
Abstract
Nearly 20 % of mothers will experience an episode of major or minor depression within the first 3 months postpartum, making it the most common complication of childbearing. Postpartum depression (PPD) is significantly undertreated, and because prospective mothers are especially motivated for self-care, a focus on the prevention of PPD holds promise of clinical efficacy. This study is a qualitative review of existing approaches to prevent PPD. A PubMed search identified studies of methods of PPD prevention. The search was limited to peer-reviewed, published, English-language, randomized controlled trials (RCTs) of biological, psychological, and psychosocial interventions. Eighty articles were initially identified, and 45 were found to meet inclusion criteria. Eight RCTs of biological interventions were identified and 37 RCTs of psychological or psychosocial interventions. Results were mixed, with 20 studies showing clear positive effects of an intervention and 25 showing no effect. Studies differed widely in screening, population, measurement, and intervention. Among biological studies, anti-depressants and nutrients provided the most evidence of successful intervention. Among psychological and psychosocial studies, 13/17 successful trials targeted an at-risk population, and 4/7 trials using interpersonal therapy demonstrated success of the intervention versus control, with a further two small studies showing trends toward statistical significance. Existing approaches to the prevention of PPD vary widely, and given the current literature, it is not possible to identify one approach that is superior to others. Interpersonal therapy trials and trials that targeted an at-risk population appear to hold the most promise for further study.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
There are over four million live births each year in the USA. Nearly 800,000—or 20 %—of these mothers will experience an episode of major or minor depression within the first 3 months postpartum (Marcus et al. 2003). This makes depression the most common complication of childbearing (Grace et al. 2003), far above both gestational diabetes (3–8 %) (Dabelea et al. 2005) and preterm birth (12.3 %) (Saigal and Doyle 2008). Maternal depression affects the entire family; it is associated with marital discord and impaired occupational and social functioning, as well as with maternal–infant interactions characterized by disengagement, hostility, and intrusion (Cicchetti et al. 1998; Grace et al. 2003; Kurstjens and Wolke 2001). Moreover, studies have consistently demonstrated the deleterious effects of postpartum depression (PPD) on cognitive and emotional development during infancy and later childhood (Zhu et al. 2014; Conroy et al. 2012).
Researchers are only at the beginning stages of discovering biological factors that may contribute to the etiology of postpartum depression, but there are numerous known psychological and social risk factors. Previous meta-analyses have identified 15: (1) lower social class, (2) life stressors during pregnancy, (3) complicated pregnancy/birth, (4) difficult relationship with family or partner, (5) lack of support from family or friends, (6) prior history of psychopathology (depression, anxiety), (7) chronic stressors postpartum (this can include problems with child care and difficult infant temperament), (8) unemployment/instability, (9) unplanned pregnancy, (10) ambivalence over becoming a pregnant, (11) poor relationship with own mother, (12) history of sexual abuse, (13) lack of a confidante, (14) bottle feeding, and (15) depression during pregnancy, with the last generally acknowledged to be the strongest predictor of PPD (Beck 2001; O'Hara and Swain 1996; Richards 1990; Seguin et al. 1999). Recent research on the biological risk factors includes studies on oxytocin (Skrundz et al. 2011) and inflammatory markers (Osborne and Monk 2013).
Postpartum depression is significantly undertreated. Many women feel that depression at what “ought” to be a joyful time is shameful, and others are influenced by society’s general stigma concerning mental health care. In addition, those women who do seek treatment often hesitate to take psychotropic medications when breastfeeding, despite substantial evidence of their relative safety (Beck 2001; Goodman 2009; Cott and Wisner 2003; Freeman 2007).
Given the public health relevance of PPD, its well-characterized psychological risk factors, and the substantial barriers to care once women become ill, a focus on the prevention of PPD holds tremendous potential for clinical efficacy. In particular, prospective mothers are especially motivated for self-care (Kost et al. 1998) and are already in frequent contact with health care providers (Beck 2001). Here, we offer a critical review of existing approaches to PPD prevention, with the dual aim of identifying effective treatment components across many modalities and identifying treatment gaps that may be amenable to novel interventions.
Methods
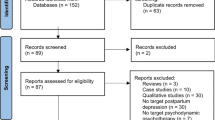
The literature review began with a PubMed search conducted by two authors (Werner and Miller, both doctoral-level clinical psychologists with specialized perinatal research training) and completed in April 2013. Figure 1 contains a flow chart outlining the search strategy. The search was limited to peer-reviewed, published, English-language, randomized controlled trials (RCTs) of biological, psychological, and psychosocial interventions. Moreover, only studies of methods of prevention of PPD (rather than those designed to examine a treatment for PPD) were included. To be included, studies needed to have some therapeutic components (at least one individual or group session with a therapist or trained facilitator). Studies that covered interventions that were purely educational (i.e., booklet or video with no human intervention) as well as those delivered by primary care practitioners without specialty training were excluded, chiefly because of space constraints. The search was not limited by date of publication, sample size, or whether the full text was available online. Four separate searches were combined, using the terms (1) prenatal, pregnancy, pregnant, antenatal, postnatal, postpartum, perinatal; (2) depression, mood; (3) prevention; and (4) intervention. Eighty potential articles were identified. Abstracts were reviewed by Werner and Miller, and 16 did not meet inclusion criteria and were eliminated. Werner and Miller then reviewed full text of the remaining 64 articles, and reference sections of these articles were cross-checked for additional material. After full-text review, an additional 19 articles did not meet inclusion criteria. A total of 45 trials were identified that met inclusion and exclusion criteria.

Flow chart of the study
The articles reviewed use a variety of screening instruments to identify risk. Each instrument generates a score on a particular scale; when a participant scores at or above a cutoff point, risk of clinically significant depression is assumed to be present. The performance (sensitivity and specificity) of each instrument depends critically on the cutoff point chosen. The three most commonly used are the Edinburgh Postnatal Depression Scale (EPDS), the Center for Epidemiologic Studies Depression Scale (CES-D), and the Predictive Index for Postpartum Depression (PIPD). The EPDS (Cox et al. 1987) was developed to assess symptoms of PPD, and the CES-D was designed as a screening tool for determining the severity level of depression symptoms. They are commonly used to determine risk for PPD. Their predictive value, when administered during pregnancy, is likely related to the fact that prenatal depression serves as a strong predictor of PPD (Beck 1996; Eberhard‐Gran et al. 2001; Radloff 1977; Thomas et al. 2001). The PIPD, a 17-item risk survey developed and validated by Cooper et al. (1996), is a screening instrument specifically designed to predict PPD. The specificity and sensitivity of this scale are limited, and at a score of 27 or more (score range = 0–63), the risk of postpartum depression is reported to be 35 %; more than a third of those who went on to develop PPD scored in this range (Cooper et al. 1996).
In addition to using a variety of screening measures, the relevant studies had important differences in their subject populations. Some studies drew from the general population of healthy pregnant women, while others defined an “at-risk” or “high-risk” group, the definition of which varied; we have included information about the population in our discussion of each study. Moreover, not all studies screened for depression during pregnancy (prior to the intervention), which raises the possibility that the interventions were actually treating, rather than preventing, a depression that began in pregnancy and continued postpartum, which may be an etiologically distinct subtype from postpartum onset (PPD). We have accordingly indicated those studies that did not screen for depression in pregnancy. In addition, while we have listed all studies that met our criteria (see Table 1), we highlight certain studies that are particularly illustrative of the approaches to, and challenges of, preventing PPD.
Biological interventions
To date, there have been very few RCTs on the prevention of PPD using biological interventions. Existing studies include treatment with antidepressants, hormones, omega-3 fatty acids, dietary calcium, thyroxine, and selenium and have met with mixed success.
Psychotropic medications
Only one RCT (Wisner et al. 2004) has evaluated antidepressant medications. This study, a follow-up to a 2001 open-label trial by the same group of nortriptyline versus monitoring, was started within 24 h of delivery in nondepressed women with a history of at least one episode of PPD. Twenty-two women were randomized at parturition to a 17-week trial of sertraline or placebo. The researchers found that sertraline was significantly more effective than placebo at preventing recurrence of depression (as measured by the Hospital Anxiety and Depression Scale (HADS) and the Structured Clinical Interview (SCID) for DSM-IV; p = 0.04). Moreover, the length of time to recurrence (when PPD did develop) was significantly greater in the medication group (p = 0.02). Of note, the study excluded data from three women in the intervention group who opted not to take the medication.
