
Abstract
Aim
To investigate the application of the new modified Chronic Kidney Disease Epidemiology Collaboration (mCKD-EPI) equation developed by Liu for the measurement of glomerular filtration rate (GFR) in Chinese patients with chronic kidney disease (CKD) and to evaluate whether this modified form is more accurate than the original one in clinical practice.
Methods
GFR was determined simultaneously by 3 methods: (a) 99mTc-diethylene triamine pentaacetic acid (99mTc-DTPA) dual plasma sample clearance method (mGFR), which was used as the reference standard; (b) CKD-EPI equation (eGFRckdepi); (c) modified CKD-EPI equation (eGFRmodified). Concordance correlation and Passing-Bablok regression were used to compare the validity of eGFRckdepi and eGFRmodified. Bias, precision and accuracy were compared to identify which equation showed the better performance in determining GFR.
Results
A total of 170 patients were enrolled. Both eGFRckdepi and eGFRmodified correlated well with mGFR (concordance correlation coefficient 0.90 and 0.74, respectively) and the Passing-Bablok regression equation of eGFRckdepi and eGFRmodified against mGFR was mGFR = 0.37 + 1.04 eGFRckdepi and −49.25 + 1.74 eGFRmodified, respectively. In terms of bias, precision and 30 % accuracy, eGFRmodified showed a worse performance compared to eGFRckdepi, in the whole cohort.
Conclusions
The new modified CKD-EPI equation cannot replace the original CKD-EPI equation in determining GFR in Chinese patients with CKD.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Chronic kidney disease (CKD) has become a worldwide epidemic problem due to the significant increase in prevalence, serious complications, and the huge expense of management including treatment and care [1–5]. The glomerular filtration rate (GFR) is recognized as the best overall indication of renal function [6–8], because it can provide an excellent measure of kidney filtering capacity and it is an important parameter for adjusting the treatment plan and assessing prognosis. Unfortunately, the inulin clearance method, the gold standard for GFR determination, cannot be applied widely in clinical practice because of the complexity and cost. Therefore, several alternative measures for estimating GFR have been devised [9–14]. Although there is continuous discussion about which one is the most accurate method, the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation developed by the Chronic Kidney Disease Epidemiology Collaboration in 2009 may be the most appropriate formula based on creatinine in determining GFR in Chinese patients with CKD [15–18].
A new modified CKD-EPI equation was developed by Liu in 2014 aimed to improve the performance of the GFR equation, and the results showed that the new modified equation achieved less bias, greater accuracy and parallel precision compared to the original CKD-EPI equation [19]. It seemed that the modified one should be preferred as the first choice instead of the original one. However, we found that the included subjects in the study were type 2 diabetic patients but not CKD patients. Moreover, the employed reference method was a calibration equation from 99mTc-diethylene triamine pentaacetic acid (99mTc-DTPA) renal dynamic imaging but not the genuine 99mTc-DTPA dual plasma sample clearance method that is recommended as the reference approach in determining GFR by the Nephrology Committee of the Society of Nuclear Medicine [20]. In order to validate the applicability of the new modified equation in determining GFR in Chinese patients with CKD and verify whether the CKD-EPI equation should be replaced by the new one, a well-designed paired cohort was set up and implemented.
Subjects and methods
Ethics statement
The study protocol was approved by Hebei Medical University ethical committee, and the written informed consent was obtained from each participant.
Patients
All enrolled participants met the diagnostic standard for CKD which was according to the National Kidney Foundation-Kidney Disease Outcomes Quality Initiative (K/DOQI) clinical practice guidelines [21], while the diagnosis of CKD did not depend on the GFR but depended on kidney damage irrespective of the level of GFR, and all patients were aged 18 years or older. Patients with complications related to acute kidney function deterioration, on renal replacement therapy, with edema, cardiac insufficiency, pleural or abdomen effusion, with a disabled limb, or on treatment with cimetidine or trimethoprim were excluded [22].
The true GFR (mGFR) measurement by the dual plasma sample clearance method has been described previously [22], and was estimated from a single exponential formula derived from the blood samples between 2 and 4 h after injection [23].
