
Abstract
Implementing social emotional learning (SEL) programs in school settings is a promising approach to promote critical social and emotional competencies for all students. However, there are several challenges to implementing manualized SEL programs in schools, including program cost, competing demands, and content that is predetermined and cannot be tailored to individual classroom needs. Identifying core components of evidence-based SEL programs may make it possible to develop more feasible approaches to implementing SEL in schools. The purpose of this study was to systematically identify the core components in evidence-based elementary school SEL programs, using the five interrelated sets of competencies identified by the Collaborative for Academic, Social, and Emotional Learning (CASEL) as an organizing framework. We present the components that were identified, and the rates at which each component was included in the sample of evidence-based SEL programs. The core components that occurred most frequently across programs were Social Skills (100% of programs), Identifying Others’ Feelings (100% of programs), Identifying One’s Own Feelings (92.3% of programs), and Behavioral Coping Skills/Relaxation (91.7% of programs). These findings illustrate the feasibility of systematically identifying core components from evidence-based SEL programs and suggest potential utility of developing and evaluating modularized SEL programs.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
The Core Components of Evidence-Based Social Emotional Learning Programs
Schools play an important role in the promotion of social and emotional competencies for all students. The implementation of universal social and emotional learning (SEL) programs in school settings is a promising approach to foster affective, cognitive, and behavioral skills among all children. The benefits of SEL curricula are well documented. Several recent meta-analyses indicate that universal SEL interventions are effective in improving a broad array of outcomes, including social skills (January et al. 2011), attitudes, behavior, and academic performance (Durlak et al. 2011; Sklad et al. 2012).
To assist in the broad dissemination of SEL curricula, The Collaborative for Academic, Social, and Emotional Learning (CASEL) published a framework for organizing SEL competencies and systematically identifying well-designed, evidence-based SEL programs. Given the abundance of SEL programs, the CASEL Guide aimed to assist educators in selecting carefully evaluated curricula with well-documented impact and efficacy on student outcomes. The guides published by CASEL provide a list of SEL programs that meet CASEL standards to be considered evidence based. For each program, the guide presents information about program design (e.g., target grade/age range, number of sessions per year) and implementation support as well as information about the evidence of effectiveness (e.g., sample characteristics, specific outcomes measured; CASEL 2013). Additionally, the CASEL framework organizes the skills targeted by SEL programs into five interrelated sets of competencies: self-awareness, self-management, social awareness, relationship skills, and responsible decision-making. Programs included in the CASEL Guide address all five of these competencies. However, the guide does not include additional information about how it was determined whether a competency was addressed, or which “core components” (i.e., the discrete skills taught within SEL curricula) compose these broad competencies.
Another recent effort aimed to provide schools and organizations with information about the content and features of popular SEL and character education programs to aid in program selection (Jones et al. 2017). This report classified programs by the percentage of program activities that target skills in five skill domains (i.e., cognitive regulation, emotional processes, interpersonal skills, character, and mindset), as well as by the instructional methods employed (e.g., didactic instruction, discussion, game). For each curriculum, a “program snapshot” provides information about the evidence of effectiveness, percentages of program activities targeting each of the five skill domains, percentages of program activities employing each teaching method, and information about program components (e.g., support for family engagement; Jones et al. 2017). This information was intended to facilitate schools’ selection and adoption of SEL programming by providing information on curricular content and program features relevant to decision making.
Given that there are more than 200 SEL programs (Hoffman 2009), the frameworks put forth by CASEL (2013) and Jones et al. (2017) are useful in that they organize programs according to their features and targets, thereby potentially helping administrators, teachers, and counselors select programs that are a good fit for the needs of their intended population. At the same time, selection of an SEL program is still a complex decision; in that, there are multiple programs that target each CASEL competency and much of the curricular content is similar across programs.
Following program selection, there are a host of barriers to SEL program adoption and implementation. Factors affecting implementation of school-based prevention programs have been organized in a three-level framework consisting of individual-level factors (e.g., intervention perceptions and attitudes), school-level factors (e.g., personnel expertise, alignment with school mission/policy), and macro-level factors (e.g., policies and financing; Domitrovich et al. 2008). At the school and macro levels, SEL programs may not be viewed as aligning with schools’ mission of academic achievement and may compete with achievement testing priorities (Forman et al. 2009). Also, there may be limited financial (Forman et al. 2009) and personnel (Mihalic and Irwin 2003) resources to support implementation. Indeed, costs of manualized SEL programs generally include materials and equipment, training, teacher time, and lost academic instructional time (Hunter et al. 2018). At the individual level, school counselors and teachers may view implementing lengthy SEL programs as outside of the scope of their role or may cite inadequate time in the day to implement such programs (Forman et al. 2009). Similar to mental health clinicians delivering a manualized intervention, teachers may not implement SEL programs in their entirety (e.g., stopping because the program is too lengthy or picking and choosing only sections they wish to implement) or may feel that certain program components are not relevant to their students (Waller and Turner 2016). Given these barriers, low-cost resources to teach SEL skills that can be applied flexibly and during brief periods of time are warranted.