Reproductive hormones
Estrogen and progesterone levels fluctuate dramatically during the perinatal period, increasing tenfold during pregnancy and returning to pre-pregnancy levels within 72 h of delivery (Bloch et al. 2003). This rapid hormonal decline is thought to contribute to PPD in vulnerable women, although a consistent link between hormone levels and PPD has yet to be demonstrated (Bloch et al. 2003). High-dose estrogen (studied in an open-label trial by Sichel et al. 1995, in which it was found to improve the rate of relapse among women with a history of PPD), may be one promising direction, but only one RCT has evaluated hormone administration as a prevention for PPD. In a double-blind trial of 180 South African women in the general population who were not screened for antenatal depression, Lawrie et al. (1998) showed that women who were randomized to an intramuscular injection of 200 mg norethisterone enanthate (a common progestogen contraceptive) within 48 h of delivery had significantly higher scores on the Montgomery–Asberg Depression Rating Scale (MADRS) and EPDS at 6 weeks postpartum than women in the placebo group (p = 0.0111 and p = 0.0022, respectively).
Micronutrients
The efficacy of omega-3 fatty acids in the prevention of PPD has been investigated in three published RCTs. In a study of US women in the general population (N = 89), Llorente et al. (2003) randomized breastfeeding women to 200 mg DHA versus placebo for 4 months, beginning 1 week after delivery. No significant differences were found between placebo and treatment groups on the Beck Depression Inventory (BDI) at the 4-month follow-up visit. Doornbos et al. (2009) randomized 119 Dutch women in the general population to receive DHA (220 mg), DHA and AA (arachidonic acid; 220 mg of each), or a placebo daily, from enrollment (14 to 20 weeks pregnant) until 3 months after delivery. There were no significant differences among EPDS scores of the three groups at 16- or 36-week gestation or at 6 weeks postpartum, nor in the scores on a maternal blues questionnaire administered within 1 week postpartum. Finally, Makrides et al. (2010) randomized 2,399 Australian women who were less than 21-week gestation to either an intervention group, which received 800 mg/day of DHA, or a control group, which received a daily placebo, from study entry to birth. There was no significant difference between the DHA and control groups in the percentage of women with high levels of depressive symptoms (EPDS score >12) during the first 6 months postpartum (p = 0.09).
Other biological agents
Three studies have evaluated the efficacy of alternative biological approaches to preventing PPD: thyroxine, dietary calcium, and selenium. None of the groups chose its sample based on risk for PPD; the selenium trial screened subjects for antenatal depression using the BDI and excluded those scoring ≥31 (indicative of moderate to severe depression on the BDI), while the other two did not screen for antenatal depression. Analyzing data from a larger US two-site trial evaluating calcium as a preventive measure for preeclampsia, Harrison-Hohner et al. (2001) found that women given 2,000 mg calcium daily during pregnancy and the postpartum period had a significantly lower incidence of severe PPD, as defined by an EPDS score ≥14, than the placebo group at 12 weeks postpartum (n = 247; p = 0.014). In contrast, Harris et al. (2002), in a study of 446 (analyses done of 342) thyroid-antibody-positive pregnant women, found no evidence that 100 μg thyroxine administered daily to the subjects from 6 to 24 weeks postpartum had an effect on the incidence of depression as compared to women in the placebo group. Mokhber et al. (2011), in a study of 166 primipara in Iran, found that women given 100 μg of selenium daily (as selenium yeast) from their first trimester through delivery had significantly lower EPDS scores (p < 0.05), as measured within the first 8 weeks after delivery, than women in the control group, who received daily matching placebo yeast tablets.
In summary, out of eight RCTs of biological interventions for the prevention of PPD, three found a positive effect (Harrison-Hohner et al. 2001, for calcium; Wisner et al. 2004, for sertraline; Mokhber et al. 2011, for selenium), four found no effect (Harris et al. 2002, for thyroxine; Llorente et al. 2003, for omega-3s; Doornbos et al. 2009, for omega-3s; Makrides et al. 2010, for DHA), and one found a negative effect (Lawrie et al. 1998, for progestogen). Based on these results, antidepressants and nutrients both hold promise for prevention, thought this does not rule out other biological pathways due to a paucity of evidence. Even the three clearly negative studies of omega-3s do not rule out further research in this area because they tested only DHA and AA, while the commonly used formulation for clinical mood symptoms is DHA combined with EPA. It should also be noted that few of these studies selected women at risk for PPD based on known risk factors, which might have diminished the likelihood of finding effects for the interventions.
Psychological and psychosocial methods of PPD prevention
In contrast to the scant data on biological interventions, there have been numerous studies of psychological and psychosocial preventive interventions for PPD. These studies are difficult to compare, as they vary widely in terms of screening and outcome measures, training of personnel/clinicians, dosages of treatment, timing of the initiation of treatment (during pregnancy or postpartum), and follow-up times.
Psychological interventions
Interpersonal therapy
Interpersonal therapy (IPT) is a short-term psychotherapy focusing on the present and emphasizing the interpersonal context in which depressive symptoms occur (Klerman and Weissman 1993). IPT originally was developed to treat major depressive disorder in a general adult population but has been adapted to treat women during the perinatal period (Spinelli and Endicott 2003). Seven studies have evaluated IPT’s efficacy in preventing PPD. Three of them incorporated IPT into the Reach Out, Stay strong, Essentials for new mothers (ROSE) program, while a fourth assessed the efficacy of an adaptation of the ROSE program (Relaxation, Encouragement, Appreciation, Communication, Helpfulness (REACH)) aimed specifically at racially and ethnically diverse pregnant adolescents. The ROSE program is a brief, manualized IPT-based group intervention designed by Zlotnick and colleagues (Zlotnick et al. 2001, 2006) to help pregnant women on public assistance improve close relationships, build social support networks, and manage the role transition to motherhood. The intervention comprises four weekly 60-min group sessions during pregnancy. Session topics included identifying and managing role transitions, setting goals, developing social supports, and identifying and resolving interpersonal conflict. In a 2001 pilot study of the ROSE program, Zlotnick and colleagues studied 37 US pregnant women (35 study completers) who reported at least one risk factor for postpartum depression on a survey (e.g., previous episode of depression or PPD, mild to moderate levels of depressive symptoms, poor social support, or a life stressor within the last 6 months). All subjects were enrolled in standard antenatal care, and half of the subjects were randomized to receive the four-session group intervention. Within 3 months postpartum, six (33 %) of the control group had developed PPD (as measured by the major depression module of the SCID for DSM-IV) versus none of the intervention subjects. Further, the change in BDI scores (administered before and after the intervention) for subjects in the intervention group showed a reduction in score and a significantly greater change when compared to the scores of the women in the control group (p < 0.001).
In 2006, the same group performed an expanded study of 99 women at 23- to 32-week gestation who were on public assistance and assessed as at-risk for PPD based on a score of ≥27 on Cooper’s 17-item PIPD. Subjects were randomly assigned to receive either standard antenatal care alone or standard antenatal care plus the ROSE program intervention (as described above), with an individual booster session after delivery. The 50-min booster session reinforced skills introduced in earlier sessions and also addressed any mood changes related to interpersonal difficulties that had arisen since the birth of the baby. Depressive symptoms were assessed at baseline and again at 3 months after delivery using the BDI. In addition, the Longitudinal Interval Follow-Up Evaluation, an interviewer-based assessment, was used to determine whether participants developed PPD. At 3 months postpartum, two (4 %) of the women in the intervention condition, versus eight (20 %) in the standard antenatal care condition, had developed PPD (p = 0.04).
The third ROSE intervention was conducted by Crockett et al. (2008), who studied 36 rural African American women on public assistance between 24–31-week gestation who scored ≥27 on the PIPD. Women were randomized to the ROSE program or treatment as usual. Subjects in the intervention group received four 90-min weekly group sessions and a 50-min individual booster session 2 weeks after delivery. There were no significant between-group differences in EPDS scores at 2 weeks and 3 months postpartum.
The ROSE program was adapted by Phipps and colleagues, who published a 2011 US pilot study of 106 primiparous pregnant adolescents (≤17 years old when they conceived their pregnancy and <25 weeks gestational age at their first prenatal visit). Participants were screened for depression in pregnancy and were randomly assigned to receive either the REACH program, a highly structured adaptation of the ROSE program targeted toward pregnant adolescents, or to an attention and dose-matched control program. The REACH program consists of five 1-h prenatal sessions as well as a postpartum booster session. Sessions, which included video, role-playing, and homework components, focused on improving relationships via enhanced communication skills, developing social supports, managing stress, setting goals, and providing psychoeducation regarding PPD, expectations about motherhood, and psychosocial resources for new mothers. All subjects were given the book Baby Basics: Your Month by Month Guide to a Healthy Pregnancy, and the control condition involved using the book as a guide for a more general didactic program concerning maternal health, fetal development, nutrition, preparation for labor, and preparation for taking a new baby home.
Of note, while the initial study design involved group sessions for both control and intervention conditions, qualitative assessment from participants led the researchers to conclude that participants preferred individual sessions; accommodations were thus made to deliver sessions individually in both conditions. All participants were assessed for PPD (defined as an episode of Major Depressive Disorder (MDD) that occurred within the first 6 months after delivery) using the SCID for DSM-IV, childhood version (KID-SCID) twice during pregnancy, once before randomization and once after intervention, and three times postpartum: within 48 h of delivery and again at 6-week and 3- and 6-month follow-up visits. Intent-to-treat analyses showed no significant differences in incidence of PPD between intervention and control participants, though the authors note that the study was underpowered due to small sample size.