Measurement of serum creatinine
Serum creatinine (Scr) level was measured by the enzymatic method on an automatic biochemical analyzer (VITROS 5.1, Johnson & Johnson, New Brunswick, NJ, USA; reagents from the same company). The results of Scr were recalibrated with isotope dilution mass spectrometry.
GFR measurement by CKD-EPI equation (eGFRckdepi)
The CKD-EPI equation is as follows [11]:
For females:
-
With Scr concentration ≤0.7 mg/dl: eGFRckdepi = 144 × (Scr/0.7)−0.329 × (0.993)age;
-
With Scr concentration >0.7 mg/dl: eGFRckdepi = 144 × (Scr/0.7)−1.209 × (0.993)age;
For males:
-
With Scr concentration ≤0.9 mg/dl: eGFRckdepi = 141 × (Scr/0.9)−0.411 × (0.993)age;
-
With Scr concentration >0.9 mg/dl: eGFRckdepi = 141 × (Scr/0.9)−1.209 × (0.993)age.
GFR measurement by the new modified CKD-EPI equation (eGFRmodified)
For females:
-
With Scr concentration ≤0.7 mg/dl: eGFRmodified = 94 × (Scr/0.7)−0.511 × 0.998age;
-
With Scr concentration >0.7 mg/dl: eGFRmodified = 128 × (Scr/0.7)−543 × 0.992age;
For males:
-
With Scr concentration ≤0.9 mg/dl: eGFRmodified = 117 × (Scr/0.9)−0.277 × 0.994age;
-
With Scr concentration >0.9 mg/dl: GFR = 102 × (Scr/0.9)−0.558 × 0.994age.
Normalization of GFR
The mGFR (ml/min) was normalized for a body surface area of 1.73 m2 according to Haycock’s equation [24].
Statistical analysis
Measurement data were expressed as \( \bar{x} \pm s \). T test and Wilcoxon’s test were used to compare quantitative variables. The diagnostic performance of eGFRckdepi and eGFRmodified was determined by calculating Passing-Bablok regression and Lin correlation. Additionally, the Bland-Altman method was employed to evaluate the agreement between estimated GFR (eGFR) and mGFR. The bias between mGFR and eGFR was defined as eGFRckdepi minus mGFR or eGFRmodified minus mGFR. The precision was measured by means of the standard deviation of bias. The accuracy was determined as the proportion of eGFR within 30 % deviation of mGFR. T test and F test for paired samples were applied to compare, respectively, bias and precision [25]. For the comparison of accuracy, the McNemar test was employed. A value of p < 0.05 was considered statistically significant. All statistical analyses were performed using SPSS (version 17.0, SPSS, Chicago, IL, USA) and Medcalc (version 4.3, Medcalc software, Mariekerke, Belgium) software.
Results
Characteristics of enrolled CKD patients
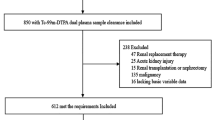
During the study time-frame, a total of 170 patients were enrolled including 82 males and 88 females with a mean age of 53 ± 17 and 58 ± 15 years, respectively (t = 1.770, p = 0.079). Patients’ demographic and clinical characteristics are presented in Table 1. A wide variety of clinical diagnoses causing CKD were observed, including chronic glomerulonephritis, diabetic nephropathy, chronic pyelonephritis, hypertensive nephropathy, chronic interstitial nephritis, immunoglobulin (Ig)A nephropathy, polycystic kidney disease, and other causes in the remaining three cases. It should be noted that the proportion of diabetic nephropathy in CKD was only 21 %.
Performance of the new modified CKD-EPI and the original one
The mean ± standard deviation (SD) index GFR for the 170 patients evaluated by the three methods was mGFR 58 ± 37, eGFRckdepi 56 ± 34 and eGFRmodified 61 ± 21 ml/min/1.73 m2, respectively. The concordance correlation coefficient for mGFR in the original CKD-EPI equation and the new modified CKD-EPI equation was 0.90 and 0.74, respectively. The Passing-Bablok regressions were constructed based on the scatter plot (Figs. 1, 2) and the regression equation of eGFRckdepi and eGFRmodified against mGFR was mGFR = 0.37 + 1.04 eGFRckdepi and mGFR = −49.25 + 1.74 eGFRmodified, respectively.