The complexity of intervention selection and implementation is also well known in the related field of child and adolescent mental health services, where an alternate way of synthesizing research on effective treatments has been promoted. In contrast to an approach that organizes evidence for the use of specific treatment programs (e.g., Coping Cat for anxiety; Kendall 1994), the distillation approach (Chorpita and Daleiden 2009; Chorpita, Daleiden, & Weisz 2005) aggregates findings across studies to present the frequency of treatment components of evidence-based mental health interventions. These “common elements” (Chorpita, Becker, & Daleiden 2007; Garland et al. 2008) refer to discrete practices or skills (e.g., relaxation, problem solving) that comprise the evidence-based interventions. The distillation method and its resulting core components offer another way to represent the research literature on effective programs, and one that is complementary to program-based methods such as those put forth by CASEL (2013) and Jones et al. (2017). Although the common elements or “core components” approach is not a treatment design approach in its own right, in the children’s mental health field, the conceptualization of treatment programs in terms of their components has influenced the development of modular treatments implemented by research clinicians and community therapists (e.g., Chorpita et al. 2017; Kolko et al. 2009; Weisz et al. 2012). In contrast to standard manualized interventions whereby the treatment developers specify treatment content, as well as the sequencing and pacing of that content, modular interventions in which each module’s content is not dependent upon another module facilitates the selection, sequencing, and pacing of content that is tailored to the population and context. Evidence from randomized controlled trials has found superior outcomes for youth treated by community therapists using a modular treatment, compared to evidence-based manualized treatment (Weisz et al. 2012) and community-based implementation of multiple evidence-based practices (Chorpita et al. 2017).
There is also evidence that core components can be distilled from practices outside of traditional psychotherapy. For example, a recent study identified 24 common practice elements found in comprehensive interventions models and discrete practices delivered in early childhood classrooms targeting 3–5-year-old children who exhibit problem behavior (McLeod et al. 2017). The authors argue that this framework could be used for training teachers and the development of quality indicators (McLeod et al. 2017). Other recent work distills core components from health-related prevention programs for adolescents (Boustani et al. 2015).
Delineating the core components of evidence-based interventions may make it possible to empirically examine which core components are critical for program effectiveness, clarifying the mechanisms through which interventions operate (Embry and Biglan 2008). Furthermore, real-world implementation of evidence-based interventions includes significant variation in implementation fidelity, dosage, and quality, and often includes adaptations that differ from the empirically validated program (Dariotis et al. 2008; Durlak and DuPre 2008). It is also becoming increasingly clear that poor implementation results in decreased intervention effectiveness (Durlak and DuPre 2008). Given that implementation often varies by core component (e.g., Molloy et al. 2013), recent studies have examined the relationship between implementation of specific core components and outcomes of evidence-based interventions, including Positive Behavior Interventions and Supports (Molloy et al. 2013) and Responsive Classroom, an SEL program focused on teacher instructional practices (Abry et al. 2017). In order to examine the relationship between implementation of SEL core components and outcomes, it is first necessary to identify the specific core components addressed by evidence-based SEL programs, using a more granular delineation of core components than the five overarching CASEL competencies.
Additionally, parallel to the development of modular psychotherapies, the distillation of core components of SEL may enable the development and testing of modular SEL programs. Modular designs may be particularly attractive for SEL programs delivered in school settings, where resource constraints can make manualized evidence-based programs difficult to implement (Kininger et al. 2018). In particular, stand-alone modules could be implemented flexibly during brief periods of time (Lyon et al. 2014) and could be integrated within academic curricula, which would be likely to increase acceptability and feasibility of sustained implementation. While evaluations including feasibility and cost-benefit analyses are necessary, it is plausible that publicly available modular programs may, at least in part, address financial implementation barriers. Of course, it would be necessary to empirically test the acceptability, feasibility, and effectiveness of modular SEL programs, as has been done for modular psychotherapies (e.g., Chorpita et al. 2017), as the identification of core components alone does not indicate whether any particular component is necessary or sufficient for program effectiveness (Chorpita et al. 2007).
