
Abstract
Purpose
To assess the predictive validity of the 15 components of the Tilburg Frailty Indicator (TFI), a self-report questionnaire, for quality of life domains physical health, psychological, social relations and environmental in community-dwelling older persons in a longitudinal study.
Methods
The predictive validity of the components of the TFI was tested in a sample of 484 community-dwelling persons aged 75 years and older in the Netherlands in 2008 (response rate 42 %). A subset of all respondents participated two years later, in 2010 (n = 261, 54 %), and a subset of these respondents participated again in 2012 (n = 196, 75 %). The WHOQOL-BREF was used for measuring four quality of life domains.
Results
Four physical frailty components (physical unhealthy, difficulty in maintaining balance, difficulty in walking and physical tiredness), one psychological frailty component (feeling down) and one social frailty component (lack of social support) predicted future scores on quality of life domains, even after controlling for background characteristics and diseases.
Conclusion
This longitudinal study showed that quality of life is predicted by physical as well as psychological and social frailty components. This finding emphasizes the relevance of a multidimensional assessment of frailty. To improve quality of life of older persons, special attention should go to the screening and subsequent interventions focusing on the frailty components difficulty in walking, feeling down and lack of social support.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Frailty has become an increasingly relevant concept in gerontology and geriatrics. However, there is still no consensus on the definition of frailty [1]. The debate mainly focused on whether frailty should be defined purely in terms of biomedical factors (e.g., the phenotype of frailty) [2] or whether psychological and social factors should be included as well [3, 4]. According to more and more researchers, an integral approach is needed to understand the concept of frailty [3–7]; if the definition of frailty is exclusively focused on biomedical factors, attention for the older person as a whole will be jeopardized [3, 8].
After a literature study and consultation of experts, we have proposed the following multidimensional definition of frailty: ‘Frailty is a dynamic state affecting an individual who experiences losses in one or more domains of human functioning (physical, psychological, social), caused by the influence of a range of variables and which increases the risk of adverse outcomes’ [4, 9]. An integral conceptual model of frailty was formulated, including both antecedents (life-course determinants and diseases) and consequences of frailty (disability, health care utilization, death) [10, 11]. Moreover, a multidimensional instrument for assessing frailty, the Tilburg Frailty Indicator (TFI), was constructed [12]. Employing the TFI, the Netherlands Institute for Social Research estimated that in the Netherlands, 24 % of community-dwelling persons aged 65 years and older was frail in 2007 [13]. Early identification of frail older persons is important because frailty is predictive of adverse outcomes, including disability [2, 14, 15], hospitalization [2], institutionalization [16, 17] and mortality [2, 16, 17]. Cross-sectional research shows that frailty is also associated with reduced quality of life of older persons [12, 18–20].
Quality of life has been defined by the World Health Organization Quality of Life Group (1995, p. 1405) as ‘an individual’s perception of their position in life in the context of the culture and value system in which they live and in relation to their goals, expectations, standards and concerns’ [21]. This definition reflects the view that quality of life refers to a subjective evaluation that is embedded in a cultural, social and environmental context [22] and implies a broad assessment of the concept related to many aspects of human life [23]. Quality of life is not only an important variable in itself, it also predicts adverse outcomes. For instance, poor quality of life in community-dwelling persons aged 65 and older is a predictor of nursing home placement as well as death within a year, after controlling for disability and physical frailty [24]. Therefore, from a preventive interventions perspective, it is important to attempt to predict quality of life.
A recent cross-sectional study carried out in a sample of Dutch people aged 65 years and older showed that all dimensions of frailty (physical, psychological, social), assessed with the TFI, were associated with each quality of life domain (physical health, psychological, social relations, environmental) [25]. The cross-sectional study showed that the physical frailty component physical tiredness and the psychological frailty component feeling down were associated with each quality of life domain. The aim of this study was to assess the predictive validity of the components of the TFI for quality of life domains physical health, psychological, social relations and environmental in community-dwelling older persons in a longitudinal study. The present study is a continuation at 4 years of follow-up of a previous published study with 2-year follow-up that included frailty and quality of life as well as other adverse outcomes [26]. This study not only differs from the previous study and other studies [11, 12] in time frame but also in focusing on the predictive potential of frailty components rather than on dimensions of frailty; frailty components are more specific, providing more guidance for interventions by health care professionals.