Three studies used IPT outside of the ROSE program. Zlotnick et al. (2011) studied the effect of an IPT-based intervention aimed at reducing depression and posttraumatic stress disorder (PTSD) in low-income pregnant women reporting intimate partner violence (IPV) within the previous year (n = 54). Potential subjects were screened using the SCID for current affective disorders, PTSD, and substance use, and those screening positive were excluded from the study. Subjects were randomly assigned to receive either standard care, which included a listing of resources for IPV, or an intervention consisting of four individual 60-min sessions over a 4-week period, followed by a 60-min postpartum individual booster session within 2 weeks of delivery. This intervention combined components similar to those in the ROSE program—such as helping participants improve close relationships, build social support networks, and manage the role transition to motherhood—with components based on empowerment and stabilization models, which are models of treatment for women with IPV.
The EPDS was administered at intake, 5 to 6 weeks after intake, 2 weeks after delivery, and 3 months postpartum, while a measure of the incidence of MDD (Longitudinal Interval Follow-Up Examination (LIFE)) was administered at 3 months postpartum. Intent-to-treat analyses showed that there were no significant differences between the two groups in terms of cases of MDD as measured by the LIFE interview; depressive symptoms as measured by the EPDS were significantly lower in the intervention group than in the control group at 5 to 6 weeks after intake (during pregnancy; p = 0.05), but no differences were found at 2 weeks or 3 months postpartum.
Grote et al. (2009) randomly assigned socioeconomically disadvantaged, nontreatment-seeking women in the US scoring >12 on the EPDS to receive either enhanced usual care or a manualized intervention called enhanced brief interpersonal psychotherapy (IPT-B) (n = 53). Women in the enhanced usual care group received depression education materials and a referral to the behavioral health center in the same OB-GYN clinic, and their social workers were notified of their elevated depressive symptoms. Enhanced IPT-B consists of an engagement session, eight acute IPT-B sessions before birth, and biweekly or monthly maintenance IPT for up to 6 months after delivery. The engagement session was designed to assess each subject’s barriers to care and then address these using collaborative problem-solving. Subsequent sessions were aimed at helping subjects with interpersonal difficulties including role transition, role dispute, and grief. Intent-to-treat analysis showed that both before birth (3 months after baseline) and 6 months postpartum women in the intervention group experienced significant reductions in depression diagnoses (as determined by the SCID; p < 0.003 and p < 0.005, respectively) and depressive symptoms (as measured by a 50 % improvement on the EPDS; p < 0.001 and p < 0.001, respectively).
Finally, Gao and colleagues, who studied 194 women in the general population in China (2010), randomized subjects to either a control group that received only “routine antenatal education,” consisting of two 90-min sessions conducted by midwives, or an intervention group that received both the routine antenatal sessions and an IPT-based childbirth psychoeducation program. The intervention consisted of two 2-h group sessions during pregnancy and one telephone follow-up session within 2 weeks of delivery. Intervention sessions, which were held following routine childbirth education classes to encourage attendance, focused on topics including managing role transition, identifying and establishing support systems, and improving communication. The follow-up phone session reinforced skills learned in previous sessions. Results showed a reduction at 6 weeks in mean EPDS scores from preintervention to postintervention for the intervention group, while mean EPDS scores for the control group increased from preintervention to postintervention. The changes in EPDS scores from preintervention to posttest were significantly different between groups (p = 0.000).
In summary, of the seven RCTs evaluating IPT for prevention of PPD, four (including two pilot studies) demonstrated a reduction in the likelihood of developing depression postpartum. The majority of these trials were based on selecting women at risk for PPD and importantly, given IPT’s conceptual model, targeted the interpersonal conflicts that make up the psychological risk factors for PPD. Thus, the IPT orientation may be exceptionally well suited to PPD prevention. Finally, some of the successful approaches used nonclinical staff, suggesting that these interventions could have widespread application.
Cognitive behavioral therapy
Cognitive behavioral therapy (CBT) is a short-term psychotherapy combining components from cognitive therapy and behavior therapy; the former is aimed at identifying and challenging distorted thinking, while the latter focuses on learning techniques and skills to modify negative patterns of behavior. Findings on CBT have been more variable than those on IPT, with six studies (four of which targeted at-risk women only) reporting success and six with negative findings.
The first study reporting positive results was conducted by Chabrol et al. (2002), who randomized 241 French women determined to be at risk by EPDS score >9 to an intervention group or a control group. Mothers in the intervention received a 1-h individual prevention session 2 to 5 days postpartum, while still in the hospital. These sessions included an educational component (giving information about parenthood and guidance regarding infant development), a supportive component (featuring empathic listening, acknowledgement of maternal ambivalence and negative feelings, and normalizing mothers’ experiences), and a CBT component (aimed at challenging expectations of being a “perfect mother” and promoting problem-solving). All participants were given a second EPDS and instructed to complete the questionnaire and return it to the researchers 4 to 6 weeks postpartum. At 4 to 6 weeks, some women in each group had a significant reduction in the frequency of depression as defined by an EPDS score of ≥11; the proportion experiencing a reduction in the intervention group (48.2 %) was greater than the proportion in the control group (30.2 %, p = 0.0067). In addition, the mean EPDS score was significantly lower in the prevention group than the control group (p < 0.0024). An intention to treat analysis, which included all subjects with an EPDS score ≥9 immediately postpartum as well as subjects who refused further assessment and did not return the second EPDS, was also conducted; a repeated measures ANOVA showed a significant group × assessment interaction in favor of prevention (p < 0.01). Of note, the commonly used clinical cutoff for PPD on the EPDS is 13.
In a small 2008 pilot study in Korea, Cho et al. randomly assigned 27 at-risk pregnant women to either a control or an intervention group. Risk was determined by a BDI score >16. Those in the intervention group met with a clinical psychologist during pregnancy for nine 1-h individual CBT sessions every 2 weeks. These sessions focused on psychoeducation about depression; identifying and modifying irrational or negative thoughts, particularly those related to the marital relationship; and communication and behavioral skills training. Women in the control group received one psychoeducational session about depression and strategies for minimizing depressive symptoms. Women who received the CBT intervention had a significantly lower rate of PPD assessed at 1 month postpartum than women in the control group, as measured by the BDI (p < 0.01). The researchers hypothesize that the intervention’s efficacy was a result of the individual sessions and treatment compliance with the multiple session approach.
Milgrom et al. (2011) studied 143 Australian women determined to be at risk by EPDS and/or Risk Assessment Checklist score ≥13. Women, who were recruited at 20- to 32-weeks gestation, were randomly assigned to usual care or to receive a CBT-based self-help workbook, as well as eight weekly individual telephone support sessions. The workbook included sections on nurturing the mother–baby and father–baby relationships, managing relationship and life changes, and behavioral and cognitive strategies for coping with anxiety and depression. Participants in the intervention group were instructed to read a portion of the workbook each week and then discuss the content with a therapist over the phone. The first seven sessions occurred during late pregnancy, while the eighth session occurred 6 weeks after birth. Results indicated that participants in the intervention group reported significantly lower levels of depression on the BDI-II than the control subjects at 12 weeks postpartum (p < 0.01).
Tandon et al. (2011) studied 61 low-income at-risk US women (as determined by CES-D score ≥16 and/or a lifetime depressive episode) enrolled in a home visiting program. Of note, this study included both pregnant women and women who had a child fewer than 6 months old, which raises the possibility that for women in the latter category, the intervention was actually treating rather than preventing PPD. Participants were randomized to an intervention group, who received a six-session weekly CBT-based group intervention in addition to home visits, and a control group, who received routine home visits plus information regarding perinatal depression (but not the CBT-based program). The group intervention was a modified version of Munoz et al.’s Mothers and Babies (MB) course, a CBT-based program aimed at preventing perinatal depression by teaching participants to manage mood. Group sessions were supplemented by one-on-one reinforcement of key group material by home visitors between group sessions (in contrast to women in the control group, who also received one-on-one home visits but without the added CBT reinforcement component). Results indicated that at 3 months postintervention, 33 % of women in the control group reported levels of depressive symptoms that met clinical cutoff for depression on the MMS (Maternal Mood Screener, Le and Muñoz 1998), versus 9 % of women in the intervention group, a statistically significant difference (p < 0.05).
