
Abstract
Although postpartum depression (PPD) symptoms are fairly common among new mothers and fathers, new parents still perceive a stigma associated with having the “baby blues.” Research has extensively examined the role of perceived stigma on help-seeking for clinical PPD, but little is known about the process of perceived stigma in new parents. We examined the role of perceived stigma in postpartum depressive symptoms using the dual-pathway model (Mickelson and Williams 2008). Specifically, we tested whether internalized stigma would influence PPD symptoms through parenting efficacy, whereas experienced stigma would influence PPD symptoms through indirect support-seeking. We also examined whether the internalized pathway was stronger for fathers while mothers would utilize both pathways. Using longitudinal data from a community sample of first-time parents in the United States, we found parenting efficacy was a mediator between internalized stigma and PPD symptoms for mothers and experienced stigma and PPD symptoms for fathers; indirect support-seeking was only a cross-sectional mediator for mothers between internalized stigma and PPD symptoms. Understanding how new mothers and fathers perceive the stigma attached to PPD symptoms and the process by which it impacts symptom reporting can help to improve interventions aimed at new parents.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Any new parent can tell you about the joy and happiness of having a baby; less openly discussed are feelings of distress and depression associated with the new parent role. Even so, approximately 10–20 % of U.S. mothers (Horowitz and Goodman 2005) and 10 % of U.S. fathers (Paulson and Bazemore 2010) experience clinical postpartum depression (PPD)—or peripartum depression as it is now termed in the DSM-5 (American Psychiatric Association 2013)—and even more mothers experience non-clinical levels of postpartum depression symptoms. Although PPD symptoms can be concealed, its association with mental illness means that it is still socially stigmatized. Numerous online websites and popular books discuss how PPD symptoms are minimized by society, but the primary focus of empirical stigma research is on mothers and barriers to seeking help for clinical PPD (see McCoughlin 2013; Werner et al. 2015, for reviews). Furthermore, to our knowledge, there are no studies on perceived stigma of PPD among fathers, nor on the process of perceived PPD stigma in first-time parents. In the current study, we utilize the dual-pathway model of perceived stigma (Mickelson and Williams 2008), which suggests internalized stigma impacts intrapersonal constructs such as self-efficacy, whereas experienced stigma impacts interpersonal constructs such as social support. We propose mothers and fathers will differ in mean levels of internalized and experienced PPD stigma, as well as the pathways by which perceived stigma impacts PPD symptom reporting. Please note that all studies cited in this paper are U.S. based (unless otherwise stated).
Perceived Stigma and PPD Symptoms
Definitions of stigma have ranged from having a personal characteristic that deviates from societal norms (Goffman 1963) to social stereotyping or categorization (see Jones et al. 1984, for a review). Stigma has traditionally been defined from the perspective of the perpetrator’s labeling of the target, rather than the target’s perceptions of stigma. In the past two decades, research has examined the concept of perceived stigma, finding that, regardless of whether society continues to label a condition or characteristic as stigmatizing, individuals who belong to groups (or have characteristics) that have been traditionally marginalized can vary quite dramatically in their perceptions of stigma (Corrigan and Calabrese 2005; Crandall 1991). Additionally, some researchers have distinguished between self- and experienced-subtypes of perceived stigma (Corrigan et al. 2006; Watson et al. 2007). For the present study, we will utilize Mickelson and Williams’ (2008) two dimensional definition of perceived stigma. Specifically, internalized perceived stigma is defined as a person’s negative feelings (e.g., embarrassment, shame, or deviance) about their postpartum depression symptoms, whereas experienced perceived stigma is defined as a person’s perception of being stigmatized by others because of their postpartum depression symptoms (which may or may not accurately reflect network members’ behaviors and feelings).
Research on stigma related to general depression is extensive (Corrigan et al. 2006; Link et al. 2001), as is research with a specific focus on stigma related to clinical PPD (see McCoughlin 2013, for a review). Researchers examining PPD stigma have discussed the uniqueness of this stigma in mothers. Specifically, the stigma of PPD for mothers includes being seen as an incompetent parent and being ashamed for feeling sad when one should feel happy at the birth of their child (Mauthner 2002; Taylor 1996). As stated above, the primary emphasis of prior research is on how stigma impacts mothers’ help-seeking for clinical PPD. We have not been able to locate any studies that examine whether perceived PPD stigma actually influences one’s reporting of postpartum depression symptoms, and, if so, what processes explain the association.
Unlike research with mothers, research on perceived PPD stigma among fathers is virtually nonexistent. This inattention is likely due to paternal PPD only recently being acknowledged and examined in the empirical literature. Prevalence rates of clinical paternal PPD in community samples have ranged widely from 1.2 to 25.5 % (see Goodman 2004, for a review), with a meta-estimate of 10.4 % (Paulson and Bazemore 2010). Yet, research on paternal PPD is quite scarce. A recent meta-analysis of prenatal and postpartum depression in fathers identified only 43 research studies that included the incidence rates of clinical paternal postpartum depression during the first year following the baby’s birth (Paulson and Bazemore 2010).
No known published research has quantitatively examined whether fathers feel a sense of stigma attached to their PPD symptoms. There are several qualitative studies suggesting fathers do attach a stigma to paternal PPD (Davey et al. 2006 – Australian sample; Edward et al. 2015; Melrose 2010). These studies, like the ones on mothers, never go further and examine the perceived stigma process for fathers. The first aim of the current study is to examine the degree to which mothers and fathers report perceived stigma related to PPD symptoms and whether there are gender differences between mothers and fathers in terms of perceived PPD stigma. Given that PPD symptoms are more common among mothers than fathers, the relative rarity of paternal PPD suggests fathers may report greater perceived stigma than do mothers. On the other hand, being a “good mother” has been more strongly connected with female gender identity than being a “good father” is with male gender identity (Ireland 1993); thus, this stereotype suggests mothers might report greater perceived stigma than do fathers. Given that the literature provides speculation for both directions of gender differences, we do not propose a specific hypothesis regarding gender differences in internalized or experienced PPD stigma.
Dual-Pathway Model of Perceived Stigma
Numerous studies have shown that perceived stigma (internalized and/or experienced) is related to emotional distress in a wide variety of samples (Baxter 1989 – Australian sample; Coffey et al. 1996; Devins et al. 1994 – Canadian sample; Hermann et al. 1990 – British sample). Additionally, two longitudinal studies have found that perceived stigma actually increases depression over time in mentally ill, substance-abusing men (Link et al. 1997) and in parents of special needs children (Mickelson 2001).
