
Abstract
Objective
To verify whether the new Asian modified CKD-EPI equation improved the performance of original one in determining GFR in Chinese patients with CKD.
Method
A well-designed paired cohort was set up. Measured GFR (mGFR) was the result of 99mTc-diethylene triamine pentaacetic acid (99mTc-DTPA) dual plasma sample clearance method. The estimated GFR (eGFR) was the result of the CKD-EPI equation (eGFR1) and the new Asian modified CKD-EPI equation (eGFR2). The comparisons were performed to evaluate the superiority of the eGFR2 in bias, accuracy, precision, concordance correlation coefficient and the slope of regression equation and measure agreement.
Results
A total of 195 patients were enrolled and analyzed. The new Asian modified CKD-EPI equation improved the performance of the original one in bias and accuracy. However, nearly identical performance was observed in the respect of precision, concordance correlation coefficient, slope of eGFR against mGFR and 95 % limit of agreement. In the subgroup of GFR < 60 mL min−1/1.73 m2, the bias of eGFR1 was less than eGFR2 but they have comparable precision and accuracy. In the subgroup of GFR > 60 mL min−1/1.73 m2, eGFR2 performed better than eGFR1 in terms of bias and accuracy.
Conclusion
The new Asian modified CKD-EPI equation can lead to more accurate GFR estimation in Chinese patients with CKD in general practice, especially in the higher GFR group.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Chronic kidney disease (CKD) has been a worldwide problem because of the high prevalence and severe financial burden [1–5]. Glomerular filtration rate (GFR) is an important index of kidney function in the diagnosis, staging, evaluation of therapeutic effect and prognosis prediction [6–9]. The most accurate method to determine GFR is inulin clearance rate, but it is not applied widely in clinical practice due to the time-consuming and cumbersome proceeding. Several available methods were developed to estimate GFR with the advantage of simplicity and low cost [10–17]. It is widely believed that the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation is the most accurate and recommended method based on serum creatinine [18–23]; however, the equation only considered Blacks and others. Creatinine generation differs among racial-ethnic groups, so the researchers developed a new CKD-EPI equation that includes a four-level race variable (Black, Asian, Native American and Hispanic and others) [24]. We hypothesized that it requires more studies to verify whether the new equation improved the performance of original one in determining GFR in Chinese patients with CKD. Here, a well-designed paired cohort was set up in this study to assess the applicability of new Asian modified CKD-EPI equation comparing with the original one.
Subjects and methods
Ethics statement
The study protocol was approved by Hebei Medical University ethical committee. All the participants provided written informed consent for this research.
Patients
The diagnosis of CKD and the exclusion criteria was same with our study published in 2012 [25]. Data collected from each patient’s included height, weight, age, sex, the volume of 24-h urine, serum urea nitrogen, the causes of CKD and CKD stages.
Measurement of GFR by dual plasma sample clearance method (mGFR)
The results of 99mTc-diethylene triamine pentaacetic acid (99mTc-DTPA) dual plasma sample clearance method were considered as the measured GFR in this study. The detailed operating procedures of 99mTc-DTPA dual plasma sample clearance method were described previously [25], which was estimated from a single exponential formula derived from the blood samples between 2 and 4 h after injection. The mGFR (mL min−1) was normalized for a body surface area of 1.73 m2 according to Haycock’s equation [26].
The measurement of serum creatinine
Serum creatinine (Sc) level was measured by the enzymatic method on an automatic biochemical analyzer (VITROS 5.1, Johnson Company, USA). And the results of Sc were recalibrated with isotope dilution mass spectrometry.
The estimated GFR determined by original CKD-EPI equation (eGFR1)
The CKD-EPI equation is as follows [11]:
Female with the concentration of serum creatinine ≤0.7 mg dL−1,
Female with the concentration of serum creatinine >0.7 mg dL−1,
Male with the concentration of serum creatinine ≤0.9 mg dL−1,
Male with the concentration of serum creatinine >0.9 mg dL−1,
The unit of Scr and age is mg dL−1 and year, respectively.
The estimated GFR determined by new Asian modified CKD-EPI equation (eGFR2)
The new Asian CKD-EPI equation is as follows [11]: Female with the concentration of serum creatinine ≤0.7 mg dL−1,
Female with the concentration of serum creatinine >0.7 mg dL−1,
Male with the concentration of serum creatinine ≤0.9 mg dL−1,
Male with the concentration of serum creatinine >0.9 mg dL−1,
The unit of Scr and age is mg dL−1 and year, respectively.