Scatter plot and Passing-Bablok regression of eGFRckdepi against mGFR in 170 subjects. eGFRckdepi estimated glomerular filtration rate by the original CKD-EPI equation, mGFR glomerular filtration rate determined by 99mTc-DTPA dual plasma sample clearance method

Scatter plot and Passing-Bablok regression of eGFRmodified against mGFR in 170 subjects. eGFRmodified estimated glomerular filtration rate by the new modified CKD-EPI equation, mGFR glomerular filtration rate determined by 99mTc-DTPA dual plasma sample clearance method
A comparison of GFR estimation equations is presented in Table 2. The bias of the original CKD-EPI equation was −1.80; in contrast, the result for the new modified one was 3.14 (t = 4.095, p < 0.001). The original CKD-EPI equation was more precise than the modified one (15.51 vs. 21.38 ml/min/1.73 m2, F = 24.808, p < 0.001). The overall percentages within 30 % of mGFR were 78.23 % for the original CKD-EPI equation and 52.15 % for the new modified one (p < 0.001). There was an obvious index that the slope of the original CKD-EPI equation was significantly much closer to the identical line and displayed the smaller intercept. Bland-Altman analysis showed a better agreement between the eGFRckdepi and mGFR and the 95 % limit of agreement for eGFRckdepi and mGFR was 60.80 ml/min−1/(1.73 m2)−1 (Figs. 3, 4).

Bland–Altman plot showing the disagreement between eGFRckdepi and mGFR. The solid long line indicates the mean of difference and the dotted long line represents the 95 % limits of agreement (2 SD). eGFRckdepi estimated glomerular filtration rate by the original CKD-EPI equation, mGFR glomerular filtration rate determined by 99mTc-DTPA dual plasma sample clearance method, SD standard deviation

Bland–Altman plot showing the disagreement between eGFRmodified and mGFR. The solid long line indicates the mean of difference and the dotted long line represents the 95 % limits of agreement (2 SD). eGFRmodified estimated glomerular filtration rate by the new modified CKD-EPI equation, mGFR glomerular filtration rate determined by 99mTc-DTPA dual plasma sample clearance method, SD standard deviation
Discussion
Accurate estimation of GFR is essential for the diagnosis and treatment of patients with CKD. A large number of methods have been developed to determine GFR more simply and accurately in view of the impracticality of the gold standard method. The CKD-EPI equation is the most frequently used and favored one in North America, Europe, Australia and China [15, 26]. Recently, a new modified CKD-EPI equation was developed and it seemed that the new modified equation was much better than the original one. But the included objects of the new equation were Chinese patients with type 2 diabetes. As is known to all, type 2 diabetes is only one of the causes of CKD. So it is necessary to assess the applicability of the new one in the patients with CKD.
In this study, we evaluated the accuracy of the new modified equation to estimate GFR in Chinese patients with CKD. Based on the dual plasma sample clearance method of 99mTc-DTPA, we found that either the new modified or the original one could be a good choice to determine GFR of CKD patients. This finding is consistent with the previous research of Liu [19].
In terms of bias, precision and accuracy, the most important three indicators in evaluating the validity of the method in determining GFR [27], the new modified formula did not outperform the original one in this study. Furthermore, the concordance correlation coefficient, intercept and slope of eGFR against mGFR and Bland-Altman analysis also supported the conclusion that the new modified formula was not better than the original one. However, the accuracy within 30 % of the original CKD-EPI remains unsatisfied in this study, which was consistent with the previous study [17, 18, 22]. But there is no working method to overcome the shortcomings of the equation as yet.
Our findings were contrary to those of Liu’s research, which might due to the following two reasons. First, the enrolled subjects of Liu’s research were patients with type 2 diabetes but not CKD patients, which may account for the difference in bias, precision and accuracy. The serum glucose level and body mass index of patients with type 2 diabetes are drastically different from those of “ordinary” CKD patients, which might affect the accuracy of GFR [28–30]. Another reason may be the difference of the selected reference method to determine true GFR. A calibration equation from 99mTc-DTPA renal dynamic imaging was employed as the reference method in Liu’s research. However, 99mTc-DTPA renal dynamic imaging can be affected by a large number of factors such as the sketching of region of interest [31] and the dosage of administration [32]. Moreover, it may overestimate the true GFR and be less accurate than the CKD-EPI equation. So 99mTc-DTPA renal dynamic imaging may be unsuitable to use as the reference method in determining GFR, even the linear regression equation derived from it. Accordingly, in this study we used the 99mTc-DTPA dual plasma sample clearance method, which may provide a perfect true GFR resulting in more a reliable conclusion.
