
Abstract
This study sought to compare Bupropion versus Sertraline in the treatment of depressed patients with Binge Eating Disorder (BED) prescribed off-label. Medical records of outpatients with diagnosis of BED and Depression (DSM-IV-TR criteria) were selected: 15 patients were treated with bupropion 150 mg/per day, and 15 with sertraline 200 mg/per day. During the screening and control visits (2°–6°–14°–24° week), the selected patients were first weighed and then evaluated using the following questionnaires: Binge Eating Disorder-Clinical Interview (BEDCI), Beck Depression Inventory (BDI), State-Trait Anxiety Inventory X (STAI-X) and Arizona Sexual Experience Scale (ASEX). Both drugs reduced anxious-depressive symptoms and binge frequency: Bupropion showed a better effectiveness in reducing weight and improving sexual performances; weight loss related to it was proportional to the body mass index. Bupropion may be associated with more weight loss in BED, depressed patients than sertraline.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Binge Eating Disorder (BED) is characterized by binge eating episodes without inappropriate compensatory behaviours [1]. BED is really uncommon in men [2, 3]. It is usually associated with obesity in nearly 65% of patients [4], representing a chronic severe disorder [5].
Even though BED frequency is growing, up-dated guidelines for its treatment are not available [6]. In clinical practice antidepressants, in particular SSRIs, are often used [7, 8]. Among SSRIs, fluoxetine and fluvoxamine are the most extensively used; however, at the moment evidence about their effectiveness is controversial [9–11]. From a general point of view, antidepressants are effective in solving BED psychopathology, but they don’t promote long term weight loss [12]. The weight gain, as an adverse effect of these drugs, limits compliance. Among the second generation antidepressants without weight gain effect, sertraline showed effectiveness in reducing binge frequency and weight [13, 14]. Also citalopram [15] and escitalopram [16] showed effectiveness in the treatment of BED. Moreover, also bupropion showed effectiveness in reducing depressive symptoms but it also showed more tolerability and effectiveness in reducing weight. Several studies have demonstrated that bupropion is useful in the treatment of hyperphagic depressive patients, overweight subjects or those risking a weight gain [17–21].
The aim of this retrospective cohort study is to compare the effectiveness of sertraline and bupropion over a period of 24 weeks in overweight/obese patients with BED. We focused our attention on the capability of these drugs to reduce weight, binge frequency and depressive symptoms.
Methods
This is a retrospective study carried out on adult patients with BED and depressive symptoms, receiving treatment from April 2009 to September 2010. The diagnosis of BED was formulated according to research criteria of the Appendix in The American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) [22]. All the patients were overweight or obese and presented a score of ≥17 at the Beck Depression Inventory (BDI) [23, 24]. None of the patients involved in the study had a history of vomiting.
Subjects with other eating or convulsive disorders, with severe liver and renal failure, or other significant systemic pathologies, or treated with reducing convulsive threshold drugs, or with other antidepressants were excluded from the study.
A written informed consent was obtained from all the patients. The study was approved by the local Ethical Committee.
Patients were evaluated during a screening check (T0) and four control visits (T1 after 2 weeks, T2 after 6 weeks, T3 after 14 weeks and T4 after 24 weeks).
During the screening visit, the patients were weighed, their height measured following standard procedures and assessed by an expert interviewer using the Structured Clinical Interview for DSM-IV Axis I Disorders (SCID-I) [25] and the Structured Clinical Interview for DSM-IV Axis II Personality Disorders (SCID-II) [26]. During the following visits, the patients were weighed again and administered the BEDCI, BDI, STAI-X and ASEX. Patients with Axis I (except Depression) and Axis II comorbidity were excluded from the study. Weight was measured using a biomedical electronic balance scale (SECA, Birmingham, UK) with a precision of 0.1 kg: patients wore light clothes for all the visits, and they were barefoot. Height was measured using a stadiometro with a precision of 0.1 cm. Body Mass Index (BMI) was calculated through the following formula: Weight/Height2 (kg/m2) [27].
All the subjects answered the following questionnaires:
-
The Binge Eating Disorder-Clinical Interview (BEDCI) consists of 47 items: apart from the diagnostic items (the presence and frequency of binge eating, and the absence of regular purging behaviours for an exclusionary diagnosis of bulimia nervosa), the other items provide additional historical information (e.g. demographics; degree to which self-esteem is dependent on weight and shape; brief psychiatric history, etc.). This interview presents a good internal consistency and test–retest reliability. Prediction is about 70% [28].