Methods
Study population and data collection
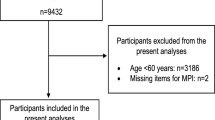
The data used in this article are part of a larger study on frailty [26, 27], based on a sample of 1,154 community-dwelling older people (≥75 years) randomly drawn from a register of the municipality in Roosendaal (the Netherlands), a town of 78,000 inhabitants, in 2008. A total of 484 persons participated in the study (42 % response rate) [26, 27]. In June 2008, the participants completed the TFI and the WHOQOL-BREF and answered questions on socio-demographic background characteristics and chronic diseases. A subset of all 484 respondents completed the same questionnaire again 2 years later, in June 2010 (n = 261, 54 % response rate), and a subset of those who participated in June 2010 once more, 2 years later, in June 2012 (n = 196, 75 % response rate).
Informed consent for the collection and use of information was obtained from all participants. Medical ethics approval was not required since particular treatments or interventions were not offered or withheld from respondents as a consequence of participating in the study (the main criterion in medical ethical procedures in the Netherlands) [28].
Measures
Frailty
Frailty was assessed using part B of the TFI, a user-friendly self-report questionnaire. Part B contains fifteen questions on components of frailty [12]. Physical frailty consists of eight components: unexplained weight loss, physical unhealthy, difficulty in walking, difficulty in maintaining balance, vision problems, hearing problems, lack of strength in the hands and physical tiredness. Psychological frailty includes problems with memory, feeling down, feeling anxious or nervous and unable to cope with problems. Social frailty consists of three components: living alone, lack of social relations and lack of social support. Eleven items from the TFI have two response categories, ‘yes’ and ‘no’; four items have three response categories, ‘yes,’ ‘sometimes’ and ‘no’; the item problems with memory was dichotomized into ‘yes’ and ‘sometimes or no,’ the other three items (feeling down, feeling anxious or nervous and lack of social relations) were dichotomized into ‘yes or sometimes’ and ‘no.’ The score ‘1’ was given per component if participants reported a problem; the score ‘0’ was given if they reported no problem. In previous studies using samples of community-dwelling people, the TFI has shown good reliability and construct validity [12, 29], and good predictive validity for adverse outcomes disability and indicators of health care utilization [26]. The TFI was also a powerful predictor of death, independent of age, sex and education [30].
Quality of life
The WHOQOL-BREF was developed as a shortened version of the WHOQOL-100 for use in situations in which time is restricted, respondent burden must be minimized, and when facet-level detail is unnecessary [31]. The WHOQOL-BREF is a cross-cultural, self-report scale that contains 24 items divided into four domains: physical health (seven items), psychological (six items), social relations (three items) and environmental (eight items). All items are rated on a 5-point scale with a higher score indicating a better quality of life [22]. Domain scores for the WHOQOL-BREF were calculated as usual by multiplying the mean of all items included within the domain by a factor of four [22]. Potential scores for each domain, therefore, range from 4 to 20. The WHOQOL-BREF has good internal consistency, test–retest reliability, discriminate validity, criterion validity and concurrent validity [22, 31].
Socio-demographic background characteristics
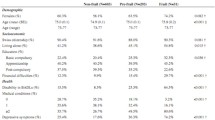
The socio-demographic background characteristics considered were age (in years), sex, marital status (four categories), ethnicity (Dutch versus other), highest education attained (three categories) and net household income (seven categories). Table 1 presents a detailed description of the answering categories.
Chronic diseases
Chronic diseases often negatively affect quality of life of older people [32–34]. Following Puts et al. [35], seven self-reported chronic diseases, most frequent in the older Dutch population, were examined: diabetes mellitus, chronic obstructive pulmonary disease, cardiac disease, cerebrovascular accidents, peripheral arterial disease, cancer and rheumatoid arthritis or osteoarthritis. A previous study among community-dwelling older persons found that respondents’ self-reports on chronic diseases compared with general practitioners’ information were fairly accurate for most diseases studied [36]. The total number of self-reported chronic diseases was used for analysis.
Analysis strategies
Before analyses were carried out, some variables were re-coded. As in a previous study [11], dummies were created for marital status (“1” married or cohabiting and “0” rest), and sex (“1” woman, “0” man) and linear effects of age, education, income and diseases were incorporated into the analyses. The variable ethnicity was excluded from further analyses because of the low incidence of non-Dutch respondents (3.4 %). After creating total scores for the quality of life domains, both Cronbach’s alpha and test–retest reliabilities were calculated for these scales.
