
Abstract
Introduction
The question of when an intraepithelial urothelial carcinoma becomes invasive into the lamina propria of the urinary bladder is an unresolved issue. Our objective was to analyse a series of consecutive superficial carcinomas to assess the importance of growth pattern in tumour recurrence and progression.
Materials and methods
The pathological staging of 200 superficial (pTa/pT1) bladder carcinomas was reviewed. Non-invasive lesions and tumours invading the lamina propria were distinguished. Both infiltrating and pushing patterns of growth were regarded as lamina propria invasion.
Results
A total of 35 (17.5%) pTa and 165 (82.5%) pT1 tumours were identified. Among pT1 tumours, 39 (23.6%) displayed the infiltrating pattern of invasion and 126 (76.4%) the pushing pattern. Differences in five-year recurrence-free (P = 0.01) and progression-free (P = 0.001) survival were demonstrated between pTa and pT1 tumours, and between pT1 infiltrating and pT1 pushing subcategories. Invasive growth pattern has a 1.86 times higher risk of tumour recurrence and 3.01 times higher risk of progression.
Conclusions
The pT1 category of bladder carcinoma should include a group of tumours defined by its pushing pattern of growth. Some cases may have been previously considered pTa, but follow an intermediate clinical course between pTa and pT1 tumours with infiltrating growth pattern.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Urothelial bladder carcinomas (UBC) are very common neoplasms in hospital practice. Occupational exposure, diet, smoking, drugs, and many other predisposing factors [1, 2] actually make this disease a health problem of major concern in industrialised areas. As a result, these tumours rank among the most common malignancies in most tumour registers in developed countries [2], a tendency which seems likely to continue in the near future [3]. Approximately 75–80% of patients with UBC have a superficial non-muscle-invasive tumour at diagnosis [4] and this gives most of them an a priori good prognosis, because only 15–20% will progress to muscle invasive disease in five years.
However, this potentially curative phase of the disease is far from being homogeneous. It includes a wide spectrum of tumours with complex and rather unpredictable behaviour in terms of tumour recurrence or development of invasive disease. Most superficial bladder tumours exhibit a loss of heterozygosity of chromosome 9 and activating mutations in the HRAS and FGFR3 genes [4]. The cases which progress to invasive disease have been investigated in depth in an attempt to define the clinical, pathologic, or molecular factors, for example incorrect clinical staging, incomplete resections, blood group, Rb gene, K-ras, and many others, which may make them progress to invasive disease [4]. So far, no molecular markers have been found to selectively reveal superficial cases that will progress to invasive disease.
Another important question is exact definition of when an intraepithelial UBC becomes invasive into the lamina propria (LP) of the bladder, particularly in low-grade tumours. It is currently believed that tumour cells that arrange themselves in slender cords or small nests within the LP are the hallmark for diagnosis of invasion [1].
Urologists consider “superficial” UBC, high-grade, with LP invasion (pT1-G3) a distinct group of urothelial tumours with higher risk of progression, especially if associated with in-situ carcinoma or deep LP invasion [5, 6]. Low-grade tumours (G1–G2) may eventually invade the LP but, in such instances, assessment of invasion may become very difficult if the “infiltrating pattern” only is accepted as invasion. In fact, low-grade tumours do not usually invade with an infiltrating pattern.
We present a critical review of pathological staging and survival, focussing on tumour recurrence and progression, for a series of 200 superficial (pTa/pT1) UBCs with long-term follow-up. The objective of the study was to define the clinical behaviour of superficial UBC with pushing pattern of growth, and to determine whether recognition of growth pattern subtype is of prognostic value in superficial UBCs.
Materials and methods
This retrospective study analysed transurethral resection (TUR) specimens of 200 consecutive superficial exophytic papillary or flat UBCs diagnosed and uniformly treated by the same team. After TUR, the patients received intravesical instillations of either mitomycin C (low/intermediate-grade tumours) or BCG (high-grade tumours). Cases with poorly preserved material or with difficulties in histological evaluation, and patients with less than one-year of clinical follow up, were not included in the study. UBCs with inverted growth pattern were excluded. Every patient was followed until recurrence or progression. The average follow-up of cases was 44 months (range, 14–121). Tumour size and focality were assigned by the urologist at the time of TUR. The same pathologist reviewed all the cases and applied uniform diagnostic criteria when assigning grade and level of invasion. Because randomized biopsies of the bladder were not performed systematically, the presence of concomitant in-situ carcinoma was not properly evaluated.