Two studies conducted in 2012, one by Mao et al. in China and the other by Kozinszky et al. in Hungary, both showed positive outcomes for CBT using group interventions with participants not at risk for PPD. Mao et al.’s study, which looked at 240 primiparous women starting in their 32nd week of pregnancy, randomized participants to either standard antenatal education, which consisted of four 90-min childbirth education sessions conducted by obstetrics nurses, or the Emotional Self-Management Group Training (ESMGT) program, which comprised four weekly group sessions and one individual counseling session. Participants attended the intervention sessions as a couple. Themes of the group sessions included understanding emotional and interpersonal implications of Chinese cultural norms around delivery (e.g., negative reaction to birth of female baby), problem-solving and positive communication, relaxation exercises and cognitive restructuring, and enhancing self-confidence. Scores on the Patient Health Questionnaire-9 (PHQ-9) administered at completion of the intervention (36 weeks) were significantly lower for women in the intervention group than for those in the control group (p < 0.01). Moreover, mean EPDS scores at 6 weeks postnatal were also significantly lower for the intervention group than the control group (p < 0.05). Using the SCID at 6 weeks postpartum to assess for PPD among participants who scored >11 on the EPDS revealed a significantly lower incidence of PPD (2.7 %) in the intervention group versus the control group (9.3 %; p < 0.05).
Participants in Kozinszky et al.’s study (n = 1719) were randomly assigned to either a control group, which attended four group meetings consisting of routine education on pregnancy, childbirth, and baby care (which is more or less identical to treatment as usual) or an experimental group, which received four 3-h group psychotherapeutic/psychoeducational sessions; these latter sessions incorporated elements of psychoeducation, CBT, IPT, and group therapy. Fathers were permitted to attend sessions. At 6 weeks postpartum, PPD prevalence, as determined by a cutoff score of 11/12 on the Leverton Questionnaire (LQ), was significantly lower among intervention participants than control participants (p < 0.01). Moreover, depressive symptoms assessed with the LQ at 6 to 8 weeks after delivery were significantly lower in the intervention group versus the control group (p < 0.001).
While the six studies highlighted above all found positive effects for a CBT intervention, six additional studies found the opposite. In a US pilot study of low-income mothers of preterm infants (≤33-week gestation; Silverstein et al. 2011, n = 50), participants, who were not screened for antenatal depression, were randomized to receive either problem-solving education (PSE), a one-on-one CBT-based problem-solving intervention, or usual hospital services, which included access to a social worker through the time the infant was discharged. Subjects in the intervention group received four individual sessions ranging from 25 to 60 min, beginning while infants were still in the hospital and continuing weekly or biweekly. Sessions were conducted in a location of the subject’s choosing (usually hospital or home). In each session, educators helped subjects identify a problem, set goals, choose a solution, and make an action plan. There were no significant group differences in the rates of moderately severe depression symptoms (as defined by a score of ≥11 on the Quick Inventory of Depressive Symptoms (QIDS)) occurring in the intervention versus control groups, though there was a trend for the intervention subjects toward a lower chance of experiencing an episode of such symptoms.
Hagan et al. (2004, in Australia) studied 199 mothers of very preterm (<33 weeks) or very low birth weight (<1,500 g) infants. Participants were evaluated 2 weeks postpartum using the Schedule for Affective Disorders and Schizophrenia (SADS); those who were judged not depressed were then randomized to a control group, who received standard care for mothers of preterm infants (including social work contact, regular biweekly parent education groups, and a developmental physiotherapy playgroup during the first postpartum year), and an intervention group, who received standard care plus a brief individual debriefing session regarding their experience during pregnancy and then six weekly 2-h sessions of group CBT between 2 and 6 weeks postpartum. CBT session content included adjusting to parenthood with a preterm infant, information about PPD, identifying and modifying negative thinking patterns, and short- and long-term goal settings. All participants were given the SADS at 2, 6, and 12 months; results revealed no significant differences in the incidence of depression between intervention and control groups at any time point.
Austin et al. (2008) studied 277 Australian women who had an EPDS score >10 and/or a score of >23 on the Antenatal Risk Questionnaire or a reported prior history of depression. They were randomized to a control group, which received an information booklet in addition to standard care, and an intervention group, which received a CBT group intervention in addition to the information booklet and standard care. The intervention, which consisted of six weekly 2-h group sessions plus a later follow-up session, focused largely on behavioral strategies, such as goal setting, problem-solving, and relaxation training, to prevent and manage low mood, anxiety, and stress in the postpartum period. Participants completed the EPDS at the initial interview (time 1), after the final session of the CBT program (time 2), 2 months postpartum (time 3), and 4 months postpartum (time 4), as well as the depression and anxiety subsections of the Mini International Neuropsychiatric Interview (MINI) at times 1, 3, and 4. Intent-to-treat analyses showed no significant group differences in EPDS scores at times 2, 3, and 4, and no reduction in the incidence of depression as measured by the MINI.
Finally, three additional studies used the same intervention as Tandon et al. (in a successful study cited above) but showed no effect. Munoz et al., whose work in 1995 in depression in a primary care setting was the initial basis for the intervention, conducted a pilot study in 2007 in 41 high-risk Latina women in the USA determined to be at risk by a past history of MDE and/or a CES-D score ≥16. Participants were randomized to either a control group or an intervention group, which received the MB course, a 12-week CBT group intervention followed by four individual booster sessions at 1, 3, 6, and 12 months. After 1 year, 14 % of the women in the intervention group versus 25 % of the women in the control group developed a new onset of major depression, but this difference did not reach statistical significance.
In a multisite study, Zayas et al. (2004) studied 187 African–American and Latina women in the USA determined to be at risk for PPD by a BDI score ≥14 in their third trimester. They were randomized to a control group receiving treatment as usual from their health center and an intervention group who received a three-part intervention consisting of eight group sessions of CBT, four psychoeducation sessions on infant development and maternal sensitivity, and social support building from the therapist. Results showed no significant group differences in BDI scores at 2 weeks and 3 months postpartum.
Similarly, Le et al. 2011 studied 217 low-income US Latina women determined to be at high risk by CES-D score ≥16 and/or self-reported personal or family history of depression. Participants were randomized to receive usual care or a CBT group intervention modified from Munoz’s MB course and consisting of eight weekly 2-h sessions focusing on developing mood regulation skills to prevent perinatal depression, followed by three postpartum individual booster sessions conducted at 6 weeks and 4 and 12 months. Participants were evaluated at five time points, twice during pregnancy—preintervention (T1) and postintervention (T2)—and three times after birth, at 6 weeks (T3), 4 months (T4), and 12 months postpartum (T5). Results showed that the intervention had a significant short-term effect on depressive symptoms (from T1 to T2—that is, from early to late pregnancy (as measured by the BDI; p = 0.03))—but that these results did not persist into the postpartum period. There were no significant differences in the rates of major depressive episodes (as measured by Lawrie et al. 1998) at any of the time periods or cumulatively. Le et al. attribute this lack of significant group differences in part to the low depressive symptoms and relatively low incidence of major depressive episodes among women in both the intervention and control groups. They offer multiple possible explanations for this low incidence, including attrition (30 % of subjects were lost to follow-up) and low session attendance (roughly half of the intervention participants did not attend all four classes, and 12 % did not attend any).
The interventions evaluated in the six successful studies varied widely in terms of sample characteristics, duration and intensity of the intervention, modality of delivery (i.e., individual versus group), and level of training of the interveners. Of note, three of the four studies using individual CBT (Milgrom et al., Cho et al., and Chabrol et al.) were successful, while five of the eight group-based interventions (Le et al., Austin et al., Munoz et al., Zayas et al., and Hagan et al.) were not. Two of the three studies that used a group-based approach with individual booster sessions administered after the completion of the group sessions (Munoz and Le) were not successful. However, Tandon’s study was successful using group sessions plus individual sessions between group sessions. It is also notable that two of the unsuccessful studies enrolled mothers of early preterm babies only, which may have affected participants’ risk of developing PPD.
Postnatal psychological debriefing
Psychological debriefing is a controversial treatment typically consisting of a single semi-structured psychological interview during which the interviewer explores a person’s experience of a traumatic event with the aim of reducing psychological distress after trauma and preventing PTSD. These interviews are usually administered within a month of a potentially traumatic event (Rose et al. 2002). A 2002 Cochrane review of 11 studies comparing subjects who received psychological debriefing with no-intervention controls concluded that psychological debriefing was not successful in preventing PTSD; two trials found that it actually made subjects symptomatically worse (Rose et al. 2002).
In the postnatal setting, debriefing most often takes the form of a discussion of labor and delivery experiences with an empathic listener in a structured format soon after delivery (Small et al. 2000). Five RCTs have examined the effect of postnatal psychological debriefing on the prevention of PPD. Two studies showed positive effects, and three showed no difference. Lavender and Walkinshaw (1998) studied 120 British women in the general population with normal spontaneous at-term vaginal deliveries. Subjects, who were not screened for antenatal depression, were randomized to receive treatment as usual or a single debriefing session prior to discharge with a midwife not formally trained in counseling. The session consisted of “an interactive interview in which they spent as much time as necessary discussing their labor, asking questions, and exploring their feelings.” All participants were mailed a HADS questionnaire 3 weeks after discharge and asked to return it. Scores on the HADS range from 0 to 21. Results showed that women who received the intervention were significantly less likely to have high depression (defined as a depression score >10 points; p < 0.0001), as well as high anxiety (defined as an anxiety score >10 points; p < 0.001) 3 weeks after delivery. Of note, the HADS has not been validated for postnatal care, though it has been validated in many health service fields. The researchers explain that they used the HADS rather than the EPDS because it allows for subgroup analysis, which defines both anxiety and depression.