Correlations of the fifteen frailty components with each of the four quality of life domains were tested as a first step to assess the predictive validity of the individual frailty components. Following Cohen, correlations were evaluated as small (.1), medium (.3) or large (.5) [37]. Subsequently, sequential linear regression analyses were run to verify which frailty components of the TFI improved the prediction of each quality of life domain, after controlling for the effects of the socio-demographic background characteristics, chronic diseases and the remaining frailty components. We checked for multicollinearity using the VIF and concluded there were no multicollinearity problems. The sequential linear regression analyses consisted of three blocks of variables assessed at baseline. The effect of socio-demographic background characteristics was estimated in the first block. The second block contained the number of chronic diseases, and in the third block, the fifteen individual frailty components of the TFI were added to the model. We tested whether each block increased the prediction of each quality of life domain at baseline and two and 4 years later, using the F test of change in R 2. Effect size was evaluated using Cohen’s f 2, with values .02, .15 and .35, representing small, medium and large effects, respectively [37]. Effects of individual predictors were also tested using the regression coefficients of the final model including all three blocks. Given the actual sample size of 192 in 2012, the statistical power of testing one regression coefficient in the final model is .8 if f 2 = .04, whereas power equals 1.00 for a medium effect size [38].
All statistical analyses were performed using SPSS version 18.0 (SPSS, IBM Corp., Somers, NY, USA). All reported p values are two-tailed.
Results
Scale and participant characteristics
The data of ten participants were excluded from the analyses as they had too many omissions. With the exception of the Cronbach’s alpha for the social relations scale, all values were well above .7 on all three occasions; alpha for the social relations scale varied from .59 to .64. Same-scale correlations over time were also at least .7 (except for social relations) for both the 2-year and 4-year interval. All quality of life domain scores were strongly correlated, with correlations varying from .41 to .73 at baseline, .52–.77 in 2010 and .47–.78 in 2012, with the strongest correlations between the physical health and psychological scales.
Table 1 shows the descriptive statistics of the 474 participants. Participants’ mean age at baseline was 80.2 years (SD = 3.8) and 56.8 % were women; 37.8 % of the participants were widowed. Analyses of dropouts showed significantly different scoring (p < .05) on many variables from participants who did not drop out. More particularly, those who dropped out in 2010 were older and scored worse on physical and psychological quality of life, and the frailty components unexplained weight loss, difficulty in walking, difficulty in maintaining balance, physical tiredness and feeling nervous or anxious, than those who did not drop out.
Correlations between frailty components and quality of life domains
Table 2 shows the correlations between fifteen components of frailty and the four quality of life domains and their significance. Nine components (five physical, three psychological and one social) predicted each quality of life domain on most, if not all, occasions. Six components, i.e., three physical (unexplained weight loss, poor hearing and poor vision), one psychological (problems with memory) and two social (living alone and lack of social relations) components have zero or small (<.3) correlations with the corresponding or other quality of life domain.
Five physical frailty components (physical unhealthy, difficulty in walking, difficulty in maintaining balance, lack of strength in the hands and physical tiredness) correlated on average strongly (about .5) with the corresponding quality of life physical health domain on all occasions. Three psychological frailty components (feeling down, feeling nervous or anxious and unable to cope with problems) on average correlated medium to strong (on average .37) with their corresponding quality of life domain, but these correlations became weaker over time. The five physical and three psychological components correlated about strongly with the psychological quality of life domain, and these three psychological components correlated about equally with the physical and psychological quality of life domains. Of the social frailty components, only lack of social support had generally weak correlations, but only with the social and environmental quality of life domains. The environmental domain generally correlated strongest (about .3) with the aforementioned five physical components, but also correlated (up to .3) with the three psychological and the lack of social support component.
Regression analyses
Table 3 presents the results of the sequential regression analyses on the four quality of life domains. Total explained variances were highest for 2008 (except for social relations with highest total explained variance (32 %) for 2010) and lowest for 2012, but explained variances did not decrease much, from 64 to 55 % for physical health, 55–44 % for psychological, 30–25 % for social and 43–34 % for environmental quality of life.