To date, little is known about how the common element approach can be applied to universal SEL programs within the CASEL framework. This is an important gap in the literature, given the benefits of SEL, the ubiquity of CASEL as an organizing framework for SEL programs, and the potential utility of core components in synthesizing the literature and enabling the testing of mechanisms of change. This paper describes the process of identifying the specific core components addressed in evidence-based elementary school SEL programs, using the five interrelated sets of overarching competencies identified by CASEL as an organizing framework. Identifying these core components at a more granular level than used by CASEL provides the foundation for the development of a flexible, modular approach to SEL, may enable the measurement of specific mechanisms of behavior change, and may inform training programs and quality indicators (McLeod et al. 2017). We identified a group of SEL programs for inclusion based on the CASEL standards. Through an iterative process, we then developed definitions of core components present in the programs, and systematically coded each program for the presence or absence of each element. Here, we describe the systematic coding process, and present the core components we identified in evidence-based elementary school SEL programs and the rates at which they were present.
Method
Program Selection
SEL programs were selected for inclusion in our analysis using the 2013 CASEL Guide for Elementary School grades, which identified evidence-based SEL programs using several criteria. The CASEL Guide classified a program as “SELect” (evidence-based) when it met the following criteria:
-
1)
Targets all five areas of CASEL competence,
-
2)
Provides opportunities to practice,
-
3)
Offers multi-year programming,
-
4)
Offers training and other implementation support,
-
5)
Has at least one evaluation study that included a comparison group and pre-post measures,
-
6)
Documents a positive impact on one of the four outcome domains (Academics, Reduce conduct problems, Reduce emotional distress, Increase positive social behavior).
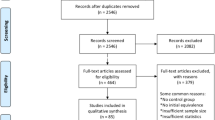
See CASEL (2013; www.casel.org/preschool-and-elementary-edition-casel-guide) for a complete description of the inclusion criteria. SEL programs were required to be qualified as a “CASEL SELect” program in order to meet criteria for inclusion in the current study; as such, all the programs in the study showed evidence of effectiveness from at least one evaluation study. Additionally, CASEL classifies programs as including “explicit skills instruction” in SEL skills, “teacher instructional practices,” or both. Because the goal of the current study was to identify the core components of SEL skills, programs were required to be classified as including explicit skills instruction, rather than solely consisting of teacher instructional practices, in order to qualify for inclusion in the study. A total number of 15 programs were reviewed, with 14 included in the study. One program, Competent Kids, Caring Communities, was excluded from the current study because we were not able to obtain enough information to meaningfully determine which components were included.
Coding Process
The components of SEL programs were coded using an iterative process that is consistent with the distillation work in other studies (e.g., Chorpita et al. 2005; Garland et al. 2008). We used CASEL as an organizing framework throughout this process. First, we examined the program manuals of seven SEL programs and generated a list of core components of each program, noting overlapping components. Each component was classified into the most closely related core competency (i.e., self-management, self-awareness, social awareness, relationship skills, responsible decision making), according to the definitions of these categories used by CASEL (CASEL; www.casel.org/preschool-and-elementary-edition-casel-guide).
We then used this information to iteratively develop a formalized coding manual, which provided definitions for 12 practices (e.g., “identifying one’s own feelings”), classified according to the CASEL categories (e.g., “self-awareness”). Practices were defined by a list of indicators for the presence of the code (e.g., “identify feelings based on face and body cues, and context” and “monitor intensity of feelings” were both indicators for “identifying one’s own feelings”). Table 1 shows the practices and indicators that were identified through the iterative coding process. The coding manual was refined as programs were coded; for example, definitions of practices and indicators were clarified to address issues that arose during the initial coding.
After developing the coding manual, two coders (authors GL and MM) independently coded each of the programs for the presence or absence of each common practice and sub-practice. Eleven programs were coded by both coders, with the final decision made by consensus in cases of disagreement. Three programs were coded by one of the two coders (GL), who made the final coding decision.
Consistent with published methods on distillation (e.g., Chorpita and Daleiden 2009), we obtained program manuals, which tend to contain more detailed information than published articles, for use in coding whenever possible. The full program manual was obtained for 10 of the programs. For these programs, the program manual was used as the only source of information to make coding decisions. When more than one program manual was available for a particular SEL program (e.g., manuals for multiple distinct grade levels), the manual for the grade that was closest to third grade was used.
For programs for which the full program manual was not obtained, information was gathered from the program website, published articles used by CASEL as program evaluation references for the program, and by requesting additional information from program developers.
