subjects (aged 60 years and older) in clinic or hospitalized were included, from four hospitals in China between October 2009 and December 2014. The same inclusion and exclusion criteria were demanded in all participant hospitals. The inclusion was that subjects should be stable, or they were excluded, especially in these following conditions: acute renal failure, skeletal muscle atrophy, edema, ascites, pleural effusion, malnutrition, amputation, severe heart failure, ketoacidosis, use of cimetidine or trimethoprim, and patients who had ever received renal replacement therapy. The “stable” status meant that the outpatients had no condition changes, and the inpatients gradually recovering to discharge from hospital or ahead of operation.
Laboratory measurements
Identical research standard was requested in all the four hospitals to minimize inter-institutional variation. The researchers and staff underwent the same training. Subjects had to be fasting for 6 h before the examination. Blood samples were collected between 8:00 and 10:30 am, then centrifuged at 3000 rpm for 15 min, 1 h later and determined within 12 h.
Serum creatinine was determined using the isotope dilution mass spectrometry (IDMS) standardized enzymatic method (Kehua Dongling Diagnostic Products Co., Ltd, Shanghai, China) with a reported coefficient of variation of 6 %, reference range 44–136 umol/l, and traceable to National Institute of Standards and Technology creatinine standard reference material (SRM 967) [9]. Serum cystatin C was measured by particle-enhanced immunoturbidimetry (Leadman Biomedical Co., Ltd, Beijing, China) with a reported coefficient of variation of 8 % and reference range 0.60–1.55 mg/l, which was calibrated referring from the international certified reference material ERM-DA471.
GFR measurements
9mTc-DTPA (radiochemical purity 95–99 %) dynamic renal imaging was used to measure GFR (mGFR) [10]. Identical operational procedures were trained in all four hospitals. Subjects were demanded to avoid dehydration on the test day, drink 300–500 ml water in 30 min, empty their bladder and finally accept a bolus injection of 185 MBq 99mTc-DTPA in the elbow vein. Dynamic renal images were acquired on single-photon emission computed tomography (Gates method).
Mathematical algorithm modification
A total of 674 subjects were randomly selected as the training set, the remaining 165 subjects as the validation set. The hill-climbing algorithm was applied to modify the 2012 CKD-EPI equations with MATLAB software (version R2009a, Math Works Inc., USA). To search the optimal solution, each coefficient of the original equations was subsequently fixed and then iteratively adjusts the other coefficients until no further improvement was detected. Priority of the coefficients was repeatedly converted, to avoid inaccuracy caused by diverse weights of the coefficients.
Statistical analysis
All continuous variables were presented as mean ± SD. Bias was defined as the difference between eGFR and mGFR (eGFR–mGFR). The interquartile range (IQR) of the median difference was calculated as another assessment index. P 15 and P 30 were defined as the percentage of eGFR deviating within 15 % and 30 % of mGFR. The Bland–Altman plot analysis was also used to calculate the mean difference and precision between mGFR and eGFR. Crosstabs were used to understand the misclassification before and after modification. Root-mean-square error (RMSE) was also used to guide the modification process. All calculations and statistical analysis were performed with SPSS software (version 17.0; SPSS, Chicago, IL, USA) and MedCalc for Windows (version 11.6.1.0; MedCalc Software, Mariekerke, Belgium).
Results
Participant characteristics
A total of 839 subjects aged ≥60 years were recruited, including 525 men and 314 women. The age, sCr and sCys were 70.05 ± 7.19 years, 1.87 ± 1.75 mg/dl and 1.91 ± 1.09 mg/l, respectively. The mGFR was 51.88 ± 22.60 ml/min/1.73 m2. Detailed characteristics are listed in Table 1.
Performances of the modification
The equations before and after modification are described in Tables 2 and 3. Compared with the original equations, the modified CKD-EPIcys and CKD-EPIscr–cys equations were significantly improved in terms of bias, precision and accuracy (Table 4). Table 5 presents the misclassification before and after modification. The original misclassification in CKD 3–4 stages was obviously corrected after modification.