Turning to the effects of blocks of variables, the five background characteristics together explained physical health, psychological (except for 2012) and environmental quality of life, but never more than 10 % of the variance. They did not explain social relations quality of life. The number of chronic diseases increased the explained variances of all quality of life domains on all occasions, with small to medium increases for social (f 2 from .038 to .071; f 2 values not shown in Table 3), environmental (.065–.12), and psychological (.12–.16), and large increase for physical (.25–.39). Subsequently adding the frailty components resulted in the largest increase in explained variance of all domains on all occasions, with medium to large increases for social (f 2 from .19 to .34), and large increases for physical (.62–.97), psychological (.52–.89) and environmental (.28–.49).
We interpret the effect of one predictor on a quality of life domain, only if its effect is significant on at least two occasions. In this way, we check for the problem of testing multiple hypotheses [39]. Women had higher social and environmental quality of life than men up to 4 years later. Higher education predicted better future physical health, psychological and environmental quality of life. Higher income predicted lower psychological and social quality of life. Age and marital status did not predict future quality of life after controlling for the effects of all other predictors, whereas the number of chronic diseases only predicted physical health quality of life up to 2 years later.
Physical frailty components difficulty in walking and physical tiredness had a negative effect on both physical health and psychological quality of life. Difficulty in maintaining balance had a negative effect on physical health, whereas physical unhealthy had a negative effect on environmental quality of life. Unexplained weight loss, lack of strength in the hands, poor hearing and poor vision had no consistent effect on quality of life. Finally, none of the physical components had an effect on social quality of life. Of the four psychological frailty components, only feeling down had a consistent significant negative effect on psychological quality of life. The three other psychological components also had negative effects on the quality of life domains, but these effects were not consistently significant. Of the social frailty components, lack of social support consistently predicted lower psychological, social and environmental quality of life, but not physical health quality of life. Living alone and lack of social relations had no consistent negative effect on quality of life.
Discussion
The generally high correlations across time indicate that inter-individual differences in quality of life of older persons are fairly stable over time. The finding that quality of life domains were strongly correlated suggests there is one underlying quality of life higher-order dimension in older persons, although the multidimensionality of quality of life is widely accepted [21–23]. The best predictor of quality of life domains was the block of frailty components, underlining the importance of considering frailty and its components when attempting to predict future quality of life. The frailty components’ importance is further supported by their prediction of quality of life on all four domains 4 years later.
Although the effect of frailty components as a whole was large, the effect of individual predictors after controlling for the effects of all other predictors was small. This is characteristic of results of regression analysis when predictors are moderately to highly correlated, since regression analysis tests the unique contribution of each predictor and not the effect shared by the predictor. This should be kept in mind when interpreting the results of our analysis.
Of the background characteristics being female, higher education and lower income were associated with higher scores on at least two of four quality of life domains. Our finding that being a woman is associated with higher quality of life is supported by Lee et al. [40] and Gobbens et al. [25]. Other studies also observed a positive association between higher education and quality of life [41, 42], whereas other studies found no such association [43, 44]. Our finding that lower income is associated with higher quality of life is striking and differs from that of our previous Dutch cross-sectional study [25] and a study in Canada and Brazil [23]. No consensus currently exists on effects of these socio-demographic characteristics on quality of life [40]. More knowledge about the effects of these characteristics on older people’s quality of life is needed as population aging becomes a reality worldwide.
In our study, the number of chronic diseases only improved the prediction of quality of life physical health in 2008 and 2010, after controlling for the other variables. Chronic diseases are acknowledged to affect especially the physical domain of quality of life of older persons negatively [45–47].
The regression analyses showed that particularly four physical, one psychological and one social frailty component predicted future quality of life. The physical frailty components were physical unhealthy, difficulty in maintaining balance, difficulty in walking and physical tiredness. The last two correspond roughly to criteria of the phenotype of frailty (slowness and poor endurance), a frequently cited operational definition of frailty, developed by Fried et al. [2]. Two cross-sectional studies employing this phenotype observed the strongest negative effect on quality of life of poor endurance and slowness [18, 48]. In our longitudinal study, difficulty in walking was the most powerful predictor of quality of life, especially in the physical domain. This finding contrasts with a recent cross-sectional Dutch study that found mainly an effect of physical tiredness on quality of life [25]; possibly the difference can be explained by the difference in mean age of the participants, 80.2 years (SD = 3.8) (at baseline) and 73.4 years (SD = 5.8) [25]. It is important to consider difficulty in walking for assessment of quality of life of older people. In addition, slowness is also a predictor for the onset of functional dependence [49, 50], cognitive impairment [49], institutionalization [49, 51] and mortality [49, 52].
