
Abstract
Background
The recent guidelines recommend using the estimated glomerular filtration rate (eGFR) to evaluate renal function. There are two reported full-age-spectrum (FAS) equations in 2017, which are based on serum cystatin C concentrations with or without accompanying serum creatinine level (FASCr–Cys or FASCys). We compared the performance and assessed the applicability of the new FAS equation with the 2012 CKD-EPI (CKD-EPICys and CKD-EPICr–Cys) equation in Chinese subjects.
Methods
A total of 1184 patients, mean aged 55.06 year who underwent 99mTc-DTPA GFR measurements (rGFR) from four hospitals were enrolled. The bias (eGFR-rGFR), precision (interquartile range of difference [IQR]), and accuracy (the proportion of eGFR within 30% of rGFR [P30]) of eGFR and rGFR calculated by four equations were compared.
Results
Generally, the equation based on the combination of Cys and Scr performed superior to that on the basis of Cys alone, either the CKD-EPICr–Cys or the FASCr–Cys. Detailedly, referred to rGFR (67.33 ml/min/1.73 m2), the CKD-EPICys, CKD-EPICr–Cys, FASCys, and the FASCr–Cys estimated GFR 56.46 ml/min/1.73 m2, 62.79 ml/min/1.73 m2, 56.45 ml/min/1.73 m2, and 61.04 ml/min/1.73 m2, gave ROCAUC0.944, 0.954, 0.943, and 0.953, respectively. Another comparison as to bias, precision, P30, and RMSE with FASCr–Cys were − 2.87 ml/min/1.73 m2, 19.01 ml/min/1.73 m2, 74.16%, and 17.84 ml/min/1.73 m2 showed that FASCr–Cys performed approximately more accurate than other equations, as well as the diagnostic consistency of GFR staging. In the rGFR < 60 ml/min/1.73 m2 subgroup, the FASCr–Cys equation showed the best performance. In older subjects, compared with FASCys, CKD-EPICr–Cys, and CKD-EPICys, the FASCr–Cys equation had relatively less bias (− 8.09 vs. − 9.63, − 7.52, − 11.04, P < 0.05), most precise (15.18 vs. 16.32, 15.22, 16.63), and most accuracy, P30 was statistically different from the other equations, and achieved a ideal value > 70%.
Conclusion
The performance of the FASCr–Cys equation is better than that of the CKD-EPICr–Cys equation in the Chinese population, particularly in the elderly. Yet, further modification of FAS equations from a large-scale study could be more suitable for the Chinese population, particularly in older people.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Chronic kidney disease (CKD) has been recognized as a public health problem worldwide [1,2,3]. In China, the 2012 epidemiological survey showed that the prevalence of CKD is 10.8%, that means there are more than 120 million CKD patients [4]. Accurately estimating glomerular filtration rate (GFR) is essential to CKD diagnosis, drug dose adjustment, and prognosis prediction [5,6,7]. Isotope double plasma method has been recommended by the American Nuclear Medical Association as a standard way for GFR determination. However, this method needs twice blood sampling and complicated procedures. To reserve the advantage of isotope method and simplify the steps, 99mTc-DTPA renal dynamic imaging (RDI) occurred. The RDI method shows the image of each kidney isotope metabolism, and is also easily repeated again [8, 9]. Some researchers reported that RDI method can reflect renal function as well as the double plasma method [10]. However, the expensive, radioactive, and invasive disadvantages limit their clinical application.
GFR estimation equations, simulated from the isotope methods, have been recommended to predict GFR as the first choice [11,12,13,14]. The equations are always based on serum creatinine (Scr) and/or serum cystatin C (Cys). Among these equations, the 2012 CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration) equation performed better, especially the CKD-EPICr–Cys [15,16,17]. Our previous studies also demonstrated that the CKD-EPICr–Cys equation performed more accurate than CKD-EPICr equation and CKD-EPICys equation in Chinese subjects [18, 19].
