
Abstract
The aim of this study was to determine whether an intervention from the Triple P Positive Parenting Program system was effective in reducing parental reports of child behavioral difficulties in urban low-income settings in Panama City. A pilot parallel-group randomized controlled trial was carried out. A total of 108 parents of children 3 to 12 years old with some level of parent-rated behavioral difficulties were randomly assigned to a discussion group on “dealing with disobedience” or to a no intervention control. Blinded assessments were carried out prior to the intervention, 2 weeks, 3 months, and 6 months later. Results indicated that parental reports of child behavioral difficulties changed over time and decreased more steeply in the intervention than in the control group. The effects of the intervention on parental reports of behavioral difficulties were moderate at post-intervention and 3-month follow-up, and large at 6-month follow-up. Parents who participated in the discussion group reported fewer behavioral difficulties in their children after the intervention than those in the control condition. They also reported reduced parental stress and less use of dysfunctional parenting practices. There is a limited amount of evidence on the efficacy of parenting interventions in low-resource settings. This pilot trial was carried out using a small convenience sample living in low-income urban communities in Panama City, and therefore, the findings are of reduced generalizability to other settings. However, the methodology employed in this trial represents an example for future work in other low-resource settings.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
It is estimated that approximately 9.5 to 14.2 % of children worldwide present early onset behavioral problems (Brauner and Stephens 2006). Preventive interventions tackling risk and protective factors from an early stage are beneficial for the individual and for society as they have been associated with reductions in substance use (Fergusson et al. 2005), crime (Jakobsen et al. 2012) and mental health difficulties in adulthood (Fergusson et al. 2005). One of the most important modifiable risk factors contributing to the development of problems in children is the quality of parenting (Borkowski et al. 2009). Parenting interventions have been developed to provide support to parents and prevent difficulties in children (Biglan et al. 2012). Those derived from social learning and cognitive-behavioral principles are considered interventions of choice, and there are several meta-analyses documenting their effectiveness (e.g., Kaminski et al. 2008). However, most trials have been carried out in high-income, English-speaking settings, and there is limited evidence on their efficacy with other cultures and in low-resource settings. In two recent systematic reviews of parenting interventions in low- and middle-income countries (LMIC), only one study with a rigorous design was found (Knerr et al. 2013; Mejia et al. 2012). However, while low-resource settings are more readily encountered in LMICs, they are almost universally prevalent throughout the world.
Risk Factors for Children and Parents in Low-Resource Settings
Parents and children living in low-resource settings experience societal stressors such as poverty, urban violence, and limited access to health services which can place them at risk of difficulties (Walker et al. 2007). For example, it is well-established that poverty affects children’s health (Yoshikawa et al. 2012) through stress and other neurobiological, cognitive, and social-emotional processes (O’Connell et al. 2009). In addition, other factors that are usually associated with poverty, such as education and exposure to violence, also have an impact on children’s health (Shonkoff and Phillips 2000). These pathways are relevant in low-resource settings in Latin America. In a study in low-income neighborhoods in Brazil, a relationship between poverty, low educational level, and parenting violence was found (Pierantoni and Cabral 2009), while in a different study in low-income communities in Mexico, poverty and poor cognitive development in the child were mediated by parenting stress (Vera-Noriega et al. 2005).
Dissemination of Interventions Across Cultures: Adaptation Versus Fidelity
Improving the mental health of children worldwide through better access to interventions is a priority on global public health agendas (Patel et al. 2013). The Grand Challenges in Global Mental Health Initiative, a consortium of researchers and advocates around the world, have made an urgent call for cost-effective interventions to ensure sustainable implementation by public services (Collins et al. 2011).
A crucial question is whether existing interventions already trialed in high-income, English-speaking settings need to be culturally adapted to fit other cultures and low-resource settings or whether they can be delivered unadapted. On one side, some scholars advocate for adaptation before dissemination in order to increase recruitment, engagement, ecological validity, and successful implementation (Domenech-Rodriguez et al. 2011; Smith et al. 2011). There is empirical evidence suggesting that culturally adapted interventions are more effective than nonadapted ones (Griner and Smith 2006; Smith et al. 2011) and some authors have tested the efficacy of culturally adapted interventions (e.g., Coard et al. 2007) and have delineated the adaptation process (e.g., Parra-Cardona et al. 2009; Bernal and Domenech-Rodriguez 2012; Dumas et al. 2010). However, other scholars have pointed out that adapting interventions might compromise their efficacy, especially if the core components are modified (Elliot and Mihalic 2004; Chaffin et al. 2004; Gray et al. 2003). Their argument centers on the need for fidelity to original protocols in order to achieve effectiveness in different cultural settings (Chaffin et al. 2004).
