
Abstract
Social functioning (SF) is the ultimate target aimed in treatment plans in schizophrenia, thus it is critical to know what are the factors that determine SF. Gender is a well-established variable influencing SF, yet it is not known how social variables and symptoms interact in schizophrenia patients. Furthermore, it remains unclear whether the interaction between social variables and symptoms is different in men compared to women. Our aim is to test whether social variables are better predictors of SF in community-dwelled individuals with schizophrenia, and whether men and women differ in how symptoms and social variables interact to impact SF. Community-dwelling individuals with schizophrenia (N = 231) were randomly selected from a register. Participants were assessed with symptom measures (PANSS), performance-based social scale (LSP), objective social and demographic variables. Stratification by gender and stepwise multivariate regression analyses by gender were used to find the best-fitting models that predict SF in both gender. Men had poorer SF than women in spite of showing similar symptom scores. On stepwise regression analyses, gender was the main variable explaining SF, with a significant contribution by disorganized and excitatory symptoms. Age of onset made a less marked, yet significant, contribution to explain SF. When the sample was stratified by gender, disorganized symptoms and ‘Income’ variable entered the model and accounted for a 30.8% of the SF variance in women. On the other hand, positive and disorganized symptoms entered the model and accounted for a 36.1% of the SF variance in men. Community-dwelling men and women with schizophrenia differ in the constellation of variables associated with SF. Symptom scores still account for most of the variance in SF in both genders.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Social functioning (SF) in schizophrenia is defined as the patient’s capacity to adjust to personal, family, social, and professional needs. In addition, SF includes the person’s ability to take care of him/herself and perform socially defined roles in a particular culture [1, 2]. Such a combination of different high-order components makes SF a highly complex concept, which, in turn, is determined by a myriad variables belonging to different epistemological levels. Specifically, cognitive deficits and psychopathology, objective social variables such as marital status or living situation, or course variables such as age of onset or duration of untreated psychosis have been implicated in determining the level of functioning achieved by individuals afflicted by schizophrenia [3–7]. Being a multi-factorial determined concept, the search for determinants of SF in schizophrenia constitutes a challenging task where variables are better explored in context rather than in isolation.
Although there are current effective pharmacological treatments, psychological therapies, and rehabilitation strategies that achieve significant improvements in symptoms, individuals with schizophrenia still have severely impaired SF [8]. Moreover, SF is relevant because it is a measure closely related to the concept of everyday performance, and, therefore, is becoming the focus of any preventive, therapeutic, and rehabilitation plan [9]. Nonetheless, to ultimately pursue such a relevant goal, it is critical to elucidate which variables impact SF, how they interact with each other, and whether this interaction is different in women compared to men.
In this regard, gender is a well-known non-modifiable risk variable in schizophrenia. Specifically, women have better SF than men in spite of having the same levels of symptom [10–12]. There are a number of studies that point to biological differences such as hormonal differences [13], disrupted normal sexual brain dimorphisms in men [14], or preserved emotional prosodic processing in women to explain this difference in SF [15]. Nonetheless, the number of studies addressing questions regarding social variables is rather scarce; therefore, the question of whether men and women differ in their social profile set of risk factors remains unanswered.
We aim to explore the extent to which social variables play a role in determining SF in schizophrenia and the extent to which men and women differ in this regard. In other words, our primary hypothesis was that men’s and women’s profiles differ in the type and number of variables that explain their SF impairment. In addition, we hypothesized that social variables would have a more relevant role in explaining SF in a community-dwelling sample of individuals with schizophrenia.
Method
Participants
A total of 231 participants with schizophrenia were randomly selected from a register that included all patients under treatment in five mental health teams [ME2](MHT). The five catchment areas (Cerdanyola, Ciutat Vella, Cornella, Gava, and El Prat) contain a estimated population of 440,000 adults from the city of Barcelona and its surroundings, and house people of different socio-demographic backgrounds. Inclusion criteria were as follows: (a) primary diagnosis of schizophrenia (DSM-IV criteria) [16]; (b) age between 18 and 65 years; (c) live in the catchments areas of the participating MHT; and (d) have made at least one outpatient visit during the 6 months prior to the beginning of the study. Patients with a diagnosis of mental retardation or neurological disorder were excluded.
Diagnoses of all the selected individuals were reviewed by their treating psychiatrist; in case of discrepancy between the treating psychiatrist’s diagnosis and the diagnosis of schizophrenia that was in the register, the case was evaluated by two psychiatrists to make a final decision regarding the inclusion of the patient.