Newly, Pottel et al. developed a full-age-spectrum (FAS) equation for assessing GFR, based on European healthy subjects with a novel modeling approach in 2017 [20]. The principle of the modeling is that GFR is negatively correlated with the normalized Scr (QCr) and Scys (QCys) (Q value was regarded as the mean or median of Scr and Cys levels, corresponding to the age/gender of the healthy population). Thus, the standard Q value was endowed with age and gender characteristics. Due to this merit, age, gender, and other parameters to estimate GFR are no longer needed. The FAS equation gets simpler. Not only that, external validation studies demonstrated the FAS equation performed superior to the CKD-EPI equations both in the European population and Caucasian participants. In addition, a meta-analysis based on a healthy Caucasian population found that the average GFR was 107 ml/min/1.73 m2 before 40 years, and the GFR began to decline after 40 years, which support the theoretical basis for the development of the FAS equations [21].
Whether the applicability of the newly developed full-age equations in China is better, and whether it is more accurate than the 2012 CKD-EPI equations have not yet been verified. Thus, the goals of this study was to investigate the adaptability of the 2017 new FAS equations and compare its performance with 2012 CKD-EPI equations of the Chinese multi-center cohort.
Methods
Participants’ characteristics
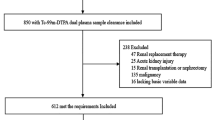
We performed a multi-center, retrospective study from October 2009 to December 2016. The participants were recruited from four various hospitals: the First Affiliated Hospital of Nanjing Medical University, the Third Affiliated Hospital of Sun Yat-sen University, the Affiliated Wuxi No. 2 Hospital of Nanjing Medical University, and the Fourth Hospital of Jilin University. All four hospitals had the same inclusion and exclusion criteria. The inclusion was that subjects should be stable with referenced GFR (rGFR), Scr, and Scys analysis. (The “stable” status meant that the outpatients had no condition changes, including healthy population and the inpatients gradually recovering to discharge from hospital or ahead of operation) The participants with severe heart failure, acute renal failure, pleural or abdominal effusion, serious edema or malnutrition, skeletal muscle atrophy, amputation, ketoacidosis should be excluded. Patients who were taking trimethoprim, cimetidine, or ACEI/ARB and those who had recently received glucocorticoid and hemodialysis therapy had to be excluded.
Laboratory assay
Identical research standard was requested in all the four hospitals to minimize inter-institutional variation. Researchers and staffs underwent the same training. Blood fasting samples were drawn between 8:00 and 10:30 a.m., then centrifuged at 3000 rpm for 15 min and detected within 12 h. Scr was determined using the isotope dilution mass spectrometry (IDMS) and standardized enzymatic method (Kehua Dongling Diagnostic Products Co., Ltd., Shanghai, China) with a reported coefficient of variation of 6% (reference range: 44-136 µmol/l), and traceable to National Institute of Standards and Technology creatinine standard reference material (SRM 967) [12]. Cys was measured by particle-enhanced immunoturbidimetry (Leadman Biomedical Co., Ltd., Beijing, China) with a reported coefficient of variation of 8% (reference range: 0.60–1.55 mg/l), which was calibrated referring from the international certified reference material ERM-DA471.
rGFR measurements
The 99mTc-DTPA (radiochemical purity 95–99%) RDI was taken as referenced GFR (rGFR). Identical operational procedures were trained in all four hospitals. Subjects were demanded to avoid dehydration on the test day, drink 300–500 ml water in 30 min, empty their bladder, and finally accept a bolus injection of 185 MBq 99mTc-DTPA in the elbow vein. Dynamic renal images were acquired on single-photon emission computed tomography (Gates method).
GFR equations expression
The detailed expressions of the 2012 CKD-EPI and 2017 FAS equations are presented in Table 1.