-
The BDI [23, 24]: a 21 question multiple-choice self-report inventory composed of items relating to depressive as well as physical symptoms, such as fatigue and lack of interest in sex. It is used world-wide for depression assessment, and presents a high internal consistency and a high content validity, besides an international propagation [29].
-
The State-Trait Anxiety Inventory-X (STAI-X) [30]: it consists of 20 items that measure state anxiety in adults and its validity and utility has been demonstrated in clinical populations. The concepts of state and trait anxiety find support from these findings [31].
-
The Arizona Sexual Experience Scale (ASEX): a user-friendly five-item rating scale that quantifies sexual functioning, useful to identify sexual dysfunctions among BED patients, and to investigate the negative effect of drugs. In addition, it presents a good reliability and validity [32].
Fifteen patients were treated with bupropion and 15 patients with sertraline. In previous studies both drugs had been demonstrated to be moderately more effective than placebo in reducing weight in BED patients [13, 18]. Bupropion was administered in a single dose of 150 mg/day; sertraline in a dose of 200 mg/day (two tablets of 100 mg/day).
After starting the therapy, during all the control visits, the patients were weighted and administered the previously described questionnaires.
Data Analysis
All data analyses were generated using the Statistical Package for Social Sciences (SPSS, 2000). The researcher, who analysed the data, was not informed about the kind of treatment the patients were receiving. We have described the sample group and two treatment groups with descriptive statistics.
A t test for independent samples was used to determine the validity of randomization. The association among categorical descriptive variables was tested through paired-samples t test used in order to investigate the association between body weight, binge frequency and a reduction in BDI scores during the study period in the same treatment group. A final independent sample t test was used to compare the two groups. The association among depressive symptoms, binges and weight was investigated by using the Pearson test. Only values of P < 0.05, P < 0.01 and P < 0.001 were considered statistically significant.
Results
Thirty patients (22 F and 8 M) were selected. All the subjects were treated for at least 24 weeks.
In Table 1 sample characteristics are shown.
Before starting the treatment, the bupropion group presented a T0 weight of 92.6 ± 18.89 kg and a BMI of 33.4 ± 6.1 kg/m2. The Sertraline group presented a T0 weigh of 91.20 ± 10.1 kg and a BMI of 32.9 ± 3.1 kg/m2.
The score at the BDI was 31.4 ± 12 in the bupropion group, and 32.5 ± 10.55 in the sertraline group (severe depression).
In Tables 2 and 3, clinical results at the end of the 24 weeks of treatment are shown.
Weight Variations
After 24 weeks of treatment, the weight reduction was of 5.5 ± 3.68 kg (6% of the T0 weight) in the bupropion group and of 1.9 ± 1.25 kg (2% of the T0 weight) in the sertraline group. A significant difference between T0 weight and the weight at the following visits in the bupropion group was noticed (T1: 1.2 ± 1.02; t = 4.6, P < 0.001); (T2: 2.2 ± 1.92 t = 4.52, P < 0.001); (T3: 3.8 ± 2.74, t = 5.41, P < 0.001); (T4: 5.5 ± 3.68; t = 5.75, P < 0.001) and in the sertraline group (T1: 1.1 ± 0.59; t = 7.38, P < 0.001); (T2: 2.4 ± 1.17; t = 7.90, P < 0.001); (T3: 2.0 ± 1.45; t = 5.32, P < 0.001); (T4: 1.9 ± 1.25; t = 5.73, P < 0.001). During the first 6 weeks of treatment, no difference was noticed between the two groups regarding weight reduction; however, at the 14° and 24° week of treatment, there was a higher weight reduction in the bupropion group (respectively P < 0.05 and P < 0.001). 60% of the subjects (nine on 15) receiving bupropion lost >5% of their weight at T0. The highest reduction was of 16 kg. Nobody in the sertraline group lost such a percentage, and the highest reduction was of 5 kg.
In the bupropion group, the patients with a higher BMI presented a higher weight loss.
Binge Frequency
At the end of the 24 weeks, compared to T0, patients receiving bupropion had a reduction of weekly binges of 75% (P < 0.001),while those in the sertraline group had a reduction of 72% (P < 0.001). No differences between the two groups were noticed in the reduction of weekly binge frequency (P > 0.5).