We computed inter-rater reliability for the coding decisions at the practice level from the seven interventions that were independently coded by both coders. For 10 codes, kappas were above published standards (at least 0.40; Fleiss 1981). The kappa value was below published standards (i.e., < 0.40; Fleiss 1981) for one code (i.e., identifying other people’s feelings); however, the percent agreement for this code was 81.8%. Kappas could not be calculated for one code (i.e., social skills) due to the high base rate of this practice. For this practice, the raters showed 100% agreement.
Results
Program Selection
Fifteen SEL programs met inclusion criteria for the study: Second Step, Incredible Years–Incredible Teachers, PATHS, I Can Problem Solve, Social Decision Making/Social Problem Solving, MindUp, Michigan Model for Health, 4Rs, Competent Kids, Caring Communities, Open Circle, Positive Action, Raising Healthy Children, Resolving Conflict Creativity, Steps to Respect, and Too Good for Violence. Citations for the materials that were used to code each of these programs (e.g., manuals, journal articles) are included in Table 2.
Core Components Identified in SEL Programs
The 14 SEL programs were coded for the presence or absence of the identified core components. Four of the five CASEL competencies were addressed by all SEL programs, with the exception of Responsible Decision Making, which 85.71% of programs covered.
Results of the full coding are displayed in Table 3. The core components that occurred most frequently were Social Skills (100% of available programs), Identifying Others’ Feelings (100% of available programs), Behavioral Coping Skills/Relaxation (92.9% of available programs), and Identifying One’s Own Feelings (87.7% of available programs).
The core components that occurred least frequently were Mindfulness (20% of available programs), Valuing Diversity (63.6% of available programs), Cognitive Coping/Self-Talk (75% of available programs), and Goal Setting and Planning (75% of available programs).
Table 1 displays the percentage of SEL programs that addressed each indicator. Only the programs for which full manuals were available were coded at the indicator level, and the percentages given in Table 1 reflect these 10 programs. The Social Skills practice included the largest number of indicators, and programs varied widely in their inclusion of specific indicators. Frequently identified indicators were “listening when somebody is speaking to you” (80% of available programs) and “giving compliments” (60% of available programs). Less frequently identified indicators were “Asking for permission” (10% of available programs), “suggesting an idea” (10% of available programs), and “apologizing” (10% of available programs). Within the practices of Identifying Others’ Feelings, the most frequently identified indicators were “identifying feelings based on face and body cues and context” (100% of available programs). Within the practice of Behavioral Coping Skills/Relaxation, the most frequently identified indicators were “counting” (80% of available programs), “belly breathing” (70% of available programs), and “distraction-based behavioral coping skills” (60% of available programs).
Discussion
The current study demonstrates the feasibility of systematically identifying common core components from evidence-based elementary school SEL programs. Using an iterative process, we defined 12 core components and systematically identified which components were included in a set of 14 evidence-based SEL programs according to the CASEL Guide for Elementary School grades. There was considerable overlap in core components across programs. Seven of the components were identified in at least 10 of the 14 SEL programs, indicating that the majority of the components were present in the majority of the programs. The most frequently occurring components were social skills, feeling identification skills, and behavioral coping skills.
These results indicate that our sample of evidence-based elementary school SEL programs contain components across the five interrelated sets of competencies defined by CASEL (i.e., self-awareness, self-management, social awareness, relationship skills, and responsible decision making). There were similarities, as well as a number of distinctions, between the specific components distilled from the SEL programs and the competency definitions used by CASEL (2013). For example, the CASEL Guide defines the self-awareness competency as “the ability to accurately recognize one’s emotions and thoughts and their influence on behavior. This includes accurately assessing one’s strength sand limitations and possessing a well-grounded sense of confidence and optimism.” The distilled components emphasize the recognition of emotions and their influence on behavior, but do not represent identifying one’s strengths and limitations. Similarly, the components distilled for social awareness include perspective taking, but have less emphasis on recognizing “family, school, and community resources and supports” as defined by CASEL (2013). The coding process did not identify components that could not be classified in one of the five CASEL competencies, although it is possible that we would have identified components outside of these domains if we had included SEL programs outside those included in the CASEL Guide.
At the elementary school level, which was the scope of the current study, simple behavioral skills (e.g., listening, identifying feelings, behavioral coping skills) were most commonly represented, whereas more complex and cognitive skills (goal setting, cognitive coping skills, mindfulness) were included in SEL programs less consistently. It will be important for future studies to use a similar process to identify the common core components of secondary school SEL programs, as it is likely that the skills commonly included for this age group differ from those identified in the current study. Whereas the current study focused on the core components of explicit instruction in SEL skills, the majority of evidence-based high school SEL programs use teaching practices, rather than free-standing SEL lessons, to promote SEL (CASEL 2015). Examining the core components of teacher instructional practices to promote SEL at both the elementary and secondary levels remains an important topic for future research.