Statistical analysis
All continuous variables were expressed as mean ± standard deviation (SD). Bias was calculated as the median difference between eGFR and rGFR (eGFR-rGFR). Precision was expressed as the inter-quartile range (IQR) of the median difference. P30was defined as the percentage of eGFR deviating within 30% of rGFR. The Bland–Altman plot analysis was also used to calculate the mean difference and precision between eGFR and rGFR. All calculations and statistical analysis were done with SPSS software (version 17.0; SPSS, Chicago, IL, USA) and MedCalc for Windows (version 11.6.1.0; MedCalc Software, Mariekerke, Belgium).
Results
Basic characteristics of the subjects
Altogether 1184 subjects (median age 55.06 ± 16.32 years) were enrolled in this study, including 671 males and 513 females. The average values of Cys, Scr, and rGFR were 1.73 ± 1.17 mg/l, 1.80 ± 1.92 mg/dl, and 65.29 ± 30.27 ml/min/1.73 m2 (Table 2).
Performance of the 2012 CKD-EPI equation and 2017 FAS equation
Generally, the equation based on the combination of Cys and Scr performed superior to that on the basis of Cys alone (Table 2), either the CKD-EPICr–Cys or the FASCr–Cys. In addition, the diagnostic value analysis results and Bland–Altman plots also indicated the similar conclusion: equations combined with both Cys and Scr predicted more accurate eGFR than that based on solo Cys (Table 3; Fig. 1). The FASCr–Cys equation predicted similar eGFR with the CKD-EPICr–Cys equation.

Comparison between estimated glomerular filtration rate (eGFR) and referenced GFR (rGFR). a, b Serum cystatin C-based chronic kidney disease epidemiology collaboration (CKD-EPICys) equation; c, d serum creatinine- and cystatin C-based chronic kidney disease epidemiology collaboration (CKD-EPICr–Cys) equation; e, f serum cystatin C-based full-age-spectrum (FASCys) equation; g, h serum creatinine- and cystatin C-based full-age-spectrum (FASCr–Cys) equation. The gray line in the scatter plot represents the identical line. Solid and dashed black lines in the Bland–Altman plot represent the mean and 95% limits of agreement (LoA) of bias, respectively
Detailedly, referred to rGFR (67.33 ml/min/1.73 m2), the CKD-EPICys, CKD-EPICr–Cys, FASCys, and the FASCr–Cys-estimated GFR 56.46 ml/min/1.73 m2, 62.79 ml/min/1.73 m2, 56.45 ml/min/1.73 m2, and 61.04 ml/min/1.73 m2 (Table 2), gave ROCAUC0.944, 0.954, 0.943, and 0.953 (Table 3), respectively. Another comparison as to bias, precision, P30, and RMSE with FASCr–Cys were − 2.87 ml/min/1.73 m2, 19.01 ml/min/1.73 m2, 74.16%, and 17.84 ml/min/1.73 m2, which showed that FASCr–Cys performed approximately more accurate than other equations, as well as the diagnostic consistency of GFR staging (Tables 4, 5).
Performance of the four equations in subgroups
Another, in the case of the ability to predict accuracy in various GFR stages and age groups, the CKD-EPICr–Cys equation and FASCr–Cys equation also performed lower bias, higher IQR, and accuracy than CKD-EPICys equation and FASCys equation.
In subgroups with rGFR≥60 ml/min/1.73 m2, the CKD-EPICr–Cys equation showed the lowest bias, and the highest IQR, accuracy (P30 reached 84.91%, RMSE was 18.80). The FASCr–Cys performed slightly inferior to the CKD-EPICr–Cys, but it did not achieve statistical significance. The FASCys equation and CKD-EPICys performance were worse than the two combined equation. In the group with rGFR < 60 ml/min/1.73 m2, compared with the other three equations, the FASCr–Cys equation showed the lowest bias, the highest precision, and the highest accuracy. However, the P30 of all four equation all did not reach 70% (Table 4).