Evidence seems to support the argument that fidelity to the core components of an intervention is important, but successful engagement of different cultures in low-resource settings can be promoted through carefully conducted adaptations. In other words, there appears to be a need for reaching a balance between adaptation and fidelity (Center for Substance Abuse Prevention [CSAP] 2001). Some researchers are working to identify the core components that make interventions work (Small and Huser 2012). Integrating these components in culturally adapted interventions might be a way forward as research shows that ethnic minorities are more receptive to core components of existing interventions if their cultural experiences are acknowledged (Kumpfer et al. 2008).
The Project in Panama
In 2009, the National Secretariat of Science in Panama (SENACYT) funded a project aiming to test the acceptability and efficacy of existing parenting programs. Panama is a relatively small country, with around 3.5 million people, mostly ethnically classified as Amerindians-Mestizos (68 %). About 32.7 % of the country’s population lives below the poverty line (World Bank [WB] 2012). A pressing concern in the country is violence (i.e., gang crime, child maltreatment), as currently, this is the second highest cause of mortality (Panamanian Ministry of Health 2012). The local government committed to identify evidence-based parenting programs after the United Nations Human Development Report stressed that Panama needed to invest in children in order to prevent violence (United Nations Development Program [UNDP] 2014). This project was supported by this initiative.
One of the interventions chosen for this project was a brief intervention from the Triple P Positive Parenting Program System (Sanders 2012). This brief Triple P intervention was chosen from a range of intervention packages by academics in Panama (SENACYT) in collaboration with academics from the UK because Triple P is a prevention-based approach with a substantial body of empirical evidence supporting its efficacy (Nowak and Heinrichs 2008) and positively reviewed by the United Nations Office on Drugs and Crime (2009). In 2011, two acceptability studies were carried out with 136 parents and 80 practitioners in low-income communities in Panama (Mejia et al. 2014a, b). Intention to participate and views on delivery formats were examined. Parents were presented with Triple P materials and a description of its strategies and theoretical foundations. They found the program acceptable and said that they would be willing to participate in a program like Triple P if one was offered, particularly favoring self-directed formats such as centers with materials on loan.
While parents favored self-directed formats in our acceptability study (Mejia et al. 2014a), a Triple P self-directed format could not be trialed at this stage, as one was not yet available in Spanish. A minimal and very brief face-to-face intervention with supporting materials for parents to use at home was therefore adopted. A pilot efficacy trial of one Triple P intervention (level 3 discussion groups on “dealing with disobedience”) was carried out, and findings on its efficacy are presented in this paper. It is important to note that most trials of Triple P only evaluate one level or format of the system. The system as a whole has rarely been trialed (e.g., Prinz et al. 2009).
The rationale for choosing a very brief single-session intervention from the Triple P system is justified on the basis of research showing that a significant number of parents with difficulties do not access parenting programs (Zubrick et al. 2005) and that a potential reason for this lack of engagement is the costs, both financial and time, involved in standard intensive interventions that last 8 to 24 sessions (Nixon 2002). These represent barriers both for parents and for services (Ensor and Cooper 2004). Brief targeted support for parents based on the principle of minimal sufficiency is therefore desirable. Minimal sufficiency denotes simplicity in designs and procedures as well as investment of the right amount of effort (Peterson 2009; Shapiro 2011). However, few studies (e.g., Faircloth and Cummings 2008) have examined the efficacy of brief targeted approaches for improving parenting, and their advantage over intensive interventions is still unknown.