The current study should be considered in the context of some limitations. First, our sample of SEL programs was limited to those identified as evidence based in the 2013 CASEL Guide. As such, programs developed or evaluated in more recent years were not included in the sample, which may have prevented us from identifying components that have only been included in recently developed SEL programs. Furthermore, SEL programs in the CASEL Guide may have been inspired by existing, validated SEL programs; it is therefore possible that programs in our sample were not truly independent from each other, which may have led to an overestimation of the frequency of the identified practice elements. We also were unable to access the full manual for five SEL programs that met inclusion criteria. While we obtained enough information to report core components for four of these programs, these programs are incompletely captured, and the fact that an element was not identified in one of these programs does not necessarily indicate that it was not present. Notably, while the CASEL Guide required included programs to address all five interrelated competencies, the current coding found a small number of cases where a program was not coded as addressing any of the core components within a CASEL competency. This may be because the current set of core components were narrowly defined than the competencies used by CASEL, or because the current approach used different standards for determining whether a practice element was included. Additionally, one practice yielded a kappa value below published standards; it may therefore be important for future work to revise the codebook’s definition of this category. Nevertheless, we were able to identify a set of common core components from a diverse group of elementary school SEL programs, which represents an important step in understanding the content of evidence-based SEL programs, and provides a foundation for empirically examining which core components are critical for program effectiveness.
At a practical level, this study represents a first step in the process of developing a modular approach to SEL programs. Parallel to the evolution of modular approaches to evidence-based child and adolescent mental health treatments (e.g., Chorpita et al. 2005), all 14 core components identified across the varied manualized SEL programs could be combined into a single toolkit presenting teaching strategies for individual SEL skills. Rather than learning several different programs that have some distinct (e.g., mindfulness, valuing diversity) yet some overlapping skills (e.g., social skills), teachers would access one comprehensive resource. A modular approach to SEL may also facilitate teachers’ ability to tailor SEL to individual student need; for example, teachers might assess students’ SEL skills and then implement specific SEL modules to small groups of students with specific identified strengths and needs. Lessons could be implemented flexibly into busy school schedules, and might have the potential for integration into academic curricula. Intervention modules would also have the potential to be integrated within a school-wide multi-tiered system of support, either as classroom-wide interventions at tier 1 or as targeted interventions to students identified as in need of additional support at tier 2 (Stephan et al. 2015). Such an approach would require the use of data-based decision making, which could potentially include the direct assessment of SEL skills, an area of emerging research (e.g., McKown et al. 2016).
However, essential to the development of a modular SEL system is decision-making support to guide teacher decisions about the selection and ordering of skills. This study was a first step toward identifying the sample of skills in SEL programs, yet more work needs to be done to figure out how to coordinate their application in the classroom. In children’s mental health, the distillation and matching model (Chorpita et al. 2005; Chorpita and Daleiden 2009) lays out this logic. Specifically, distillation aims to identify the universe of skills (as we did in this study), but the matching part of the model offers ideas about what skills should be used with whom and for what purpose. Building a treatment simply by distilling manualized interventions into their components would not be an evidence-informed approach to intervention design and would introduce more potential problems into its delivery than would using manualized evidence-based interventions. Furthermore, just like with a manualized SEL programs (CASEL 2013), the successful implementation of a modular SEL program would require extensive implementation supports, including training, supervision, and monitoring of intervention integrity and outcomes. An additional focus on teacher instructional practices, which were not captured in the current distillation approach, may also be important.
Of course, it remains to be seen whether modular SEL programs are acceptable, feasible, and effective. Indeed, the issue of when and how to adapt evidence-based programs is an area of current research and debate (e.g., Castro and Yasui 2017). It is possible that the sequencing of SEL programs is important: Students may need to successfully master one skill (e.g., feelings identification) before they are prepared to learn another (e.g., cognitive coping skills). Furthermore, just as the components identified by evidence-based therapy protocols are not necessarily sufficient or necessary for clinical change (Chorpita et al. 2007), it is not correct to infer that the core components identified from evidence-based SEL programs are necessarily “evidence-based” in isolation. Similarly, we cannot infer that the core components that occur more frequently in evidence-based SEL programs are necessarily more effective than other core components. As such, as has been done with modular child psychotherapies, it will be important for future research to empirically study the effectiveness of modular SEL programs, as well as the acceptability, feasibility, and strategies needed to support the implementation of such programs.
