
Abstract
Purpose
Binge eating disorder (BED) has a considerable clinical relevance by virtue of its high numerous psychiatric and medical comorbidities; among the latter, the most frequent is obesity. Available treatments for BED have shown frequent relapse of binges or weight regain in the long term. The new combination of naltrexone and bupropion sustained release (NB) has proved to be effective for weight loss among obese patients. As NB acts on hypothalamic and reward circuits, that seem involved in the pathogenesis and maintenance of BED symptoms, this study aims to evaluate the efficacy of NB in improving pathological eating behavior and losing weight in BED patients.
Methods
In this preliminary study, 23 obese-BED patients and a control group of 20 obese non-BED patients (respectively, Groups 1 and 2) who had previously undergone at least 5 unsuccessful weight-loss programs were treated with NB in addition to modified life style. Evaluation at t0 and after 16 weeks of treatment (t1) included anthropometric measurement, eating behavior assessment and psychopathological questionnaires (EDE-Q, BES, YFAS, BDI and STAI).
Results
A significant and similar weight loss (ΔBMI% ≈ 8%) was evident for both groups. Pathological eating behavior (i.e., binge, grazing, emotional eating, craving for carbohydrates, and post-dinner eating), BES score and YFAS severity significantly improved, especially among BED. NB was well tolerated and drop-out rate was low.
Conclusion
Treatment with NB, in addition to a reduced-calorie diet and increased physical activity, seems an effective and well-tolerated option for improving pathological eating behavior and losing weight in obese-BED patients.
Level of evidence
Level III case–control study.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Binge eating disorder (BED) is the most frequent eating disorder in the general population affecting all age groups, from childhood to adulthood, and both sexes [1, 2]. Genetic, environmental and neurobiological factors seem involved in its pathogenesis. BED is of considerable clinical relevance by virtue of its numerous psychiatric [3] and medical comorbidities; among the latter, the most frequent is obesity [4]. Treatments for BED (i.e., psychotherapy, educational interventions and pharmacological therapies) have traditionally targeted the improvement of eating behavior and the associated psychopathology and, for those patients who are also overweight or obese, weight loss. Despite the variety of proposed interventions, no treatment has demonstrated significantly superior efficacy and long-term studies do not support the maintenance of efficacy [5]. In recent years, the pharmacological approach has gained growing interest in the treatment of BED [6, 7]. The FDA approved the indication for lisdexamfetamine in the treatment of BED and although its effectiveness has been demonstrated, lisdexamfetamine is not exempt from significant adverse events and high discontinuation rates [8] Naltrexone, an opioid antagonist, also seems a useful drug in managing binge eating/abnormal eating behaviors [7, 9] and reducing purging in eating disorders [9] that are crucial for the regulation of energy balance. More recently, the combination of naltrexone/bupropion extended release (NB) has demonstrated to be effective for weight loss treatment either among obese patients (BMI ≥ 30 kg/m2) or overweight patients with severe medical comorbidities (e.g., diabetes, hypertension and dyslipidemia) (BMI = 25–29.9 kg/m2) [7, 10,11,12,13]. Considering that this formulation includes an anti-opioid agent and an antidepressant that exert their function at the level of appetite and food intake regulation (the hypothalamic circuit of melanocortin) [14, 15] and the reward pathway (mesolimbic dopaminergic circuit) [16] that seems involved in the pathogenesis and maintenance of BED symptoms, it could be interesting to evaluate the efficacy of NB in the treatment of pathological eating behavior among patients with BED.
Thus, the aim of this preliminary study was to evaluate the efficacy and tolerability of NB in the treatment of pathological eating behaviors and weight loss among BED-obese patients. We hypothesize that NB is not only effective for reducing weight but also improves pathological eating behaviour among obese BED patients.
Methods
Participants
Treatment-seeking obese (BMI ≥ 30 kg/m2) individuals, with and without BED, presenting to a weight-loss treatment program were recruited consecutively at an Eating Disorder unit from 1 July 2018 to 30 June 2019. During this period, a control group of obese no-BED patients was simultaneously recruited in this unit. Inclusion criteria were: male and female patients; age 18–65 years; diagnosis of BED according to DSM-5; obesity (BMI ≥ 30 kg/m2); having undergone at least five weight-loss programmes without success; and able to respond autonomously to self-administered questionnaires. Conversely, patients were excluded from the study in the case of: age out of the range 18–65 years; incapable of expressing valid consent; psychotic disorders; suicidal risk; alcohol or substance abuse; pregnant women or women within 12 months of childbirth and/or breastfeeding; antidiabetic or hypoglycemic therapy; and contraindications to the use of NB (e.g., anorexia nervosa, bulimia nervosa, uncontrolled hypertension, history of seizure disorders, severe kidney or hepatic failure). With the sole exception of the diagnosis of BED, which was considered an exclusion criterion, the same inclusion and exclusion criteria were applied to the control group.