Two trials of this very brief discussion group intervention from the Triple P system have previously been carried out in Australia showing effect sizes above d = 1.00 (Joachim et al. 2010; Morawska et al. 2011). For the present investigation, it was decided to firstly evaluate the intervention unadapted in a pilot study. This decision was based on previous experience in testing Triple P in other cultures. Two trials of a Level 4 Triple P intervention without adaptations, one in China and the other in Japan, suggested significant differences between intervention and control group in parental reports of child behavioral difficulties (d = .99 in Leung et al. (2006); d = .11 in Matsumoto et al. (2010)). Based on those findings, it was decided to use minimally adapted resources in this project (i.e., only language translations) to explore the setting, establish acceptability, and test for efficacy. The intervention was delivered as secondary level prevention, and only parents with some preexisting level of difficulties were eligible to take part in the trial. This study did not aim to test the superiority of minimally adapted interventions over more highly adapted ones but rather to establish a benchmark for the efficacy of a minimally adapted intervention (only language translations) in this low-resource setting. This can be considered as groundwork for future adaptation research. Given the research gap on the efficacy of parenting programs in low-resource settings, this study aimed to be a case example of a methodologically rigorous pilot randomized controlled trial (RCT). Its methodology could be replicated in other low-resource settings worldwide.
Methods
Trial Design
This was a parallel-group RCT with two groups: intervention (n = 54) and no intervention control (n = 54).
Participants
Parents were eligible if 1) they were 18 and over and if 2) they had a child between 3-12 years old with somelevel of behavioral difficulties as measured by the Eyberg Child Behavior Inventory (ECBI; Eyberg and Pincus 1999). Participants completed multiple questionnaires, and literacy assistance was beyond our resources. Therefore, illiteracy was an exclusion criterion. No participants were excluded on this criterion.
Participants were recruited between April 2012 and May 2012 in six state-owned (public) primary schools located in low-income communities in Panama City. Teachers selected parents of children with known behavioral difficulties to nominate for invitation to the study. These parents then undertook eligibility screening measures.
Intervention
Parents were randomized to either receiving a parenting intervention or to a no intervention control group. After baseline assessments, parents in the intervention group took part in a Triple P Level 3 discussion group entitled “dealing with disobedience,” a one-session, 2-h long group intervention, which combines group activities and practical exercises. The groups are interactive and discussion-based, and a PowerPoint presentation with embedded video clips is used to aid the facilitator. The key points covered in the discussion group include reasons for disobedience (based on social learning principles), parenting traps, encouraging good behavior, and managing disobedience. The three main strategies in which parents are trained are quiet time, time-out, and the use of behavioral charts. Parents also received a workbook that includes the content covered in the discussion group and two follow-up telephone calls to check how they were doing after the session. All videos and materials used the original video footage and did not reflect any situation or images particular to the Panamanian culture. Minimal adaptations in terms of language translation took place, but the content/protocol of the intervention was the same as the original Australian protocol. Materials were translated into Spanish by expert translators commissioned by Triple P International. In the videos, speech was presented in English and subtitles in Spanish. The facilitator (AM) was a native Spanish-speaker from Panama.
The intervention took place in classrooms in the community schools. Seven intervention groups were facilitated by the first author (AM) who is an accredited Triple P practitioner. Triple P international in Australia provided the facilitator with regular training, supervision, and support via Skype throughout delivery of the intervention in order to increase adherence to the protocol. Unfortunately, due to resource and language constraints (i.e., finding available assessors of fidelity who speak Spanish), no assessments could be completed to guarantee fidelity and ensure that the process and content of the intervention was followed.
Outcome Measures
Blind assessments took place at baseline (T1), post-intervention approximately 2 weeks after the discussion group (T2), and at follow-up 3 months (T3) and 6 months after (T4). Assessments were carried out by a research assistant who was blinded to group allocation and were conducted face-to-face in a classroom of the community school.
The assessment protocol was a series of self-reported questionnaires completed by parents in Spanish. The main outcome measure was the ECBI to assess parental reports of child behavioral difficulties. It consists of 36 items that assess problem behaviors reported by parents on two scales, the Intensity Scale and the Problem Scale. The Intensity Scale indicates frequency of problem behavior, while the Problem Scale assesses if the behavior is problematic or not for the parent. In this study, both scales showed high internal consistency, the Cronbach’s alpha (α) for the Intensity scale being .88 and the Problem scale .92.