In 2005, Gamble and colleagues studied 103 Australian women who had experienced a distressing or traumatic birth, as defined by criterion A of DSM-IV for PTSD: women were asked within 72 h of birth if during labor or birth they had feared for their or their baby’s life, or feared serious injury or permanent damage. Women who responded positively to these questions, and thus met criterion A of DSM-IV, were randomized to a single debriefing session within 72 h after birth, as well as a telephone follow-up at 4 to 6 weeks, or to treatment as usual. There were no statistically significant differences between the groups with respect to rate of obstetric intervention in the current pregnancy. At 3 months postpartum, women in the intervention group were significantly less likely to develop PPD (as determined by an EPDS score >12) than women in the control group (p = 0.002). While there was no difference at 4 to 6 weeks or 3 months postpartum between groups in numbers of women meeting criteria for PTSD, the total PTSD symptoms scores at 3 months (but not at 4 to 6 weeks) were significantly higher in the control group than in the intervention group (p = 0.035), suggesting that the intervention was effective in reducing symptoms over the longer term.
The remaining three studies of postnatal debriefing did not have significant results. Small et al. (2000, 2006) conducted an RCT with 1,041 Australian women not screened for antenatal depression who had operative births (defined by the study authors as birth by Caesarean section, forceps, or vacuum extraction). Women were randomized to a debriefing session prior to discharge or to a control group who received a pamphlet about resources for postpartum mothers (intervention subjects were given the pamphlet as well). There were no significant group differences in rates of depression (as defined by EPDS score ≥13) at either 6 months (Small et al. 2000) or 4 to 6 years postpartum (Small et al. 2006).
Similarly, Tam et al. (2003) studied 516 women in Hong Kong recruited within 48 h after delivery who experienced “suboptimal outcomes” during pregnancy and delivery (e.g., antenatal complications resulting in hospital admission, such as gestational diabetes or placenta previa; elective and emergency Caesarean sections; or instrumental vaginal delivery). Women were randomized to an intervention group, which received educational counseling, or to a control group, which received treatment as usual. The intervention consisted of two parts, an educational component and a counseling component; the former, based on the premise that lack of information contributed to psychological symptoms, consisted of explanation and clarification of the events surrounding the birth, while the latter entailed encouraging participants to discuss their emotional reactions to the unexpected events. Number and duration of sessions were decided by the research nurse on a case-by-case basis; the number of sessions ranged from one to four, and total duration over all sessions ranged from 25 to 50 min, with a median total time of 35 min. Results of the HADS and Global Health Questionnaire (GHQ) (Goldberg and Williams 1988) administered before intervention, at 6 weeks after delivery during a postnatal follow-up visit, and at 6 months (via mail) showed no significant group differences in terms of depressive symptoms (as measured by the HADS) or rates of possible cases of PPD (using 4/5 cutoff on the GHQ), although among women who underwent elective Cesarean sections, those in the intervention group had significantly lower depression scores than those in the control group (p = 0.009).
Also in 2003, Priest et al. studied 1,730 Australian women in the general population recruited 24 to 72 h after delivery. Participants were randomized either to a control condition, consisting of standard postnatal care, or to an intervention, consisting of a single standardized debriefing session in their hospital rooms. The sessions ranged from 15 min to 1 h and were conducted by research midwives with training in critical incident stress debriefing. EPDS questionnaires were mailed at 2, 6, and 12 months postpartum, and participants with EPDS scores >12 at any time point were given the SADS within 2 weeks of the questionnaire by research clinical psychologists to further assess symptomatology and diagnosis. Results indicated no significant differences between groups in EPDS scores at 2, 6, or 12 months or in proportions of participants meeting diagnostic criteria for major or minor depression.
In summary, the debriefing trials include two studies with positive effects and three showing no difference. However, the factors associated with success varied tremendously, e.g., women at risk for psychiatric or medical reasons or without any predisposing factors, length of intervention. More research on using debriefing as a preventive intervention for PPD must be conducted to determine the potential for this clinical strategy.
Across psychological interventions as a whole, 12 trials showed positive effects (four IPT, six CBT, and three debriefing), with an additional two IPT pilot studies showing a trend toward a positive result that did not reach statistical significance. One IPT study, six CBT studies, and three debriefing studies did not show a difference. Factors that contribute to these differences will be discussed at greater length in the conclusion.
Psychosocial interventions
Antenatal and postnatal classes
To date, six RCTs have been conducted to evaluate group-based psychoeducational interventions to prevent PPD; two RCTs have looked at individual psychoeducational approaches to preventing PPD. The approaches assessed in the group-based studies varied in terms of the content of the sessions as well as the number and timing of sessions, group size, and type of facilitator. Common topics included a general introduction to PPD and how to identify and treat it; discussion of the social and emotional challenges of pregnancy; and education about self-care, social support, and problem-solving skills. In addition, several of the interventions addressed unrealistic beliefs about pregnancy and motherhood.
Three of the six group-based studies showed a difference between intervention and control groups. In the UK in 2000, Elliot and colleagues studied 99 women at risk for clinical depression (as determined by a reported history of depression and/or CESD score ≥16). Women were randomized to 11 group sessions (five during pregnancy and six postpartum); the control group received standard prenatal and postnatal care. There was a significant decrease in depressive symptoms and rates of clinical depression in at-risk primiparous, but not at-risk multiparous, women (p < 0.005).
In Australia, Matthey et al. (2004) randomized 268 women in the general population to three conditions: usual service (“control”), experimental (“empathy”), or nonspecific control (“baby-play”). The latter condition controlled for the nonspecific effects of the intervention, which were the provision of an extra class, asking couples to think about the early postpartum weeks, and receiving two booster sessions. All subjects received six routine antenatal classes. Those in the experimental group were randomized to receive an additional class in week 5 focused on postpartum psychosocial issues. In the nonspecific control condition, the extra class focused on the importance of play for infants. Participants in the usual service condition received the six antenatal classes only. Results showed a significant interaction between condition and self-esteem on maternal mood at 6 weeks, but not 6 months: women with low self-esteem who had received the intervention scored significantly lower on the EPDS at 6 weeks, but not at 6 months, than women with low self-esteem in either of the two control conditions (p < 0.01). This study differed from the others reviewed in this article in its inclusion of partners in all sessions (both control and experimental).
Lara et al. (2010) also found significant reductions in clinical depression incidence and symptomatology in their treatment group, this time in Mexico (n = 136). Lara et al. examined at-risk pregnant women (as determined by CESD score ≥16 and/or a self-reported history of depression). Participants were randomized to either a usual care or an intervention group. All participants received a self-help book about depression, which included a directory of community mental health services. The intervention groups, which met weekly for eight 2-h sessions, were composed of five to ten participants each. Session topics included information about pregnancy and the postpartum period, as well as strategies to reduce depression through improving self-care and self-esteem, increasing social support, engaging in positive thinking, and addressing issues related to past grief and loss, as well as unrealistic expectations regarding pregnancy and motherhood. Childcare was offered during the classes. Two individual booster sessions were provided by trained research assistants at 6 weeks and 4 to 6 months postpartum. The researchers found that the cumulative incidence of major depression over the course of the study, as measured by the SCID, was significantly lower in the intervention groups than in the control group (p < 0.05). In contrast, there were no significant group differences in reduction of depressive symptoms (as measured by the BDI-II). Of note, there was a substantial difference in attrition before the start of the intervention, with substantially higher attrition in the intervention group than the control group; 57.6 % of randomized intervention participants never attended the intervention, versus 7.8 % of control participants who were lost in this same period. Because of this disparity, findings of this study should be interpreted with caution.
The remaining three group-based studies of at-risk women failed to demonstrate prevention of PPD symptoms. Stamp et al. (1995) offered women in the intervention group two sessions during pregnancy and one postpartum, led by a midwife educator (n = 144, Australia); sessions focused on planning for and managing life changes around having a baby. The control group received care as usual. In Buist et al. (1999) (n = 45, Australia), subjects were randomized to a control group who received care as usual or an intervention group who received ten sessions (authors did not indicate which sessions were given during pregnancy and which were offered postpartum), which focused on parenting and coping strategies. Brugha et al. (2000) offered to women in the experimental group a six-session antenatal intervention, led by nurses and occupational therapists with no formal training in psychological interventions (n = 209, in the UK). The control group received care as usual. The intervention focused on cognitive and problem-solving approaches as well as enhancing social support. Participants in the intervention group also met for a reunion class at 8 weeks postpartum. Importantly, these three trials had serious methodological limitations. All three studies were conducted with women identified as at-risk based on screening questionnaires designed by the researchers (versus validated approaches). The studies had low group attendance (Stamp et al.; Brugha et al.), high attrition (Stamp et al.; Brugha et al.), and small sample size (Buist et al.). In addition, the interveners in the studies of Stamp et al. and Brugha et al. did not have any specific training, whereas among the positive studies, Lara et al. describes their trained facilitators as having “extensive experience” and Elliot et al.’s groups were run by a health visitor and clinical psychologist.