In the young group, the CKD-EPICr–Cys had the lowest bias and RMSE, and the results had the significance with the other three equations. The FASCr–Cys equation had the highest P30, but with no significance from other three equations. The P30 of all four equations reached 70% in this group. In the subgroup with age ≥ 60 years old, FASCr–Cys equation had relatively lower bias, highest precision, and accuracy and its P30 was 70.37%. The P30 of other three equations did not reach 70% (Table 4).
Discussion
Our previous study demonstrated that neither of the 2012 CKD-EPI equations achieved an ideal accuracy in aging cohorts with moderately severely impaired GFR [18, 19]. Thus, we wonder whether the adaptability of the newly FAS equations in Chinese participants is better and whether their performance is more accurate than the 2012 CKD-EPI equations. The main finding of this study was that the FASCr–Cys equation had the best diagnostic accuracy in the whole subjects, particularly in older patients with moderately severely injured GFR. However, the CKD-EPICr–Cys had a better diagnostic consistency of GFR stage between the eGFR and rGFR. While in young participants with normal or mildly injured GFR, the CKD-EPICr–Cys performed better than others.
Up to now, a higher prevalence of CKD in older patients as the mean age of the general population is rising, which has paid enough notice worldwide. Accurately assessing GFR is indispensable for detection and staging of CKD, especially in older subjects [22,23,24,25]. Recently, a clinical practice guideline focused on the management of older patients with chronic kidney disease stage 3b or higher draws our attention much. The guideline recommended using estimating equations to assess renal function. However, there is not any sufficient evidence to prefer one equation over another, although it suggested the use of CKD-EPICr–Cys may be an acceptable alternative [12]. In this article, we found the CKD-EPICr–Cys was not the best equation in the elderly. Moreover, the accuracy of the FASCr–Cys equation performed better in Chinese.
Meanwhile, we found the performance of the CKD-EPICr–Cys equation and the FASCr–Cys equation was superior to the CKD-EPICys equation and the FASCys equation. Stevens et al. [26] found that in CKD patients, the equations of combined Scr, Cys with age, sex, and race performed better than equations that used Scr or Cys alone. The development of CKD-EPI equation also found that the equation in combination of Cys with Scr was more accurate than the one using single marker-based equation alone. The reason for considering the use of the two markers in combination compared with the equation using one marker alone, the errors caused by the non-GFR determinant of Scr and Cys are independent and smaller.
The development of 2012 CKD-EPI equations is based on the characteristics of its development population, which set up the mean value of rGFR as 120–130 ml/min/1.73 m2, and it is thought that the GFR decreases from the early stage with age [11]. This is different from the theory that the FAS equation with 107 ml/min/1.73 m2 as the mean value, and GFR begins to decline with age after 40 years [20]. In this study, the FASCr–Cys equation is found to be the best in Chinese, and the deviation, precision, and accuracy are the best. The CKD-EPICr–Cys equation is similar to the FASCys equation, which is second to the FASCr–Cys equation. It is suggested that the mean value of FAS equation is more accurate than CKD-EPI equation, and the equations of the combination of Scr and Cys are superior to the single Cys equations.
This article shows that the applicability of the FASCys equation, 2012 CKD-EPI equations in the group with GFR < 60 ml/min/1.73 m2 was not ideal (the P30 values were less than 70%). In the group with age ≥ 60 years old, FASCr–Cys equation performed better than the other three equations. At the same time, with the increase of age, the GFR declined and the accuracy of the evaluated equation is reduced, which has considered the age factor; FAS equations also exist in this phenomenon. Considering the following reasons for interpretation of this phenomenon, on the one hand, the development of QCr and QCys values was matched with healthy population; however, the age span is too large (divided into < 18 years old, 18–70 years old, 70 years old). In 18–70 years old group, the levels of Scr and Cys increased with age may have a greater difference. On the other hand, the mean GFR of Chinese population which matched the age/gender of healthy population was different from white people. Ma et al. [27] found the mean GFR measured with 99mTc-DTPA in the Chinese healthy population with age under 50 years as follows: male was 104 ml/min/1.73 m2, female was 110.1 ml/min/1.73 m2. And with age above 60 years, the mean GFR was 76.1 ml/min/1.73 m2, which was lower than the mean of GFR in the Western population.
