
Abstract
Objective
Fatigue is one of the most prevalent and significant symptoms experienced by breast cancer patients. This study aimed to investigate potential population heterogeneity in fatigue symptoms of the patients using the innovative non-normal mixture modeling.
Methods
A sample of 197 breast cancer patients completed the brief fatigue inventory and other measures on cancer symptoms. Non-normal factor mixture models were analyzed and compared using the normal, t, skew-normal, and skew-t distributions. Selection of the number of latent classes was based on the Bayesian information criterion (BIC). The identified classes were validated by comparing their demographic profiles, clinical characteristics, and cancer symptoms using a stepwise distal outcome approach.
Results
The observed fatigue items displayed slight skewness but evident negative kurtosis. Factor mixture models using the normal distribution pointed to a 3-class solution. The t distribution mixture models showed the lowest BIC for the 2-class model. The restored class (52.5 %) exhibited moderate severity (item mean = 2.8–3.2) and low interference (item mean = 1.1–1.9). The exhausted class (47.5 %) displayed high levels of fatigue severity and interference (item mean = 5.8–6.6). Compared to the restored class, the exhausted class reported significantly higher perceived stress, anxiety, depression, pain, sleep disturbance, and lower quality of life.
Conclusions
The non-normal factor mixture models suggest two distinct subgroups of patients on their fatigue symptoms. The presence of the exhausted class with exacerbated symptoms calls for a proactive assessment of the symptoms and development of tailored interventions for this subgroup.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Cancer-related fatigue is a subjective symptom experience that is rarely relieved by sleep or rest [1]. It is described as persistent feelings of exhaustion and lack of energy and is one of the most commonly reported symptoms among breast cancer patients [2]. It can occur during the course of the disease and persist for years after treatment completion [3]. An essential characteristic of cancer-related fatigue is the inability of the patient to maintain a prior level of physical functioning, thus affecting daily life and work performance. Rather than as an isolated symptom, fatigue often arises in symptom clusters [4] and has been associated with other symptoms such as pain, anxiety, depression, and sleep problems [5, 6]. Given its prevalence and influence on breast cancer patients, valid and precise assessment of fatigue is necessary. A common goal of categorical analytic approach is to explore the cluster patterns in study samples. The conventional practice of artificial categorization of continuous variables (e.g., dichotomization on a median split) suffers from methodological drawbacks, namely, attenuation in correlations among variables, measurement precision, and statistical power [7].
Dirksen, Belyea, and Epstein [8] conducted a latent profile analysis to investigate the cluster patterns of fatigue symptoms among 86 breast cancer survivors. Three latent classes, including exhausted (35 %), tired (41 %), and restored (24 %) subgroups, were identified. The exhausted subgroup showed significantly higher levels of insomnia, anxiety, depression, and lower quality of life than the other subgroups. Latent profile analysis is a categorical modeling technique that classifies individuals into unobserved subgroups with distinct profiles [9] and is methodologically more applicable than artificial categorization. Yet, this technique assumes conditional independence for the fatigue items and does not account for expected within-subgroup heterogeneity. Factor mixture analysis is a hybrid and flexible mixture modeling technique which simultaneously investigates the existence of unobserved subgroups while accounting for the underlying factor structure [10]. It explicitly models the heterogeneity both between and within the latent classes.
The aim of this study was to investigate potential population heterogeneity in fatigue symptoms of breast cancer patients via factor mixture modeling. However, it is well known that traditional mixture modeling relies heavily on the within-class normality assumption [11]. Violation of this assumption can result in formation of spurious classes, i.e., latent subgroups that exist only to accommodate the heavy tails of non-normal distributions [12]. That non-normality can lead to extraction of non-substantive latent classes in traditional mixture modeling could compromise the authenticity of the results. The present study adopted the non-normal mixture modeling approach implemented recently in Mplus version 7.2 by Asparouhou and Muthén [13]. This pioneering approach explicitly allows the within-class distributions to be skewed and to have heavy tails, thereby preventing the formation of spurious classes that merely compensate for distributional deviations from standard normal distribution [14]. To our knowledge, this study is the first to apply non-normal mixture modeling in the context of fatigue symptoms.