The institutional review board and the clinical ethical committee approved the study protocol in accordance with the declaration of Helsinki [17]. Informed consent was obtained by the treating psychiatrist.
Evaluation
Outcome/Dependent Variables
Social Functioning
The Life Skills Profile (LSP) is a specific instrument developed to evaluate SF in schizophrenia community samples and has been shown to have excellent psychometric properties in terms of reliability and validity for both the original English version and the Spanish one [18, 19]. A trained research staff administered the LSP to the person who was most familiar with the participant’s functioning (e.g. relatives, friends, case manager). The LSP evaluates SF through a 39-item questionnaire that assesses specific areas of SF in a jargon-free language. Answers are codified in an ordinal scale from 1 to 4, with 1 being the least functional and 4 the most functional; therefore, the higher the score the better the SF. The scale has five domains: Self-Care (SC) assesses aspects related to ordinary duties (e.g., Does the patient usually do his/her laundry without a reminder required?); non-turbulence (NT) assesses the presence of disruptive behaviors (e.g., Does the patient destroy anyone else’s belongings?); Socialization (S) assesses the extent to which the patient is able to fluently interact (e.g., Does the patient usually get offended?); Communication (C) assesses whether social communication skills are properly used and put in action (e.g., Does the patient have difficulties initiating or answering during a conversation?); and finally, Responsibility (R) assesses the extent to which the patient is able to develop an autonomous lifestyle (e.g., Is the patient able to usually cook his/her own meals?).
Predictive/Independent Variables
Demographic Variables
Clinically related demographic variables such as age, age of onset, and duration of illness were obtained through a comprehensive review of several complementary sources of information to enforce maximum level of accuracy: the patient’s electronic clinical chart, the paper-based clinical chart, patient interview, family interview, and attending psychiatrist.
Objective Social Variables
Marital status, income, education, occupation, and living situation were thoroughly assessed through questionnaires by interviewing patients as well as all other available collateral information sources (i.e., closest caregiver, staff, and family).
Psychopathology
The Positive and Negative Syndrome Scale (PANSS), the Spanish version [20, 21], was administered by the treating psychiatrist. PANSS items were grouped according to a five-dimensional classification scheme with the domains of Positive, Negative, Excited, Disorganized, and Depression symptoms [22].
Data Analyses
χ2 and Student t tests were used to compare the differences in objective social, demographic, and psychopathological variables by gender. Stepwise multiple regression analyses were employed to evaluate the association of subscales of LSP with demographic, objective social, and psychopathological variables. Total LSP score and LSP sub-scores were the dependent variables and gender, age, age of onset, duration of illness, income, marital status, living situation, occupation, education, PANSS total score, and PANSS sub-scores were the independent variables. To further explore and control for gender-related unbalance, we stratified the sample by gender and fitted a regression analysis for each gender.
All statistical analyses were calculated with SPSS for Windows 10.0.
Results
Descriptive Statistics
Demographic, social, and psychopathological variables are thoroughly presented in Table 1. Briefly, the majority of the 231 participants (63.6%) were men. Mean age of women was higher than that of men (44 vs. 37 years, respectively, p < 0.001). While men had a lower mean age of onset than women (22 vs. 24 years, p = 0.02), women had a longer mean duration of the disorder (24 vs. 20 years, p < 0.001).
In regards to subjective social indicators, women displayed a higher level of SF (LSP total 124.52 vs. 117.84, p = 0.003), scoring significantly higher on the SF scale in both total and sub-scale scores, with the exception of the NT sub-scale. On the other hand, we observed that women had better objective social indices for each of the variables assessed under this label.
Finally, no statistically significant differences in the PANSS scores were found for either total score or any of the five dimensions, reflecting a similar level of psychopathological severity in men and women.
Multivariate Stepwise Regression Models
Whole Sample
In the model with all the patients (Table 2), gender was the most important predictors of overall SF (i.e., LSP total score as a dependent variable) with a b coefficient of 6.59 in the final equation model, thus indicating that being a woman was related to better SF. In addition, as detailed above, women had significantly better LSP scores compared to men both for total SF score and all the sub-scores, except for NT (Table 1). In addition, PANSS disorganized and excited dimensions showed negative b coefficients. Age of onset also entered the model with a positive b coefficient.
Since our sample is not evenly composed of the same proportion of male and female, and gender is a critical variable influencing SF, we further explore SF using a stratification strategy. Hence, stepwise regression models were computed separately for men and women.