Procedures
Patients were informed individually about the aim, procedures and anonymity of the study and that participation was voluntary with no monetary cost. Each patient was duly informed of the possible risks of NB and they were also given the chance to leave the study at any time.
Participants then underwent a medical/nutritional visit to evaluate their physical health, anthropometric data and previous and current eating history. Finally, a psychiatrist with adequate training in the field of eating disorders interviewed each participant using the Structured Clinical Interview for psychiatric disorders according to DSM-5 (SCID-I), the Binge Eating Disorder Clinical Interview (BED-CI) and the Altered Eating Behaviours Checklist (already described elsewhere) [17] to assess psychiatric disorders, eating behaviors (e.g., night eating, post-dinner eating, hyperphagia, social eating, sweet eating, emotional eating, grazing, craving for carbohydrates) and to verify the BED diagnosis.
Each patient was evaluated using the following scales:
Binge Eating Scale (BES) [18]. This self-administered test is widely used in research to measure binge-eating severity in the binge eating population. Total BES scores of < 17, 17–27 and > 27 indicate that the risk of an individual having BED is unlikely, possible and probable, respectively.
Eating Disorder Examination Questionnaire 6.0 (EDE-Q) [19]. This is a 28-item instrument to assess features of eating disorders and core eating disorder behaviors. It has four subscales, each consisting of five to eight items: Eating Restraint, Eating Concern, Weight Concern and Shape Concern, which are used to calculate a global EDE-Q score.
Yale Food Addiction Scale 2.0 (YFAS), Italian version [20,21,22,23]. The YFAS 2.0 assesses addiction-like eating behavior over the past 12 months. The scale consists of 35 items, scored on an eight-point scale ranging from never (score = 0) to every day (score = 7), that account for 11 symptoms.
Mood Disorder Questionnaire (MDQ) [24]. The MDQ is used to determine the lifetime presence of bipolar features and consists of three questions. The first question evaluates bipolar symptoms through 13 dichotomous (yes/no) items and the other two questions assess family history, past diagnoses and disease severity. Participants are considered positive if they simultaneously answer ‘yes’ to at least 7/13 items in Question 1 and indicate that the symptoms clustered within the same time period (‘yes’ to Question 2) caused moderate or serious problems (‘moderate’ or ‘serious’ for Question 3).
Beck Depression Inventory II (BDI) [25]. This self-report questionnaire assesses the severity of depressive symptoms. Scores of < 10, 10–16, 17–29 and 30 indicate minimum, mild, moderate and severe depression, respectively. A total score of > 16 is considered the clinical cut-off.
State–Trait Anxiety Inventory (STAI) [26]. This self-administered questionnaire is made up of 40 items that assess state anxiety (STAI-S) and trait anxiety (STAI-T). Only STAI-S was considered in this study.
Patients started therapy with NB after all evaluations were completed. NB is available as prolonged-release, film-coated tablets containing 8 mg of naltrexone·HCl and 90 mg of bupropion·HCl. Therapy was slowly increased from 1 tablet a day up to a maximum of 2 tablets twice a day after the third week; then therapy lasted for another 13 weeks, making a total of 16 weeks. Participants were allowed not to receive the maximum dose in cases of bearable side effects (e.g., nausea, constipation). Alongside the NB therapy, a lifestyle modification was prescribed at baseline that consisted of a hypo-caloric diet (reducing daily calorie intake of about 500 kcal), behavioral counseling and moderate aerobic physical activity (i.e., 20-min walk every day) during the 16 weeks. The study protocol was conducted in accordance with the ethical principles of the Declaration of Helsinki after being approved by the local ethics committee (no. 65/2018).
Data analysis
The data analysis was performed with the SPSS.21 statistical package. Analysis included the description (frequencies and percentages for categorical variables; means and standard deviations for continuous variables) and group comparison (Fisher’s exact test and Student’s t test). Variations between t0 and t1 were evaluated through general linear model (GLM) with repeated measures controlling for diagnosis and sex or Wilcoxon signed-rank, as appropriate. A value of p < 0.05 was considered statistically significant. For significant results, eta-squared (η2) for GLM, and Cohen’s d for Student’s t were calculated as measures of effect size [27].
Results
Sample description
From the 72 patients initially considered as potential candidates to be enrolled in this study, 27 were discharged because either did not fulfill the inclusion criteria (N = 5) or met at least one exclusion criteria (N = 22). Only 2 patients refused to participate because not interested in. Thus, twenty-three consecutive obese BED patients (Group 1: 17 females, 6 males) and a control group of 20 obese non-BED patients (Group 2: 10 females, 10 males) were enrolled. Four patients in Group 1 (2 females and 2 males) and 5 patients in Group 2 (3 males, 2 females) dropped out from the study for several reasons (i.e. 2 for city change, 1 for pregnancy, 4 for nausea, 1 for constipation, 1 for itch). Thus, 19 obese BED patients (Group 1) and a control group of 15 obese non-BED patients (Group 2) completed the 16-week protocol. The samples were matched for BMI, gender and age. The control group had a slightly higher but comparable BMI at t0 (Group 1 = 39.0 ± 7.8 vs Group 2 = 43.8 ± 9.6; t = − 1.608; p = 0.118). Sociodemographic characteristics of the sample are given in Table 1. Patients with depression were overrepresented in Group 1 (see Table 1).