Methods
Sample
A secondary analysis was conducted with data obtained from a randomized clinical trial that evaluated the efficacy of a movement-based psychotherapy program between January 2011 and December 2012. Study participants were female patients diagnosed with breast cancer and aged 18 years old or above. The exclusion criteria included metastases of breast cancer, a history of psychiatric illness, pregnancy, and inability to understand Chinese. A total of 370 breast cancer patients were invited via mail and telephone and 53 of them were not eligible to join the study. The data used in this analysis were obtained at baseline from 197 women who were recruited via convenience sampling from local hospitals and community cancer support centers in Hong Kong. Ethical approval was obtained from the local institutional review board.
The participants provided written informed consents and completed a self-report questionnaire in a paper-and-pencil format. The participants reported a mean age of 49.4 years (SD = 8.0) and an average cancer duration of 23.1 months (SD = 7.5). Most of the participants were married (64.5 %), had completed at least secondary education (77.7 %), and were diagnosed with stage I (26.0 %) or II (43.2 %) breast cancer. The majority of the sample had received lumpectomy (56.4 %), chemotherapy (78.1 %), and was receiving adjuvant radiotherapy (70.1 %).
Measures
Fatigue symptoms among the cancer patients were assessed by the 9-item, 11-point brief fatigue inventory (BFI) [15]. The first three items inquire fatigue severity at the current, usual, and worst times during the past 24 h. The following six items assess the interference caused by fatigue on general activity, mood, walking ability, normal work, relationships with other people, and enjoyment of life. Previous studies [15, 16] suggest a unidimensional structure for the BFI. Nevertheless, none of these studies systematically verify the structure against alternative factor models. In the present study, the model fit of the one-factor model was statistically evaluated and compared with the two-factor model via confirmatory factor analysis.
The self-report questionnaire also included measurement instruments on several psychopathological variables. Perceived stress was measured by the 10-item, 5-point Perceived Stress Scale [17], with the scale score ranging from 0 to 40. Anxiety and depression were assessed using the 14-item, 4-point Hospital Anxiety and Depression Scale [18], with the scale scores for anxiety (7 items) and depression (7 items) ranging from 0 to 21. Pain was measured by the 11-item, 11-point Brief Pain Inventory [19], with the scale scores for pain severity (4 items) and pain interference (7 items) ranging from 0 to 10. Sleep disturbance was assessed by the 19-item Pittsburgh Sleep Quality Index [20]. The scale measures seven components on a 4-point format, with the scale score ranging from 0 to 21. Quality of life was measured by the 36-item, 5-point Functional Assessment of Cancer Therapy—Breast [21], with the scale score ranging from 0 to 144. In this study, satisfactory reliability was found for all of the measurement scales (Cronbach’s α = 0.79–0.97).
Data analysis
Confirmatory factor analysis
The factor structure of the BFI was examined using confirmatory factor analyses on the one- and two-factor models. The two-factor model specified two factors on fatigue severity (measured by three items) and interference (measured by six items). The model fit was evaluated via the following fit indices: comparative fit index (CFI), root mean square error of approximation (RMSEA), and standardized root mean square residuals (SRMR) [22]. chi-square difference test was used to compare the model fit of the two models. All analyses were carried out in Mplus version 7.2 [23] using robust maximum-likelihood estimator. Missing data were handled via full-information maximum likelihood under the missing-at-random assumption [24].
Factor mixture models
We first scrutinized the skewness, kurtosis, and distributions of the BFI items. For conventional mixture models, violations of within-class normality assumption can result extracting non-substantive latent classes that merely represent statistical features of the data [12]. Non-normal mixture modeling resolves this problem by facilitating specification of a mixture of non-normal distributions to the data [13]. In addition to normal distributions, a range of non-normal distributions, namely, skew-normal, t, and skew-t [25], can be specified. The skew-normal distribution accounts for excessive skewness by adding a skew parameter to the model [26, 27]. The t distribution accounts for excessive kurtosis by adding a degree of freedom parameter. The skew-t distribution accounts for both excessive skewness and kurtosis, by adding skew and degree of freedom parameters [14, 28]. Essentially, non-normal mixture models can fit the data considerably better than normal mixtures and reduce the risk of extracting spurious latent classes due to non-normality.