The question remains how perceived stigma is connected to mental health outcomes. Mickelson and Williams (2008) argued for a dual-pathway model to explain the association. Specifically, they proposed that internalized perceived stigma (i.e., feelings of shame, deviance) will be related to depression primarily through lower self-esteem and self-efficacy; whereas experienced perceived stigma (i.e., beliefs about how others treat them) will be related to depression primarily through impaired social support. Their rationale for the internalized pathway is found in Corrigan et al.’s (2006) work in which they argue that agreeing with stereotypes held by the public, along with believing that these stereotypes apply to themselves, leads to decreased feelings of self-worth and self-competence. For the experienced pathway, Mickelson and Williams (2008) argue that an individual’s awareness of social stereotypes, as well as actual or anticipated experiences with discrimination, has been shown to negatively impact social relationships, with stigmatized individuals withdrawing or restricting their social activities. In their study of impoverished women, they found support for the dual-pathway model in the link between perceived stigma of poverty and depression symptoms.
For the second aim of the current study, we propose applying the dual-pathway model to understand how perceived stigma is related to reporting PPD symptom for both new mothers and fathers. Specifically, we propose that internalized stigma will be related to PPD symptoms through decrements in parenting efficacy; that is, believing/accepting the stereotypes of not being a good mother or father because you have PPD symptoms may make an individual feel less efficacious in their parenting skills. Research supports this association because general self-efficacy has been linked with perceived stigma (Corrigan et al. 2006) and with PPD symptoms (Zhang and Jin 2014 - Chinese sample). Parenting efficacy is more domain-specific but has also been connected with PPD symptoms, such that lower levels of parenting efficacy are related to higher levels of PPD symptoms (Cutrona and Troutman 1986).
Experienced stigma will be related to PPD symptoms through greater indirect support-seeking from family and friends; that is, if you feel others are looking down on you or treating you differently because of your PPD symptoms, then you may be less likely to directly seek support from them. Again, research has consistently found social support to be connected to both perceived stigma (Boath et al. 2013 – British sample) and PPD symptoms (Collins et al. 1993). In sensitive systems interactions (SSI) theory, Barbee and Cunningham (1995) outlined the importance of the support seeker during supportive interactions. Whereas direct support-seeking is overt and informative of the support seeker’s needs, Barbee and Cunningham argue that indirect support-seeking is passive, subtle, and less informative. Indirect support seekers engage in behaviors such as whining, speaking equivocally about the issue, or repeatedly sighing without providing any useful explanation for what is wrong.
Barbee and Cunningham (1995) theorized that indirect support-seeking is used to avoid embarrassment and to preserve self-esteem for the support seeker. The individual is not specifically requesting support; thus, rejection is not overt and disclosure of potentially risky or embarrassing information is at least initially removed from the support process. Ironically, although indirect support-seeking may be used by the seeker as a form of self-protection, it may actually elicit unsupportive or negative responses from the support provider, which can lead to worse well-being (or, in our case, greater reporting of PPD symptom). Relatedly, Don et al. (2013) found that among first-time parents, indirect support-seeking from one’s spouse was related to greater negative spousal support responses. Based on SSI theory, we argue that experienced perceived PPD stigma will lead individuals to engage in more indirect support-seeking and, as a result, increased PPD symptoms.
Gender Differences in the Dual-Pathway Model
When examining potential gender differences in the dual-pathway model, we turn to the general literature on clinical PPD. Research on predictors of clinical PPD suggest intrapersonal predictors may be stronger for fathers than interpersonal predictors (Kamalifard et al. 2014 – Iranian sample; Matthey et al. 2003 – Australian sample; Morse et al. 2000 – Australian sample). For mothers, a combination of intrapersonal and interpersonal factors predict clinical PPD (Beck 2001; Righetti–Veltema et al. 1998 – Swiss sample; Robertson et al. 2004 – Canadian sample). One potential reason for this gender difference is that women tend to be more relationship-oriented (i.e., communal) whereas men tend to be more agentic (i.e., focused on the self; Helgeson 1994). In other words, men may rely more on their own cognitive resources when dealing with stress than women. Thus, we predict the internalized stigma pathway will be stronger for fathers than the experienced stigma pathway. On the other hand, for mothers, both internalized and experienced stigma pathways should be significant.
The Present Study
Research on perceived PPD stigma typically focuses on its role in help-seeking for mothers only. The current study will examine the process of perceived stigma and PPD symptoms (controlling for prenatal depression symptoms) in both mothers and fathers during the transition to parenthood. Because of conflicting evidence, we do not make a specific gender difference prediction regarding mean levels of internalized and experienced perceived PPD stigma (Research Question 1). We will apply the dual-pathway model (Mickelson and Williams 2008) to the process of PPD stigma. Specifically, we predict internalized PPD stigma will be related to greater PPD symptoms through lower levels of parenting efficacy (Hypothesis 1). Experienced PPD stigma, on the other hand, will be related to greater PPD symptoms through higher levels of indirect support-seeking from family and friends (Hypothesis 2). Finally, based on past clinical PPD research and gender, we predict fathers’ internalized pathway will be stronger than their experienced pathway, whereas mothers will utilize both pathways in the perceived stigma process (Hypothesis 3).
Because one of our goals was to understand how new mothers and fathers differ in perceived stigma and PPD symptoms, only heterosexual married/cohabiting couples were eligible for our study. We also focused on couples pregnant with their first child because the manifestation of PPD symptoms is substantively different in subsequent (i.e., multiparous) births (Gameiro et al. 2008 – Portuguese sample). Moreover, because high-risk and difficult pregnancies can influence PPD symptoms, couples were screened to ensure that only those with relatively low-risk pregnancies were included in our sample. We also sought a homogenous low-risk sample with respect to education and income. In other words, we did not recruit from low-income neighborhoods. Our rationale is that because socioeconomic status (SES) is related to PPD symptoms (Goyal et al. 2010) and our potential mediators (Ali et al. 2005; House et al. 1990), we did not want to confound potential findings with SES. Rather, we feel it is important to first understand perceived PPD stigma during the transition to parenthood for average, low-risk, non-clinical mothers and fathers before proceeding to examine social contextual factors that may moderate these relationships. Finally, because of the strong association between prenatal depression and postpartum depression symptoms (Robertson et al. 2004), all our analyses will control for prenatal depression symptoms.
Method
Participants
The sample was a subset of heterosexual married or cohabitating primiparous couples (i.e., no other biological or adopted children for either individual in the couple) who completed a longitudinal study on the transition to parenthood from pregnancy to 9-months postpartum. The current analyses were based on the 92 couples (N = 184 individuals) who completed the 1 and 4-month postpartum interviews. Other eligibility requirements included that both the expectant mother and father were fluent in English and employed at the time of the baseline interview (third trimester of pregnancy). Participants were recruited from local birthing classes in Northeast Ohio (49.1 %) and across the Unites States through online message boards (50.9 %). As shown in Table 1, fathers were older (M = 29.87 years) than mothers (M = 28.09 years). Also, the majority of both mothers and fathers were White, college educated, and middle-to-upper income. Finally, over half the couples had a baby girl (56.7 %), with most parents (82.7 %) reporting no postpartum health problems with their baby. See Table 1 for additional sample characteristics by gender at 1-month postpartum.