Bland–Altman analysis indicated that the accuracy of modified equations also achieved improvement. According to this assessment, the mean difference of CKD-EPIcys reduced from −7.6 ml/min/1.73 m2 to 0.8 ml/min/1.73 m2, and that of CKD-EPIscr–cys decreasing from −7.5 ml/min/1.73 m2 to 0.5 ml/min/1.73 m2. Meanwhile, deviation range of CKD-EPIcys narrowed from 49.12 ml/min/1.73 m2 to 45.10 ml/min/1.73 m2 and CKD-EPIscr–cys reducing from 49.28 ml/min/1.73 m2 to 43.50 ml/min/1.73 m2). None of the equations surpassed the tolerance line (<60 ml/min/1.73 m2) (Table 6; Fig. 1).

Bland–Altman plot of estimated GFR and reference GFR before and after modification (ml/min/1.73 m2). Horizontal solid line represents the bias of eGFR. Horizontal dashed line represents the 95 % confidence interval of standard deviation. Tilting dashed line represents the regression line of bias
Discussion
It is of necessity to accurately evaluate kidney function for elderly population. As known, 2012 CKD-EPI equations performed apparently superior to the former equations in general population [11]. However, our previous studies indicated the present GFR prediction equations, including the 2012 CKD-EPI equations predicted inaccurate for elderly Chinese population [7]. Taking P 30 (an accuracy index) as example, the K/DOQI guideline requires the acceptable level of P 30 should be beyond 70 % [12], whereas P 30 of the 2012 CKD-EPI equations in our previous validation study did not reach the criteria; the similar diagnostic results were also exited before modification in this study. Based on these facts, an improvement study was conducted.
Mathematical algorithms have powerful optimization capabilities. In 2013, we ever modified the 2009 CKD-EPI equation using mathematical algorithms and then gained desired results in the general Chinese population [8]. In the current study, the mathematical algorithm was also applied to modify the 2012 CKD-EPI equations and for the elderly Chinese. The hill-climbing method, one of mathematical algorithms, is a simple, greedy search algorithm. It iteratively searches a better solution by orderly changing one coefficient to the next. However, the hill-climbing algorithm sometimes falls into a local optimal solution, but not reaches the global optimal solution. Researchers overcome this limitation in combination with the simulated annealing algorithm. Considering that the original 2012 CKD-EPI equations have provided an optimal solution for the general population, it did not need to apply the simulated annealing algorithm. Therefore, the hill-climbing algorithm became the main modification tool for this study.
To avoid sampling error, the coefficients of the equations were adjusted three times with various random data. To be delighted, all the three solutions were similar, namely that the coefficients finally achieved optimal solution, on the view of mathematics. In addition, from the evidences of accuracy assessment, such as bias, P 30, RMSE and Bland–Altman analysis, this modification attempt improved the applicability of the equations, as well.
Exact CKD stage is essential to classify the risk stratification. CKD 3–4 stages are the vital important phase to protect the residual renal function. That is precisely what the advantage of the results was. Misclassification was obviously corrected in CKD 3–4 stages after modification.
Previous studies demonstrated that the equations combined with sCr and sCys were more accurate than the equations based on one marker [13]. Most of the reasons were the combination could reduce the influences with non-GFR determinants [11]. However, this study found the accuracy of CKD-EPIscr–cys equation was similar to the CKD-EPIcys equation. In a few aspects, the CKD-EPIcys equation even performed superior to the CKD-EPIscr–cys equation. Zhu et al. [7] ever also found that the CKD-EPIscr–cys equation performed substantially worse than the CKD-EPIcys equation. As far as we are concerned, the accuracy of an estimation equation is closely related to the basis renal function parameter, but to non-GFR determinants. Due to fewer influence factors [15, 16], sCys has been proved to be superior to sCr [17]. Our previous meta-analysis further proved the fact, as well [14]. Thus, an equation based on sCys alone might be more accurate and simpler. This assumption is our next step to be accomplished in the near future.
In conclusion, we developed a new modified 2012 CKD-EPI equations for elderly Chinese individuals. The new equations were similar to the original ones in forms, but more accurate. Extensive external validation was welcome to these new equations.