At T4, 53% (eight on 15) of the subjects treated with bupropion showed a complete remission of binges versus 33% (five on 15) of the sertraline group.
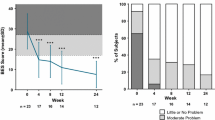
Beck Depression Inventory Score
At the end of the analysed period, the score at the BDI was 16.6 ± 10.55 in the bupropion group, and 16.9 ± 8.03 in the sertraline one with a significant improvement in depression features (P < 0.001) in both groups. 46.7% of the bupropion group had a reduction on the total BDI score >50% versus 73.3% of the sertraline one.
No significant differences on the reduction of depressive features between the two groups were found (P > 0.5).
Anxious Symptoms
After 6 months of treatment, the STAI-X score was 50.4 ± 12.31 for the bupropion group (P < 0.005) and 50.5 ± 8.84 for the sertraline one (P < 0.001). Even though bupropion presented a minor effect on anxiety than sertraline, no significant differences were found between the two groups in anxious symptoms reduction.
Sexual Dysfunction
At the end of the study period, while the bupropion group presented a slight improvement of sexual performances (ASEX score declined below baseline values of 1.47; P < 0.01), the sertraline group’s performance was worse (ASEX score increased above baseline values of 1.73; P < 0.01).
Correlation Between Depressive Symptoms, Binge and Weight
No statistically correlation were found between depressive symptoms (BDI) and weight (BMI) or between depressive symptoms and binge frequency.
Side Effects
Some patients presented side effects but none of the patients had severe ones (see Table 4).
To our knowledge, this is the first study that compares bupropion versus sertraline in the treatment of BED.
Discussion
In our retrospective study, bupropion and sertraline showed a significant score reduction at the BDI, confirming their effectiveness, as antidepressant, noticed in previous studies [33–36]. Both drugs are useful in weight reduction but bupropion showed a major activity in long-term studies. The subjects treated with bupropion, in fact, continued to lost weight during the study period, while the subjects of the sertraline group showed only an initial weight loss. The BMI influenced the weight loss only in the bupropion group: the patients, who presented the highest BMI at the beginning of the study, showed a major reduction of their weight at the end. This is an advantage in those cases where a weight reduction is not a positive result (e.g. in depressive people with a normal or low BMI). At the end of the 24 analysed weeks, 60% of the subjects of the bupropion group, versus none of those in the sertraline one, lost at least 5% of their body weight. How bupropion causes a weight reduction is unknown. A recent study [37] noticed that the weight reduction in obese patients is probably due to an improvement of thermogenesis and of an energy expenditure. Considering BED patients, the weight loss could be due to a reduction in binge frequency. Our study has shown that bupropion and sertraline are both effective in reducing binge frequency. The presence of binge has been associated with a higher dissatisfaction with specific body areas, as well as a higher harm avoidance [38] than in non-BED obese women [39]. Patients with a binge behaviour often present affective instability, insecure attachment and impulsivity [40].
Some theories considered “binge” as a defense mechanism to better manage negative emotions [41]. As a consequence, bupropion and sertraline could cause a binge reduction (and a weight loss) through a reduction of depressive symptoms. Actually, we have not found any correlations between binge frequency and depressive symptoms, nor between binge frequency and weight. Probably, the bupropion and sertraline mechanism on weight reduction is different and independent from their effectiveness as antidepressants.
In addition, patients treated with sertraline reported sexual dysfunction; while patients treated with bupropion reported an improvement in their sexual performance. This result confirms a previous study on bupropion effectiveness in the treatment of sexual dysfunction [42].
In conclusion, bupropion and sertraline showed the same effectiveness in solving depressive symptoms, and the frequency of binge with a similar tolerability profile. Bupropion, contrary to sertraline, also presented the advantage of inducing a higher reduction in the baseline body weight, a lower daytime somnolence and an improvement in sexual performance. Hence, bupropion, is more useful than sertraline in the treatment of BED, depressed patients needing weight loss and a better sexual life. This study presents significant limitations: the retrospective nature of the study, the small sample size in both treatment groups and the exclusion of subjects with Axis I (except depression) and II comorbidity. Prospective studies are necessary to confirm these results in larger samples.