Regression Models for Men
Regression models for men are detailed in Table 3. The best-fit model for overall SF (i.e. LSP total score) included the ‘Positive’ and ‘Disorganized’ PANSS scores, both with negative b coefficients of similar magnitude. The model accounted for a 36.1% of the variance in SF, with ‘Positive’ symptoms contributing a 82% of the total variance. Neither demographic variables nor objective social variables entered the model.
The regression model for the LSP ‘Responsibility’ sub-score, also showed negative b coefficients for the ‘Disorganized’ PANSS score. In addition, the variables ‘Income’ and ‘Living situation’ had also negative b coefficients of higher magnitude than the ‘Disorganized’ PANSS variable that entered the model. On the other hand, ‘Education’ had a positive b score of similar magnitude than the other objective social variables. These four independent variables explained the highest amount of variance on any LSP score with a 39.2% the variance of the ‘Responsibility’ sub-score.
The regression models for the LSP sub-scores of ‘NT’ and ‘SC’ included ‘Age of onset’ in the model with a positive b score. Also, two psychopathology domains entered the model with a negative score: ‘Positive’ and ‘Disorganized’ in ‘NT’ model; ‘Positive’ and ‘Disorganized’ in ‘SC’ model. In both models the amount of variance that independent variables explained was similar, being around 29% of variance.
‘Communication’ and ‘Sociability’ models of SF in men exclusively included psychopathological variables. Specifically, ‘Negative’ PANSS score entered the model for ‘Communication’, while ‘Positive’ and ‘Disorganized’ PANSS scores entered the ‘SC’ model. All of them had negative b coefficients, and the models accounted for a similar amount of variance in the 28% vicinity.
Regression Models for Women
Regression models for women are detailed in Table 4. The best-fit model for overall SF (i.e. LSP total score) included ‘Disorganized’ PANSS and ‘Income’ variables. While ‘Disorganized’ variable entered the model with a negative b score, ‘Income’ variable entered the model with a positive b score. Both variables together accounted for a 30.8% of the variance in SF, being ‘Disorganized’ the variable that contributed the most part of the total variance with a 78%.
The regression model for the LSP sub-score of ‘Communication’ included the ‘Negative’ PANSS score and the ‘Age of onset’ variable in the model. Their b coefficients had and opposite sign: negative for the ‘Negative’ PANSS, and positive for ‘Age at onset’. The two variables accounted for the highest amount of variance in the regression models with a 35.6% of the variance of ‘Communication’.
On the other hand, the remainder four models for ‘Responsibility’, ‘NT’, ‘Sociability’, and ‘SC’ only included psychopathology variables. While ‘Positive’ PANSS score and ‘Disorganized’ PANSS score entered the model for ‘Responsibility’, and only the ‘Excited’ PANSS score entered the other three models. In these models, all independent variables but ‘Positive’ had a negative b score. The amount of variance explained was 26.1% in the ‘Responsibility’ mode. The remainder three models scarcely accounted for a variance around the 13% mark.
Discussion
Our results show that men and women with schizophrenia who live in the community differ in their profile of variables associated with SF. Although their symptomatic status is stable and they are responding to the treatment to be living in the community, the psychopathological variables still account for SF in both gender. On the other hand, objective social variables barely account for variance in SF.
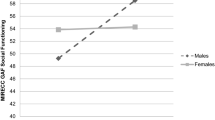
We expected that social variables would explain differences in SF in a sample living in the community. This finding may be related to challenges related to the nature of the objective variables. Objective social variables are facts about the social situation (e.g. marital status or income) that can be measured unequivocally. However, they are distal outcome measures, are less susceptible to change, have floor and ceiling effects, and are susceptible to cultural background differences [2]. Therefore, it may be methodologically challenging to relate social outcome with objective variables. Alternatively, it could be that certain psychopathological domains are exquisitely sensitive to SF performance, and even small changes have an impact. Considering even small changes on excitable, disorganized, or positive symptoms as a source of decline in SF seems a very intuitive and plausible explanation. Figure 1 visually summarizes gender-related differences in the profile of variables that account for SF impairment in our sample (i) the impact of positive symptoms on SF is mostly relevant for men, (ii) objective social variables only have some impact on SF in women and (iii) disorganized symptoms have a relevant impact on SF mostly in women.