Efficacy in weight loss
A significant weight loss was evident for completers over 16 weeks of treatment with high effect size (η2 > 0.8) regardless diagnosis or sex [F(1,27) = 112.097; p < 0.001]. Weight loss was similar in both groups (ΔBMI%: Group 1 = 8.0 ± 3.9 vs. Group 2 = 7.8 ± 2.9; t = 0.162; p = 0.872) and reached a similar BMI after treatment (Group 1 = 35.8 ± 6.8 vs Group 2 = 40.3 ± 8.8; t = − 1.687; p = 0.101). Overall, 85% of patients lost at least 5% of their initial weight (Fig. 1).

Reduction of BMI at 16 weeks
Only five patients (10%) had a poor weight loss (ΔBMI% < 5%); most of them from Group 1, had a comorbid bipolar disorder type 2 and showed poor adherence to modification of their lifestyle (e.g., changing their diet and increasing physical activity) from the beginning. The maximum NB dose reached was similar in both groups (3.74 ± 0.56 and 3.36 ± 0.67 tablets in obese BED and non-BED patients, respectively).
Eating behaviour
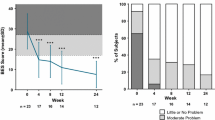
Pathological eating behaviour of BED patients considerably improved at 16 weeks with significant reductions in binge (p = 0.003), grazing (p = 0.013), craving for carbohydrates (p = 0.001), emotional eating (p = 0.021) and post-dinner eating (p = 0.021). Differences were also evident in Group 2 in hyperphagia (p = 0.031), social eating (p = 0.031), grazing (p = 0.008) and craving for carbohydrates (p = 0.031). (Fig. 2).

Modification of pathological eating behaviour within the two groups
Psychopathology
Among BED patients, EDE-Q Eating Restraint significantly increased (p = 0.031; η2 = 0.156) and BES score significantly decreased (p = 0.04; η2 = 0.133) at t1. EDE-Q Weight Concern (p = 0.048; η2 = 0.128) decreased at t1 in the control group (Table 2). A noteworthy overall reduction in the severity of food addiction was evident at the end of the study (Fig. 3) and the total number of DSM-5 criteria significantly decreased at t1 (p = 0.03; η2 = 0.143), specially among BED female patients.

Reduction of food addiction (FA) severity within the two groups
Tolerability
All drop-outs due to side effects were registered within the third week of therapy. Age (t = 0.311; p = 0.758), sex (χ2 = 1.64; p = 0.200) and diagnosis distribution (χ2 = 0.000; p = 0.986) were similar between completers and dropouts. Side effects were comparable among completers and drop-outs (see Supplementary material). The only significant difference between patients who dropped out and completers was related to anxiety: compared to their counterparts, drop-outs showed a higher baseline STAI-S score (57.9 ± 12.9 vs. 44.1 ± 10.8; t = 3.271; p = 0.002) and more weight concern at EDE-Q scale (4.8 ± 1.4 vs 3.6 ± 1.5; t = 2.138; p = 0.039).
Although nausea was very frequent (67%) among completers, it appeared in the first weeks of treatment and was successfully managed. Other side effects reported were anxiety (22%), headache (11%), diarrhea (11%) and sweating (11%). Instead, no hypertensive crisis or maniac/hippomaniac switches were observed. Side effects were successfully managed with a reduction in the NB dose or a slower titration.
Discussion
This preliminary study aimed to evaluate the tolerability and efficacy of NB in the treatment of pathological eating behavior and weight loss among BED-obese patients. Our results suggest that NB can be useful for improving pathological eating behaviors and weight loss in obese BED patients [28,29,30,31,32,33] according to our hypothesis. The reason may be the peculiar mechanism of action on NB in the control of hunger and appetite [34]. Bupropion stimulates hypothalamic POMC neurons, promoting a cascade of actions that result in reduced energy intake and increased energy expenditure [35]. Naltrexone blocks POMC auto-inhibition mediated by μ-opioid receptors, thus increasing POMC activation, amplifying effects on energy balance and facilitating weight loss. As a result, the combination of bupropion and naltrexone works synergistically to produce a greater increase in POMC activity than either drug alone [7, 31]. Furthermore, NB is also hypothesized to induce weight loss through sustained modulation of central nervous system reward pathways, an effect likely to be mediated by changes in dopamine concentration within the mesolimbic system [7, 33].
Efficacy of NB on pathological eating behavior and psychopathology
The Eating Restraint subscale of EDE-Q is considered to be a measure of the reduction in food intake. In obese BED patients, as hypothesized, there was a significant improvement in self-reported binge behavior assessed with the BES.