References
American Psychiatric Association: Practice guideline for the treatment of patients with eating disorders, third edition. American Journal of Psychiatry 163:4–54, 2006
Støving RK, Andries A, Brixen K, et al.: Gender differences in outcome of eating disorders: A retrospective cohort study. Psychiatry Research 186(2–3):362–366, 2010
Feldman MB, Meyer IH: Comorbidity and age of onset of eating disorders in gay men, lesbians, and bisexuals. Psychiatry Research 180:126–131, 2002
Striengel-Moore RH, Cachelin FM, Dohm FA, et al.: Comparison of binge eating disorder and bulimia nervosa in a community sample. International Journal of Eating Disorders 29:157–165, 2001
Pope HG Jr, Lalonde JK, Pindyck LJ, et al.: Binge eating disorder: A stable syndrome. American Journal of Psychiatry 163:2181–2183, 2006
Brownley KA, Berkman ND, Sedway JA, et al.: Binge Eating Disorder treatment: A systematic review of randomized controlled trials. International Journal of Eating Disorders 40:337–348, 2007
Carter WP, Hudson JI, Lalonde JK, et al.: Pharmacologic treatment of Binge Eating Disorder. International Journal of Eating Disorders 34:74–88, 2003
Hudson JI, Carter WP, Pope HG Jr: Antidepressant treatment of binge eating disorder: Research findings and clinical guidelines. Journal of Clinical Psychiatry 57:73–79, 1996
Arnold LM, McElroy SL, Hudson JI, et al.: A placebo-controlled, randomized trial of fluoxetine in the treatment of binge-eating disorder. Journal of Clinical Psychiatry 63:1028–1033, 2002
Pearlstein T, Spurell E, Hohlstein LA, et al.: A double-blind, placebo-controlled trial of fluvoxamine in binge eating disorder: A high placebo response. Archives of Women’s Mental Health 6:147–151, 2003
Ricca V, Manucci E, Mezzani B, et al.: Fluoxetine and fluvoxamine combined with individual cognitive-behaviour therapy in binge eating disorder: A one year follow up study. Psychotherapy and Psychosomatics 70:298–306, 2001
Hirschfeld RM: Long-term side effects of SSRIs: Sexual dysfunction and weight gain. Journal of Clinical Psychiatry 64:20–24, 2003
McElroy SL, Casuto LS, Nelson EB, et al.: Placebo-controlled trial of sertraline in the treatment of binge eating disorder. American Journal of Psychiatry 157:1004–1006, 2000
Leonbruni P, Pierò A, Brustolin A, et al.: A 12 to 24 weeks pilot study of sertraline treatment in obese women binge eaters. Human Psychopharmacology 21:181–188, 2006
McElroy SL, Hudson JI, Malhorta S, et al.: Citalopram in the treatment of binge eating disorder: A placebo controlled trial. Journal of Clinical Psychiatry 64:807–813, 2003
Guerdjikova AI, McElroy SL, Kotwal R, et al.: High dose escitalopram in the treatment of binge eating disorder with obesity: A placebo controlled monotherapy trial. Human Psychopharmacology 23:1–11, 2008
Gadde KM, Parker CB, Maner LG, et al.: Bupropion for weight loss: An investigation of efficacy and tolerability in overweight and obese women. Obesity Research 9:544–551,2001
Jain AK, Kaplan RA, Gadde KM, et al.: Bupropion SR vs placebo for weight loss in obese patients with depressive symptoms. Obesity Research 10:1049–1056, 2002
Anderson JW, Greenway FL, Fujioka K, et al.: Bupropion SR enhances weight loss: A 48-week double-blind, placebo-controlled trial. Obesity Research 10:633–641, 2002
Jefferson JW, Rush AJ, Nelson JC, et al.: Extended-release bupropion for patients with major depressive disorder presenting with symptoms of reduced energy, pleasure, and interest: Finding from a, randomized, double-blind placebo-controlled study. Journal of Clinical Psychiatry 67:865–873, 2006
Jamerson BD, Krishnana KR, Roberts J, et al.: Effect of bupropion SR on specific symptom clusters of depression: Analysis on the 31-item Hamilton Rating Scale for Depression. Psychopharmacology Bulletin 37:67–78, 2003
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders Text Revision (DSM-IV-TR), 4th edn. Washington, DC, American Psychiatric Association, 2002