Tumours were graded in accordance with the 1973 WHO criteria [7] with modifications with regard to definition of the intermediate grade. According to Pauwels et al. [8], this population was subclassified depending on the preservation (G2a) or absence (G2b) of nuclear polarity in tumour cells. With the intention of improving reproducibility, G1 and G2a tumours were grouped as low-grade category while G2b and G3 tumours were grouped as high grade.
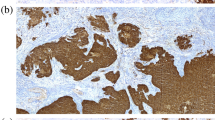
Regarding the level of invasion, tumours were staged in accordance with the 2002 TNM classification guidelines [9]. From a histological perspective, three different categories were recognised: pTa, pT1 pushing pattern, and pT1 infiltrating pattern (Fig. 1). pTa category in UBCs was diagnosed by applying the WHO criteria [7]. pT1 tumours were subdivided according to their pattern of growth. For this purpose different criteria were applied. An infiltrating pattern was considered when single cells, cords, or small nests invaded the LP, often inducing some kind of stromal reaction, for example chronic inflammation or desmoplasia. On the other hand, a pushing pattern of growth was recognised only in well oriented TUR chips when large, solid, and expansive tumour nests were seen pushing down into the LP. The tumour/stroma interface in these areas shows some degree of stromal reaction, with fibrosis and, eventually, lymphoid infiltrates. TUR chips that, because of orientation of the sections, could not be properly assessed for invasion of the lamina propria were not considered in this study to avoid diagnostic inconsistency.

Architectural spectrum of papillary superficial urothelial tumours in the urinary bladder. a Exophytic growth with intact basal limit in pTa carcinoma. b Exophytic growth with expansive borders at the basal limit in the pushing pattern of bladder carcinoma (note the well oriented normal urothelium on the right side). c Infiltrating tumour nests in the infiltrating pattern of bladder carcinoma
Statistical analysis included descriptive statistics and a survival study focussing on recurrence-free and progression-free survival (Kaplan–Meier curves and log-rank test) using SPSS 13.0 for Windows (SPSS, Chicago, IL, USA). The correlation between pattern of invasion and other variables (sex, tumour size, multiplicity, tumour grade) was assessed by use of the χ 2 test.
Results
Males predominated in the series (173 M/27 F), with an average age of 63 years (range 13–87). Table 1 summarises the diagnostic categories and histological grade distribution. There were 35 pTa and 165 pT1 tumours (161 were papillary and four flat). Among pT1 tumours, 39 displayed the infiltrating and 126 the pushing pattern of growth. All pTa tumours were low-grade (G1, G2a). Within the pT1 category 71 cases were G1, 82 were G2, and 13 were G3 carcinomas. Almost all G3 tumours displayed the infiltrating pattern of growth. Conversely, pT1G1 infiltrating lesions were very rare. The pushing pattern of growth was shared by pT1 tumours of all tumour grades. Tumour characteristics that are related to depth and pattern of growth are listed in Table 2.