Drugs such as sibutramine [36], rimonabant [37] or pramlintide [38] have been approved for long-term weight management and have shown an improvement in controlling binge eating behavior in obese patients and a reduction in BES scores but have recently been withdrawn from the market or had research stopped due to safety concerns. Previously, an open-label single-arm study of participants with obesity and major depressive disorder treated with NB and a lifestyle modification demonstrated a significant reduction in BES scores supporting the notion that NB may help BED-obese patients in controlling their eating behavior [39]. Recently, the data were also replicated in another multicenter, randomized, controlled, open-label trial [40]. Lisdexamfetamine, the only FDA approved medication for BED, reduces significantly the number of binge episodes [6] but is not completely free of side effects and is not indicated for weight loss; its effects on obesity are unknown, and similar medication classes have been associated with cardiovascular adverse events in the past [41].
Although most medications that have not the indication for the treatment of BED such as the antidepressants (fluoxetine, sertraline, citalopram, escitalopram, vortioxetine) are relatively well tolerated, a number of patients’ experience side effects [6]. However, significant weight loss was not evident among subjects treated with antidepressant drugs, probably due to the short duration (8 weeks) of the trials on a chronic disorder such as BED [42].
Topiramate is more effective than placebo in promoting weight loss, reducing the weekly and daily frequency of binge episodes, and improving the psychopathology of BED [43].
Our patients exhibited better control of eating behavior after treatment with NB. Not only a trend towards greater food restriction, but also a reduction in binge eating, grazing, craving for carbohydrates and less severe food addiction were evident. The explanation may be due to the double mechanism of action of NB on the mesolimbic dopamine system (related to the reward system and the regulation of eating behavior) [9, 44] and the µ-opioid receptors (related to “liking” and “wanting”) [45], and in particular to the synergistic effect of naltrexone and bupropion [7, 46].
In vivo [33] studies have shown superior efficacy in reducing food intake of the injection of naltrexone/bupropion combination that would act synergistically with respect to the separate injection of each drug. Further, as the neurobiological substrates of the two systems are strongly connected [47], this could further explain the positive impact of NB on food addiction in our patients. Food addiction is extensively related to BED and obesity [48] and research has demonstrated that the severity of food addiction is closely associated with more severe eating psychopathology (e.g., frequency of binges) and psychological impairment [49, 50]. Adults with food addiction have elevated dopamine-related neural activations [51] with increased activation of dopamine D1 and µ-opioid receptors in response to food cues [52], similar to those observed among adults with substance use disorders [53, 54]. The improvement of other pathological eating behaviors (i.e., grazing, emotional eating and craving for CH) may be similarly explained.
Efficacy of NB on body weight
Previous studies have demonstrated the efficacy of NB for reducing body weight in obese or overweight patients with medical comorbidities [28,29,30,31,32, 55, 56] and present results are in line with the cited studies: overall, 85% of patients lost at least 5% of their body weight at 16 weeks, the minimum treatment time needed to assess the effectiveness of the drug, with an average mean of 8% weight loss. Old and new anti-obesity medications approved by the FDA for the treatment of obesity as lorcaserin, orlistat, phentermine/topiramate extended release and liraglutide are the most commonly used anti-obesity medications [41, 57] that although effective have reported undesirable side effects, contraindications, or drug–drug interactions [57]. Naltrexone/bupropion extended release was approved for the treatment of obesity in 2014. Bupropion is a dopamine and norepinephrine reuptake inhibitor that was FDA approved as an antidepressant in 1989 and as a smoking cessation aide in 1997. Naltrexone is an opioid antagonist that was FDA approved for the treatment of opioid dependence in 1984 and alcohol use disorder in 1994 [57].
Bupropion monotherapy is capable of producing modest weight loss [58, 59]; whereas, naltrexone is associated with negligible weight loss effects. Their action on the hypothalamic system explains the weight reduction: the central hypothalamic relay regulates homeostasis, controlling food intake and energy expenditure balance [60] and metabolism [61, 62]. However, naltrexone has a synergistic effect when combined with bupropion, promoting a reduction of energy intake and an increase in energy expenditure [7]. As a result, patients lose weight, with no differences between obese BED or non-BED subjects [63] in line with the literature that conducted trials to evaluate the effect of naltrexone/bupropion plus lifestyle modification in patients with overweight or obesity [12, 13, 28, 31, 32].
Tolerability of NB
Current data on tolerability of NB seem to be in line with previous reports [64, 65]. Although nausea was very frequent during the titration phase of treatment, side effects in most cases were transient and not grounds for stopping treatment and were managed through the adjustment of the dose or a lower titration. NB showed quite a safe profile as no rare or serious effects occurred: despite data in the literature reporting possible elevations or hypertensive crises (to be attributed to the sympathomimetic effects of bupropion) that create concerns for cardiovascular safety, no patient developed hypertensive crises and there were no switches towards hypo or maniac phases in any patient, even where the drug was given to patients with bipolar disorders or in association with other antidepressants [65]. As note, bupropion treatment can increase the risk of seizures and therefore its use in underweight patients or in those with anorexia or bulimia nervosa is contraindicated. In our sample, no new-onset epileptic seizures were recorded. Furthermore, the frequency of adverse symptoms was comparable between completers and drop-outs even if their intensity was not measured.