The effect of psychological frailty component feeling down is corroborated by our cross-sectional study [25] and other studies. For example, Baernholdt et al. [53] found that more depression was associated with poorer health-related quality of life, social functioning and emotional well-being, and Bilotta et al. [19] demonstrated that depression negatively affected quality of life independently of physical frailty status. Another study points to the need for an effective treatment of depression in older people living alone in order to improve their quality of life [54].
Only one social frailty component, lack of social support, predicted future quality of life domains, namely social, environmental and also psychological. Other studies also demonstrate the significant contribution of social support to the prediction of quality of life [55, 56] and as a buffer to stress [55]. A qualitative study by Puts et al. [57] on the meaning of quality of life for older persons in the Netherlands concluded that when participants’ health was poor, there was a shift from health to social contacts as the most important aspect to quality of life. Moreover, a recent longitudinal study showed that social frailty, consisting of living alone, lack of social contacts and lack of social support, was associated with receiving nursing-care and the number of contacts with health care professionals [26]. All these findings underline the importance of distinguishing and assessing social frailty when predicting quality of life and other adverse outcomes. However, our findings suggest that the social dimension of frailty and the social quality of life domain need further examination. The number of components related to the social frailty dimension is lower than the number of components related to physical and psychological dimensions. This probably resulted in both a low reliability of the social quality of life scale and the lowest additional explained variance by the social frailty components.
Our study includes several strengths. To our knowledge, this study is the first to predict quality of life of older persons 2 and 4 years after a multidimensional assessment of frailty, consisting of physical, psychological and social components. In addition, we used two validated questionnaires, the TFI for measuring frailty [12, 26] and the WHOQOL-BREF for measuring quality of life [22, 31].
A limitation of our study were the response rates (42 % at baseline, 54 % in 2010, 40 % in 2012), which were lower than in another study in the Netherlands that used the TFI for measuring frailty (77 %) [58]. The response rate in the latter study was probably higher because older people were asked to participate by a general practitioner; participants’ mean age was lower (77.2 vs. 80.2) too. Our analysis of dropouts revealed that age and the related lower scores on physical and psychological quality of life and health-related variables were indeed related to dropout. This does not imply, however, that the associations between quality of life domains and the other variables will be different for participants and those who dropped out. A second limitation is the low Cronbach’s alpha (.59–.64) for the quality of life domain social relations, which is probably related to the limited numbers of items (three) of this domain. Third, it is important to consider the effects of potential overlap between the wording of some frailty components and quality of life items. We identified three TFI components that show clear overlap with two WHOQOL-BREF items. One TFI component on social support clearly relates to one item on social support of the quality of life domain social relations and two TFI components (feeling down, feeling nervous or anxious) clearly relates to the same item of the quality of life domain psychological. But these three frailty components were not only associated with the related quality of life domains, but also to at least one other quality of life domain.
Health and social care professionals have a major task in detecting frail older persons at an early stage in order to avoid unnecessary loss of quality of life and to make timely preventive or curative interventions possible. Developing and implementing interventions is an essential next step in increasing quality of life of frail older persons. A recent study showed that Hartslag Limburg, a community-based cardiovascular diseases prevention program in the Netherlands, had no beneficial effect on people’s physical and mental quality of life after 5 years of intervention [59]. There is a great need to further examine the use of physical, psychological, social and environmental interventions to improve quality of life of community-dwelling older people.
In conclusion, this longitudinal study showed that quality of life domains physical health, psychological, social relations and environmental are predicted by different components of frailty. This finding emphasizes the relevance of a multidimensional assessment of frailty. Based on our findings, to improve quality of life of older persons, special attention should go to the screening and subsequent interventions focusing on the frailty components difficulty in walking, feeling down and lack of social support.
References
Abellan Van Kan, G., Rolland, Y., Bergman, H., et al. (2008). The I.A.N.A Task Force on frailty assessment of older people in clinical practice. The Journal of Nutrition, Health & Aging, 12 (1), 29–37.