References
*Reference used to code SEL program
Abry, T., Rimm-Kaufman, S. E., & Curby, T. W. (2017). Are all program elements created equal? Relations between specific social and emotional learning components and teacher–student classroom interaction quality. Prevention Science, 18, 193–203.
Boustani, M. M., Frazier, S. L., Becker, K. D., Bechor, M., Dinizulu, S. M., Hedemann, E. R., … Pasalich, D. S. (2015). Common elements of adolescent prevention programs: Minimizing burden while maximizing reach. Administration and Policy in Mental Health and Mental Health Services Research, 42, 209–219. https://doi.org/10.1007/s10488-014-0541-9.
*Brown, E. C., Low, S., Smith, B. H., & Haggerty, K. P. (2011). Outcomes from a school-randomized controlled trial of steps to respect: A bullying prevention program. School Psychology Review, 40, 423–443.
*Bruene Butler, L., Romasz-McDonald, T., & Elias, M. (2011). Social decision making/social problem solving: A curriculum for academic, social, and emotional learning. Champaign: Research Press.
Castro, F. G., & Yasui, M. (2017). Advances in EBI development for diverse populations: Towards a science of intervention adaptation. Prevention Science, 18, 623–629.
*Catalano, R. F., Mazza, J. J., Harachi, T. W., Abbott, R. D., Haggerty, K. P., & Fleming, C. B. (2003). Raising healthy children through enhancing social development in elementary school: Results after 1.5 years. Journal of School Psychology, 41, 143–164.
Chorpita, B. F., & Daleiden, E. L. (2009). Mapping evidence-based treatments for children and adolescents: Application of the distillation and matching model to 615 treatments from 322 randomized trials. Journal of Consulting and Clinical Psychology, 77, 566–579.
Chorpita, B., Daleiden, E., & Weisz, J. (2005). Identifying and selecting the common elements of evidence based interventions: A distillation and matching model. Mental Health Services Research, 7, 5–20. https://doi.org/10.1007/s11020-005-1962-6.
Chorpita, B. F., Becker, K. D., & Daleiden, E. L. (2007). Understanding the common elements of evidence-based practice. Journal of the American Academy of Child & Adolescent Psychiatry, 46, 647–652. https://doi.org/10.1097/chi.0b013e318033ff71.
Chorpita, B. F., Daleiden, E. L., Park, A. L., Ward, A. M., Levy, M. C., Cromley, T., … Krull, J. L. (2017). Child STEPs in California: A cluster randomized effectiveness trial comparing modular treatment with community implemented treatment for youth with anxiety, depression, conduct problems, or traumatic stress. Journal of Consulting and Clinical Psychology, 85, 13–25. https://doi.org/10.1037/ccp0000133.
Collaborative for Academic, Social, and Emotional Learning (CASEL). (2013). Effective Social and Emotional Learning Programs – Preschool and Elementary School Edition. Chicago: Author.
Collaborative for Academic, Social, and Emotional Learning (CASEL). (2015). Effective Social and Emotional Learning Programs – Middle and High School Edition. Chicago: Author.
*Committee for Children. (2011). Second step: Skills for social and academic success. Grade 3 teaching materials.
Dariotis, J. K., Bumbarger, B. K., Duncan, L. G., & Greenberg, M. T. (2008). How do implementation efforts relate to program adherence? Examining the role of organizational, implementer, and program factors. Journal of Community Psychology, 36, 744–760.
Domitrovich, C. E., Bradshaw, C. P., Poduska, J. M., Hoagwood, K., Buckley, J. A., Olin, S., et al. (2008). Maximizing the implementation quality of evidence-based preventive interventions in schools: A conceptual framework. Advances in School Mental Health Promotion, 1, 6–28. https://doi.org/10.1080/1754730X.2008.9715730.
Durlak, J. A., & DuPre, E. P. (2008). Implementation matters: A review of research on the influence of implementation on program outcomes and the factors affecting implementation. American Journal of Community Psychology, 41, 327–350. https://doi.org/10.1007/s10464-008-9165-0.
Durlak, J. A., Weissberg, R. P., Dymnicki, A. B., Taylor, R. D., & Schellinger, K. B. (2011). The impact of enhancing students’ social and emotional learning: A meta-analysis of school-based universal interventions: Social and emotional learning. Child Development, 82, 405–432. https://doi.org/10.1111/j.1467-8624.2010.01564.x.
Embry, D. D., & Biglan, A. (2008). Evidence-based kernels: Fundamental units of behavioral influence. Clinical Child and Family Psychology Review, 11, 75–113. https://doi.org/10.1007/s10567-008-0036-x.