The presence of an anxious trait was predictive of poor compliance and, therefore, of premature dropout [66]. This could be explained by the greater difficulty in tackling a path not only pharmacologically but also with the accompanying change in lifestyle, which were both necessary conditions to enter the protocol study and also for weight loss. These observations further suggest the need to identify more accurately those patients to whom to propose treatment and who are motivated enough to be adherents.
Limitations and strengths
To date, this is the first Italian study aiming to evaluate the effectiveness of this NB drug combination in an obese BED sample compared to an obese control group. This allowed us to identify a new population with an eating disorder that may benefit from NB treatment. Patients with BED, with a history of numerous diet programmes and/or other previous treatments for weight reduction that were not completely effective and with other medical comorbidities found an important aid in reducing body weight.
Among the limitations of this preliminary report, the small number of patients enrolled should be considered. The data refer to a consecutive and naturalistic recruitment of patients for an open label trial, not blinded, not randomized, nor placebo controlled. Results should be considered in light of a possible placebo response associated with BED in those with less severe eating pathology as previously suggested [67]. For this reason, other studies that can corroborate and replicate the results are needed. Because BED requires long-term management (e.g., > 16 weeks), data regarding the longer-term efficacy of NB are needed, as well as longer evaluation periods for a safety profile in these patients. Thus, a longer follow-up is needed to ascertain the true utility. The intensity of side effects do to NB assumption was not evaluated, but just the presence/abscense of adverse effects.
Practical considerations
If on the one hand, there are clinicians and researchers who believe that the main focus should be on reduction of BED symptoms and that too much focus on weight loss may worsen, not improve, BED symptoms, we instead think that weight reduction should be simultaneously addressed together with pathological eating behaviors as in most cases it is the main motivation for patients to look for treatment.
Despite the variety of proposed interventions, no strategy has demonstrated a clear superiority in the long term to treat the complex clinical picture of obese patients with BED.
NB is a pharmacological treatment that has shown a significant benefit for obese BED patients with not life-threatening for health side effects. The use of NB for obese BED patients who had previously undergone several weight-loss programmes without success might help patients not only with loosing weight (and thus the associated physical comorbidities) but also to increase their motivation and engagement in the treatment of the psychiatric disorder. As a result, it is possible to state that NB may represent an acceptable therapeutic option for BED, not only for both induction of weight loss and its maintenance, but also for improvement of the psychopathological aspects related to the disorder, in association with a lifestyle change.
Conclusion
The sustained release NB combination (8–90 mg), in addition to a hypocaloric diet and physical activity, seems an effective and well-tolerated option for treating altered eating behaviours and lose weight in obese adults with BED who are resistant to weight-loss programmes. Future studies could assess both the long-term safety and the possible changes induced by NB on inflammatory indices, glyco-metabolic indices and risk of cardiovascular complications of BED-obese patients who, due to the natural history of the eating disorder, are generally exposed to severe medical complications.
What is already known on this subject?
BED has numerous psychiatric and medical comorbidities, among the latter, the most frequent is obesity. Available treatments for BED have shown frequent relapse of binges or weight regain in the long term. NB, which has already proved its efficacy weight loss among obese patients, acts on hypothalamic and reward circuits, that seem involved in the pathogenesis and maintenance of BED symptoms.
What does this study add?
This preliminary study suggests that the sustained release naltrexone/bupropion combination may be an effective and well-tolerated option in the treatment of pathological eating behaviour of adult obese-BED patients. Long-term studies should test the tolerability and the maintenance of efficacy of NB in BED.