Two RCTs, one conducted in Australia by Hayes et al. (2001) (n = 206) and the other in the USA by Howell et al. (2012) (n = 540), assessed the preventive effects of individual psychoeducation sessions on postpartum depressive symptoms in women in the general population. In the multisite study by Hayes and colleagues, women in the intervention group received an information booklet about PPD, an audiotape of one woman’s experience with PPD, and a single individual session with a midwife with experience in antenatal education, who reviewed the materials with them. The control group received care as usual. No significant group differences were found on the Profile of Mood States (POMS) at 8 to 12 weeks nor at 16 to 24 weeks.
In Howell’s study, conducted with black and Latina mothers, women in the intervention group received two sessions, the first while still in the hospital after delivery and the second over the phone 2 weeks later. The control group received enhanced usual care, consisting of a list of community resources and a control telephone call at 2 weeks. In the first intervention session, the therapist reviewed with the mother written materials describing typical symptoms of the postpartum experience and suggesting ways to manage these; additionally, the mother was provided information about social support and community resources. In the second session, 2 weeks later, the therapist assessed the subject’s symptoms and her skills in managing these; action plans and to-do lists were also reviewed and created. Depressive symptoms were assessed using the EPDS at four time points: before randomization and then 3 weeks and 3 and 6 months later. Positive screens (defined as EPDS score ≥10) were significantly less common at 3 weeks postpartum among women in the intervention group than among those in the usual care group (p = 0.03); values for 3 and 6 months did not reach significance (p = 0.09 and p = 0.11, respectively).
Postnatal support
Five RCTs have evaluated a variety of postnatal support interventions as a means of preventing PPD. None of these studies screened for antenatal depression. Of the five, two showed effectiveness in preventing PPD and three had negative results. In a 1999 Australian study showing effectiveness in preventing PPD, Armstrong et al. studied 181 women who reported at least one first-tier risk factor for “family dysfunction” on a questionnaire (e.g., physical forms of domestic violence, childhood abuse of either parent, single parenthood, and ambivalence toward pregnancy) and/or at least three second-tier risk factors (e.g., maternal age <18, unstable housing, financial stress, less than 10 years of maternal education, low family income, social isolation, history of mental health disorder in either parent, alcohol or drug abuse, and domestic abuse other than physical violence). Subjects were recruited just after delivery and were randomly assigned to receive either standard community child health services care or structured home visits from trained child health nurses supported by a pediatrician and social worker. Of note, the intervention was designed to benefit (and assess) infant and family health outcomes in addition to maternal health outcomes. Home visits occurred weekly for the first 6 weeks, every 2 weeks until 3 months, and then monthly until 6 months postpartum. Mothers in the intervention group had significantly lower EPDS scores at 6 weeks (p < 0.05), and there was a significant difference between the percentage in each group with EPDS scores greater than the clinical threshold of 12 (p < 0.05), in favor of the intervention group.
In 2009, Dennis et al. screened at-risk women within the first 2 weeks postpartum using the EPDS, and randomized those scoring >9 (n = 612) to care as usual or to individualized telephone-based peer support from a volunteer who had previously recovered from PPD and attended a 4-h training session. The authors found that women in the intervention had significantly lower EPDS scores at 12 weeks (p < 0.001) than those in the control group. There were no group differences at 24 weeks, but the authors attribute this to the fact that participants who were identified as clinically depressed at 12 weeks were referred for treatment.
Three additional studies showed no effect of an intervention. In 2000, Morrell et al. studied 623 at-risk women in the UK (defined as those women who scored ≤24 on the Maternity Social Support Scale and/or those having a past history of mental illness, family psychiatric history, past PPD, or a mother who had PPD). Participants were randomized to usual postpartum care (which included care at home by community midwives) or to an intervention group who received lay support by trained support workers in addition to usual care. Support workers, who underwent 8 weeks of training, provided both practical and emotional support (e.g., building mothers’ confidence in caring for their babies and reinforcing midwifery advice about feeding). Participants in the intervention group received up to ten visits from the support workers, with each visit lasting between 10 and 375 min. The primary outcome measure was general health, as measured by the short form-36 (SF-36); depressive symptoms, as assessed by the EPDS (which were distributed and returned via mail), were a secondary outcome. There were no group differences in EPDS scores at either or 24 weeks postpartum.
In 2002, Reid and colleagues in Scotland randomized 1,004 primiparous women in the general population between 34 and 37 weeks pregnant to one of two intervention groups. One group received a mailed invitation 2 weeks postpartum to a local weekly postnatal support group run by a facilitator; the other group received a postnatal support manual in the mail 2 weeks postpartum. The manual, which was written and pilot-tested with women of varying ethnic and socioeconomic backgrounds, offers information and advice aimed at new mothers and their babies (e.g., regarding maternal sleep and support needs, and infant crying). The groups, which lasted 2 h, were run by trained facilitators with a midwifery background and experience with group work; the group agendas were decided by facilitators in conjunction with participants and tended to focus on issues relating both to the baby and to maternal health and well-being. After the first session, participants received a second invitation informing them of the date of the next group session in their locality. Mothers in both groups completed EPDS questionnaires at baseline (preintervention, 2 weeks postpartum) and at 3 months (postintervention) and 6 months (follow-up). Results indicated no significant differences in EPDS scores between control and intervention arms in terms of either the proportion scoring ≥12 or for mean EPDS scores at 3 and 6 months. The 95 % confidence intervals for the difference in mean EPDS scores effectively excluded a change in mean scores of greater than 10 % with either intervention; a p value is not given in the article.
In 2005, Wiggins and colleagues in the UK randomized 731 socioeconomically disadvantaged women in the general population to one of two intervention groups or to a control group receiving health visitor services, a standard medical practice in the UK. Subjects in one intervention group received a year of monthly supportive listening by a support health visitor, with a primary focus on the woman rather than the child. Subjects in the other intervention group were assigned for 1 year to community groups that offered services for new mothers, including drop-in sessions, home visiting, and/or telephone support. There was no evidence that either intervention reduced the incidence of depression (as measured by EPDS scores at 8 weeks and 14 months and GHQ scores at 20 months) as compared with the control condition. The results of these postpartum support preventive interventions are mixed, and the two successful studies were only able to show group differences in depression up to 6 and 12 weeks postpartum, suggesting that additional research is needed to determine if the effects of these types of interventions can have more long-term effects.
In summary, of the psychosocial interventions, which include both antenatal and postnatal support and education, only five of 13 trials were able to demonstrate significant differences between the control and intervention groups. In the next section, we will turn to a discussion of the characteristics of these trials and factors that may contribute to the variability in results —and point to possible directions for the future.
Conclusion
Postpartum depression is the most common complication of childbirth, with close to 20 % of new mothers experiencing an episode. We are only at the beginning stages of understanding the biological risk factors that underlie the condition; psychosocial risk factors include, most importantly, depression during pregnancy. Postpartum depression is significantly undertreated, in part because of the stigma associated with illness during what “should” be a happy time, in part because of lack of knowledge, and in part because of many mothers’ reluctance to use psychotropic medications during breastfeeding. The low rate of treatment makes it all the more urgent to find new ways to prevent postpartum depression, thus eliding the need for treatment.
In this paper, we have provided a qualitative review of recent literature on interventions to prevent postpartum depression. We reviewed eight studies of biological interventions, among which interventions with antidepressants and nutrients provided the most evidence of successful prevention. Further studies on biological prevention could include additional antidepressants and nutrients, as well as additional studies of omega-3s, which have not yet been studied in their most usually prescribed form.
Across the 37 RCTs of psychological and psychosocial interventions for the prevention of PPD, 17 found a positive effect for the intervention while 20 did not. Of the 17 studies showing an effect, eight were primarily group-based, eight were primarily individual, and one was combined. Of the 20 showing no effect, six were group-based, eight were individual, and six were combined. However, as indicated, several of the group interventions had methodological weaknesses (e.g., use of nonvalidated approaches to measure risk, low attendance) that may have influenced the poor results rather than the group format per se. Overall, the successful studies varied with respect to sample characteristics (at risk or not); modality of and theoretical approach to treatment; number, timing, and duration of sessions; and level of training of interveners. On the one hand, this diversity would seem to challenge the easy identification of directions to pursue for treatment development. On the other hand, important trends emerge: out of 17 successful trials, 13 were conducted with at-risk populations, suggesting that harnessing data on the known psychological contributors to PPD and targeting women by these criteria may aid in the effectiveness of PPD prevention treatment. In addition, four out of seven IPT-based interventions were successful, and an additional two IPT studies were pilot studies showing trends toward significance. The interpersonal focus of IPT may therefore be an especially useful conceptual model for the development of prevention treatments for PPD, in line with the largely relationship oriented psychological risk factors for the disorder. While only half of the CBT studies were successful, there was a higher rate of success with individual than with group CBT, and this difference may be worth exploring in future studies.