Overall SF, diagram by gender. Dependent variable is represented by the larger bubble, independent variables that enter the model are represented within the larger bubble; dimension of the bubble are proportional to the amount of variance they explain. Variables not entering the model are represented on equal size out of the main bubbles
Our study replicates previous studies that showed that women do better in SF in spite of having a similar symptom severity [8, 11]. In this regard, several hypotheses have been proposed to explain gender differences in SF. While some authors highlight the protective role of estrogens [13] or disrupted normal sexual brain dimorphisms in men but not women [14], others focus on differential gender social expectations [23]. Another line of reasoning links women having a later age of onset with the fact that early age of onset is one of the most strongly associated factors with worse overall prognosis and functioning [24–27]. However, our results show that ‘Age of onset’ enters the models for ‘NT’ and ‘SC’ in men, and for ‘Communication’ in women. Thus pointing to an effect of age at onset on SF regardless of gender. Furthermore, Häfner and colleagues suggest that gender differences in SF are already apparent before onset, thus reducing the likelihood of those differences being a result of just an earlier age of disease onset [28]. Nevertheless, our study was not designed to explore the role of biological variables such as hormonal differences and, therefore, we are not able to rule out the possibility that age of onset is an intermediate variable reflecting the effect of other biological factors.
Slight differences in variable profile occurred regarding psychopathology as a function of gender. SF in men was affected by positive symptoms in overall performance and in three out of five domains: NT, socialization, and SC. On the other hand, for women, PANSS positive entered the model just for the domain of responsibility; more intriguingly, the b coefficient positively indicated that the higher the score in positive symptoms, the higher the score in SF. Beyond this particular counterintuitive relationship, which might be explained by the presence of a confounding effect by a third variable not included in the analyses, the observed trend shows that SF is affected by the presence of residual positive symptoms in men, but not so much in women. Given that both genders have an equal and stable level of positive symptoms, and these interfere with SF mostly in men, we hypothesize that coping strategies and/or service use differences might account for positive symptoms interfering more in men (i.e., either men cope less efficiently and/or do not use provided treatment services as much as women do), an idea that has support in the literature [29, 30].
Finally, it is noteworthy that, in contrast to what had been reported before by some authors, our results showed that neither mood nor negative symptoms play a significant role in explaining overall social impairment (i.e., LSP total) [31, 32]. This could be due to the fact that some of those previous studies, such as Aki et al. [33] for instance, used a three-domain scale and some aspects related to excited or disorganized symptoms could be taken into account under negative. In this regard, as Salokangas et al. [34] point out, we are of the view that a five dimension psychopathological scale sorts out meaningfully the psychopathological domains, showing that presence of either disorganized or excitatory symptoms impairs SF.
There are several limitations to this study. The sample consists of a middle aged community-dwelling cohort who were stable, and perhaps had lower psychopathology scores compared to inpatient groups of individuals. Therefore, the external validity and generalization of the results to a different groups age or an inpatient sample may be limited. In addition, the cross-sectional design of the study does not allow us to consider the models from a longitudinal perspective, thus limiting the study’s inferential capacity.
In addition, other variables might have been useful to explore in our study. According to Ochoa et al. [35, 36], the number of unmet needs is positively and highly correlated with symptom severity: the more unmet needs, the higher the psychopathological severity. Moreover, such a correlation is particularly strong with disorganized and excited symptoms. Thus, it would have been interesting to include this variable in our study.
Given that SF is the ultimate therapeutic target, it would be very exciting to explore whether different types of treatment are associated to better SF (e.g. intramuscular vs. oral antipsychotics, or typical vs. atypical antipsychotics). Indeed, there are increasing numbers of drug clinical trials that are starting to assess SF as the main outcome [37]. Furthermore, since our data not only shows that men and women have different SF impairments, but also that the impairment is related to a different set of variables, it would be interesting to see whether there is any relationship between SF and therapeutic response in women compared to men, a question that is under current scrutiny [38].
In summary, our findings indicate that in spite of being symptomatically stable, variations in critical psychopathological domains impair SF. Further, these critical psychopathological domains differ in men and women. While men’s SF is affected by positive symptoms, women’s SF is impaired by disorganized symptoms. Our study also shows that objective social variables may be too distal as an outcome measure or may have ceiling effects that make it difficult to capture change. Alternative intermediate variables may be considered in better predicting SF as an outcome variable [39, 40]. Finally, this study supports and furthers the notion that men and women with schizophrenia differ in the variables that impair their SF, thereby prompting for tailoring in treatment plans as a function of gender. Also, it has potential critical implications for measuring outcome in clinical trials.