References
Guerdjikova AI, Mori N, Casuto LS, McElroy SL (2019) Update on binge eating disorder. Med Clin N Am 103:669–680. https://doi.org/10.1016/j.mcna.2019.02.003
Hay P (2020) Current approach to eating disorders: a clinical update. Intern Med J 50:24–29. https://doi.org/10.1111/imj.14691
Segura-Garcia C, Caroleo M, Rania M et al (2017) Binge eating disorder and bipolar spectrum disorders in obesity: psychopathological and eating behaviors differences according to comorbidities. J Affect Disord 208:424–430. https://doi.org/10.1016/j.jad.2016.11.005
Succurro E, Segura-Garcia C, Ruffo M et al (2015) Obese patients with a binge eating disorder have an unfavorable metabolic and inflammatory profile. Medicine (United States) 94:1–7. https://doi.org/10.1097/MD.0000000000002098
Brownley KA, Berkman ND, Peat CM et al (2016) Binge-eating disorder in adults a systematic review and meta-analysis. Ann Intern Med 165:409–420
Amodeo G, Cuomo A, Bolognesi S et al (2019) Pharmacotherapeutic strategies for treating binge eating disorder. Evidence from clinical trials and implications for clinical practice. Expert Opin Pharmacother 20:679–690
Valbrun LP, Zvonarev V (2020) The opioid system and food intake: use of opiate antagonists in treatment of binge eating disorder and abnormal eating behavior. J Clin Med Res 12:41–63. https://doi.org/10.14740/jocmr4066
Fornaro M, Solmi M, Perna G et al (2016) Lisdexamfetamine in the treatment of moderate-to-severe binge eating disorder in adults: systematic review and exploratory meta-analysis of publicly available placebo-controlled, randomized clinical trials. Neuropsychiatr Dis Treat 12:1827–1836. https://doi.org/10.2147/NDT.S109637
Stancil SL, Adelman W, Dietz A, Abdel-Rahman S (2019) Naltrexone reduces binge eating and purging in adolescents in an eating disorder program. J Child Adolesc Psychopharmacol 29:721–724. https://doi.org/10.1089/cap.2019.0056
Contrave Prescribing Information (2014) https://www.accessdata.fda.gov/drugsatfda_docs/label/2014/200063s000lbl.pdf. Accessed 20 Mar 2020
Mysimba | European Medicines Agency. https://www.ema.europa.eu/en/medicines/human/EPAR/mysimba. Accessed 20 Mar 2020
Hollander P, Gupta AK, Plodkowski R et al (2013) Effects of naltrexone sustained-release/bupropion sustained-release combination therapy on body weight and glycemic parameters in overweight and obese patients with type 2 diabetes. Diabetes Care 36:4022–4029. https://doi.org/10.2337/dc13-0234
Wadden TA, Foreyt JP, Foster GD et al (2011) Weight loss with naltrexone SR/bupropion SR combination therapy as an adjunct to behavior modification: the COR-BMOD trial. Obesity (Silver Spring) 19:110–120. https://doi.org/10.1038/oby.2010.147
Morton GJ, Meek TH, Schwartz MW (2014) Neurobiology of food intake in health and disease. Nat Rev Neurosci 15:367–378. https://doi.org/10.1038/nrn3745
Morton GJ, Blevins JE, Williams DL et al (2005) Leptin action in the forebrain regulates the hindbrain response to satiety signals. J Clin Invest 115:703–710. https://doi.org/10.1172/JCI22081
Volkow ND, Wang G-J, Baler RD (2011) Reward, dopamine and the control of food intake: implications for obesity. Trends Cogn Sci 15:37–46. https://doi.org/10.1016/j.tics.2010.11.001
Caroleo M, Primerano A, Rania M et al (2018) A real world study on the genetic, cognitive and psychopathological differences of obese patients clustered according to eating behaviours. Eur Psychiatry 48:58–64. https://doi.org/10.1016/j.eurpsy.2017.11.009
Gormally J, Black S, Daston S, Rardin D (1982) The assessment of binge eating severity among obese persons. Addict Behav 7:47–55
Fairburn CG, Beglin SJ (1994) Assessment of eating disorders: interview or self-report questionnaire? Int J Eat Disord 16:363–370
Aloi M, Rania M, Rodríguez Muñoz RC et al (2017) Validation of the Italian version of the Yale Food Addiction Scale 2.0 (I-YFAS 2.0) in a sample of undergraduate students. Eat Weight Disord 22:527–533. https://doi.org/10.1007/s40519-017-0421-x
Manzoni GM, Rossi A, Pietrabissa G et al (2018) Validation of the Italian Yale Food Addiction Scale in postgraduate university students. Eat Weight Disord 23:167–176. https://doi.org/10.1007/s40519-018-0495-0
Imperatori C, Fabbricatore M, Lester D et al (2019) Psychometric properties of the modified Yale Food Addiction Scale Version 2.0 in an Italian non-clinical sample. Eat Weight Disord 24:37–45. https://doi.org/10.1007/s40519-018-0607-x
Manzoni GM, Rossi A, Pietrabissa G et al (2020) Structural validity, measurement invariance, reliability and diagnostic accuracy of the Italian version of the Yale Food Addiction Scale 2.0 in patients with severe obesity and the general population. Eat Weight Disord. https://doi.org/10.1007/s40519-020-00858-y
Hardoy M, Cadeddu M, Murru A et al (2005) Validation of the Italian version of the Mood Disorder Questionnaire for the screening of bipolar disorders. Clin Pract Epidemiol Mental Health 1:8. https://doi.org/10.1186/1745-0179-1-8