We analysed recurrence and progression rate of pTa and pT1 carcinomas. Fifty percent of the total series were free from recurrence at five years. According to the level of invasion, 73.9% of pTa, 50.1% of pT1 with pushing pattern, and 29.2% of pT1 with infiltrating pattern were free from recurrence at that time (log-rank, P = 0.01). The prognostic impact of tumour recurrence of other potentially prognostic variables was also assessed and hazard ratios were recorded (Table 3). pT1 cases with infiltrating pattern of growth had a 1.86 times higher risk of tumour recurrence. Regarding tumour progression, 82% of the cases were progression-free at five years, and so were 95.2% of pTa cases, 84% of pT1 with pushing pattern, and 61% of pT1 with infiltrating pattern (log-rank, P = 0.001). The prognostic impact on tumour progression of other histopathological prognostic variables and the corresponding hazard ratios were also recorded (Table 4). The infiltrating pattern of growth in pT cases led to a 3.01 times higher risk of tumour progression. Kaplan–Meier curves illustrate the impact of considering depth of invasion and growth pattern in superficial tumours, on prediction of both tumour recurrence (Fig. 2a) and tumour progression (Fig. 2b). A significant difference was noted between patients with an initial diagnosis of pTa and pT1 pushing pattern, and also between patients with a diagnosis of pT1 pushing and pT1 infiltrating pattern, regarding both recurrence and progression. Mean survival time for pT1 with pushing pattern and pTa tumours was very similar in this series, both for recurrence and progression, and much longer than mean survival time for pT1 with infiltrating pattern (Tables 3 and 4).

Kaplan–Meier curves revealing recurrence-free (a, log rank test P = 0.01) and progression-free (b, log rank test P = 0.001) survival for patients with pTa, pT1 pushing, and pT1 infiltrative pattern tumours. The numbers of patients at risk are specified below
Cox regression analysis revealed that the depth of invasion with assessment of the growth pattern is the only histological variable that predicts tumour recurrence (β coefficient, 0.652, P = 0.026) (Table 5), and that no histological variable (depth of invasion, tumour grade in three categories, tumour grade in two categories) really predicts tumour progression in this series. Among these, the grade defined by the 1973 WHO criteria is the only variable that nearly reaches statistical significance (β coefficient, 0.423, P = 0.07) (Table 6).
Discussion
Superficial UBC is a common and very heterogeneous disease characterised by its high propensity to recur and a worrisome tendency to progress to muscle-invasive disease [10]. It is not surprising that urologists treat it very heterogeneously. In fact, management of T1 disease is not standardised, at least in part because identification of the population at higher risk of progression is not always easy. Tumour stage at diagnosis is the most important factor predicting survival in UBCs [11–13], and the depth of tumour invasion can be reliably determined in approximately 60% of patients evaluated when assessing invasion of the muscularis mucosae layer [14].
From the pathologist’s point of view, various approaches assessing the depth of invasion into the LP have been described, i.e., direct measurement of the depth of invasion by use of a micrometer or by measurement of the length of the invasive front [15–18]. However, none of these methods has gained widespread acceptance to date. The term microinvasive carcinoma is often used, but there is no a generalised consensus on its definition [16]. However, using depth of invasion as the only criterion to assess infiltration can be misleading [18].
Among superficial tumours, assignment of the pTa and pT1 categories has been a crucial issue for both urologist and patient. The pathologist notes, usually on TUR specimens, if a tumour is confined to the basal membrane or it invades the LP. In the urinary tract, a pTa tumour is defined as an intraepithelial, papillary, and low or high-grade neoplasm excluding carcinoma in situ, and pT1 as a neoplasm that invades the LP, irrespective of whether the lesion is papillary or flat, or low or high-grade. The prognostic implications of this distinction seem obvious. However, a reliable distinction is difficult to make and certainty whether the LP is invaded or not is a subject of significant disagreement among pathologists [16, 19]. Current belief states that a tumour invades the LP when small nests, cords, or single cells definitely lie within the stroma, often inducing some degree of local reaction that takes the form of desmoplasia and/or chronic inflammation. Following this definition, pT1 tumours in the bladder seem to be nearly restricted to high-grade neoplasms, because this pattern of invasion is typical of high-grade tumours. Proportionally, these lesions are relatively infrequent. Describing a series of consecutive bladder cancer specimens, Köllerman and Helpap [20] state that only 3.3% of 667 UBCs were pT1-G3 tumours. There is also heterogeneous recognition of the category pTa-G3 in the urologic literature. Some authors define it as a large population within high-risk superficial bladder cancer [10, 21] while others omit this category altogether [22].