Fried, L. P., Tangen, C. M., Walston, J., et al. (2001). Frailty in older adults: Evidence for a phenotype. Journal of Gerontology: Medical Sciences, 56(3), M146–M156.
Markle-Reid, M., & Browne, G. (2003). Conceptualizations of frailty in relation to older adults. Journal of Advanced Nursing, 44(1), 58–68.
Gobbens, R. J., Luijkx, K. G., Wijnen-Sponselee, M. T., & Schols, J. M. (2010). In search of an integral conceptual definition of frailty: Opinions of experts. Journal of the American Medical Directors Association, 11(5), 338–343.
Hogan, D. B., MacKnight, C., & Bergman, H. (2003). Models, definitions, and criteria of frailty. Aging Clinical and Experimental Research, 15(3 Suppl), 1–29.
Levers, M. J., Estabrooks, C. A., & Ross Kerr, J. C. (2006). Factors contributing to frailty: Literature review. Journal of Advanced Nursing, 56(3), 282–291.
De Witte, N., Gobbens, R., de Donder, L., et al. (2013). The comprehensive frailty assessment instrument: Development, validity and reliability. Geriatric Nursing, 34(4), 274–281.
Gobbens, R. J., Luijkx, K. G., Wijnen-Sponselee, M. T., & Schols, J. M. (2007). Frail elderly. Identification of a population at risk. Tijdschrift Gerontologie en Geriatrie, 38(2), 65–76.
Gobbens, R. J., Luijkx, K. G., Wijnen-Sponselee, M. T., & Schols, J. M. (2010). Toward a conceptual definition of frail community dwelling older people. Nursing Outlook, 58(2), 76–86.
Gobbens, R. J., Luijkx, K. G., Wijnen-Sponselee, M. T., & Schols, J. M. (2010). Towards an integral conceptual model of frailty. The Journal of Nutrition, Health & Aging, 14(3), 175–181.
Gobbens, R. J., van Assen, M. A., Luijkx, K. G., & Schols, J. M. (2012). Testing an integral conceptual model of frailty. Journal of Advanced Nursing, 68(9), 2047–2060.
Gobbens, R. J., van Assen, M. A., Luijkx, K. G., Wijnen-Sponselee, M. T., & Schols, J. M. (2010). The Tilburg Frailty Indicator: Psychometric properties. Journal of the American Medical Directors Association, 11(5), 344–355.
Van Campen, C. (2011). Frail older persons in the Netherlands. The Hague: The Netherlands Institute for Social Research.
Boyd, C. M., Xue, Q. L., Simpson, C. F., Guralnik, J. M., & Fried, L. P. (2005). Frailty, hospitalization, and progression of disability in a cohort of disabled older women. The American Journal of Medicine, 118(11), 1225–1231.
Puts, M. T., Lips, P., & Deeg, D. J. (2005). Static and dynamic measures of frailty predicted decline in performance-based and self-reported physical functioning. Journal of Clinical Epidemiology, 58(11), 1188–1198.
Rockwood, K., Song, X., MacKnight, C., et al. (2005). A global clinical measure of fitness and frailty in elderly people. Canadian Medical Association Journal, 173(5), 489–495.
Jones, D. M., Song, X., & Rockwood, K. (2004). Operationalizing a frailty index from a standardized comprehensive geriatric assessment. Journal of the American Geriatrics Society, 52(11), 1929–1933.
Lin, C. C., Li, C. I., Chang, C. K., et al. (2011). Reduced health-related quality of life in elders with frailty: A cross-sectional study of community-dwelling elders in Taiwan. PLoS ONE,. doi:10.1371/journal.pone.0021841.
Bilotta, C., Bowling, A., Case, A., et al. (2010). Dimensions and correlates of quality of life according to frailty status: A cross-sectional study on community-dwelling older adults referred to an outpatient geriatric service in Italy. Health and Quality of Life Outcomes,. doi:10.1186/1477-7525-8-56.
Masel, M. C., Ostir, G. V., & Ottenbacher, K. J. (2010). Frailty, mortality, and health-related quality of life in older Mexican Americans. Journal of the American Geriatrics Society, 58(11), 2149–2153.
WHOQOL group. (1995). World Health Organization Quality of Life assessment (WHOQOL): Position paper from the World Health Organization. Social Science and Medicine, 41(10), 1403–1409.
WHOQOL Group. (1998). Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychological Medicine, 28(3), 551–558.