Procedure
Couples agreed to participate in a year-long, longitudinal study called Baby T.I.M.E. (Transitions in Marital Exchanges). Data collection occurred at four time points: (a) during the third trimester of pregnancy (between 24 and 32 weeks of pregnancy) (n = 104 couples), (b) at 1-month postpartum (n = 92 couples), (c) at 4-months postpartum (n = 85 couples), and (d) at 9-months postpartum (n = 83 couples). Participants first completed online questionnaires (either from work or home) and then completed a second portion of the interview within 24 h over the phone with trained interviewers. Participants completed both the online and phone questionnaire independent of their partner; the majority of couples completed their interviews within the same 24-h period of time. The combined online and phone interview took each participant approximately 1 h to complete. Follow-up interviews utilized the same online and telephone interview format. Couples were compensated for each wave of interviews. For purposes of the current study’s aims, we will only be using data from the first two postpartum waves (1 and 4-months) because these were the only waves for which perceived PPD stigma and the proposed mediators were all assessed.
Measures
Sociodemographics
Several demographic characteristics were assessed. Years married was measured as the number of years the couple had been married and/or cohabiting. Age range in this sample was from 18 to 52 years-old and was represented as a continuous variable. Education consisted of five categories: some high school, high school, some college, college, or an advanced degree. Household Income represented total family income at the time of the interview and was categorized as less than $20,000, $20,001–$40,000, $40,001–$60,000, $60,001–$80,000, $80,001–$100,000, $100,001–$120,000, or more than $120,000. Employment status was coded as (1) working (i.e., full-time, part-time, self-employed) or (0) currently not working. Race/ethnicity was self-reported and coded as (1) non-Hispanic White or (0) Other (i.e., African American, Hispanic, Asian, or Other). Baby sex was assessed at 1-month postpartum and coded as (1) female and (0) male. Baby health problems asked whether the baby had health problems at each postpartum wave (yes or no). These variables were included for sample description, as well as possible control variables, because prior research has suggested each has the potential to be related to perceived stigma (Ellison and Hall 2003; O’Mahen et al. 2011 – British sample), social support (Dunkel-Schetter et al. 1996; Green and Rodgers 2001; Mickelson and Kubzansky 2003), self-efficacy (Bandura 1997; Salonen et al. 2009 – Finnish sample), and PPD symptoms (Rich-Edwards et al. 2006; Robertson et al. 2004).
Prenatal Depression Symptoms
These symptoms were assessed during the third trimester interview using the Center for Epidemiologic–Depression Inventory (CES–D; Radloff 1977), which is a well-validated and reliable measure. Participants answered 20 questions assessing their mood over the past week (e.g., “How often have you felt depressed in the past 7 days?”). Responses ranged from 0 [none/rarely (<1 day)] to 3 [most (5–7 days)]; a total prenatal depression score was created by summing scores from the individual items (possible range = 0–60). The scale demonstrated adequate internal consistency for both mothers (α = .87) and fathers (α = .88) at pregnancy. Based on the clinical cut-offs using the CES–D (i.e., a score of 16 or higher; see McDowell 2006, for a review), 23.6 % (n = 22) of mothers and 9.9 % (n = 9) of fathers met the criteria for possible clinical depression. Prenatal depression symptoms were included as a control variable for PPD symptoms in all analyses.
Postpartum Depression Symptoms
To measure postpartum depression symptoms in both mothers and fathers, a modified shortened version of the Postpartum Depression Screening Scale (Beck and Gable 2000) was administered. Participants were asked to report how they felt in the past week on 11 items assessing their postpartum mood state. Example items included “I got anxious over even the littlest things that concerned my baby,” “I felt like I was not the parent I wanted to be,” and “I had trouble sleeping even when the baby was asleep.” Responses ranged from 1 (strongly disagree) to 5 (strongly agree), with higher scores indicating greater PPD symptom reporting. A total PPD symptom score was created for both mothers and fathers by summing the scores from the individual items (possible range = 11–55). The scale demonstrated high internal consistency at both waves of data collection (1-month: αfathers = .86, αmothers = .83; 4-months: αfathers = .81, αmothers = .83).
Perceived Stigma
Perceived stigma of PPD symptoms was measured using eight items reflecting an individual’s perceptions of stigma associated with having postpartum depression symptoms (adapted from Mickelson 2001). For the current analyses, we used perceived stigma scores at 1-month postpartum. Participants were asked to think about their current feelings and to respond by indicating the extent to which they agreed or disagreed with each of the statements using a 5-point scale, ranging from 1 (definitely disagree) to 5 (definitely agree). The eight items tap into the two dimensions of perceived stigma (each consisting of four items): (a) internalized stigma (“I feel that I am odd or abnormal because of the feelings I am having about myself or my baby,” “There have been times when I have felt ashamed because of the feelings I am having about myself or my baby,” “I never feel self-conscious when I am in public with my baby” [reversed scored], and “I never feel embarrassed about the feelings I am having about myself or my baby” [reverse scored]) (α fathers = .61; α mothers = .68) and (b) experienced stigma (“I feel that others look down on me because of how I feel or act towards my baby,” “People treat me differently because of how I feel or act towards my baby,” “I have found that people say negative or unkind things about me behind my back because of how I feel or act towards my baby,” and “I have been excluded from work, school, and/or family functions because of how I feel or act towards my baby”) (α fathers = .64; α mothers = .66). For analytic purposes, mean scores were calculated for internalized stigma and experienced stigma with higher scores indicating greater internalized and experienced stigma (possible ranges = 1–5).
Parenting Efficacy
Parenting efficacy was assessed using the Self-Efficacy for Parenting Tasks measure (Coleman and Karraker 2003). For the current analyses, we used parenting efficacy scores at 1 and 4-months postpartum. The scale included 14 items (e.g., “I am successful in getting my baby to eat on a fairly regular schedule,” and “I am very good at never leaving my baby unattended”). Responses ranged from 1 (disagree strongly) to 6 (agree strongly); a total parenting efficacy score was created by summing scores across the individual items (after reverse coding appropriate items; possible range = 14–84). The scale demonstrated adequate internal consistency for both mothers and fathers (1-month: αfathers = .67; αmothers = .67; 4-months: αfathers = .85; αmothers = .87).