In the present study, non-normal mixture modeling was performed using the new DISTRIBUTION = TDIST/SKEWNORMAL/SKEWT command in Mplus version 7.2. We first estimated the one-class factor mixture model using default normal distributions and compared its model fit to the non-normal mixture counterparts using t, skew-normal, and skew-t distributions. Skew and degree of freedom parameters were incorporated in the mixture models when necessary to correct for non-normality of the variables. Factor mixture models with increasing classes were then specified subsequently to the data to determine the optimal number of class in the sample. The models were fitted with class-invariant factor loadings and residual variances and class-varying item intercepts, factor variances, and factor covariance. To avoid convergence on a local solution, all mixture models were estimated using 100 random starting values and 20 final stage optimizations to replicate the best log-likelihood.
Model selection was based on the Bayesian information criterion (BIC) [29, 30]. The BIC balances the model log-likelihood by imposing a penalty term for the number of model parameters, with a lower value of BIC to be preferred. Differences of 2 to 6, 6 to 10, and greater than 10 denote positive, strong, and very strong evidence against the models with higher BIC, respectively. Average posterior class probabilities and entropy of the models were reported [31]. Entropy is a measure of the model’s classification accuracy with a value close to 1 denotes greater accuracy. Substantive checking of the latent classes was performed in relation to the demographic profiles, clinical characteristics, and psychopathological variables [32]. Equality of means or proportions across the classes were tested for continuous or categorical variables, respectively, using the stepwise distal outcome method [33].
Results
BFI items statistics
Table 1 displays the descriptive statistics of the BFI items. The participants reported moderate (≈5) mean levels of fatigue severity. On average, they showed low to moderate levels of fatigue interference, with a range of 3.3 (relationships with others) to 4.5 (normal work). The items showed small degree of skewness (|skew| ≈ 0.5). However, negative kurtosis was found for all items, in particular the six items assessing fatigue interference (kurtosis = −1.00 to −1.30). Figure 1 shows as an example the histogram for item 9 (enjoyment of life). Despite the overall mean of 4.0, only 6.1 % of the participants showed a score of 4 for this item, with 24.5 % scoring 3 or 5. Comparable proportions of participants showed either high (22.9 % scoring 7 or 8) or low (26.6 % scoring 0 or 1) levels of interference. The platykurtic distributions found for the items revealed signs of bimodal distributions.

Histogram and descriptive statistics for BFI item 9 (enjoyment of life)
Confirmatory factor analysis
The one-factor model fitted the data poorly, with χ 2(27) = 291.7, p < .001, CFI = 0.73, RMSEA = 0.22, and SRMR = 0.07. The two-factor model yielded an acceptable fit to the data with χ 2(26) = 67.3, p < .001, CFI = 0.96, RMSEA = 0.09, and SRMR = 0.04 and provided a significantly better fit than the one-factor model (Δχ 2(1) = 70.1, p < .001). As shown in Table 1, the factor loadings for the two factors (severity and interference) were significant (p < .001) and salient (λ ≥ 0.74). The two factors were positively and strongly correlated (r = 0.79, p < .001).
Factor mixture models
For the factor mixture models, the two latent factors, fatigue severity and interference, were modeled either as normal, t, skew-normal, or skew-t variables. The residuals of the factor indicators were assumed normal. Fit statistics of the factor mixture models under various distributions are presented in Table 2. Among the four 1-class models, both the t and skew-t distribution models showed improvements in BIC over the normally distributed model while the skew-normal distribution model resulted in a higher BIC. In the skew-t distribution model, the degree of freedom parameter (df = 3.34, SE = 0.66, p < .001) deviated considerably from that of the normal distribution (with df ≥ 30). Insignificant skew parameters were found for fatigue severity (skew = 0.72, SE = 0.71, p = .31) and interference (skew = −0.45, SE = 0.80, p = .57). These results suggest the need to account for excessive kurtosis but not excessive skewness in the present sample. Subsequent multi-class mixture models were estimated only under normal and t distributions. Under the normal distribution, the 3-class model displayed the lowest BIC (the 4-class model did not converge). Using the t distribution for the latent factors, however, showed the lowest BIC for the 2-class model. Importantly, the 2-class t distribution mixture model provided a substantially better BIC than the 3-class normal mixture model.