Bladder cancer series in US do include a large number of pTa-G3 tumours and, at the same time, tend to consider pT1-G1/G2 cases a rarity. For instance, Amling [23] states that approximately 70% of superficial tumours are pTa and that most pT1 cases are clinically aggressive high-grade (G3) neoplasms because they have already demonstrated invasive potential. We believe that this huge proportion of pTa cases is not tenable and also that pT1 low to intermediate (G1–G2) tumours do exist in a more significant proportion [11]. In the same sense, the studies performed by the EORTC Genitourinary Group [24] show a clear tendency to assume that superficial tumours can be Ta/T1 G1 to G3, and a large number of essays have been produced on the population of low-intermediate risk of progression (Ta/T1 G1–G2). Another unresolved issue is that some pTa tumours, both at TUR and cystectomy, may develop lymph node metastases and even may pursue a fatal course [25, 26]. Herr [26] found a similar death rate between pTa-G3 and T1 tumours in a series after 15 years of follow up. However, we have difficulty accepting that a strictly speaking intraepithelial papillary tumour, diagnosed and treated appropriately, may kill a patient.
All these arguments suggest there is no agreement to define when and how an UBC invades the LP. Traditionally, this confusion tends to be avoided by the policy that considers non-muscle invasive bladder cancer (pTa, pTis, pT1) as a whole [21] but, conversely, others plead for the need to appropriately distinguish and uncouple Ta and T1 lesions [19, 27]. The absence of fully accepted histopathological criteria on this issue and the profusion of litigation so common in many western societies may have led pathologists to a defensive attitude when diagnosing non-muscle invasive bladder carcinomas. This could be the reason pathologists consider UBCs with pushing pattern of growth as mere intraepithelial neoplasms. However, the concept of pushing borders is not new and is well recognised and accepted in several neoplasia of other sites [28, 29].
If these considerations are taken into account when reviewing superficial bladder cancer, the number of pTa cases will surely diminish to more realistic numbers, no patient with a pTa tumour would be expected to die of the disease, and pushing and infiltrating patterns, and high and low-grade tumours, could be all identified among pT1 category. In the series we present, tumours characterised as pT1 with pushing pattern tend to be of smaller size and of lower grade than those with infiltrating pattern, as do pTa lesions. Besides, pTa and pT1 patients with pushing pattern of growth also tend to be younger. Nevertheless, despite the associations, this mixed definition of tumour invasion and growth pattern is, by itself, a definite marker of tumour recurrence in our series. Therefore, the recognition of a formerly underestimated subcategory in T1 bladder cancer, defined by its pushing pattern of growth, would lead to more precise assignment of prognosis within the TNM staging system. Following our own experience and that of others [30, 31], the redistribution of tumour grade suggested in the 1998 WHO/ISUP consensus [32] could be simpler, but adds nothing to the three-grade 1973 WHO system in terms of predicting outcome. In this regard, although a very recent proposal by van der Kwast et al. [33] clarifies the terminology for classifying superficial bladder neoplasms, the question of when an intraepithelial carcinoma becomes invasive into the LP still remains unresolved. The solution to this permanent dilemma might be to avoid the word “invasion” in this group of superficial UBCs and reserve it only for muscle-invasive UBCs. Instead, identification of the growth pattern could be enough to subclassify bladder superficial tumours in terms of risk of recurrence and progression, as proved in this work.
To summarise, this study is intended to call the attention of pathologists to a subset of UBCs characterised, in terms of clinical evolution (recurrence and progression), by intermediate behaviour between intraepithelial and classical LP infiltrating neoplasms. This group of tumours includes those of a significant number of patients in the urological consultation and is defined histologically by its pushing pattern of growth into the LP.