Support Seeking
Indirect support seeking from family and friends was assessed at 1 and 4-months postpartum using an adapted version of Williams and Mickelson’s (2008) measure, which was based on a measure developed by Barbee and Cunningham (1995). The measure includes five items asking participants how often they behaved in a certain way towards six different support sources (mom, dad, siblings, in-laws, other relatives, friends) when looking for support over the past month (e.g. “How often did you come across as sad or down but didn’t exactly state why or give details?”; “How often did you feel like you wanted comfort from them but didn’t tell them why?”). Responses ranged from 0 (not at all) to 4 (very often). A mean score was created across the items for each of the six support sources, and then a mean score was calculated for the five family sources to create a family indirect support-seeking score (possible range = 0–4). If a participant did not have siblings or their parents or in-laws were deceased, their mean score was calculated only for sources with a score. Finally, a sum score was calculated using the mean family score and the friend score; higher scores indicate more indirect support-seeking (possible range = 0–8). Internal consistency was similar to levels in Williams and Mickelson’s (2008) study (1-month: αfathers = .81; αmothers = .82; 4-months: αfathers = .76; αmothers = .81).
Results
Overview of Analyses
We tested the proposed meditational models using the MEDIATE macro for SPSS (Hayes and Preacher 2014). Using MEDIATE allows us to test for multiple mediators with multiple predictors and covariates. Although we make specific predictions about which pathways will be significant for mothers and fathers, MEDIATE tests for all possible indirect effects. MEDIATE reports all direct effects with the outcome and mediators as well as all indirect effects. Preliminary examination of the data revealed that all of the assumptions of multiple regression (i.e., linearity, normality, homogeneity of regressions) were met in the current dataset. Examination of the bivariate correlation matrix did not reveal any problems with multicollinearity (see Table 2). We also bootstrapped the indirect effects using 5,000 replications to address issues of power, and we report the indirect effect, standard error, and 95 % confidence intervals. A significant indirect effect is inferred if the bias-corrected confidence intervals do not include zero (Hayes and Preacher 2014). We examined both a cross-sectional mediational model at 1-month postpartum and a longitudinal mediational model (1-month perceived stigma predicting 4-month postpartum mediators and 4-month PPD symptoms). Due to the interdependence of observations between mothers and fathers, we conducted separate models for mothers and fathers to examine gender differences and tested for significant differences between their parameter estimates.
We tested for differential attrition on major demographic and study variables for participants who dropped out of the study after baseline (pregnancy) and did not return. Chi-square analyses and MANOVAs were conducted separately for mothers and fathers. There were no significant attritional differences in any of the major study variables for mothers or fathers. To test for differential attrition on pregnancy and baby-related variables (including postpartum distress variables), attrition rate was measured for mothers and fathers who dropped out of the study after 1-month postpartum and did not return. There were again no significant attritional differences in any of the pregnancy or postpartum variables for mothers or fathers.
Descriptive Statistics
In order to examine gender differences in the major study variables, we conducted a MANCOVA (with gender as the fixed factor). Based on bivariate correlations with the major study variables by gender (see Table 2), we controlled for race/ethnicity (Mothers: r = −.26, p < .05 with 4-month PPD symptoms, r = −.22, p < .05 with internalized stigma at 1-month postpartum), education (Mothers: r = .23, p < .05 with internalized stigma at 1-month postpartum, r = −.25, p < .05 with parenting efficacy at 1-month postpartum, r = −.41, p < .001 with parenting efficacy at 4-months postpartum; Fathers: r = −.24, p < .05 with parenting efficacy at 1-month postpartum), and marital status (Mothers: r = .43, p < .001 with prenatal depression symptoms, r = .30, p < .01 with 4-month PPD symptoms). The overall multivariate test for gender differences was significant, F (11, 124) = 3.62, p < .001, ηp2 = .24. Examination of Bonferroni pairwise comparisons (adjusted for covariates) revealed significant gender differences for most of the major study variables.
As stated previously, due to conflicting speculation, we did not make a prediction regarding gender differences in perceived stigma of PPD. As shown in Table 3, mothers reported significantly greater internalized PPD stigma than did fathers at 1 and 4-months postpartum. However, mothers and fathers did not differ in their reports of experienced PPD stigma at 1-month or 4-months postpartum. With respect to the other main study variables, mothers reported significantly more parenting efficacy at 4-months than did fathers; there was no gender difference at 1-month postpartum. Mothers reported significantly more indirect support-seeking from family and friends than did fathers at both 1 and 4-months postpartum. With respect to depression symptoms, mothers reported significantly more prenatal depression symptoms and PPD symptoms at both 1 and 4-months postpartum.
We also examined changes in the major study variables over time and found that PPD symptoms significantly declined from 1 to 4-months postpartum for both mothers, t(81) = 5.05, p < .001, and fathers, t(81) = 4.03, p < .001, whereas parenting efficacy significantly increased from 1 to 4-months postpartum for both mothers, t(83) = −3.52, p = .001, and fathers, t(83) = −3.14, p = .002. Indirect support-seeking significantly declined from 1 to 4-months postpartum for fathers, t(72) = 2.25, p = .03, but not did not change for mothers, t(72) = 1.54, p = .13. Finally, there were no significant changes in either internalized or experienced stigma from 1 to 4-months postpartum for mothers or fathers.
Dual-Pathway Model for Mothers
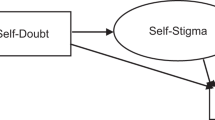
All analyses include prenatal depression symptoms as a control variable. Cross-sectional analyses at 1-month postpartum revealed that internalized stigma directly predicted 1-month PPD symptoms, parenting efficacy, and indirect support-seeking from family and friends. In addition, there was evidence of partial mediation through both pathways. Specifically, bootstrapped estimates of the indirect effects revealed both parenting efficacy (z = 1.20, SE = .44, 95 % CI [.50, 2.26]) and indirect support-seeking from family and friends (z = .58, SE = .32, 95 % CI [.11, 1.42]) emerged as significant mediators between internalized stigma and maternal PPD symptoms at 1-month postpartum (see Fig. 1). In other words, the more internalized stigma mothers felt at 1-month postpartum regarding their PPD symptoms, the less parenting efficacy they reported and the more indirect support-seeking from family and friends, which in turn predicted more PPD symptoms at 1-month postpartum. Experienced stigma showed no direct or indirect associations with 1-month PPD symptoms.

Cross-sectional mediation model at 1-month postpartum. Mothers’ path estimates are bolded above the respective paths and fathers’ path estimates are below the respective paths and not bolded. Prenatal depression symptoms were included in the model for both mothers and fathers. These paths to the mediators and outcome are not represented in the figure for ease of presentation. (The authors will provide the model with this variable and the pathway estimates, upon request). *p < .05. **p < .01. ***p < .001
Longitudinal analyses revealed that internalized stigma at 1-month postpartum directly predicted 4-month PPD symptoms. In addition, there was evidence of partial mediation through parenting efficacy at 4-months postpartum. Specifically, bootstrapped estimates of the indirect effects revealed 4-month parenting efficacy (z = .34, SE = .21, 95 % CI [.03, .90]) emerged as a significant mediator between 1-month internalized stigma and maternal PPD symptoms at 4-month postpartum (see Fig. 2). In other words, the more internalized stigma mothers felt at 1-month postpartum regarding their PPD symptoms, the less parenting efficacy they reported at 4-months postpartum, which in turn predicted more PPD symptoms at 4-months postpartum. Experienced stigma at 1-month postpartum showed no direct or indirect effect on 4-month PPD symptoms.