The limitation of the present study is that the sample size was so small that it was inadequate to compare the application of the two equations according to CKD stage, causes of CKD, and the age of patients.
In conclusion, the new modified CKD-EPI equation did not show an improved performance with respect to the original one. Therefore, we propose that the modified equation be ignored and the original CKD-EPI equation remain the first choice for the measurement of GFR in Chinese CKD patients, in spite of the unsatisfactory accuracy within 30 %.
References
Stevens PE, O’Donoghue DJ, de Lusignan S, Van Vlymen J, Klebe B, Middleton R et al (2007) Chronic kidney disease management in the United Kingdom: NEOERICA project results. Kidney Int 72(1):92–99
Zhang Q-L, Rothenbacher D (2008) Prevalence of chronic kidney disease in population-based studies: systematic review. BMC Public Health 8:117
Coresh J, Astor BC, Greene T, Eknoyan G, Levey AS (2003) Prevalence of chronic kidney disease and decreased kidney function in the adult US population: Third National Health and Nutrition Examination Survey. Am J Kidney Dis 41(1):1–12
Excerpts from the USRDS Annual Data Report (2006) Am J Kidney Dis 49(Suppl 1):S1–S296
Kim NH, Hyun YY, Lee KB, Chang Y, Ryu S et al (2015) Environmental heavy metal exposure and chronic kidney disease in the general population. J Korean Med Sci 30(3):272–277
Lee CK, Swinford RD, Cerda RD, Portman RJ, Hwang W et al (2012) Evaluation of serum creatinine concentration-based glomerular filtration rate equations in pediatric patients with chronic kidney disease. Pharmacotherapy 32(7):642–648
Lujambio I, Sottolano M, Luzardo L, Robaina S, Krul N et al (2014) Estimation of glomerular filtration rate based on serum cystatin C versus creatinine in a uruguayan population. Int J Nephro 2014:837106
Lopez-Giacoman S, Madero M (2015) Biomarkers in chronic kidney disease, from kidney function to kidney damage. World J Nephrol. 4(1):57–73
Cockcroft DW, Gault MH (1976) Prediction of creatinine clearance from serum creatinine. Nephron 16(1):31–41
Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N et al (1999) Modification of Diet in Renal Disease Study Group. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Ann Intern Med 130(6):461–470
Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF 3rd et al (2009) CKD-EPI (chronic kidney disease epidemiology collaboration). A new equation to estimate glomerular filtration rate. Ann Intern Med 150(9):604–612
Larsson A, Malm J, Grubb A, Hansson LO (2004) Calculation of glomerular filtration rate expressed in mL/min from plasma cystatin C values in mg/L. Scand J Clin Lab Invest 64(1):25–30
Grubb A, Nyman U, Björk J, Lindström V, Rippe B et al (2005) Simple cystatin C-based prediction equations for GFR compared with the MDRD prediction equation for adults and the Schwartz and the Counahan-Barratt prediction equations for children. Clin Chem 51(8):1420–1431
Gates GF (1982) Glomerular filtration rate: Estimation from fractional renal accumulation of 99Tcm-DTPA (stannous) [J]. Am J Roentgenol 138(3):565–570
Xie P, Huang JM, Lin HY, Wu WJ, Pan LP (2013) CKD-EPI equation may be the most proper formula based on creatinine in determining glomerular filtration rate in Chinese patients with chronic kidney disease. Int Urol Nephrol 45(4):1057–1064
Stevens LA, Schmid CH, Greene T, Zhang YL, Beck GJ et al (2010) Comparative performance of the CKD epidemiology collaboration (CKD-EPI) and the modification of diet in renal disease (MDRD) Study equations for estimating GFR levels above 60 ml min−11.73 m−2. Am J Kidney Dis 56(3):486–495