While many of the above interventions hold promise for future research, there is another possible direction as well. All of the studies above focus on the mother, the identified patient in a case of PPD—but a mother and new baby are a dyad. One way to move forward with identifying successful interventions may be to focus on the dyad. Difficult infant temperament has been identified as one possible risk factor for PPD (Beck 1996), and studies have shown strong associations between infant fuss/cry and poor sleep behavior and maternal depression (Maxted et al. 2005; Vik et al. 2009; Meyer and Erler 2011). Preventive interventions with a dyadic focus may provide therapeutic benefits. Studies have shown that sleep interventions can help with changing parent behavior and improving infant sleep (Pinilla and Birch 1993; Symon et al. 2005). There are also effective behavioral techniques to reduce infant fussing and crying (St James-Roberts et al. 1995; Hunziker and Barr 1986).
Our laboratory hopes to address the dyadic contribution to PPD with a novel protocol for the prevention of PPD. Practical Resources for Effective Postpartum Parenting (PREPP), currently under study, comprises unique targeted psychotherapy techniques along with the established infant behavioral interventions (Pinilla and Birch 1993; Hunziker and Barr 1986). We hypothesize that women’s elicitation of behavioral change from their infants may be protective against PPD through several possible mediating pathways: (1) an increase in parenting efficacy and resulting diminishment of negative self attributions; (2) an improved sense of social support from coaching sessions by the clinician; (3) better maternal sleep; (4) more effective parenting skills leading to a more responsive and rewarding baby; and (5) increased attachment to infant. This dyadic intervention has the potential to reduce the incidence of PPD in women at risk and to affect directly the developing mother–child relationship, the mother’s view of her child, and child developmental outcomes.
References
Armstrong K, Fraser J, Dadds M, Morris J (1999) A randomized, controlled trial of nurse home visiting to vulnerable families with newborns. J Paediatr Child Health 35(3):237–244
Austin M-P et al (2008) Brief antenatal cognitive behaviour therapy group intervention for the prevention of postnatal depression and anxiety: a randomised controlled trial. J Affect Disord 105(1):35–44
Beck CT (1996) A meta-analysis of predictors of postpartum depression. Nurs Res 45(5):297–303
Beck CT (2001) Predictors of postpartum depression: an update. Nurs Res 50(5):275–285
Bloch M, Daly RC, Rubinow DR (2003) Endocrine factors in the etiology of postpartum depression. Compr Psychiatry 44(3):234–246
Brugha T et al (2000) Pragmatic randomized trial of antenatal intervention to prevent post-natal depression by reducing psychosocial risk factors. Psychol Med 30(6):1273–1281
Buist A, Westley D, Hill C (1999) Antenatal prevention of postnatal depression. Arch Wom Ment Health 1(4):167–173
Chabrol H, Teissedre F, Saint-Jean M, Teisseyre N, Roge B, Mullet E (2002) Prevention and treatment of post-partum depression: a controlled randomized study on women at risk. Psychol Med 32(6):1039–1047
Cho HJ, Kwon JH, Lee JJ (2008) Antenatal cognitive-behavioral therapy for prevention of postpartum depression: a pilot study. Yonsei Med J 49(4):553–562
Cicchetti D, Rogosch FA, Toth SL (1998) Maternal depressive disorder and contextual risk: contributions to the development of attachment insecurity and behavior problems in toddlerhood. Dev Psychopathol 10(02):283–300
Conroy S, Pariante CM, Marks M, Davies HA, Farrelly S, Schacht R, Moran P (2012) Maternal psychopathology and infant development at 18 months: the impact of maternal personality disorder and depression. J Am Acad Child Adolesc Psychiatry 19(15):1270–1273
Cooper PJ, Murray L, Hooper R, West A (1996) The development and validation of a predictive index for postpartum depression. Psychol Med 26(3):627–634
Cott A, Wisner K (2003) Psychiatric disorders during pregnancy. Int Rev Psychiatry 15(3):217–230
Cox JL, Holden JM, Sagovsky R (1987) Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Brit J Psychiatry 150(6):782–786
Crockett K, Zlotnick C, Davis M, Payne N, Washington R (2008) A depression preventive intervention for rural low-income African-American pregnant women at risk for postpartum depression. Arch Womens Ment Health 11(5–6):319–325
Dabelea D, Snell-Bergeon JK, Hartsfield CL, Bischoff KJ, Hamman RF, McDuffie RS (2005) Increasing prevalence of gestational diabetes mellitus (GDM) over time and by birth Cohort Kaiser Permanente of Colorado GDM Screening Program. Diabetes Care 28(3):579–584
Dennis C, Hodnett E, Kenton L, Weston J, Zupancic J, Stewart D, Kiss A (2009) Effect of peer support on prevention of postnatal depression among high risk women: multisite randomised controlled trial. BMJ 338. doi:10.1136/bmj.a3064.
Doornbos B, Van Goor S, Dijck-Brouwer D, Schaafsma A, Korf J, Muskiet F (2009) Supplementation of a low dose of DHA or DHA + AA does not prevent peripartum depressive symptoms in a small population based sample. Prog Neuropsychopharmacol Biol Psychiatry 33(1):49–52
Eberhard‐Gran M, Eskild A, Tambs K, Opjordsmoen S, Ove Samuelsen S (2001) Review of validation studies of the Edinburgh Postnatal Depression Scale. Acta Psychiatr Scand 104(4):243–249
Elliott SA, Leverton TJ, Sanjack M, Turner H, Cowmeadow P, Hopkins J, Bushnell D (2000) Promoting mental health after childbirth: a controlled trial of primary prevention of postnatal depression. Brit J Clin Psychol 39(3):223–241
Freeman M (2007) Antenatal depression: navigating the treatment dilemmas. Am J Psychol 164(8):1162–1165
Gamble J, Creedy D, Moyle W, Webster J, McAllister M, Dickson P (2005) Effectiveness of a counseling intervention after a traumatic childbirth: a randomized controlled trial. Birth 32(1):11–19
Gao L-l, Chan SW-c, Li X, Chen S, Hao Y (2010) Evaluation of an interpersonal-psychotherapy-oriented childbirth education programme for Chinese first-time childbearing women: a randomised controlled trial. Int J Nurs Stud 47(10):1208–1216
Goldberg D, Williams P (1988) A user’s guide to the General Health Questionnaire. NFER-Nelson, Slough
Goodman JH (2009) Women’s attitudes, preferences, and perceived barriers to treatment for perinatal depression. Birth 36(1):60–69
Grace SL, Evindar A, Stewart D (2003) The effect of postpartum depression on child cognitive development and behavior: a review and critical analysis of the literature. Arch Womens Ment Health 6(4):263–274
Grote N, Swartz H, Geibel S, Zuckoff A, Houck P, Frank E (2009) A randomized controlled trial of culturally relevant, brief interpersonal psychotherapy for perinatal depression. Psych Serv 60(3):313–321
Hagan R, Evans SF, Pope S (2004) Preventing postnatal depression in mothers of very preterm infants: a randomised controlled trial. BJOG 111(7):641–647
Harris B et al (2002) Randomised trial of thyroxine to prevent postnatal depression in thyroid-antibody-positive women. Brit J Psychiatr 180(4):327–330
Harrison-Hohner J, Coste S, Dorato V, Curet L, McCarron D, Hatton D (2001) Prenatal calcium supplementation and postpartum depression: an ancillary study to a randomized trial of calcium for prevention of preeclampsia. Arch Womens Ment Health 3(4):141–146
Hayes BA, Muller R, Bradley BS (2001) Perinatal depression: a randomized controlled trial of an antenatal education intervention for primiparas. Birth 28(1):28–35
Howell EA, Balbierz A, Wang J, Parides M, Zlotnick C, Leventhal H (2012) Reducing postpartum depressive symptoms among Black and Latina mothers: a randomized controlled trial. Obstet Gynecol 119(5):942
Hunziker UA, Barr RG (1986) Increased carrying reduces infant crying: a randomized controlled trial. Pediatrics 77(5):641–648
Klerman GL, Weissman MM (1993) New applications of interpersonal psychotherapy: American Psychiatric Publishing, Arlington, VA
Kost K, Landry DJ, Darroch JE (1998) Predicting maternal behavior during pregnancy: does intention status matter? Fam Plann Perspect 30(2):79
Kozinszky Z et al (2012) Can a brief antepartum preventive group intervention help reduce postpartum depressive symptomatology? Psychother Psychosom 81(2):98–107
Kurstjens S, Wolke D (2001) Effects of maternal depression on cognitive development of children over the first 7 years of life. J Child Psychol Psychiatry 42(5):623–636