References
Murphy WM, Grignon DJ, Perlman EJ (2004) Tumors of the kidney, bladder, and related urinary structures. AFIP Atlas of tumor pathology, 4th Series, Fascicle 1. American Registry of Pathology, Washington, DC
Ries LAG, Eisner MP, Kosary CL, Hankey BF, Miller BA, Clegg L, et al (eds) (2004). SEER cancer statistics review, 1975–2001, National Cancer Institute. Bethesda, MD. http://seer.cancer.gov/csr/1975_2001/
Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ (2007) Cancer statistics, 2007. CA Cancer J Clin 57:43–66
Pasin E, Josephson DY, Mitra AP, Cote RJ, Stein JP (2008) Superficial bladder cancer: an update on etiology, molecular development, classification, and natural history. Rev Urol 10:31–43
Vicente J, Laguna MP, Duarte D, Algaba F, Chechile G (1991) Carcinoma in situ as a prognostic factor for G3pT1 bladder tumours. Br J Urol 68:380–382. doi:10.1111/j.1464-410X.1991.tb15355.x
Hasui Y, Osada Y, Kitada S, Nishi S (1994) Significance of invasion to the muscularis mucosae on the progression of superficial bladder cancer. Urology 43:782–786. doi:10.1016/0090-4295(94)90134-1
Mostofi FK, Sobin LH, Torloni H (1973) Histological typing of urinary bladder tumours. International classification of tumours, 19. World Health Organisation, Geneva
Pauwels RPE, Schapers RFM, Smeets AWGB, Debruyne FMJ, Geraedts JPM (1988) Grading in superficial bladder cancer. (1) Morphological criteria. Br J Urol 61:129–134. doi:10.1111/j.1464-410X.1988.tb05060.x
Sobin LH, Wittekind C (eds) (2002) TNM Classification of malignant tumours, 6th edn. Wiley, New York
Cookson MS, Herr HW, Zhang Z, Soloway S, Sogani PC, Fair WR (1997) The treated natural history of high risk superficial bladder cancer: 15-year outcome. J Urol 158:62–67. doi:10.1097/00005392-199707000-00017
Angulo JC, López JI, Flores N, Toledo JD (1993) The value of tumour spread, grading, growth pattern as morphological predictive parameters in bladder carcinoma. A critical revision of the 1987 TNM classification. J Cancer Res Clin Oncol 119:578–593. doi:10.1007/BF01372721
Hendry WF, Rawson NSB, Turley L, Dunlop A, Whitfield HN (1990) Computerisation of urothelial carcinoma records: 16 years’ experience with the TNM system. Br J Urol 65:583–588. doi:10.1111/j.1464-410X.1990.tb14825.x
Lipponen PK, Eskelinen MJ, Kiviranta J, Pesonen E (1991) Prognosis of transitional cell bladder cancer: a multivariate prognostic store for improved prediction. J Urol 146:1535–1540
Angulo JC, López JI, Grignon DJ, Sanchez-Chapado M (1995) Muscularis mucosa differentiates two populations with different prognosis in Stage I bladder cancer. Urology 45:47–53. doi:10.1016/S0090-4295(95)96490-8
Holmäng S, Hedelin H, Anderström C, Holmberg E, Johansson SL (1997) The importance of the depth of invasion in stage T1 bladder carcinoma: a prospective cohort study. J Urol 157:800–804. doi:10.1016/S0022-5347(01)65044-4
Pathologists of the French Association of Urology Cancer Committee (1993) Lamina propria microinvasion of bladder tumors, incidence on stage allocation (pTa vs pT1): recommended approach. World J Urol 11:161–164
Cheng L, Weaver AL, Neumann RM, Scherer BG, Bostwick DG (1999) Substaging of T1 bladder carcinoma based on the depth of invasion as measured by micrometer: a new proposal. Cancer 86:1035–1043. doi:10.1002/(SICI)1097-0142(19990915)86:6<1035::AID-CNCR20>3.0.CO;2-D
Van der Aa MNM, van Leenders GJLH, Steyerberg EW et al (2005) A new system for substaging pT1 papillary bladder cancer: a prognostic evaluation. Hum Pathol 36:981–986. doi:10.1016/j.humpath.2005.06.017
Bol MG, Baak JP, Buhr-Wildhagen S et al (2003) Reproducibility and prognostic variability of grade and lamina propria invasion in stages Ta, T1 urothelial carcinoma of the bladder. J Urol 169:1291–1294. doi:10.1097/01.ju.0000055471.78783.ae