The 2-class t distribution mixture model
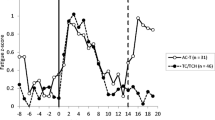
Figure 2 displays the estimated overall and class-specific distributions for BFI item 9 in the 2-class t distribution mixture model. In the figure, the overall bimodal distribution (denoted by solid curve) was decomposed into two t-distributed classes (denoted by the dotted and dashed lines) with df = 2.77 and 2.91. Figure 3 displays the response profile plot for the BFI items in the 2-class t distribution mixture model. The first class (N = 103, 52.5 %) was labeled the ‘restored’ class and showed moderate severity (item mean = 2.8–3.2) and low interference (item mean = 1.1–1.9). The second class (N = 94, 47.5 %) was labeled the ‘exhausted’ class and showed a consistent pattern of high levels of fatigue severity and interference (item mean = 5.8–6.6). Each of the item means in the exhausted class was above 5.0 and substantially higher than that in the restored class. The average posterior class probabilities (0.92 and 0.93 for the restored and exhausted class, respectively) suggest good classification accuracy for the model.

Estimated overall and class-specific distributions for BFI item 9 (enjoyment of life) in the 2-class t distribution mixture model

Response profile plot for the BFI items in the 2-class t distribution mixture model
Characteristics of the two latent classes
As shown in Table 3, the two classes did not differ significantly in age (χ 2(1) = 0.44, p = .51), cancer duration (χ 2(1) = 0.51, p = .48), education (χ 2(2) = 4.72, p = .09), marital status (χ 2(1) = 0.23, p = .63), stage at diagnosis (χ 2(3) = 1.38, p = .71), surgery type (χ 2(1) = 1.00, p = .32), chemotherapy (χ 2(1) = 0.01, p = .94), and adjuvant radiotherapy (χ 2(1) = 1.49, p = .22). The restored class was composed of a significantly greater proportion of participants who received patient support service (χ 2(1) = 3.99, p = .046).
Table 4 shows the participant scores on the psychopathological variables for the two fatigue classes. The exhausted class reported significantly higher levels of perceived stress (χ 2(1) = 60.98, p < .001), anxiety (χ 2(1) = 56.03, p < .001), depression (χ 2(1) = 57.68, p < .001), pain severity (χ 2(1) = 30.82, p < .001), pain interference (χ 2(1) = 40.72, p < .001), and sleep disturbance (χ 2(1) = 4.78, p = .029) than the restored class. The exhausted class had a significantly lower level of quality of life (χ 2(1) = 84.11, p < .001) than the restored class.
Discussion
As Piper and Cella [34] remarked, it is clinically relevant to determine whether cancer patients can be classified into specific distinct and meaningful subgroups based on their fatigue symptoms. The present study investigated potential population heterogeneity in fatigue symptoms in a sample of breast cancer patients via an innovative use of non-normal mixture modeling. Regarding the latent structure of the BFI, the two-factor model composing of fatigue severity and fatigue interference was found to be superior to the one-factor model. This finding suggests future research to differentiate the degrees of severity and interference caused by fatigue in various aspects of life for a deeper understanding of cancer-related fatigue.
Results of factor mixture modeling suggest the existence of two latent subgroups with distinct profiles of fatigue symptoms. Nearly, half of the sample (47.5 %) belonged to the exhausted class with consistently high levels of fatigue severity and interference. This class showed significantly greater perceived stress, anxiety, depression, pain severity, pain interference, and sleep disturbance than the restored class. In line with the literature on symptom clustering [35, 36], these exacerbated symptoms may coexist and interact in leading to a poor quality of life in the exhausted class. This finding informs clinicians to be aware of a comprehensive treatment of not only the fatigue symptoms, but also the comorbid symptoms of the patients for a holistic improvement. Active management of the associated symptoms in an earlier stage of treatment may facilitate prevention or amelioration of cancer-related fatigue in the patients.