Lara MA, Navarro C, Navarrete L (2010) Outcome results of a psycho-educational intervention in pregnancy to prevent PPD: a randomized control trial. J Affect Disord 122(1):109–117
Lavender T, Walkinshaw SA (1998) Can midwives reduce postpartum psychological morbidity? A randomized trial. Birth 25(4):215–219
Lawrie TA, Justus Hofmeyr G, Jager M, Berk M, Paiker J, Viljoen E (1998) A double‐blind randomised placebo controlled trial of postnatal norethisterone enanthate: the effect on postnatal depression and serum hormones. BJOG 105(10):1082–1090
Le H-N, Perry DF, Stuart EA (2011) Randomized controlled trial of a preventive intervention for perinatal depression in high-risk Latinas. J Consult Clin Psychol 79(2):135
Le H, Muñoz R (1998) The Maternal Mood Screener (MMS). Unpublished questionnaire, University of California, San Francisco
Llorente AM, Jensen CL, Voigt RG, Fraley JK, Berretta MC, Heird WC (2003) Effect of maternal docosahexaenoic acid supplementation on postpartum depression and information processing. Am J Obstet Gynecol 188(5):1348–1353
Makrides M, Gibson RA, McPhee AJ, Yelland L, Quinlivan J, Ryan P (2010) Effect of DHA supplementation during pregnancy on maternal depression and neurodevelopment of young children: a randomized controlled trial. JAMA 304(15):1675–1683
Mao HJ, Li HJ, Chiu H, Chan WC, Chen SL (2012) Effectiveness of antenatal emotional self‐management training program in prevention of postnatal depression in Chinese women. Perspect Psychiatr Clin 48(4):218–224
Marcus SM, Flynn HA, Blow FC, Barry KL (2003) Depressive symptoms among pregnant women screened in obstetrics settings. J Womens Health 12(4):373–380
Matthey S, Kavanagh DJ, Howie P, Barnett B, Charles M (2004) Prevention of postnatal distress or depression: an evaluation of an intervention at preparation for parenthood classes. J Affect Disord 79(1):113–126
Maxted AE et al (2005) Infant colic and maternal depression. Inf Ment Health J 26(1):56–68
Meyer LE, Erler T (2011) Swaddling: a traditional care method rediscovered. World J Pediatr 7(2):155–160
Milgrom J, Schembri C, Ericksen J, Ross J, Gemmill AW (2011) Towards parenthood: an antenatal intervention to reduce depression, anxiety and parenting difficulties. J Affect Disord 130(3):385–394
Mokhber N et al (2011) Effect of supplementation with selenium on postpartum depression: a randomized double-blind placebo-controlled trial. J Matern Fetal Neonatal Med 24(1):104–108
Morrell CJ, Spiby H, Stewart P, Walters S, Morgan A (2000) Costs and effectiveness of community postnatal support workers: randomised controlled trial. Brit Med J 321(7261):593
Muñoz RF et al (2007) Prevention of postpartum depression in low-income women: development of the Mamás y Bebés/Mothers and Babies course. Cogn Behav Pract 14(1):70–83
O'Hara MW, Swain AM (1996) Rates and risk of postpartum depression—a meta-analysis. Int Rev Psychiatr 8(1):37–54
Osborne LM, Monk C (2013) Perinatal depression—the fourth inflammatory morbidity of pregnancy?: theory and literature review. Psychoneuroendocrinology 38(10):1929–1952
Phipps MG, Raker CA, Ware CF, Zlotnick C (2013) Randomized controlled trial to prevent postpartum depression in adolescent mothers. Am J Obstet Gynecol. doi:10.1016/j.ajog.2012.12.036
Pinilla T, Birch LL (1993) Help me make it through the night: behavioral entrainment of breast-fed infants’ sleep patterns. Pediatrics 91(2):436–444
Priest SR, Henderson J, Evans SF, Hagan R (2003) Stress debriefing after childbirth: a randomised controlled trial. Med J Aust 178(11):542–545
Radloff LS (1977) The CES-D scale a self-report depression scale for research in the general population. App Psych Meas 1(3):385–401
Reid M, Glazener C, Murray G, Taylor G (2002) A two‐centred pragmatic randomised controlled trial of two interventions of postnatal support. BJOG 109(10):1164–1170
Richards JP (1990) Postnatal depression: a review of recent literature. Brit J Gen Pract 40(340):472
Rose S, Bisson J, Churchill R, Wessely S (2002) Psychological debriefing for preventing post traumatic stress disorder (PTSD). Cochrane Database Syst Rev, 2(2)
Saigal S, Doyle LW (2008) An overview of mortality and sequelae of preterm birth from infancy to adulthood. Lancet 371(9608):261–269
Seguin L, Potvin L, St‐Denis M, Loiselle J (1999) Depressive symptoms in the late postpartum among low socioeconomic status women. Birth 26(3):157–163
Sichel DA, Cohen LS, Robertson LM, Ruttenberg A, Rosenbaum JF (1995) Prophylactic estrogen in recurrent postpartum affective disorder. Biol Psychiatry 38(12):814–818
Silverstein M et al (2011) Problem-solving education to prevent depression among low-income mothers of preterm infants: a randomized controlled pilot trial. Arch Womens Ment Health 14(4):317–324
Skrundz M, Bolten M, Nast I, Hellhammer DH, Meinlschmidt G (2011) Plasma oxytocin concentration during pregnancy is associated with development of postpartum depression. Neuropsychopharmacology 36(9):1886–1893
Small R, Lumley J, Donohue L, Potter A, Waldenström U (2000) Randomised controlled trial of midwife led debriefing to reduce maternal depression after operative childbirth. Brit Med J 321(7268):1043–1047
Small R, Lumley J, Toomey L (2006) Midwife-led debriefing after operative birth: four to six year follow-up of a randomised trial [ISRCTN24648614]. BMC Med 4(1):3
Spinelli MG, Endicott J (2003) Controlled clinical trial of interpersonal psychotherapy versus parenting education program for depressed pregnant women. Am J Psychiatr 160(3):555–562
St James-Roberts I et al (1995) Supplementary carrying compared with advice to increase responsive parenting as interventions to prevent persistent infant crying. Pediatrics 95(3):381–388
Stamp GE, Williams AS, Crowther CA (1995) Evaluation of antenatal and postnatal support to overcome postnatal depression: a randomized, controlled trial. Birth 22(3):138–143
Symon BG, Marley JE, James Martin A, Norman ER (2005) Effect of a consultation teaching behaviour modification on sleep performance in infants: a radomised controlled trial. Med J Aust 182(5):215–218
Tam WH, Lee DTS, Chiu HFK, Ma KC, Lee A, Chung TKH (2003) A randomised controlled trial of educational counselling on the management of women who have suffered suboptimal outcomes in pregnancy. BJOG 110(9):853–859
Tandon SD, Perry DF, Mendelson T, Kemp K, Leis JA (2011) Preventing perinatal depression in low-income home visiting clients: a randomized controlled trial. J Consult Clin Psychol 79(5):707
Thomas JL, Jones GN, Scarinci IC, Mehan DJ, Brantley PJ (2001) The utility of the CES-D as a depression screening measure among low-income women attending primary care clinics. Int J Psychiatry Med 31(1):25–40
Vik T et al (2009) Infantile colic, prolonged crying and maternal postnatal depression. Acta Paediatr 98(8):1344–1348
Wiggins M et al (2005) Postnatal support for mothers living in disadvantaged inner city areas: a randomised controlled trial. J Epidemiol Commun Health 59(4):288–295
Wisner KL, Perel JM, Peindl KS, Hanusa BH, Piontek CM, Findling RL (2004) Prevention of postpartum depression: a pilot randomized clinical trial. Am J Psychiatr 161(7):1290–1292
Zayas LH, McKee MD, Jankowski KR (2004) Adapting psychosocial intervention research to urban primary care environments: a case example. Ann Fam Med 2(5):504–508
Zhu P et al (2014) Does prenatal maternal stress impair cognitive development and alter temperament characteristics in toddlers with healthy birth outcomes? Dev Med Child Neurol 56(3):283–289
Zlotnick C, Capezza NM, Parker D (2011) An interpersonally based intervention for low-income pregnant women with intimate partner violence: a pilot study. Arch Womens Ment Health 14(1):55–65
Zlotnick C, Johnson SL, Miller IW, Pearlstein T, Howard M (2001) Postpartum depression in women receiving public assistance: pilot study of an interpersonal-therapy-oriented group intervention. Am J Psychiatr 158(4):638–640
Zlotnick C, Miller I, Pearlstein T, Howard M, Sweeney P (2006) A preventive intervention for pregnant women on public assistance at risk for postpartum depression. Am J Psychiatr 163(8):1443–1445
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
About this article

Cite this article
Werner, E., Miller, M., Osborne, L.M. et al. Preventing postpartum depression: review and recommendations. Arch Womens Ment Health 18, 41–60 (2015). https://doi.org/10.1007/s00737-014-0475-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00737-014-0475-y