Beck AT, Ward CH, Mendelson M et al (1961) An inventory for measuring depression. Arch Gen Psychiatry 4:561–571
Spielberger C, Gorsuch R, Lushene R (1970) STAI Manual for the State-Trait Anxiety Inventory. Palo Alto
Cohen J (1988) Statistical power analysis for the behavioral sciences, 2nd edn. Lawrence Erlbaum Associates Inc., Hillsdale
Greenway FL, Dunayevich E, Tollefson G et al (2009) Comparison of combined bupropion and naltrexone therapy for obesity with monotherapy and placebo. J Clin Endocrinol Metab 94:4898–4906. https://doi.org/10.1210/jc.2009-1350
Smith SR, Fujioka K, Gupta AK et al (2013) Combination therapy with naltrexone and bupropion for obesity reduces total and visceral adiposity. Diabetes Obes Metab 15:863–866. https://doi.org/10.1111/dom.12095
Sherman MM, Ungureanu S, Rey JA (2016) Naltrexone/bupropion ER (Contrave): newly approved treatment option for chronic weight management in obese adults. P T 41:164–172
Apovian CM, Aronne L, Rubino D et al (2013) A randomized, phase 3 trial of naltrexone SR/bupropion SR on weight and obesity-related risk factors (COR-II). Obesity (Silver Spring) 21:935–943. https://doi.org/10.1002/oby.20309
Greenway FL, Fujioka K, Plodkowski RA et al (2010) Effect of naltrexone plus bupropion on weight loss in overweight and obese adults (COR-I): a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 376:595–605. https://doi.org/10.1016/S0140-6736(10)60888-4
Billes SK, Sinnayah P, Cowley MA (2014) Naltrexone/bupropion for obesity: an investigational combination pharmacotherapy for weight loss. Pharmacol Res 84:1–11. https://doi.org/10.1016/j.phrs.2014.04.004
Davis C (2017) A commentary on the associations among ‘food addiction’, binge eating disorder, and obesity: overlapping conditions with idiosyncratic clinical features. Appetite 115:3–8. https://doi.org/10.1016/j.appet.2016.11.001
Gadde KM, Allison DB, Ryan DH et al (2011) Effects of low-dose, controlled-release, phentermine plus topiramate combination on weight and associated comorbidities in overweight and obese adults (CONQUER): a randomised, placebo-controlled, phase 3 trial. Lancet (London, England) 377:1341–1352. https://doi.org/10.1016/S0140-6736(11)60205-5
Appolinario JC, Godoy-Matos A, Fontenelle LF et al (2002) An open-label trial of sibutramine in obese patients with binge-eating disorder. J Clin Psychiatry 63:28–30. https://doi.org/10.4088/JCP.v63n0106
Pataky Z, Gasteyger C, Ziegler O et al (2013) Efficacy of rimonabant in obese patients with binge eating disorder. Exp Clin Endocrinol Diabetes 121:20–26. https://doi.org/10.1055/s-0032-1329957
Smith SR, Blundell JE, Burns C et al (2007) Pramlintide treatment reduces 24-h caloric intake and meal sizes and improves control of eating in obese subjects: a 6-wk translational research study. Am J Physiol Endocrinol Metab 293:E620–E627. https://doi.org/10.1152/ajpendo.00217.2007
McElroy SL, Guerdjikova AI, Kim DD et al (2013) Naltrexone/bupropion combination therapy in overweight or obese patients with major depressive disorder: results of a pilot study. Prim Care Companion J Clin Psychiatry. https://doi.org/10.4088/PCC.12m01494
Halseth A, Shan K, Gilder K et al (2018) Quality of life, binge eating and sexual function in participants treated for obesity with sustained release naltrexone/bupropion. Obes Sci Pract 4:141–152. https://doi.org/10.1002/osp4.156
Reas DL, Grilo CM (2015) Pharmacological treatment of binge eating disorder: update review and synthesis. Expert Opin Pharmacother 16:1463–1478
Stefano SC, Bacaltchuk J, Blay SL, Appolinário JC (2008) Antidepressants in short-term treatment of binge eating disorder: systematic review and meta-analysis. Eat Behav 9:129–136
Leombruni P, Lavagnino L, Fassino S (2009) Treatment of obese patients with binge eating disorder using topiramate: a review. Neuropsychiatr Dis Treat 5:385–392
Kelley AE, Berridge KC (2002) The neuroscience of natural rewards: relevance to addictive drugs. J Neurosci 22:3306–3311. https://doi.org/10.1523/JNEUROSCI.22-09-03306.2002
Peciña S, Berridge KC (2005) Hedonic hot spot in nucleus accumbens shell: where do mu-opioids cause increased hedonic impact of sweetness? J Neurosci 25:11777–11786. https://doi.org/10.1523/JNEUROSCI.2329-05.2005
Sinnayah P, Wallingford N, Evans A, Cowley M (2007) Bupropion and naltrexone interact synergistically to decrease food intake in mice. In: North American association for the study of obesity annual scientific meeting, New Orleans
Kessler RM, Hutson PH, Herman BK, Potenza MN (2016) The neurobiological basis of binge-eating disorder. Neurosci Biobehav Rev 63:223–238. https://doi.org/10.1016/j.neubiorev.2016.01.013
Jiménez-Murcia S, Agüera Z, Paslakis G et al (2019) Food addiction in eating disorders and obesity: analysis of clusters and implications for treatment. Nutrients 11:2633. https://doi.org/10.3390/nu11112633