Statistical analysis
The performance of eGFR1 and eGFR2 was assessed by the comparisons of bias, accuracy, precision, concordance correlation coefficient and the slope of regression equation, and a Bland–Altman analysis to measure agreement. The bias was defined as mGFR minus eGFR. The precision was inferred from the standard deviation of bias. The accuracy was calculated as the percentage of eGFR within 30 % deviation of mGFR. The concordance correlation coefficient and the slope of regression equation were calculated by means of Passing–Bablok regression and Lin correlation. Paired T test, F test and McNemar test were applied for comparing bias, precision and accuracy, respectively. All Statistical analyses were performed using SPSS (version 17.0, SPSS. Chicago IL, USA) and Medcalc (version 4.3, Medcalc software, Mariekerke, Belgium).
Results
During the study frame, a total of 195 CKD patients aged 21–83 years (mean age 55.46 ± 15.36 years, 52.30 % women) were enrolled and analyzed. The clinical characteristics of the patients are presented in Table 1. The causes of CKD were chronic glomerulonephritis 37.44 % (73/195), diabetic nephropathy 24.62 % (48/195), chronic pyelonephritis 14.36 % (28/195), hypertensive nephropathy 11.28 % (22/195), chronic interstitial nephritis 4.62 % (9/195), IGA nephropathy 3.08 % (6/195), polycystic kidney disease 3.08 % (6/195) and others 1.54 % (3/195). The prevalence of CKD stage 1, 2, 3, 4 and 5 was 20.51, 24.62, 23.08, 20.00 and 11.79 % according to mGFR, respectively. The mean (± SD) value of mGFR was 63.42 ± 38.25 mL min−1/1.73 m2, and the mean (± SD) eGFR by the original CKD-EPI equation was 59.97 ± 32.76 mL min−1/1.73 m2 and 63.21 ± 34.57 mL min−1/1.73 m2 by the new one. The difference between mGFR and eGFR1 or eGFR2 was not significant (all P > 0.05).
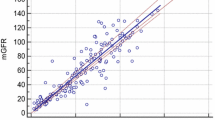
The comparison between eGFR1 and eGFR2 is presented in Table 2. In terms of both bias and accuracy, the new Asian CKD-EPI equation achieved more preferable results in estimating GFR (bias, 3.45 for eGFR1 vs. 0.21 mL min−1/1.73 m2 for eGFR2, t = 22.84, P < 0.001; 30 % accuracy, 74.36 % for eGFR1 vs. 78.46 %, P = 0.021). However, there was nearly identical performance of eGFR1 and eGFR2 in respect of precision, concordance correlation coefficient, slope of eGFR against mGFR and 95 % limit of agreement (Figs. 1, 2).

Bland–Altman plots showing the disagreement between eGFR1 and mGFR. The solid long line indicates the mean of difference and the dotted long line represents the 95 % limits of agreement (2sd). eGFR1 estimated glomerular filtration rate by the original CKD-EPI equation, mGFR glomerular filtration rate determined by 99mTc-DTPA dual plasma sample clearance method

Bland–Altman plots showing the disagreement between eGFR2 and mGFR. The solid long line indicates the mean of difference and the dotted long line represents the 95 % limits of agreement (2sd). eGFR2 estimated glomerular filtration rate by the new Asian modified CKD-EPI equation, mGFR glomerular filtration rate determined by 99mTc-DTPA dual plasma sample clearance method
In the subgroup of GFR < 60 mL min−1/1.73 m2 (n = 96), the bias of eGFR1 was less than eGFR2 (−4.36 vs. −6.23 mL min−1/1.73 m2, t = 14.559, P < 0.001) but they have comparable identical precision and accuracy (all P > 0.05). In the subgroup of GFR > 60 mL min−1/1.73 m2 (n = 99), eGFR1 was more preferable in bias and accuracy (bias, 11.03 for eGFR1 vs. 6.47 mL min−1/1.73 m2 for eGFR2, t = 28.017, P < 0.001; 30 % accuracy, 81.82 % for eGFR1 vs. 89.90 %, P = 0.008).