Fleiss, J. (1981). Statistical methods for rates and proportions (2nd ed.pp. 38–46). New York: Wiley.
Forman, S. G., Olin, S. S., Hoagwood, K. E., Crowe, M., & Saka, N. (2009). Evidence-based interventions in schools: Developers’ views of implementation barriers and facilitators. School Mental Health, 1, 26–36. https://doi.org/10.1007/s12310-008-9002-5.
*Frey, K. S., Hirschstein, M. K., Snell, J. L., Edstrom, L. V. S., MacKenzie, E. P., & Broderick, C. J. (2005). Reducing playground bullying and supporting beliefs: An experimental trial of the steps to respect program. Developmental Psychology, 41, 479–490.
*Frey, K. S., Hirschstein, M. K., Edstrom, L. V., & Snell, J. L. (2009). Observed reductions in school bullying, nonbullying aggression, and destructive bystander behavior: A longitudinal evaluation. Journal of Educational Psychology, 101, 466–481. https://doi.org/10.1037/a0013839.
Garland, A. F., Hawley, K. M., Brookman-Frazee, L., & Hurlburt, M. S. (2008). Identifying common elements of evidence-based psychosocial treatments for children’s disruptive behavior problems. Journal of the American Academy of Child & Adolescent Psychiatry, 47, 505–514. https://doi.org/10.1097/CHI.0b013e31816765c2.
*Gerber Allred, C. (2016). Positive action: Grade 3 instructor’s manual. Twin Falls: Positive Action, Inc.
*Greenberg, M.T. & Kusche, C. (2011). PATHS: Promoting alternative thinking strategies grade 3. South Deerfield: Channing Bete Company, Inc.
*Haggerty, K. P., Fleming, C. B., Catalano, R. F., Harachi, T. W., & Abbott, R. D. (2006). Raising healthy children: Examining the impact of promoting healthy driving behavior within a social development intervention. Prevention Science, 7, 257–267. https://doi.org/10.1007/s11121-006-0033-6.
*Harachi, T. W., Abbott, R. D., Catalano, R. F., Haggerty, K. P., & Fleming, C. B. (1999). Opening the black box: Using process evaluation measures to assess implementation and theory building. American Journal of Community Psychology, 27, 711–731.
*Hirschstein, M. K., Edstrom, L. V. S., Frey, K. S., Snell, J. L., & MacKenzie, E. P. (2007). Walking the talk in bullying prevention: Teacher implementation variables related to initial impact of the steps to respect program. School Psychology Review, 36, 3–21.
Hoffman, D. M. (2009). Reflecting on social emotional learning: A critical perspective on trends in the United States. Review of Educational Research, 79, 533–556.
Hunter, L. J., DiPerna, J. C., Hart, S. C., & Crowley, M. (2018). At what cost? Examining the cost effectiveness of a universal social–emotional learning program. School Psychology Quarterly, 33, 147–154. https://doi.org/10.1037/spq0000232.
January, A., Casey, R. J., & Paulson, D. (2011). A Meta-analysis of classroom-wide interventions to build social skills: Do they work?. School Psychology Review. 40. 242-256.
Jones, S., Brush, K., Bailey, R., Brion-Meisels, G., McIntyre, J., Kahn, J., Nelson, B., & Stickle, L. (2017). Navigating SEL from the inside out: Looking inside & across 25 leading SEL programs--a practical resource for schools and OST providers. Cambridge: Harvard Graduate School of Education.
Kendall, P. C. (1994). Treating anxiety disorders in children: Results of a randomized clinical trial. Journal of Consulting and Clinical Psychology, 62, 100–110.
Kininger, R. L., O’Dell, S. M., & Schultz, B. K. (2018). The feasibility and effectiveness of school-based modular therapy: A systematic literature review. School Mental Health. https://doi.org/10.1007/s12310-018-9270-7.
Kolko, D. J., Dorn, L. D., Bukstein, O. G., Pardini, D., Holden, E. A., & Hart, J. (2009). Community vs. clinic-based modular treatment of children with early-onset ODD or CD: A clinical trial with 3-year follow-up. Journal of Abnormal Child Psychology, 37, 591–609.
*Linares, L. O., Rosbruch, N., Stern, M. B., Edwards, M. E., Walker, G., Abikoff, H. B., & Alvir, J. M. J. (2005). Developing cognitive-social-emotional competencies to enhance academic learning. Psychology in the Schools, 42, 405–417. https://doi.org/10.1002/pits.20066.