Paskulin, L. M., & Molzahn, A. (2007). Quality of life of older adults in Canada and Brazil. Western Journal of Nursing Research, 29(1), 10–26. discussion 7–35.
Bilotta, C., Bowling, A., Nicolini, P., et al. (2011). Older People’s Quality of Life (OPQOL) scores and adverse health outcomes at a one-year follow-up. A prospective cohort study on older outpatients living in the community in Italy. Health and Quality of Life Outcomes. doi:10.1186/1477-7525-9-72.
Gobbens, R. J., Luijkx, K. G., & van Assen, M. A. (2013). Explaining quality of life of older people in the Netherlands using a multidimensional assessment of frailty. Quality of Life Research, 22(8), 2051–2061.
Gobbens, R. J., van Assen, M. A., Luijkx, K. G., & Schols, J. M. (2012). The predictive validity of the Tilburg frailty indicator: Disability, health care utilization, and quality of life in a population at risk. The Gerontologist, 52(5), 619–631.
Gobbens, R. J., van Assen, M. A., Luijkx, K. G., Wijnen-Sponselee, M. T., & Schols, J. M. (2010). Determinants of frailty. Journal of the American Medical Directors Association, 11(5), 356–364.
Central Committee on Research inv. Human Subjects. (2010). Does your study have to be reviewed? http://www.ccmo-online.nl (Home>For investigators>Review step plan RC>WMO) Accessed 15 June 2010.
Santiago, L. M., Luz, L. L., Mattos, I. E., Gobbens, R. J., & van Assen, M. A. (2013). Psychometric properties of the Brazilian version of the Tilburg frailty indicator (TFI). Archives of Gerontology and Geriatrics, 57(1), 39–45.
Huisman, M., & Deeg, D. (2011). The course of frailty. In Van Campen C (Ed.), Frail older persons in the Netherlands (pp. 83–90). The Hague: The Netherlands Institute for Social Research.
Skevington, S. M., Lotfy, M., & O’Connell, K. A. (2004). The World Health Organization’s WHOQOL-BREF quality of life assessment: Psychometric properties and results of the international field trial. A report from the WHOQOL group. Quality of Life Research, 13(2), 299–310.
Heo, S., Moser, D. K., Lennie, T. A., Zambroski, C. H., & Chung, M. L. (2007). A comparison of health-related quality of life between older adults with heart failure and healthy older adults. Heart and Lung, 36(1), 16–24.
Hlatky, M. A., Chung, S. C., Escobedo, J., et al. (2010). The effect of obesity on quality of life in patients with diabetes and coronary artery disease. American Heart Journal, 159(2), 292–300.
DiBonaventura, M., Paulose-Ram, R., Su, J., et al. (2012). The impact of COPD on quality of life, productivity loss, and resource use among the elderly United States workforce. Journal of Chronic Obstructive Pulmonary Disease, 9(1), 46–57.
Puts, M. T., Lips, P., & Deeg, D. J. (2005). Sex differences in the risk of frailty for mortality independent of disability and chronic diseases. Journal of the American Geriatrics Society, 53(1), 40–47.
Kriegsman, D. M., Penninx, B. W., van Eijk, J. T., Boeke, A. J., & Deeg, D. J. (1996). Self- reports and general practitioner information on the presence of chronic diseases in community dwelling elderly. A study on the accuracy of patients’ self-reports and on determinants of inaccuracy. Journal of Clinical Epidemiology, 49(12), 1407–1417.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.). Hillsdale: Lawrence Erlbaum Assoc Inc.
Faul, F., Erdfelder, E., Lang, A.-G., & Buchner, A. (2007). G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavioral Research Methods, 39(2), 175–191.
Maxwell, S. E., & Delaney, H. D. (2004). Designing experiments and analyzing data: a model comparison perspective (2nd ed.). Hillsdale: Lawrence Erlbaum Assoc Inc.
Lee, T. W., Ko, I. S., & Lee, K. J. (2006). Health promotion behaviors and quality of life among community-dwelling elderly in Korea: A cross-sectional survey. International Journal of Nursing Studies, 43(3), 293–300.
Paskulin, L., Vianna, L., & Molzahn, A. E. (2009). Factors associated with quality of life of Brazilian older adults. International Nursing Review, 56(1), 109–115.