Longitudinal mediation model. Mothers’ path estimates are bolded above the respective paths and fathers’ path estimates are below the respective paths and not bolded. Prenatal depression symptoms were included in the model for both mothers and fathers. These paths to the mediators and outcome are not represented in the figure for ease of presentation. (The authors will provide the model with this variable and the pathway estimates, upon request). * p < .05. ** p < .01. *** p < .001
Dual-Pathway Model for Fathers
As with mothers, all analyses include prenatal depression symptoms as a control variable. Cross-sectional analyses revealed that experienced stigma directly predicted 1-month PPD symptoms and parenting efficacy. In addition, bootstrapped estimates of the indirect effect revealed parenting efficacy (z = 1.11, SE = .58, 95 % CI [.24, 2.5]) emerged as a significant mediator between experienced stigma and paternal PPD symptoms at 1-month postpartum (see Fig. 1). Specifically, the more experienced stigma fathers felt at 1-month postpartum regarding their PPD symptoms, the less parenting efficacy they reported and, in turn, the more PPD symptoms they reported at 1-month postpartum. Internalized stigma showed no direct or indirect associations with 1-month PPD symptoms.
Longitudinal analyses revealed that experienced stigma at 1-month postpartum did not significantly predict PPD symptoms at 4 months (p = .095) but did significantly predict parenting efficacy at 4-months postpartum. In addition, bootstrapped estimates of the indirect effect revealed parenting efficacy at 4-months postpartum (z = .72, SE = .44, 95 % CI [.06, 1.88]) emerged as a significant mediator between experienced stigma at 1-month postpartum and paternal PPD symptoms at 4-months postpartum (see Fig. 2). Specifically, the more experienced stigma fathers felt at 1-month postpartum regarding their PPD symptoms, the less parenting efficacy they reported at 4-months postpartum, and, in turn, the more PPD symptoms they reported at 4-months postpartum. Internalized stigma at 1-month postpartum showed no direct or indirect association with 4-month PPD symptoms.
Gender Differences in Dual-Pathway Models
To test Hypothesis 3 regarding gender differences in the dual-pathway model, we examined slope (i.e. path) differences between mothers’ and fathers’ cross-sectional and longitudinal pathways (both direct and indirect). Significant gender differences in slopes emerged only with the 1-month cross-sectional model. Contrary to our prediction, at 1-month postpartum, the pathways between internalized perceived stigma and parenting efficacy, t(164) = 2.02, p = .04, and PPD symptoms, t(164) = 3.36, p = .001, were significantly stronger for mothers than for fathers, (in fact, the pathways were not even significant in the model for fathers). Additionally, contrary to our prediction, we found that at 1-month postpartum the pathways between experienced stigma and parenting efficacy, t(164) = 2.15, p = .03, and PPD symptoms, t(164) = 2.62, p = .01, were significantly stronger for fathers than for mothers (in fact, the pathways were not even significant in the model for mothers).
Discussion
Our study is the first, to our knowledge, to examine the dual-pathway model of perceived stigma and PPD symptoms in first-time parents. New mothers reported significantly greater internalized PPD stigma, but did not differ from new fathers on experienced PPD stigma. With respect to the dual-pathway, we found longitudinal support for the internalized stigma pathways for mothers, whereas for fathers, experienced stigma predicted PPD symptoms through parenting efficacy only. Although our results provided only partial support for our hypotheses, we found some interesting and important differences between new mothers and fathers in the stigma process.
A Dual-Pathway Model of Perceived PPD Stigma?
Our study sought to test the dual-pathway model of perceived stigma (Mickelson and Williams 2008) in the context of PPD symptoms and the transition to parenthood. Although we were not able to support the dual-pathway model as proposed by Mickelson and Williams (2008), we found that the pathways for internalized and experienced stigma were different for mothers and fathers. Considering both mothers’ and fathers’ models, we found the strongest evidence for parenting efficacy as a mediator in the link between perceived stigma and PPD symptoms – although mothers and fathers differed in which aspect of perceived stigma most impacted parenting efficacy. These results suggest that, at least for new parents, perceptions of stigma related to PPD symptoms are primarily impacting new parents’ PPD symptom reporting by decreasing their feelings of competence as a parent. Interestingly, the specific type of perceived stigma impacting parenting efficacy differs for mothers and fathers. Overall though, for both mothers and fathers, it appears that stigma related to their PPD symptoms make them question their capabilities to parent successfully. This finding is supported by other research that has found a link between perceived stigma and general self-efficacy (Corrigan et al. 2006). Additionally, this result is supported by research showing that those suffering from clinical PPD actually exhibit poorer parenting behaviors (e.g., detachment from baby, delayed responding to baby, less healthy feeding and sleeping practices; Paulson et al. 2006). Future research should examine whether actual parenting behaviors also mediate the relationship between perceived stigma and PPD symptoms.
Interpersonal relationships seem to only play a concurrent role with internalized stigma for mothers. Specifically, mothers appear to seek support through a more subtle form of communication when they feel embarrassed about their PPD symptoms. Due to the cross-sectional nature of the findings, perceived stigma may be driving an increase in maternal indirect support-seeking strategies or the ramifications of indirect support-seeking (e.g., rejection or ignoring of support cues) may be increasing perceptions of stigma.
Given the lack of longitudinal results with indirect support-seeking for both mothers and fathers, it does not appear that beliefs about how others are treating them based on their PPD symptoms are actually influencing how they seek support from family and friends. Because Mickelson and Williams (2008) found evidence that experienced stigma was related to decreased perceptions of support availability, it may be how individuals seek support from family and friends is not impacted as much as one’s perceptions of availability (which we did not measure in the current study). Alternately, regardless of one’s perceived stigma experiences, family and friends may provide unsolicited support after the baby’s birth. Finally, experienced stigma may instead be related to negative interactions with family and friends. Perceiving that people are treating you differently because of your PPD symptoms may be due to actual negative interactions with others, or may lead one to act defensively with others which increases the likelihood of negative interactions. Future research should examine whether perceived support availability and/or negative interactions are more likely to act as mediators between experienced stigma and PPD symptoms for new parents.