Secondary outcome measures were the Depression-Anxiety-Stress Scale 21 (DASS-21; Lovibond and Lovibond 1995) to measure stress experienced by the parent and the Parenting Scale (PS; Arnold et al. 1993) to measure parenting practices. The DASS-21 is made up of three self-report subscales designed to measure the negative emotional states of depression, anxiety, and stress. In the present study, the Cronbach’s alpha of the total DASS-21 scale was α = .93. The PS is a 30-item questionnaire measuring dysfunctional discipline practices in three subscales: laxness (permissive discipline; 5 items), over-reactivity (authoritarian discipline; 5 items), and hostility (likelihood of parent using verbal or physical force; 3 items). It is also possible to calculate a total score of dysfunctional parenting using the 30 items. Parents respond on a seven-point scale to represent their behavior. Internal consistency was moderate for the total scale (α = .75).
Sample Size and Randomization
Using scores from the ECBI Intensity Scale from a previous trial of a Triple P discussion group (Morawska et al. 2011), it was determined that to have adequate power (80 %) to detect an effect size of d = .80, assuming an intra-cluster correlation coefficient for parenting groups of 0.05 and a 20 % loss to follow-up, the trial should have at least five discussion groups of 10 parents each and 50 no intervention control participants. Recruitment continued until this number was recruited and the final sample size was N = 108.
Only those above the mean score in the ECBI Intensity Scale (96 points) were eligible to take part in the study. This decision was taken to ensure that parents with some scope for change were included in the sample. The decision to use the mean rather than the clinical cutoff of the scale (i.e., 131 points) was made to obtain a sample with a range of levels of difficulty and not only parents of children in the clinical range. In order to ensure both groups had similar levels of difficulty, those above the cutoff point in the ECBI Intensity Scale (≥131) were randomized separately from those below (≤130).
An independent statistician generated a randomization list. In order to ensure allocation concealment, sequentially numbered, opaque, sealed envelopes (SNOSE) were opened by the PI after participants agreed to take part in the study and completed a baseline assessment. The PI was not blinded to allocation, as she was also facilitating the intervention.
Statistical Method
All analyses were conducted in SPSS v20. The analytic strategy consisted of a set of preliminary analyses to check whether randomization had produced comparable groups. We employed χ 2 analysis for categorical variables and t tests for continuous variables. To examine for differences between the groups in level of attrition, we used χ 2 and t tests to compare completers and noncompleters in baseline measures and socio-demographic variables.
Linear two-level mixed models (SPSS mixed) were fitted for each of the outcomes using an unstructured covariate structure including time as a second level (a repeated measure within subjects). Mixed models were fitted in order to determine the main effects attributed to between-group differences (i.e., intervention and control), time (treated as a categorical variable at baseline, post-intervention, 3 and 6 months), and the group-by-time interaction. A significant group effect suggests that there are differences at baseline between the intervention and control group. The time effect suggests a change over time in the outcome in the control group, while a significant group * time interaction suggests that the change over time in the intervention group is additional and above the change in the control group. Hence, the interaction is the test of the treatment effect. The models were adjusted for (1) baseline scores in the outcome, (2) the particular cluster or discussion group in which parents in the intervention group participated, and (3) socio-demographic variables (i.e., gender of child, age of child, and age of parent), which were all introduced as covariates.
Data were analyzed both per protocol and with an intention to treat method (ITT). The ITT was carried out using expectation maximization (EM) (Dempster et al. 1977). EM was carried out in SPSS v20 through a maximum likelihood procedure generating regression equations relating variables to ensure an accurate prediction of means, variances, and covariances and then estimating missing values.
Results
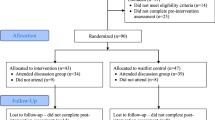
Figure 1 shows the flowchart of participants. Table 1 shows the socio-demographic characteristics of the sample. It is important to note that the majority of parents were women (86 %) and the majority of targeted children were boys (70 %).

Flowchart of participants in randomized controlled trial: intervention and no intervention control groups
Preliminary Analyses
t tests for continuous and χ 2 for categorical variables only revealed significant differences between groups at baseline in working status, χ 2 (4) = 10.071, p = .04, and in the ECBI Problem Scale, t (97) = −2.254, p = .02. Given this random dissimilarity between groups, we controlled for baseline scores in all the analyses.