White CA, Akbari A, Doucette S, Fergusson D, Knoll GA (2010) Estimating glomerular filtration rate in kidney transplantation: is the new chronic kidney disease epidemiology collaboration equation any better? Clin Chem 56(3):474–477
Pei XH, He J, Liu Q, Zhu B, Bao LH et al (2012) Evaluation of serum creatinine- and cystatin C-based equations for the estimation of glomerular filtration rate in a Chinese population. Scand J Urol Nephrol 46(3):223–231
Liu X, Gan X, Chen J, Lv L, Li M et al (2014) A new modified CKD-EPI equation for chinese patients with type 2 diabetes. PLoS One 9(10):e109743
Blaufox MD, Aurell M, Bubeck B, Fommei E, Piepsz A et al (1996) Report of the radionuclides in nephrourology committee on renal clearance. J Nucl Med 37(11):1883–1890
Eknoyan G, Levin N (2001) NKF-K/DOQI clinical practice guidelines: update 2000, Foreword. Am J Kidney Dis 37(1 suppl 1):S5–S6
Xie P, Huang J-M, Liu X-M, Wu W-J, Pan L-P et al (2013) 99mTc-DTPA renal dynamic imaging method may be unsuitable to be used as the reference method in investigating the validity of CKD-EPI equation for determining glomerular filtration rate. PLoS ONE 8(5):e62328
Blaufox MD, Aurell M, Bubeck B, Fommei E, Piepsz A et al (1996) Report of the radionuclides in nephrourology committee on renal clearance. J Nucl Med 37(11):1883–1890
Haycock GB, Schwartz GJ, Wisotsky DH (1978) Geometric method for measuring body surface area: a height-weight formula validated in infants, children and adults. J Pediatrics 93(1):62–66
Pöge U, Gerhardt T, Stoffel-Wagner B, Palmedo H, Klehr HU et al (2007) Can modifications of the MDRD formula improve the estimation of glomerular filtration rate in renal allograft recipients? Nephrol Dial Transplant 22(12):3610–3615
Earley A, Miskulin D, Lamb EJ, Levey AS, Uhlig K (2012) Estimating equations for glomerular filtration rate in the era of creatinine standardization: a systematic review. Ann Intern Med 156:785–795 (W–270, W–271, W–272, W–273, W–274, W–275, W–276, W–277, W–278)
Lee CK, Swinford RD, Cerda RD, Portman RJ, Hwang W et al (2012) Evaluation of serum creatinine concentration-based glomerular filtration rate equations in pediatri-c patients with chronic kidney disease. Pharmacotherapy 32(7):642–648
Rigalleau V, Lasseur C, Raffaitin C, Perlemoine C, Barthe N et al (2006) Glucose control influences glomerular filtration rate and its prediction in diabetic subjects. Diabetes Care 29:1491–1495
Kawamoto R, Kohara K, Tabara Y, Miki T, Ohtsuka N et al (2008) An association between body mass index and estimated glomerular filtration rate. Hypertens Res 31:1559–1564
Fontela PC, Winkelmann ER, Ott JN, Uggeri DP (2014) Estimated glomerular filtration rate in patients with type 2 diabetes mellitus. Rev Assoc Med Bras 60(6):531–537
Dopuda M, Ajdinović B, Jauković L, Petrović M, Janković Z (2008) Influence of the background activity region selection on the measurement of glomerular filtration rate using the Gates method. Vojnosanit Pregl 65(10):729–732
Assadi M, Eftekhari M, Hozhabrosadati M, Saghari M, Ebrahimi A et al (2008) Comparison of methods for determination of glomerular filtration rate: low and high-dose Tc-99m-DTPA renography, predicted creatinine clearance method, and plasma sample method. Int Urol Nephrol 40(4):1059–1065
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have declared that no competing interests exist.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Xie, P., Huang, Jm., Li, Y. et al. The modified CKD-EPI equation may be not more accurate than CKD-EPI equation in determining glomerular filtration rate in Chinese patients with chronic kidney disease. J Nephrol 30, 397–402 (2017). https://doi.org/10.1007/s40620-016-0307-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40620-016-0307-4