Gender Differences in Perceived Stigma
The other main aim of our study was to examine gender differences in perceived stigma and the dual-pathway model. Prior theory provided conflicting speculation for whether mothers or fathers would report more perceived PPD stigma. We found mothers reported significantly more internalized stigma than did fathers, but mothers and fathers did not differ on experienced stigma. Mothers may be more embarrassed and ashamed about their PPD symptoms than are fathers, but they perceive similar low levels of stigma experiences with others. The difference in internalized stigma may be related to the continued belief in society that motherhood is still closely tied to female identity (Ireland 1993), whereas the emphasis on men being more involved, good fathers has only recently been increasing (Wall and Arnold 2007). Therefore, when women experience negative emotions related to being a mother, these feelings go against lifelong gender socialization into the role of mother. These negative feelings may be taboo to some extent in the new mother’s mind, which leads to feelings of embarrassment and shame. Fathers, on the other hand, may be forgiven if the parenting role is overwhelming in the beginning because it is believed to be less “natural” for them. As a result, they may feel less embarrassment and shame for experiencing negative emotions connected with being a new parent. Future research should examine if these gender differences in internalized PPD stigma continue over the longer course of the transition to parenthood. In other words, if PPD symptoms are still experienced 6 months or 9 months after the birth of the baby, do mothers still perceive more internalized stigma than fathers? Or, do fathers start to feel similar levels of stigma because they should have adjusted to their father role by then?
In addition to mean gender differences in internalized PPD stigma, we found two primary gender differences in the dual-pathway model. First, only the internalized stigma pathways were significant for mothers and the mediation was partial because a direct link was found between internalized stigma and PPD symptoms (both cross-sectionally and longitudinally). Second, experienced stigma showed a significant indirect effect on PPD symptoms through parenting efficacy for fathers. Taken together, these two differences are both supportive and contradictory of our predictions. We predicted the intrapersonal pathway (i.e., parenting efficacy) would be more important for fathers than the interpersonal pathway (i.e., indirect support-seeking). We did find parenting efficacy was the primary mediating mechanism for perceived stigma and PPD symptoms for fathers but with experienced rather than internalized stigma. Mothers, on the other hand, only showed evidence for the internalized stigma pathways, whereas we predicted mothers would show evidence for the dual pathways of internalized and experienced stigma.
Why experienced stigma for fathers and internalized stigma for mothers? We have already discussed why we believe mothers internalize stigma more than fathers do. Feelings of shame and embarrassment can lead one to question their competence as a parent, thereby increasing PPD symptoms. Rather, for fathers, perceived stigma experiences with others appear to be impacting their beliefs about their parenting skills and, in turn, their PPD symptoms. Thus, although mothers and fathers do not differ on mean levels of experienced stigma, fathers may be more self-conscious and sensitive to how others are treating them. If they believe others are looking down on them or judging them as a bad father, it may lead them to question their own abilities as a father, which could lead to increased PPD symptoms. Future research is needed to replicate these gender differences in a larger sample and over the longer term transition to parenthood because there may be something unique about this early transition to parenthood (i.e., the first 4 months) where experienced PPD stigma is impacting fathers’ parenting efficacy.
Limitations and Future Research Directions
Several limitations in the current study need to be considered when interpreting our results. Our sample is homogenous with regard to socioeconomic status and race/ethnicity, and our results apply specifically to non-clinical, low-risk first-time parents. Although it is important to show that the challenges of perceived stigma of PPD are present in the “average” parent, we acknowledge that the processes studied may be stronger (or different) in other populations. Research has established the transition to parenthood is considerably more stressful for parents of low socioeconomic status (Goyal et al. 2010); hence, it is likely that a sample with a greater proportion of disadvantaged parents (e.g., those of low social class or with special needs children) may reveal a different pattern of results with the dual-pathway model. Future research needs to examine these issues among more diverse parents.
Future research should also examine whether the dual-pathway model is different at various stages of the transition to parenthood. It is possible that internalized and experienced PPD stigma may manifest in different ways later during the baby’s first year. Our study focused on the unique experience during the early transition to parenthood. Relatedly, although we tested a longitudinal model, it was not fully lagged (i.e., our mediators and outcome were measured at the same wave). Future research should examine fully lagged longitudinal models in order to determine causal ordering of the variables in the dual-pathway model. We also found the alphas for internalized and experienced stigma to be a littler lower (but still acceptable) than those found in other research using this instrument (Mickelson and Williams 2008). It is possible some of the stigma items may be more or less relevant for this particular population; future research should determine whether these alphas are a persistent issue or simply an artifact of the current sample.
Finally, although our study focused on gender differences and sampled couples, we did not examine Actor-Partner Interdependence Model (APIM; Kashy and Kenny 2000) effects. It is possible a partner’s perceived stigma may have an impact on the actor’s PPD symptoms and mediating mechanisms; however, we did not have the necessary sample size to conduct APIM analyses. Moreover, we did not find any evidence husbands’ and wives’ perceived stigma or PPD symptoms (nor most of the mediators) were correlated with each other. Even so, future research should examine the APIM approach to determine whether it is appropriate for modeling perceived stigma processes.
Practice Implications
The results from our study are preliminary and need to be replicated and expanded; however, the present results provide evidence that the perceived stigma attached to PPD by new parents is likely to have important consequences on their well-being. Because both mothers and fathers continue to feel the taboo of postpartum depression, pediatric and obstetric doctors need to acknowledge to new parents the prevalence (and normalcy) of postpartum depression symptoms and encourage them to seek help for these feelings—particularly for fathers who may be especially sensitive to how family and friends are reacting to their PPD symptoms. Furthermore, therapists need to explore how perceptions of stigma may be impacting new parents’ beliefs about their ability to parent. Finally, it is important to develop interventions aimed at decreasing the taboo associated with postpartum depression for both new mothers and fathers in order to break down the barriers to seeking professional help. In doing so, mothers and fathers may improve their views of themselves as parents and learn effective strategies for seeking support from family and friends as they transition to parenthood.
Conclusion
We examined gender differences in the dual-pathway model of perceived stigma and PPD symptoms during the early transition to parenthood in a non-clinical low-risk sample of U.S. mothers and fathers. Mothers reported significantly greater internalized PPD stigma, but they did not differ from fathers on experienced PPD stigma. We found only limited support for the dual-pathway model: parenting efficacy and indirect support-seeking were only significant cross-sectionally and for mothers. We also found that only the internalized stigma pathways were significant for mothers, whereas for fathers only experienced stigma predicted PPD symptoms through parenting efficacy. Overall, our results show that perceived stigma primarily impacts mothers’ and fathers’ PPD symptoms through their beliefs about their ability to parent successfully, as opposed to their strategies for seeking support from family and friends. Efforts at diminishing the stigma associated with PPD are likely to improve the chances a new parent will seek professional help for their symptoms and, as a result, enhance their beliefs in their ability to be a good parent.