The present results somewhat resemble the findings by Dirksen, Belyea, and Epstein [8], which pointed to a three-class model including the exhausted, restored, and tired classes. However, the tired class did not differ from the restored class in most of the symptoms, which weakens the discriminant validity and substantive meanings of their model. The overextraction of latent class can be attributed to violations of the local independence assumption in latent profile analysis [10]. Our factor mixture model, which allows for both within-class covariation and non-normality of the variables, is likely a more realistic and parsimonious model of the fatigue symptoms.
Identifying the population heterogeneity in fatigue symptoms could provide future directions in providing quality care to the patients. From a substantive point of view, the present two-class two-factor mixture model may hold greater clinical utility over a regular two-factor model and facilitate diagnostic decision making [37]. The current results call for a proactive assessment of the heightened symptoms and development of tailored interventions for the exhausted class. Similar to the findings by Dirksen, Belyea, and Epstein [8], our two subgroups displayed similar demographic and clinical characteristics. An exception was that the restored class comprised a significantly greater proportion of patients who had received patient support service. This appears to suggest beneficial effects of patient support service for patients with breast cancer.
From an analytical perspective, non-normal factor mixture modeling is a flexible methodology that allows us to examine the potential unobserved heterogeneity and within-class item covariation simultaneously. This technique relaxes the usual within-class normality assumption and accommodates skewed or heavy tails in the distributions. Mixture of skew-t distributions avoids the formation of spurious classes due to non-normality and skewness and is more likely to extract substantive latent classes that are of theoretical interest. In the present study, the non-normal mixture models resulted in largely insignificant skew parameters. This finding is consistent with the slight skewness of the BFI items. However, the items appeared to violate the normal distribution assumption with considerable negative kurtosis. The use of t distribution mixture model not only accounts for the observed kurtosis but also helps remove one of the classes found in the normally distributed model. In addition to eliminating the potentially spurious class that lack proper interpretation, a notably better fitting model was actually found via the non-normal mixture model. These findings support further use of non-normal mixture modeling in exploring potential underlying heterogeneity in the likely presence of non-normality of the variables.
The present study is the first of its kind to apply non-normal factor mixture modeling to evaluate the underlying population heterogeneity of cancer-related fatigue symptoms. The current findings may be limited in their generalizability due to the modest sample size and self-selection sampling bias. The present study was based on cross-sectional self-report measures and may be subject to common method bias. Despite these limitations, the results of non-normal mixture models demonstrate clear support for a two-class two-factor structure for fatigue symptoms that has clinical implications. Further studies are recommended to investigate the potential unobserved heterogeneity in larger samples of cancer patients. It would be of particular interest to elucidate significant predictors of the fatigue classes and study the longitudinal change in the fatigue-based class membership in future studies.
References
Curt, G. A., Breitbart, W., Cella, D., Groopman, J. E., Horning, S. J., Itri, L. M., et al. (2000). Impact of cancer-related fatigue on the lives of patients: New findings from the Fatigue Coalition. The Oncologist, 5(5), 353–360.
Meeske, K., Smith, A., Alfano, C., McGregor, B., McTiernan, A., Baumgartner, K., et al. (2007). Fatigue in breast cancer survivors two to five years post diagnosis: A HEAL Study report. Quality of Life Research, 16(6), 947–960. doi:10.1007/s11136-007-9215-3.
Horneber, M., Fischer, I., Dimeo, F., Rüffer, J. U., & Weis, J. (2012). Cancer-related fatigue: Epidemiology, pathogenesis, diagnosis, and treatment. Deutsches Arzteblatt International, 109(9), 161–171. (quiz 172).
Skerman, H., Yates, P., & Battistutta, D. (2012). Cancer-related symptom clusters for symptom management in outpatients after commencing adjuvant chemotherapy, at 6 months, and 12 months. Supportive Care in Cancer, 20(1), 95–105. doi:10.1007/s00520-010-1070-z.
Lockefeer, J. P. M., & De Vries, J. (2013). What is the relationship between trait anxiety and depressive symptoms, fatigue, and low sleep quality following breast cancer surgery? Psycho-Oncology, 22(5), 1127–1133. doi:10.1002/pon.3115.