Lyon, A. R., Ludwig, K., Romano, E., Koltracht, J., Vander Stoep, A., & McCauley, E. (2014). Using modular psychotherapy in school mental health: Provider perspectives on intervention-setting fit. Journal of Clinical Child & Adolescent Psychology, 43, 890–901.
McKown, C., Russo-Ponsaran, N. M., Johnson, J. K., Russo, J., & Allen, A. (2016). Web-based assessment of children’s social-emotional comprehension. Journal of Psychoeducational Assessment, 34, 322–338. https://doi.org/10.1177/0734282915604564.
McLeod, B. D., Sutherland, K. S., Martinez, R. G., Conroy, M. A., Snyder, P. A., & Southam-Gerow, M. A. (2017). Identifying common practice elements to improve social, emotional, and behavioral outcomes of young children in early childhood classrooms. Prevention Science, 18, 204–213. https://doi.org/10.1007/s11121-016-0703-y.
*Michigan. Department of Education., Michigan. Department of Community Health, & Central Michigan University Educational Materials Center. (2016). Michigan Model for Health Grade 2 Curriculum. Holt: Michigan Model for Health Clearinghouse.
Mihalic, S. F., & Irwin, K. (2003). Blueprints for violence prevention: From research to real-world settings—Factors influencing the successful replication of model programs. Youth Violence and Juvenile Justice, 1, 307–329. https://doi.org/10.1177/1541204003255841.
Molloy, L. E., Moore, J. E., Trail, J., Van Epps, J. J., & Hopfer, S. (2013). Understanding real-world implementation quality and “active ingredients” of PBIS. Prevention Science, 14, 593–605. https://doi.org/10.1007/s11121-012-0343-9.
*Phillips, M. & Roderick, T. (2015). The 4Rs teaching guide 3: Reading, writing, respect & resolution. New York: Morningside Center for Teaching Social Responsibility.
*Ray, P., Alson, S., Lantieri, L., & Roderick, T. (2007). Resolving conflict creatively: A teaching guide for grades kindergarten through six. New York: Morningside Center for Teaching Social Responsibility.
*Shure, M. (2001). I can problem solve: An interpersonal cognitive problem-solving program. Kindergarten and primary grades, 2nd edn. Champaign: Research Press.
Sklad, M., Diekstra, R., Ritter, M. D., Ben, J., & Gravesteijn, C. (2012). Effectiveness of school-based universal social, emotional, and behavioral programs: Do they enhance students’ development in the area of skill, behavior, and adjustment? Psychology in the Schools, 49, 892–909. https://doi.org/10.1002/pits.21641.
Stephan, S. H., Sugai, G., Lever, N., & Connors, E. (2015). Strategies for integrating mental health into schools via a multi-tiered system of support. Child and Adolescent Psychiatric Clinics of North America, 24, 211–231. https://doi.org/10.1016/j.chc.2014.12.002.
*The Hawn Foundation. (2011). MindUP curriculum: Brain-focused strategies for learning—and living. Grades 3–5. New York: Scholastic Inc.
Waller, G., & Turner, H. (2016). Therapist drift redux: Why well-meaning clinicians fail to deliver evidence-based therapy, and how to get back on track. Behavior Research and Therapy, 77, 129–137. https://doi.org/10.1016/j.brat2015.12.005.
*Webster-Stratton, C. (2012). Incredible teachers: Nurturing children’s social, emotional, and academic competence. Seattle: Incredible Years, Inc.
Weisz, J. R., Chorpita, B. F., Palinkas, L. A., Schoenwald. S. K., Miranda, J, Bearman, S. K., ... & The Research Network on Youth Mental Health. (2012). Testing standard and modular designs for psychotherapy treating depression, anxiety, and conduct problems in youth: A randomized effectiveness trial. Archives of General Psychiatry, 69, 274. https://doi.org/10.1001/archgenpsychiatry.2011.147.
Funding
This project was completed with funding from Baltimore County Public Schools, Consultant Contract Agreement No. JNI-748-16-02 with the University of Maryland Baltimore, as part of their Project AWARE efforts funded by the Substance Abuse and Mental Health Services, U.S. Department of Health and Human Services. The work was partially supported by T32MH109433. Its contents are solely the responsibility of the authors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Research Involving Human Participants and/or Animals
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed Consent
For this type of study, formal consent is not required.
Rights and permissions
About this article

Cite this article
Lawson, G.M., McKenzie, M.E., Becker, K.D. et al. The Core Components of Evidence-Based Social Emotional Learning Programs. Prev Sci 20, 457–467 (2019). https://doi.org/10.1007/s11121-018-0953-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11121-018-0953-y