References
Ali, S. R., McWhirter, E. H., & Chronister, K. M. (2005). Self-efficacy and vocational outcome expectations for adolescents of lower socioeconomic status: A pilot study. Journal of Career Assessment, 13, 40–58. doi:10.1177/1069072704270273.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders: DSM-5. Washington, D.C: American Psychiatric Association. doi:10.1176/appi.books.9780890425596.
Bandura, A. (1997). Self-efficacy: The exercise of control. New York: Freeman.
Barbee, A. P., & Cunningham, M. R. (1995). An experimental approach to social support communications: Interactive coping in close relationships. In B. R. Burleson (Ed.), Communication yearbooks/18 (pp. 381–413). Thousand Oaks: Sage.
Baxter, C. (1989). Investigating stigma as stress in social interactions of parents. Journal of Mental Deficiency Research, 33, 455–466. doi:10.1111/j.1365-2788.1989.tb01501.x.
Beck, C. T. (2001). Predictors of postpartum depression: An update. Nursing Research, 50, 275–285.
Beck, C. T., & Gable, R. K. (2000). Postpartum Depression Screening Scale: Development and psychometric testing. Nursing Research, 49, 272–282. doi:10.1097/00006199-200009000-00006.
Boath, E. H., Henshaw, C., & Bradley, E. (2013). Meeting the challenges of teenage mothers with postpartum depression: Overcoming stigma through support. Journal of Reproductive and Infant Psychology, 31, 352–369. doi:10.1080/02646838.2013.800635.
Coffey, P., Leitenberg, H., Henning, K., Turner, T., & Bennett, R. T. (1996). Mediators of the long-term impact of child sexual abuse: Perceived stigma, betrayal, powerlessness, and self-blame. Child Abuse and Neglect, 20, 447–455. doi:10.1016/0145-2134(96)00019-1.
Coleman, P. K., & Karraker, K. H. (2003). Maternal self-efficacy beliefs, competence in parenting, and toddlers’ behavior and developmental status. Infant Mental Health Journal, 24, 126–148. doi:10.1002/imhj.10048.
Collins, N. L., Dunkel-Schetter, C., Lobel, M., & Scrimshaw, S. C. M. (1993). Social support in pregnancy: Psychosocial correlates of birth outcomes and postpartum depression. Journal of Personality and Social Psychology, 65, 1243–1258. doi:10.1037/0022-3514.65.6.1243.
Corrigan, P. W., & Calabrese, J. D. (2005). Strategies for assessing and diminishing self-stigma. In P. W. Corrigan (Ed.), On the stigma of mental illness: Practical strategies for research and social change (pp. 239–256). Washington, DC: American Psychological Association.
Corrigan, P. W., Watson, A. C., & Barr, L. (2006). The self-stigma of mental illness: Implications for self-esteem and self-efficacy. Journal of Social and Clinical Psychology, 25, 875–884. doi:10.1521/jscp.2006.25.8.875.
Crandall, C. S. (1991). AIDS-related stigma and the lay sense of justice. Contemporary Social Psychology, 15, 66–67.
Cutrona, C. E., & Troutman, B. R. (1986). Social support, infant temperament, and parenting self-efficacy: A mediational model of postpartum depression. Child Development, 57, 1507–1518. doi:10.2307/1130428.
Davey, S. J., Dziurawiec, S., & O’Brien-Malone, A. (2006). Men’s voices: Postnatal depression from the perspective of male partners. Qualitative Health Research, 16, 206–220. doi:10.1177/1049732305281950.
Devins, G. M., Stam, H., & Koopmans, J. P. (1994). Psychological impact of laryngectomy mediated by perceived stigma and illness intrusiveness. Canadian Journal of Psychiatry, 39, 608–616.
Don, B. P., Mickelson, K. D., & Barbee, A. (2013). Indirect support seeking and perceptions of spousal support: A reciprocal relationship? Personal Relationships, 20, 655–668. doi:10.1111/pere.12006.
Dunkel-Schetter, C., Sagrestano, L. M., Feldman, P., & Killingsworth, C. (1996). Social support and pregnancy: A comprehensive review focusing on ethnicity and culture. In G. R. Pierce, B. R. Sarason, & I. G. Sarason (Eds.), Handbook of social support and the family (pp. 375–412). New York: Plenum Press.
Edward, K., Castle, D., Mills, C., Davis, L., & Casey, J. (2015). An integrative review of paternal depression. American Journal of Men's Health, 9, 26–34. doi:10.1177/1557988314526614.
Ellison, M. A., & Hall, J. E. (2003). Social stigma and compounded losses: Quality-of- life issues for multiple-birth families. Fertility and Sterility, 80, 405–414. doi:10.1016/S0015-0282(03)00659-0.
Gameiro, S., Moura-Ramos, M., & Canavarro, C. M. (2008). Maternal adjustment to the birth of a child: Primiparity versus multiparity. Journal of Reproductive and Infant Psychology, 23, 1–18. doi:10.1080/02646830802350898.
Goffman, E. (1963). Stigma: Notes on the management of spoiled identity. Englewood Cliffs: Prentice.
Goodman, J. H. (2004). Paternal postpartum depression, its relationship to maternal postpartum depression, and implications for family health. Journal of Advanced Nursing, 45, 26–35. doi:10.1046/j.1365-2648.2003.02857.x.
Goyal, D., Gay, C., & Lee, K. A. (2010). How much does low socioeconomic status increase the risk of prenatal and postpartum depressive symptoms in first-time mothers? Women's Health Issues, 20, 96–104. doi:10.1016/j.whi.2009.11.003.
Green, B. L., & Rodgers, A. (2001). Determinants of social support among low-income mothers: A longitudinal analysis. American Journal of Community Psychology, 29, 419–441. doi:10.1023/A:1010371830131.
Hayes, A. F., & Preacher, K. J. (2014). Statistical mediation analysis with a multicategorical independent variable, 67, 451–470. British Journal of Mathematical and Statistical Psychology, 67, 451–470. doi:10.1111/bmsp.12028.
Helgeson, V. S. (1994). Relation of agency and communion to well-being: Evidence and potential explanations. Psychological Bulletin, 116, 412–428. doi:10.1037/0033-2909.116.3.412.
Hermann, B. P., Whitman, S., Wyler, A. R., Anton, M. T., & Vanderzwagg, R. (1990). Psychosocial predictors of psychopathology in epilepsy. British Journal of Psychiatry, 156, 98–105. doi:10.1192/bjp.156.1.98.
Horowitz, J. A., & Goodman, J. H. (2005). Identifying and treating postpartum depression. Journal of Obstetric, Gynecologic, & Neonatal Nursing, 34, 264–273. doi:10.1177/0884217505274583.
House, J. S., Kessler, R. C., & Herzog, A. R. (1990). Age, socioeconomic status, and health. The Milbank Quarterly, 68, 383–411. doi:10.2307/3350111.
Ireland, M. S. (1993). Reconceiving women: Separating motherhood from female identity. New York: Guilford Press.