Mosher, C. E., & DuHamel, K. N. (2012). An examination of distress, sleep, and fatigue in metastatic breast cancer patients. Psycho-Oncology, 21(1), 100–107. doi:10.1002/pon.1873.
MacCallum, R. C., Zhang, S. B., Preacher, K. J., & Rucker, D. D. (2002). On the practice of dichotomization of quantitative variables. Psychological Methods, 7(1), 19–40. doi:10.1037/1082-989x.7.1.19.
Dirksen, S. R., Belyea, M. J., & Epstein, D. R. (2009). Fatigue-based subgroups of breast cancer survivors with insomnia. Cancer Nursing, 32(5), 404–411.
Vermunt, J. K., & Magidson, J. (2002). Latent class cluster analysis. In J. A. Hagenaars & A. L. McCutcheon (Eds.), Applied latent class analysis (pp. 89–106). Cambridge, MA: Cambridge University Press.
Lubke, G. H., & Muthén, B. (2005). Investigating population heterogeneity with factor mixture models. Psychological Methods, 10(1), 21–39. doi:10.1037/1082-989X.10.1.21.
Bauer, D. J., & Curran, P. J. (2003). Distributional assumptions of growth mixture models: Implications for overextraction of latent trajectory classes. Psychological Methods, 8(3), 338–363. doi:10.1037/1082-989x.8.3.338.
Bauer, D. J., & Curran, P. J. (2003). Overextraction of latent trajectory classes: Much ado about nothing? Reply to Rindskopf (2003), Muthen (2003), and Cudeck and Henly (2003). Psychological Methods, 8(3), 384–393. doi:10.1037/1082-989x.8.3.384.
Asparouhov, T., & Muthen, B. (2014). Structural equation models and mixture models with continuous non-normal skewed distributions. Mplus Web Note, 19, 1–49.
Lee, S., & McLachlan, G. J. (2014). Finite mixtures of multivariate skew t-distributions: Some recent and new results. Statistics and Computing, 24(2), 181–202. doi:10.1007/s11222-012-9362-4.
Wang, X. S., Hao, X. S., Wang, Y., Guo, H., Jiang, Y. Q., Mendoza, T. R., et al. (2004). Validation study of the Chinese version of the brief fatigue inventory (BFI-C). Journal of Pain and Symptom Management, 27(4), 322–332. doi:10.1016/j.jpainsymman.2003.09.008.
Lin, C. C., Chang, A. P., Chen, M. L., Cleeland, C. S., Mendoza, T. R., & Wang, X. S. (2006). Validation of the Taiwanese version of the Brief Fatigue Inventory. Journal of Pain and Symptom Management, 32(1), 52–59. doi:10.1016/j.jpainsymman.2005.12.019.
Leung, D. Y. P., Lam, T. H., & Chan, S. S. C. (2010). Three versions of Perceived Stress Scale: Validation in a sample of Chinese cardiac patients who smoke. BMC Public Health, 10, 513. doi:10.1186/1471-2458-10-513.
Fong, T. C. T., & Ho, R. T. H. (2013). Factor analyses of the Hospital Anxiety and Depression Scale: A Bayesian structural equation modeling approach. Quality of Life Research, 22(10), 2857–2863. doi:10.1007/s11136-013-0429-2.
Wang, X. S., Mendoza, T. R., Gao, S.-Z., & Cleeland, C. S. (1996). The Chinese version of the Brief Pain Inventory (BPI-C): Its development and use in a study of cancer pain. Pain, 67(2–3), 407–416. doi:10.1016/0304-3959(96)03147-8.
Tsai, P. S., Wang, S. Y., Wang, M. Y., Su, C. T., Yang, T. T., Huang, C. J., et al. (2005). Psychometric evaluation of the Chinese version of the Pittsburgh Sleep Quality Index (CPSQI) in primary insomnia and control subjects. Quality of Life Research, 14(8), 1943–1952. doi:10.1007/s11136-005-4346-x.
Wan, C., Zhang, D., Yang, Z., Tu, X., Tang, W., Feng, C., et al. (2007). Validation of the simplified Chinese version of the FACT-B for measuring quality of life for patients with breast cancer. Breast Cancer Research and Treatment, 106(3), 413–418. doi:10.1007/s10549-007-9511-1.