Over the last decades, the equations were mostly based on the elimination of exogenous markers or the clearance of Scr (as “gold standard”), and then a statistic method was used to develop a highly fitting equation with the “gold standard.” The FAS equation calibrates the Scr/Cys with the mean value of the healthy population matched by age/sex, which avoids the difference between the inclusion of the population and the measure methods of the “gold standard.”
However, FAS equations also had some limitations. Firstly, the method of GFR measurement is inconsistent, and the average GFR of the healthy people of < 40 years old as a constant has error. Secondly, the Q value of the healthy population is the average of the age/sex matched with healthy white people, and there are differences in other races. Thirdly, the larger age span could result in reducing accuracy of standardized Q value.
These results suggest that the QCr, QCys, and the mean values of rGFR in the more detailed age group are expected to further improve the accuracy of the FAS equation in the Chinese population if the relevant data of the multi-center healthy population in China are collected.
Conclusion
Compared with 2012 CKD-EPI equations, the development principles and models of FAS equation are more reasonable, more accurate, and simpler. However, racial differences limit the accuracy of the equation as its development population was being white. On the basis of the theory of the equation, the development of FAS equation suitable for the Chinese population is supposed to be more accurate.
References
Murphy D, McCulloch CE, Lin F et al (2016) Trends in prevalence of chronic kidney disease in united states. Ann Intern Med 165(7):473–481
deBoer IH (2012) Chronic kidney disease—a challenge for all ages. JAMA 308(22):2401–2402
Stevens LA, Coresh J, Levey AS (2008) CKD in the elderly—old questions and new challenges. Am J Kidney Dis 51(3):353–357
Zhang L, Wang F, Wang L et al (2012) Prevalence of chronic kidney disease in China: a cross-sectional survey. Lancet 379(9818):815–822
Levey AS, Inker LA, Coresh J (2014) GFR estimation: from physiology to public health. Am J Kidney Dis 63:820–834
Levey AS, Becker C, Inker LA (2015) Glomerular filtration rate and albuminuria for detection and staging of acute and chronic kidney disease in adults: a systematic review. JAMA 313(8):837–846
Soveri I, Berg UB, Bjork J et al (2014) Measuring GFR: a systematic review. Am J Kidney Dis 64:411–424
Delpassand ES, Homayoon K, Madden T et al (2000) Determination of glomerular filtration rate using a dual-detectorgamma camera and the geometric mean of renal activity: correlation with the Tc-99m DTPA plasma clearance method. Clin Nucl Med 25(4):258–262
Orsal E, Seben B, Subasi ID et al (2013) Vesicoureteral refluxin a nonfunctioning kidney detected by 99mTc-DTPA study. Jpn J Radiol 31(12):823–825
Amin A, El-Sayed S, Taher N et al (2012) Tc-99m diethylenetriamine pentaacetic acid (DTPA) renal function reserve estimation: is it a reliable predictive tool for assessment of preclinical renal involvement in scleroderma patients. Clin Rheumatol 31:961–966
Inker LA, Schmid CH, Tighiouart H et al (2012) Estimating glomerular fltration rate from serum creatinine and cystatin C. N Engl J Med 367(1):20–29
Farrington K, Covic A, Aucella F et al (2016) Clinical practice guideline on management of older patients with chronic kidney disease stage 3b or higher (eGFR < 45 ml/min/1.73 m2). Nephrol Dial Transplant 31(suppl 2):ii1–ii66
Fan L, Inker LA, Rossert J et al (2014) Glomerular filtration rate estimation using cystatin C alone or combined with creatinine as a cofirmatory test. Nephrol Dial Transplant 29:1195–1203
Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group (2013) KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl 3:1–150
Fan L, Levey AS, Gudnason V et al (2015) Comparing GFR estimating equations using cystatin C and creatinine in elderly individuals. J Am Soc Nephrol 26(8):982–1989
Kong X, Ma Y, Chen J et al (2013) Evaluation of the Chronic Kidney Disease Epidemiology Collaboration equation for estimating glomerular filtration rate in the Chinese population. Nephrol Dial Transplant 28(3):641–651
Barr EL, Maple-Brown LJ, Barzi F et al (2017) Comparison of creatinine and cystatin C based eGFR in the estimation of glomerular filtration rate in Indigenous Australians: the eGFR Study. Clin Biochem 50(6):301–308
Zhu Y, Ye XS, Zhu B et al (2014) Comparisons between the 2012 New CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration) equations and other four approved equations. PLoS ONE 9(1):e84688
Li F, Pei XH, Ye XS et al (2017) Modification of the 2012 CKD-EPI equations for the elderly Chinese. Int Urol Nephrol 49(3):467–473
Pottel H, Delanaye P, Schaeffner E et al (2017) Estimating glomerular filtration rate for the full age spectrum from serum creatinine and cystatin C. Nephrol Dial Transplant 32(3):497–507
Pottel H, Hoste L, Yayo E et al (2017) Glomerular filtration rate in healthy living potential kidney donors: a meta-analysis supporting the construction of the full age spectrum equation. Nephron 135(2):105–119
Kilbride HS, Stevens PE, Eaglestone G et al (2013) Accuracy of the MDRD (modification of diet in renal disease) study and CKD-EPI (CKD epidemiology collaboration) equations for estimation of GFR in the elderly. Am J Kidney Dis 61:57–66
Alshaer IM, Kilbride HS, Stevens PE et al (2014) External validation of the Berlin equations for estimation of GFR in the elderly. Am J Kidney Dis 63:862–865
Vidal-Petiot E, Haymann JP, Letavernier E et al (2014) External validation of the BIS (Berlin initiative study)-1 GFR estimating equation in the elderly. Am J Kidney Dis 63:865–867
Schaeffner ES, Ebert N, Delanaye P et al (2012) Two novel equations to estimate kidney function in persons aged 70 years or older. Ann Intern Med 157:471–481
Stevens LA, Coresh J, Schmid CH et al (2008) Estimating GFR using serum cystatin C alone and in combination with serum creatinine: a pooled analysis of 3418 individuals with CKD. Am J Kidney Dis 51(3):395–406
Ma YC, Zuo L, Chen L et al (2010) Distribution of measured GFR in apparently healthy Chinese adults. Am J Kidney Dis 56(2):420–421
Acknowledgements
This work was supported by the grants from the National Natural Science Foundation of China H0511-81670677, Clinical Medicine Research Special Funds of Chinese Medical Association 15020020590, Jiangsu Provincial Key Discipline of Medicine ZDXKA2016003, Jiangsu Provincial Key Laboratory of Geriatrics, Jiangsu Province’s Key Medical Talents Program ZDRCA2016021, Jiangsu Province 333 Project BRA2017409, Jiangsu Province’s Key Medical Young Talents Program QNRC2016592, and Jiangsu cadres health care research BJ16016, BJ17018.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
The study was approved by the ethics committee of the First Affiliated Hospital of Nanjing Medical University and conducted in accordance with the Declaration of Helsinki.
Rights and permissions
About this article

Cite this article
Yong, Z., Li, F., Pei, X. et al. A comparison between 2017 FAS and 2012 CKD-EPI equations: a multi-center validation study in Chinese adult population. Int Urol Nephrol 51, 139–146 (2019). https://doi.org/10.1007/s11255-018-1997-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-018-1997-4