Jones, E. E., Farina, A., Hastorf, A. H., Markus, H., Miller, D. T., & Scott, R. A. (1984). Social stigma: The psychology of marked relationships. New York: Freeman.
Kamalifard, M., Hasanpoor, S., Kheiroddin, J., Panahi, S., & Payan, S. B. (2014). Relationship between fathers’ depression and perceived social support and stress in postpartum period. Journal of Caring Sciences, 3, 57–66. doi:10.5681/jcs.2014.007.
Kashy, D. A., & Kenny, D. A. (2000). The analysis of data from dyads and groups. In H. Reis & C. M. Judd (Eds.), Handbook of research methods in social psychology (pp. 451–477). New York: Cambridge University Press.
Link, B. G., Struening, E. L., Rahav, M., Phelan, J. C., & Nuttbrock, L. (1997). On stigma and its consequences: Evidence from a longitudinal study of substance abuse. Journal of Health and Social Behavior, 38, 177–190. doi:10.2307/2955424.
Link, B. G., Struening, E. L., Neese-Todd, S., Asmussen, S., & Phelan, J. C. (2001). Stigma as a barrier to recovery: The consequences of stigma for self-esteem of people with mental illnesses. Psychiatric Services, 52, 1621–1626. doi:10.1176/appi.ps.52.12.1621.
Matthey, S., Barnett, B., Howie, P., & Kavanagh, D. J. (2003). Diagnosing postpartum depression in mothers and fathers: Whatever happened to anxiety? Journal of Affective Disorders, 74, 139–147. doi:10.1016/S0165-0327(02)00012-5.
Mauthner, N. S. (2002). The darkest days of my life: Stories of postpartum depression. Cambridge: Harvard University Press.
McCoughlin, J. (2013). Stigma associated with postnatal depression: A literature review. British Journal of Midwifery, 21, 784–791. doi:10.12968/bjom.2013.21.11.784.
McDowell, I. (2006). Measuring health: A guide to rating scales and questionnaires. New York: Oxford Press.
Melrose, S. (2010). Paternal postpartum depression: How can nurses begin to help? Contemporary Nurse, 34, 199–210. doi:10.5172/conu.2010.34.2.199.
Mickelson, K. D. (2001). Perceived stigma, social support, and depression. Personality and Social Psychology Bulletin, 27, 1046–1056. doi:10.1177/0146167201278011.
Mickelson, K. D., & Kubzansky, L. D. (2003). Social distribution of social support: The mediating role of life events. American Journal of Community Psychology, 32, 265–281. doi:10.1023/B:AJCP.0000004747.99099.7e.
Mickelson, K. D., & Williams, S. L. (2008). Perceived stigma of poverty and psychological distress: Examination of interpersonal and intrapersonal mediators. Journal of Social and Clinical Psychology, 27, 903–930. doi:10.1521/jscp.2008.27.9.903.
Morse, C. A., Buist, A., & Durkin, S. (2000). First-time parenthood: Influences on pre- and postnatal adjustment in fathers and mothers. Journal of Psychosomatic Obstetrics & Gynecology, 21, 109–120.
O’Mahen, H. A., Henshaw, E., Jones, J. M., & Flynn, H. A. (2011). Stigma and depression during pregnancy: Does race matter? The Journal of Nervous and Mental Disease, 199, 257–262. doi:10.1097/NMD.0b013e3182125b82.
Paulson, J. F., & Bazemore, S. D. (2010). Prenatal and postpartum depression fathers and its association with maternal depression. Journal of American Medical Association, 303, 1961–1969. doi:10.1001/jama.2010.605.
Paulson, J. F., Dauber, S., & Leiferman, J. A. (2006). Individual and combined effects of postpartum depression in mothers and fathers on parenting behavior. Pediatrics, 118, 659–668. doi:10.1542/peds.2005-2948.
Radloff, L. S. (1977). The CES–D Scale: A self-report depression scale for research in the general population. Applied Psychological Measurement, 1, 385–401. doi:10.1177/014662167700100306.
Rich-Edwards, J. W., Kleinman, K., Abrams, A., Harlow, B. L., McLaughlin, T. J., Joffe, H., … Gillman, M. W. (2006). Sociodemographic predictors of antenatal and postpartum depressive symptoms among women in a medical group practice. Journal of Epidemiology & Community Health, 60, 221–227. doi:10.1136/jech.2005.039370.
Righetti–Veltema, M., Conne-Perreard, E., Bousquet, A., & Manzano, J. (1998). Risk factors and predictive signs of postpartum depression. Journal of Affective Disorders, 49, 167–180. doi:10.1016/S0165-0327(97)00110-9.
Robertson, E., Grace, S., Wallington, T., & Stewart, D. E. (2004). Antenatal risk factors for postpartum depression: A synthesis of recent literature. General Hospital Psychiatry, 26, 289–295. doi:10.1016/j.genhosppsych.2004.02.006.
Salonen, A. H., Kaunonen, M., Astedt-Kurki, P., Jarvenpaa, A., Isoaho, H., & Tarkka, M. (2009). Parenting self-efficacy after birth. Journal of Advanced Nursing, 65, 2324–2336. doi:10.1111/j.1365-2648.2009.05113.x.
Taylor, V. (1996). Rock-a-by Baby: Feminism, self-help, and postpartum depression. New York: Routledge.
Wall, G., & Arnold, S. (2007). How involved is involved fathering?: An exploration of the contemporary culture of fatherhood. Gender & Society, 21, 508–527. doi:10.1177/0891243207304973.
Watson, A. C., Corrigan, P. W., Larson, J. E., & Sells, M. (2007). Self-stigma in people with mental illness. Schizophrenia Bulletin, 33, 1312–1318. doi:10.1093/schbul/sbl076.
Werner, E., Miller, M., Osborne, L. M., Kuzava, S., & Monk, C. (2015). Preventing postpartum depression: Review and recommendations. Archives of Women’s Mental Health, 18, 41–60. doi:10.1007/s00737-014-0475-y.
Williams, S. L., & Mickelson, K. D. (2008). A paradox of support seeking and social rejection among the stigmatized. Personal Relationships, 15, 493–509. doi:10.1111/j.1475-6811.2008.00212.x.
Zhang, Y., & Jin, S. (2014). The impact of social support on postpartum depression: The mediator role of self-efficacy. Journal of Health Psychology. doi:10.1177/1359105314536454.
Author Note
The current study was supported by a grant to the first author from the Ohio Board of Regents.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Mickelson, K.D., Biehle, S.N., Chong, A. et al. Perceived Stigma of Postpartum Depression Symptoms in Low-Risk First-Time Parents: Gender Differences in a Dual-Pathway Model. Sex Roles 76, 306–318 (2017). https://doi.org/10.1007/s11199-016-0603-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11199-016-0603-4