Lubetkin, E. I., Jia, H., Franks, P., & Gold, M. R. (2005). Relationship among sociodemographic factors, clinical conditions, and health-related quality of life: Examining the EQ-5D in the U.S. general population. Quality of Life Research, 14(10), 2187–2196.
Hilleras, P. K., Jorm, A. F., Herlitz, A., & Winblad, B. (2001). Life satisfaction among the very old: A survey on a cognitively intact sample aged 90 years or above. International Journal of Aging and Human Development, 52(1), 71–90.
Raphael, D., Brown, I., Renwick, R., et al. (1997). Measuring the quality of life of older persons: A model with implications for community and public health nursing. International Journal of Nursing Studies, 34(3), 231–239.
Rijken, M., van Kerkhof, M., Dekker, J., & Schellevis, F. G. (2005). Comorbidity of chronic diseases: Effects of disease pairs on physical and mental functioning. Quality of Life Research, 14(1), 45–55.
Fortin, M., Bravo, G., Hudon, C., et al. (2006). Relationship between multimorbidity and health-related quality of life of patients in primary care. Quality of Life Research, 15(1), 83–91.
Hopman, W. M., Harrison, M. B., Coo, H., et al. (2009). Associations between chronic disease, age and physical and mental health status. Chronic Diseases in Canada, 29(3), 108–116.
Chang, Y. W., Chen, W. L., Lin, F. G., et al. (2012). Frailty and its impact on health-related quality of life: A cross-sectional study on elder community-dwelling preventive health service users. PLoS ONE,. doi:10.1371/journal.pone.0038079.
Abellan van Kan, G., Rolland, Y., Andrieu, S., et al. (2009). Gait speed at usual pace as a predictor of adverse outcomes in community-dwelling older people an International Academy on Nutrition and Aging (IANA) Task Force. The Journal of Nutrition, Health & Aging, 13(10), 881–889.
Shinkai, S., Watanabe, S., Kumagai, S., et al. (2000). Walking speed as a good predictor for the onset of functional dependence in a Japanese rural community population. Age and Ageing, 29(5), 441–446.
Woo, J., Ho, S. C., & Yu, A. L. (1999). Walking speed and stride length predicts 36 months dependency, mortality, and institutionalization in Chinese aged 70 and older. Journal of the American Geriatrics Society, 47(10), 1257–1260.
Rolland, Y., Lauwers-Cances, V., Cesari, M., et al. (2006). Physical performance measures as predictors of mortality in a cohort of community-dwelling older French women. European Journal of Epidemiology, 21(2), 113–122.
Baernholdt, M., Hinton, I., Yan, G., Rose, K., & Mattos, M. (2012). Factors associated with quality of life in older adults in the United States. Quality of Life Research, 21(3), 527–534.
Bilotta, C., Bowling, A., Nicolini, P., Case, A., & Vergani, C. (2012). Quality of life in older outpatients living alone in the community in Italy. Health and Social Care in the Community, 20(1), 32–41.
Bowling, A., Seetai, S., Morris, R., & Ebrahim, S. (2007). Quality of life among older people with poor functioning. The influence of perceived control over life. Age and Ageing, 36(3), 310–315.
Gabriel, Z., & Bowling, A. (2004). Quality of life from the perspectives of older people. Ageing & Society, 24(5), 675–691.
Puts, M. T., Shekary, N., Widdershoven, G., et al. (2007). What does quality of life mean to older frail and non-frail community-dwelling adults in the Netherlands? Quality of Life Research, 16(2), 263–277.
Metzelthin, S. F., Daniels, R., van Rossum, E., et al. (2010). The psychometric properties of three self-report screening instruments for identifying frail older people in the community. BMC Public Health,. doi:10.1186/1471-2458-10-176.
Verkleij, S. P., Adriaanse, M. C., Verschuren, W. M., et al. (2011). Five-year effect of community-based intervention Hartslag Limburg on quality of life: A longitudinal cohort study. Health and Quality of Life Outcomes,. doi:10.1186/1477-7525-9-11.
Conflict of interest
None declared.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gobbens, R.J.J., van Assen, M.A.L.M. The prediction of quality of life by physical, psychological and social components of frailty in community-dwelling older people. Qual Life Res 23, 2289–2300 (2014). https://doi.org/10.1007/s11136-014-0672-1
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-014-0672-1