Discussion
It is widely believed that the CDK-EPI equation is a satisfactory and simple method to determine the GFR [18–23]. Unfortunately, only a two-level racial variable (Black vs. White and other) was utilized when the CDK-EPI equation was developed in 2009 [13]. It is proposed that the creatinine generation varies with racial, ethnic and geographic group due to muscle and diet, which is neglected by the CDK-EPI equation developers [27, 28]. The Asians (including Chinese) have less muscle mass, and lower dietary can lead to less creatinine generation. So Stevens et al. captured pooled data from ten studies (N = 8254) and developed a new four-level race variable (Black, Asian, Native American and Hispanic, and White and others) CKD-EPI equation with urinary clearance of iothalamate as the reference method. Nevertheless, only 100 Asian samples with or without kidney diseases were included. It is necessary to evaluate whether the new Asian modified CDK-EPI equation is definitely more accurate than the original one in calculating GFR in Chinese patients with CKD.
99mTc-DTPA dual plasma sample clearance method was employed as the reference method to measure GFR which guaranteed the dependability of the results in this study. Totally, 195 Chinese patients with CKD were enrolled in our study, and the results of comparison between the new Asian modified CDK-EPI equation and the original one showed that the latter one achieved less bias and greater accuracy. However, the two equations resembled each other in precision, concordance correlation coefficient, slope of eGFR against mGFR and 95 % limit of agreement. All the performance above revealed new Asian modified CDK-EPI equation was more accurate than the original one. These results were consistent with the previous findings derived from validation data set [24]. Specifically, the advantage of the new Asian modified CDK-EPI was mainly reflected in the higher GFR group.
It can be noted that there are several limitations. First, the sample size in this study was relatively small, so it is difficult to make detailed analysis according to different stages. Moreover, the included samples were all CKD patients, so more research is needed to extend the application range of new Asian modified CDK-EPI equation.
In conclusion, we confirmed that the new Asian modified CKD-EPI equation improves the performance of GFR estimation, and it should be the foremost choice in determining GFR in Chinese patients with CKD, especially in the higher GFR group.
References
Levey AS, Atkins R, Coresh J, Cohen EP, Collins AJ, Eckardt KU et al (2007) Chronic kidney disease as a global public health problem: approaches and initiatives—a position statement from kidney disease improving global outcomes. Kidney Int 72:247–259
Kim NH, Hyun YY, Lee KB, Chang Y, Ryu S et al (2015) Environmental heavy metal exposure and chronic kidney disease in the general population. J Korean Med Sci 30(3):272–277
Zhang Q-L, Rothenbacher D (2008) Prevalence of chronic kidney disease in population-based studies: systematic review. BMC Public Health 8:117
Kaze FF, Meto DT, Halle MP, Ngogang J, Kengne AP (2015) Prevalence and determinants of chronic kidney disease in rural and urban Cameroonians: a cross-sectional study. BMC Nephrol 30(16):117
Jessani S, Bux R, Jafar TH (2014) Prevalence, determinants, and management of chronic kidney disease in Karachi, Pakistan—a community based cross-sectional study. BMC Nephrol 15:90
Lee CK, Swinford RD, Cerda RD, Portman RJ, Hwang W et al (2012) Evaluation of serum creatinine concentration-based glomerular filtration rate equations in pediatric patients with chronic kidney disease. Pharmacotherapy 32(7):642–648
Lujambio I, Sottolano M, Luzardo L, Robaina S, Krul N et al (2014) Estimation of glomerular filtration rate based on serum cystatin C versus creatinine in a Uruguayan population. Int J Nephrol 2014:837106
Lopez-Giacoman S, Madero M (2015) Biomarkers in chronic kidney disease, from kidney function to kidney damage. World J Nephrol 4(1):57–73
Levey AS, Coresh J (2012) Chronic kidney disease. Lancet 379:165–180
Cockcroft DW, Gault MH (1976) Prediction of creatinine clearance from serum creatinine. Nephron 16(1):31–41
Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N et al (1999) Modification of Diet in Renal Disease Study Group. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Ann Intern Med 130(6):461–470