Gearhardt AN, White MA, Potenza MN (2011) Binge eating disorder and food addiction. Curr Drug Abuse Rev 4:201–207
Gearhardt AN, White MA, Masheb RM et al (2012) An examination of the food addiction construct in obese patients with binge eating disorder. Int J Eat Disord 45:657–663. https://doi.org/10.1002/eat.20957
Gearhardt AN (2011) Neural correlates of food addiction. Arch Gen Psychiatry 68:808. https://doi.org/10.1001/archgenpsychiatry.2011.32
Colantuoni C, Schwenker J, McCarthy J et al (2001) Excessive sugar intake alters binding to dopamine and mu-opioid receptors in the brain. NeuroReport 12:3549–3552
Davis C, Levitan RD, Kaplan AS et al (2014) Food cravings, appetite, and snack-food consumption in response to a psychomotor stimulant drug: the moderating effect of “food-addiction”. Front Psychol 5:403. https://doi.org/10.3389/fpsyg.2014.00403
Gordon EL, Ariel-Donges AH, Bauman V, Merlo LJ (2018) What is the evidence for “food addiction?” A systematic review. Nutrients. https://doi.org/10.3390/NU10040477
Yanovski SZ, Yanovski JA (2015) Naltrexone extended-release plus bupropion extended-release for treatment of obesity. JAMA 313:1213. https://doi.org/10.1001/jama.2015.1617
Ali KF, Shukla AP, Aronne LJ (2016) Bupropion-SR plus naltrexone-SR for the treatment of mild-to-moderate obesity. Expert Rev Clin Pharmacol 9:27–34. https://doi.org/10.1586/17512433.2016.1100072
Saunders KH, Umashanker D, Igel LI et al (2018) Obesity Pharmacotherapy. Med Clin N Am 102:135–148
White MA, Grilo CM (2013) Bupropion for overweight women with binge-eating disorder: a randomized, double-blind, placebo-controlled trial. J Clin Psychiatry 74:400–406. https://doi.org/10.4088/JCP.12m08071
Anderson JW, Greenway FL, Fujioka K et al (2002) Bupropion SR enhances weight loss: a 48-week double-blind, placebo- controlled trial. Obes Res 10:633–641. https://doi.org/10.1038/oby.2002.86
Witkamp RF (2011) Current and future drug targets in weight management. Pharm Res 28:1792–1818. https://doi.org/10.1007/s11095-010-0341-1
Morton GJ, Cummings DE, Baskin DG et al (2006) Central nervous system control of food intake and body weight. Nature 443:289–295. https://doi.org/10.1038/nature05026
Leibel RL, Rosenbaum M, Hirsch J (1995) Changes in energy expenditure resulting from altered body weight. N Engl J Med 332:621–628. https://doi.org/10.1056/NEJM199503093321001
Patel DK, Stanford FC (2018) Safety and tolerability of new-generation anti-obesity medications: a narrative review. Postgrad Med. https://doi.org/10.1080/00325481.2018.1435129
Bello NT (2019) Update on drug safety evaluation of naltrexone/bupropion for the treatment of obesity. Expert Opin Drug Saf. https://doi.org/10.1080/14740338.2019.1618268
Halpern B, Mancini MC (2017) Safety assessment of combination therapies in the treatment of obesity: focus on naltrexone/bupropion extended release and phentermine-topiramate extended release. Expert Opin Drug Saf 16:27–39. https://doi.org/10.1080/14740338.2017.1247807
Violante R, Santoro S, González C (2011) Prevalence of depression and anxiety in a cohort of 761 obese patients: impact in adherence to therapy and its outcome. Vertex 22:85–93
Blom TJ, Mingione CJ, Guerdjikova AI et al (2014) Placebo response in binge eating disorder: a pooled analysis of 10 clinical trials from one research group. Eur Eat Disord Rev 22:140–146. https://doi.org/10.1002/erv.2277
Acknowledgements
The authors thank all the patients who accepted to participate in this research and the pharmaceutical company Bruno Farmaceutici for providing the drug free of charge to every patient in the study.
Funding
No incentive was offered either to the patients or researchers who participated in the study.
Author information
Authors and Affiliations
Contributions
CSG designed the study. EAC, MC, MR, GC, FAS and RF collected the data. CSG and MA performed the statistical analysis. EAC, MC, MR wrote the first draft of the manuscript. CSG, GC, FAS, RF and FA made the first critical review; EAC wrote the final manuscript. All authors commented on, read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
Approval was obtained from the ethics committee of “Comitato Etico Regione Calabria, Area Centro” (no. 65/2018). The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
Informed consent
Informed consent was obtained from all individual participants included in the studies before any procedure took place.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.

Rights and permissions
About this article

{kind=link}
Cite this article
Carbone, E.A., Caroleo, M., Rania, M. et al. An open-label trial on the efficacy and tolerability of naltrexone/bupropion SR for treating altered eating behaviours and weight loss in binge eating disorder. Eat Weight Disord 26, 779–788 (2021). https://doi.org/10.1007/s40519-020-00910-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40519-020-00910-x