References
Stenvinkel P (2010) Chronic kidney disease: a public health priority and harbinger of premature cardiovascular disease. J Intern Med 268(5):456–467
Zhang L, Wang F, Wang L et al (2012) Prevalence of chronic kidney disease in China: a cross-sectional survey. Lancet 379(9818):815–822
Stevens LA, Padala S, Levey AS (2010) Advances in glomerular filtration rate-estimating equations. Curr Opin Nephrol Hypertens 19(3):298–307
Perrone RD, Madias NE, Levey AS (1992) Serum creatinine as an index of renal function: new insights into old concepts. Clin Chem 38(10):1933–1953
Liu X, Cheng MH, Shi CG et al (2012) Variability of glomerular filtration rate estimation equations in elderly Chinese patients with chronic kidney disease. Clin Interv Aging 7:409–415
Xun L, Cheng W, Hua T et al (2010) Assessing glomerular filtration rate (GFR) in elderly Chinese patients with chronic kidney disease (CKD): a comparison of various predictive equations. Arch Gerontol Geriatr 51(1):13–20
Zhu Y, Ye X, Zhu B et al (2014) Comparisons between the 2012 new CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration) equations and other four approved equations. PLoS One 9(1):e84688
Pei X, Yang W, Wang S et al (2013) Using mathematical algorithms to modify glomerular filtration rate estimation equations. PLoS One 8(3):e57852
Levey AS, Coresh J, Greene T et al (2007) Expressing the modification of diet in renal disease study equation for estimating glomerular filtration rate with standardized serum creatinine values. Clin Chem 53(4):766–772
Rehling M, Moller ML, Thamdrup B, Lund JO, Trap-Jensen J (1984) Simultaneous measurement of renal clearance and plasma clearance of 99mTc-labelled diethylenetriaminepenta-acetate, 51Cr-labelled ethylenediaminetetra-acetate and inulin in man. Clin Sci (Lond) 66(5):613–619
Inker LA, Schmid CH, Tighiouart H et al (2012) Estimating glomerular filtration rate from serum creatinine and cystatin C. N Engl J Med 367(1):20–29
National Kidney Foundation (2002) K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis 39(2 Suppl 1): S1–S266
Guo X, Qin Y, Zheng K et al (2014) Improved glomerular filtration rate estimation using new equations combined with standardized cystatin C and creatinine in Chinese adult chronic kidney disease patients. Clin Biochem 47(13–14):1220–1226
Wei L, Ye X, Pei X, Wu J, Zhao W (2014) Reference intervals for serum cystatin C and factors influencing cystatin C levels other than renal function in the elderly. PLoS One 9(1):e86066
Tangri N, Stevens LA, Schmid CH et al (2011) Changes in dietary protein intake has no effect on serum cystatin C levels independent of the glomerular filtration rate. Kidney Int 79(4):471–477
Vinge E, Lindergard B, Nilsson-Ehle P, Grubb A (1999) Relationships among serum cystatin C, serum creatinine, lean tissue mass and glomerular filtration rate in healthy adults. Scand J Clin Lab Investig 59(8):587–592
Inker LA, Astor BC, Fox CH et al (2014) KDOQI US commentary on the 2012 KDIGO clinical practice guideline for the evaluation and management of CKD. Am J Kidney Dis 63(5):713–735
Acknowledgments
This work was supported by the grants from the Major State Basic Research Development Program of China 2013CB530803, the National Natural Science Foundation of China H0511-81370843, the Chinese Medical Association of Clinical Medicine Research Special Funds 15020020590, the Innovation of Science and Technology Achievement Transformation Fund of Jiangsu Province BL2012066 and a Project Funded by the Priority Academic Program Development of Jiangsu Higher Education Institutions JX10231801.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
The study was approved by the ethics committee of The First Affiliated Hospital of Nanjing Medical University and conducted in accordance with the Declaration of Helsinki.
Additional information
Fen Li and Xiaohua Pei have contributed equally to this work.
Rights and permissions
About this article

Cite this article
Li, F., Pei, X., Ye, X. et al. Modification of the 2012 CKD-EPI equations for the elderly Chinese. Int Urol Nephrol 49, 467–473 (2017). https://doi.org/10.1007/s11255-016-1434-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-016-1434-5