References
Mueser K, Tarrier N: The Handbook of Social Functioning in Schizophrenia. Boston, Allyn & Bacon, 1998
Priebe S: Social outcomes in schizophrenia. British Journal of Psychiatry 191(suppl.50):s15–s20, 2007
Cohen AS, Dinzeo TJ, Nienow TM, et al.: Diminished emotionality and social functioning in schizophrenia. Journal of Nervous and Mental Disease 193(12):796–802, 2005
Halford WK, Hayes RL: Social skills in schizophrenia: Assessing the relationship between social skills, psychopathology and community functioning. Social Psychiatry and Psychiatric Epidemiology 30(1):14–19, 1995
Reeder C, Newton E, Frangou S, et al.: Which executive skills should we target to affect social functioning and symptom change? A study of a cognitive remediation therapy program. Schizophrenia Bulletin 30(1):87–100, 2004
Vetter P, Koller O: Clinical and psychosocial variables in different diagnostic groups: Their interrelationships and value as predictors of course and outcome during a 14-year follow-up. Psychopathology 29(3):159–168, 1996
Bowie CR, Reichenberg A, Patterson TL, et al.: Determinants of real-world functional performance in schizophrenia subjects: Correlations with cognition, functional capacity, and symptoms. American Journal of Psychiatry 163(3):418–425, 2006
Haro JM, Novick D, Suarez D, et al.: Predictors of the course of illness in outpatients with schizophrenia: A prospective three year study. Progress in Neuro-Psychopharmacology and Biological Psychiatry 32(5):1287–1292, 2008
Wiersma D, Wanderling J, Dragomirecka E, et al.: Social disability in schizophrenia: Its development and prediction over 15 years in incidence cohorts in six European centres. Psychological Medicine 30(5):1155–1167, 2000
Angermeyer MC, Goldstein JM, Kuehn L: Gender differences in schizophrenia: Rehospitalization and community survival. Psychological Medicine 19(2):365–382, 1989
Usall J, Haro JM, Ochoa S, et al.: Influence of gender on social outcome in schizophrenia. Acta Psychiatrica Scandinavica 106(5):337–342, 2002
Watt DC, Katz K, Shepherd M: The natural history of schizophrenia: A 5-year prospective follow-up of a representative sample of schizophrenics by means of a standardized clinical and social assessment. Psychological Medicine 13(3):663–670, 1983
Strous RD, Maayan R, Lapidus R, et al.: Increased circulatory dehydroepiandrosterone and dehydroepiandrosteronesulphate in first-episode schizophrenia: Relationship to gender, aggression and symptomatology. Schizophrenia Research 71(2–3):427–434, 2004
Walder DJ, Seidman LJ, Makris N, et al.: Neuroanatomic substrates of sex differences in language dysfunction in schizophrenia: A pilot study. Schizophrenia Research 90:295–301, 2007
Scholten MR, Aleman A, Kahn RS: The processing of emotional prosody and semantics in schizophrenia: Relationship to gender and IQ. Psychological Medicine 38(6):887–898, 2008
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 4th edn. Washington, DC, American Psychiatric Association, 1994
Rickham PP: Human Experimentation. Code of Ethics of the World Medical Association. Declaration of Helsinki. British Medical Journal 2(5402):177, 1964
Bulbena VA, Fernandez de Larrinoa PP, Dominguez Panchon AI: Spanish adaptation of the Life Skills Profile. Profile of activities of daily living. Structure and factorial composition. Actas Luso-Españolas de Neurologia, Psiquiatria y Ciencias Afines 20(2):51–60,1992
Rosen A, Hadzi-Pavlovic D, Parker G: The life skills profile: A measure assessing function and disability in schizophrenia. Schizophrenia Bulletin 15(2):325–337, 1989
Kay SR, Fiszbein A, Vital-Herne M, et al.: The positive and negative syndrome scale—Spanish adaptation. Journal of Nervous and Mental Disease 178(8):510–517, 1990
Peralta M, V, Cuesta Zorita MJ: Validation of positive and negative symptom scale (PANSS) in a sample of Spanish schizophrenic patients. Actas Luso-Españolas de Neurologia, Psiquiatria y Ciencias Afines 22(4):171–177, 1994
Kay SR, Sevy S: Piramidical model of schizophrenia. Schizophrenia Bulletin 16:537–544, 1990
Shirakawa I, Mari JJ, Chaves AC, et al.: Family expectation, social adjustment and gender differences in a sample of schizophrenic patients. Revista de Saude Publica 30(3):205–212, 1996