Köllermann J, Helpap B (2001) High risk superficial bladder carcinoma-pT1G3: the significance of its diagnosis on transurethral resection specimens. Urol Integrada Invest 6:24–30
Smith JA, Labasky RF, Cockett ATK, Fracchia JA, Montie JE, Rowland RG (1999) Bladder cancer clinical guidelines panel summary report on the management of nonmuscle invasive bladder cancer (stages Ta, T1 and TIS). J Urol 162:1697–1701. doi:10.1016/S0022-5347(05)68208-0
Solsona E, Iborra I, Dumont R, Rubio-Briones J, Casanova J, Almenar S (2000) The 3-month clinical response to intravesical therapy as a predictive factor for progression in patients with high risk superficial bladder cancer. J Urol 164:685–689. doi:10.1016/S0022-5347(05)67281-3
Amling CL (2001) Diagnosis and management of superficial bladder cancer. Curr Probl Cancer 25:219–278. doi:10.1067/mcn.2001.117539
Kurth KH, Bouffioux C, Sylvester R, Van der Meijden APM, Oosterlinck W, Brausi M, Members of the EORTC Genitourinary Group (2000) Treatment of superficial bladder tumours: achievement and needs. Eur Urol 37(Suppl 3):1–9. doi:10.1159/000052386
Wiesner C, Pfitzenmaier J, Faldum A, Gillitzer R, Melchior SW, Thüroff JW (2005) Lymph node metastases in non-muscle invasive bladder cancer are correlated with the number of transurethral resections and tumour upstaging at radical cystectomy. BJU Int 95:301–305. doi:10.1111/j.1464-410X.2005.05287.x
Herr HW (2000) Tumor progression and survival of patients with high grade, non-invasive papillary (TaG3) bladder tumors: 15-year outcome. J Urol 163:60–62. doi:10.1016/S0022-5347(05)67972-4
Bryan RT, Wallace DM (2002) “Superficial” bladder cancer. Time to uncouple pT1 tumours from pTa tumours. BJU Int 90:846–852. doi:10.1046/j.1464-410X.2002.03053.x
Shintani S, Matsuura H, Hasegawa Y, Nakayama B, Fujimoto Y (1997) The relationship of shape of tumor invasion to depth of invasion and cervical lymph node metastasis in squamous cell carcinoma of the tongue. Oncology 54:463–467
Tajima Y, Nakanishi Y, Ochiai A et al (2000) Histopathologic findings predicting lymph node metastasis and prognosis of patients with superficial esophageal carcinoma: analysis of 240 surgically resected tumors. Cancer 88:1285–1293. doi:10.1002/(SICI)1097-0142(20000315)88:6<1285::AID-CNCR3>3.0.CO;2-R
Oosterhuis JWA, Schapers RFM, Janssen-Heijnen MLG, Pauwels RPE, Newling DW, ten Kate F (2002) Histological grading of papillary urothelial carcinoma of the bladder: prognostic value of the 1998 WHO/ISUP classification system and comparison with conventional grading systems. J Clin Pathol 55:900–905. doi:10.1136/jcp.55.12.900
Montironi R, Lopez-Beltran A, Mazzucchelli R, Bostwick DG (2003) Classification and grading of the non-invasive urothelial neoplasms: recent advances and controversies. J Clin Pathol 56:91–95. doi:10.1136/jcp.56.2.91
Epstein JI, Amin MB, Reuter VR, Mostofi FK, Bladder Consensus Conference Committee (1998) The World Health Organization/International Society of Urological Pathology consensus classification of urothelial (transitional cell) neoplasms of the urinary bladder. Am J Surg Pathol 22:1435–1438. doi:10.1097/00000478-199812000-00001
Van der Kwast TH, Zlotta AR, Fleshner N, Jewett M, Lopez-Beltran A, Montironi R (2008) Thirty-five years of noninvasive bladder carcinoma. A plea for the use of papillary intraurothelial neoplasia as new terminology. Anal Quant Cytol Histol 30:309–315
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
López, J.I., Angulo, J.C. Growth pattern in superficial urothelial bladder carcinomas. Histological review and clinical relevance. Int Urol Nephrol 41, 847–854 (2009). https://doi.org/10.1007/s11255-009-9537-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-009-9537-x