Beck AT, Steer RA: Beck Depression Inventory, Manual. San Antonio, TX, The Psychological Corporation, 1993
Bocali C: Beck Depression Inventory. PsicoLab-Laboratorio di ricerca e sviluppo in Psicologia, 2006 (Italian)
First MB, Spitzer RI, Gibbon M, et al.: Structured Clinical Interview for DSM-IV Axis I Disorders-Outpatient Edition (SCID-O/P, version 2.0). New York, Biometric Research, New York State Psychiatric Institute, 1996
First MB, Gibbon M, Spitzer RI, et al.: Structured Clinical Interview for DSM-IV Axis II Personality Disorders (SCID-II). Washington, DC, American Psychiatric Press, 1997
Report of the World Health Organization Consultation of Obesity, Preventing and Managing the Global Epidemic of Obesity. Geneva, WHO, 1996
Spitzer RL, Yanovsky SZ, Marcus MD: Binge Eating Clinical Interview. Pittsburgh, HaPI Record, 1994
Richter P, Werner J, Heerlein A, et al.: On the validity of the Beck Depression Inventory. A review. Psychopathology 31:160–168, 1998
Spielberger CD: Manual for the State-Trait Anxiety Inventory, Revised Edition. Palo Alto, CA, Consulting Psychologists Press, 1983
Oei TP, Evans L, Crook GM: Utility and validity of the STAI with anxiety disorder patients. The British Journal of Clinical Psychology 29(Pt 4):429–432, 1990
McGahuey CA, Gelenberg AJ, Laukes CA, et al.: The Arizona Sexual Experience Scale (ASEX): Reliability and validity. Journal of Sex and Marital Therapy 26:25–40, 2000
Calandra C, Terranova F, Loiacono P, et al.: Bupropione nel trattamento del disturbo depressivo maggiore: confronto con paroxetina. Italian Journal of Psychopathology 16:128–133, 2010 (Italian)
Croft H, Houser TL, Jamerson BD, et al.: Effect on body weight of bupropion SR in patients with major depression treated for 52 weeks. Clinical Therapeutics 24:662–672, 2002
Fava M, Rush AJ, Thase ME, et al.: 15 years of clinical experience with bupropion HCl: From bupropion to bupropion-SR to bupropion-XL. The Primary Care Companion to the Journal of Clinical Psychiatry 7:106–113, 2005
Thase ME, Haight BR, Richard N, et al.: Remission rates following antidepressant therapy with bupropion or selective serotonin reuptake inhibitors: A meta-analysis of original data from 7 randomized controlled trials. Journal of Clinical Psychiatry 66:974–981, 2005
Billes SK, Cowley MA: Catecholamine reuptake inhibition causes weight loss by increasing locomotor activity and thermogenesis. Neuropsychopharmacology 33:1287–1297, 2008
Monteleone P, Santonastaso P, Mauri M, et al.: Investigation of the serotonin transporter regulatory region polymorphism in bulimia nervosa: Relationships to harm avoidance, nutritional parameters, and psychiatric comorbidity. Psychosomatic Medicine 68:99–103, 2006
Lloyd-Richardson EE, King TK, Forsyth LH, et al.: Body image evaluations in obese females with binge eating disorder. Eating Behaviors 1:161–171, 2000
Steiger H, Joober R, Israel M, et al.: The 5HTTLPR polymorphism, psychopathologic symptoms, and platelet [3H-] paroxetine binding in bulimic syndromes. International Journal of Eating Disorders 2005;37:57–60, 2005
Vinai P, Todisco P: Eziopatogenesi. La fame infinita. Turin, Centro Scientifico Editore, pp. 33–44, 2008 (Italian)
Safarinejad MR: The effects of the adjunctive bupropion on male sexual dysfunction induced by a selective serotonin reuptake inhibitor: A double-blind placebo-controlled and randomized study. BJU International 106:840–847, 2010
Acknowledgments
The authors would like to thank Dr. Antonina Luca from Catania for her precious help in the first review of this article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Calandra, C., Russo, R.G. & Luca, M. Bupropion Versus Sertraline in the Treatment of Depressive Patients with Binge Eating Disorder: Retrospective Cohort Study. Psychiatr Q 83, 177–185 (2012). https://doi.org/10.1007/s11126-011-9192-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11126-011-9192-0