Angermeyer MC, Kuhn L: Gender differences in age at onset of schizophrenia. An overview. European Archives of Psychiatry and Neurological Sciences 237(6):351–364, 1988
Faraone SV, Chen WJ, Goldstein JM, et al.: Gender differences in age at onset of schizophrenia. British Journal of Psychiatry 164(5):625–629, 1994
Häfner H, Riecher-Rossler A, An der Heiden W, et al.: Generating and testing a causal explanation of the gender difference in age at first onset of schizophrenia. Psychological Medicine 23(4):925–940, 1993
An der Heiden W, Häfner H. The epidemiology of onset and course of schizophrenia. European Archives of Psychiatry and Clinical Neuroscience 250(6):292–303, 2000
Amminger GP, Resch F, Mutschlechner R, et al.: Premorbid adjustment and remission of positive symptoms in first-episode psychosis. European Child and Adolescent Psychiatry 6(4):212–218, 1997
Pezzimenti M, Haro JM, Ochoa S, et al.: Assessment of service use patterns in out-patients with schizophrenia: A Spanish study. Acta Psychiatrica Scandinavica 114(Suppl. 432):12–18, 2006
Morgan VA, Castle DJ, Jablensky AV: Do women express and experience psychosis differently from men? Epidemiological evidence from the Australian National Study of Low Prevalence (Psychotic) Disorders. Australian and New Zealand Journal of Psychiatry 42:74–82, 2008
Greenwood KE, Landau S, Wykes T: Negative symptoms and specific cognitive impairments as combined targets for improved functional outcome within cognitive remediation therapy. Schizophrenia Bulletin 31(4):910–921, 2005
Rocca P, Bellino S, Calvarese P, et al.: Depressive and negative symptoms in schizophrenia: Different effects on clinical features. Comprehensive Psychiatry 46(4):304–310, 2005
Aki H, Tomotake M, Kaneda Y, et al.: Subjective and objective quality of life, levels of life skills, and their clinical determinants in outpatients with schizophrenia. Psychiatry Research 158:19–25, 2008
Salokangas RK, Honkonen T, Stengård E, et al.: Symptom dimensions and their association with outcome and treatment setting in longterm schizophrenia. Results of the DSP project. Nordic Journal of Psychiatry 56(5):319–327, 2002
Ochoa S, Haro JM, Usall J, et al.: Needs and its relation to symptom dimensions in a sample of outpatients with schizophrenia. Schizophrenia Research 75(1):129–134, 2005
Ochoa S, Vilaplana M, Haro JM, et al.: Do needs, symptoms or disability of outpatients with schizophrenia influence family burden? Social Psychiatry and Psychiatric Epidemiology 43(8):612–618, 2008
Burns T, Patrick D: Social functioning as an outcome measure in schizophrenia studies. Acta Psychiatrica Scandinavica 116(6):403–418, 2007
Muller MJ, Regenbogen B, Sachse J, et al.: Gender aspects in the clinical treatment of schizophrenic inpatients with amisulpride: A therapeutic drug monitoring study. Pharmacopsychiatry 39(2):41–46, 2006
Leifker FR, Patterson TL, Heaton RK, et al.: Validating measures of real-world outcome: The results of the VALERO Expert Survey and RAND Panel. Schizophrenia Bulletin, 2009. Ahead of print. doi:10.1093/schbul/sbp044.
Bowie CR, Depp C, McGrath JA, et al.: Prediction of real-world functional disability in chronic mental disorders: A comparison of schizophrenia and bipolar disorder. The American Journal of Psychiatry, 2010. Ahead of print. doi:10.1176/appi.ajp.2010.09101406.
Acknowledgments
We are thankfully indebted to patients and families who participated in the study as well as mental health staff who assisted us in this study. This project has received the financial help of the Spanish Fondo de Investigaciones Sanitarias (FIS 97/1275) and the Spanish Health Services Research Network RIRAG (G03/061) (Red de Investigacion de Resultados Aplicados a la Gestion en Discapacidad y Salud Mental). This project is supported by CIBER Salud Mental (Instituto de Salud Carlos III).
Conflict of interest
None of the authors have any conflict of interest regarding the present research.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Vila-Rodriguez, F., Ochoa, S., Autonell, J. et al. Complex Interaction Between Symptoms, Social Factors, and Gender in Social Functioning in a Community-Dwelling Sample of Schizophrenia. Psychiatr Q 82, 261–274 (2011). https://doi.org/10.1007/s11126-011-9168-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11126-011-9168-0