Liu X, Gan X, Chen J, Lv L, Li M et al (2014) A new modified CKD-EPI equation for Chinese patients with type 2 diabetes. PLoS One 9(10):e109743
Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF et al (2009) CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration). A new equation to estimate glomerular filtration rate. Ann Intern Med 150(9):604–612
Larsson A, Malm J, Grubb A, Hansson LO (2004) Calculation of glomerular filtration rate expressed in mL/min from plasma cystatin C values in mg/L. Scand J Clin Lab Invest 64(1):25–30
Grubb A, Nyman U, Björk J, Lindström V, Rippe B et al (2005) Simple cystatin C-based prediction equations for GFR compared with the MDRD prediction equation for adults and the Schwartz and the Counahan–Barratt prediction equations for children. Clin Chem 51(8):1420–1431
Gates GF (1982) Glomerular filtration rate: estimation from fractional renal accumulation of 99 Tcm-DTPA (stannous). Am J Roentgenol 138(3):565–570
Chen J, Tang H, Huang H, Lv L, Wang Y, Liu X et al (2015) Development and validation of new glomerular filtration rate predicting models for Chinese patients with type 2 diabetes. J Transl Med 13:317
Xie P, Huang JM, Lin HY, Wu WJ, Pan LP (2013) CKD-EPI equation may be the most proper formula based on creatinine in determining glomerular filtration rate in Chinese patients with chronic kidney disease. Int Urol Nephrol 45(4):1057–1064
Stevens LA, Schmid CH, Greene T, Zhang YL, Beck GJ et al (2010) Comparative performance of the CKD epidemiology collaboration (CKD-EPI) and the Modification of Diet in Renal Disease (MDRD) study equations for estimating GFR levels above 60 ml min−1 1.73 m−2. Am J Kidney Dis 56(3):486–495
White CA, Akbari A, Doucette S, Fergusson D, Knoll GA (2010) Estimating glomerular filtration rate in kidney transplantation: is the new chronic kidney disease epidemiology collaboration equation any better? Clin Chem 56(3):474–477
Pei XH, He J, Liu Q, Zhu B, Bao LH et al (2012) Evaluation of serum creatinine- and cystatin C-based equations for the estimation of glomerular filtration rate in a Chinese population. Scand J Urol Nephrol 46(3):223–231
Kilbride HS, Stevens PE, Eaglestone G, Knight S, Carter JL, Delaney MP et al (2013) Accuracy of the MDRD (Modification of Diet in Renal Disease) study and CKD-EPI (CKD Epidemiology Collaboration) equations for estimation of GFR in the elderly. Am J Kidney Dis 61(1):57–66
Hebert SA, Molony DA (2015) ACP Journal Club: the CKD-EPI equation for eGFR predicted adverse outcomes after PCI better than other equations. Ann Intern Med 163(10):JC12
Stevens LA, Claybon MA, Schmid CH, Chen J, Horio M et al (2011) Evaluation of the Chronic Kidney Disease Epidemiology Collaboration equation or estimating the glomerular filtration rate in multiple ethnicities. Kidney Int 79:555–562
Xie P, Huang J-M, Liu X-M, Wu W-J, Pan L-P et al (2013) 99mTc-DTPA renal dynamic imaging method may be unsuitable to be used as the reference method in investigating the validity of CKD-EPI equation for determining glomerular filtration rate. PLoS One 8(5):e62328
Haycock GB, Schwartz GJ, Wisotsky DH (1978) Geometric method for measuring body surface area: a height-weight formula validated in infants, children and adults. J Pediatr 93(1):62–66
Banfi G, Del Fabbro M, Lippi G (2006) Relation between serum creatinine and body mass index in elite athletes of different sport disciplines. Br J Sports Med 40:675–678
Baxmann AC, Ahmed MS, Marques NC, Menon VB, Pereira AB, Kirsztajn GM et al (2008) Influence of muscle mass and physical activity on serum and urinary creatinine and serum cystatin C. Clin J Am Soc Nephrol 3:348–354
Author contributions
YQ Provided and used the software.PX and JMH conceived and designed the experiments. PX, JMH, ZF, LGW, PF and LPP performed the experiments. PX and JMH analyzed the data. PX, JMH and YQ contributed reagents/materials/analysis tools. PX and JMH Wrote the paper.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have declared that no competing interests exist.
Additional information
This paper was partially supported by training and basic fund of clinical medicine provided by Finance Department of Hebei Province (2016).
Rights and permissions
About this article

Cite this article
Wang, J., Xie, P., Huang, Jm. et al. The new Asian modified CKD-EPI equation leads to more accurate GFR estimation in Chinese patients with CKD. Int Urol Nephrol 48, 2077–2081 (2016). https://doi.org/10.1007/s11255-016-1386-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-016-1386-9