Kline, R. B. (2011). Principles and practice of structural equation modeling (3rd ed.). New York: Guilford Press.
Muthén, L. K., & Muthén, B. (1998-2012). Mplus user’s guide (7th ed.). Los Angeles, CA: Muthen & Muthen.
Little, R. J. A., & Rubin, D. B. (1987). Statistical analysis with missing data. New York: Wiley.
Azzalini, A. (1985). A class of distributions which includes the normal ones. Scandinavian Journal of Statistics, 12(2), 171–178.
Lin, T. I., Lee, J. C., & Yen, S. Y. (2007). Finite mixture modelling using the skew normal distribution. Statistica Sinica, 17(3), 909–927.
Azzalini, A., & DallaValle, A. (1996). The multivariate skew-normal distribution. Biometrika, 83(4), 715–726. doi:10.1093/biomet/83.4.715.
Lin, T.-I. (2010). Robust mixture modeling using multivariate skew t distributions. Statistics and Computing, 20(3), 343–356. doi:10.1007/s11222-009-9128-9.
Nylund, K. L., Asparoutiov, T., & Muthén, B. O. (2007). Deciding on the number of classes in latent class analysis and growth mixture modeling: A Monte Carlo simulation study. Structural Equation Modeling-a Multidisciplinary Journal, 14(4), 535–569.
Fraley, C., & Raftery, A. E. (1998). How many clusters? Which clustering method? Answers via model-based cluster analysis. Computer Journal, 41(8), 578–588. doi:10.1093/comjnl/41.8.578.
Celeux, G., & Soromenho, G. (1996). An entropy criterion for assessing the number of clusters in a mixture model. Journal of Classification, 13(2), 195–212. doi:10.1007/bf01246098.
Muthén, B. (2003). Statistical and substantive checking in growth mixture modeling: Comment on Bauer and Curran (2003). Psychological Methods, 8(3), 369–377. doi:10.1037/1082-989x.8.3.369.
Lanza, S. T., Tan, X., & Bray, B. C. (2013). Latent class analysis with distal outcomes: A flexible model-based approach. Structural Equation Modeling: A Multidisciplinary Journal, 20(1), 1–26. doi:10.1080/10705511.2013.742377.
Piper, B. E., & Cella, D. (2010). Cancer-related fatigue: Definitions and clinical subtypes. Journal of the National Comprehensive Cancer Network, 8(8), 958–966.
Molassiotis, A., Wengström, Y., & Kearney, N. (2010). Symptom cluster patterns during the first year after diagnosis with cancer. Journal of Pain and Symptom Management, 39(5), 847–858. doi:10.1016/j.jpainsymman.2009.09.012.
Liu, L. Q., Fiorentino, L., Natarajan, L., Parker, B. A., Mills, P. J., Sadler, G. R., et al. (2009). Pre-treatment symptom cluster in breast cancer patients is associated with worse sleep, fatigue and depression during chemotherapy. Psycho-Oncology, 18(2), 187–194. doi:10.1002/pon.1412.
Sunderland, M., Carragher, N., Wong, N., & Andrews, G. (2013). Factor mixture analysis of DSM-IV symptoms of major depression in a treatment seeking clinical population. Comprehensive Psychiatry,. doi:10.1016/j.comppsych.2012.12.011.
Acknowledgments
We would like to thank Hong Kong Cancer Fund, Queen Mary Hospital, Pamela Youde Nethersole Eastern Hospital, and Dr. M.Y. Luk for their help in patient recruitment and all the patients who participated in the study. The paper would not have been possible without the expert opinions and generous help offered by Dr. Bengt Muthén and the non-normal mixture modeling recently implemented in Mplus version 7.2.
Conflict of interest
The authors report no conflict of interests. The first author (R.T.H.H.) was supported by the Research Grants Council General Research Fund (HKU745110H) for this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Ho, R.T.H., Fong, T.C.T. & Cheung, I.K.M. Cancer-related fatigue in breast cancer patients: factor mixture models with continuous non-normal distributions. Qual Life Res 23, 2909–2916 (2014). https://doi.org/10.1007/s11136-014-0731-7
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-014-0731-7