A total of n = 54 were invited to the intervention and n = 46 attended (85.1 %). Seven discussion groups were conducted with an average size of 6.57 parents (SD = 2.69; range = 8.00). All parents completed the entire workshop (i.e., none leaved early) and only one parent per family attended in all of the cases.
An attrition analysis revealed no significant difference in dropout from the study by group, χ 2 (1) = 2.02, p = .15, with 35 (65 %) from the intervention group and 41 (76 %) from the control group completing the last follow-up. At T2, n = 14 (13 %) of the sample was lost, n = 6 (11 %) from the intervention group and n = 8 (14 %) from the control. At T3, n = 21 (19 %) was lost, n = 8 (15 %) from the intervention group and n = 13 (24 %) from the control group. At T4, n = 32 (30 %) of the sample was lost, n = 19 (35 %) from the intervention group and n = 13 (24 %) from the control. Reasons for dropout at T4 were work commitments (n = 12), change of contact details (n = 10), not being the primary caregiver any more (n = 3), child dropping out of school (n = 3), not wanting to stay in the study (n = 2), moving cities (n = 1), and health problems (n = 1). Student’s t tests suggested that completers had higher scores than noncompleters in the DASS-21 Anxiety Scale, t (106) = 2.06, p < .05, and in the PS Laxness Scale, t (105) = 3.68, p < .01 at baseline. Regarding socio-demographic characteristics, t tests for continuous variables and χ 2 for categorical variables suggested that children of those who completed the study were slightly younger (M = 8.13, SD = 1.86 for completers versus M = 9.35, SD = 1.40 for noncompleters; t (104) = −3.28, p < .01).
Primary Outcome Effects on Child Behavioral Difficulties (per protocol sample)
Table 2 presents the results from the per protocol analysis. The modeling tested whether the time and the group * time effect was significant, as this would indicate if the groups performed differently over time. There were significant time, F (1, 146) = 127.7, p < .001, and group * time effects, F (1, 146) = 38.5, p < .001, for the ECBI Intensity Scale (adjusting for baseline scores, child gender, child age, parent age, and cluster of discussion group) thus suggesting that parental report of child behavioral difficulties changed over time and that they were significantly lower in the intervention group than in the control group. The between-group effects of the intervention on parental report of child behavioral difficulties were d = .52, 95 % CI [−6.5, 7.6] at post-intervention, d = .42, 95 % CI [−7.9, 8.8] at 3 months follow-up, and d = 1.09, 95 % CI [−6.9, 9.1] at 6 months follow-up. This suggests that parents in the intervention group reported significantly less intense problems in their children than those in the control group at post-intervention, 3 and 6 months follow-up.
There were also significant time, F (1158) = 80.9, p < .001, and group * time effects, F (1, 158) = 25.6, p < .001, for the ECBI Problem Scale (adjusting for baseline scores, child gender, child age, parent age, and cluster of discussion groups). The between-group effects of the intervention on parental report of problematic child behaviors were d = .23, 95 % CI [−1.6, 2.0] at post-intervention, d = .51, 95 % CI [−1.5, 2.6] at 3 months follow-up, and d = .76, 95 % CI [−1.5, 3.0] at 6 months follow-up. This suggests that parents in the intervention group reported fewer problematic behaviors in their children than those in the control group at post-intervention, 3 and 6 months follow-up.
Secondary Outcome Effects (per Protocol Sample)
The modeling suggested that there were significant time, F (1, 135) = 10.1, p < .001, and group * time effects, F (1, 135) = 8.0, p < .001, for the DASS-21 Total Scale (adjusting for baseline scores, child gender, child age, parent age, and cluster of discussion group) thus suggesting that parental reports of stress changed over time and that it was significantly lower in the intervention than in the control group. The effects of the intervention on parental reports of stress were d = .32, 95 % CI [−2.2, 2.8] at post-intervention, d = .40, 95 % CI [−2.8, 3.6] at 3 months follow-up, and d = .61, 95 % CI [−2.8, 4.0] at 6 months follow-up. When analyzing each subscale, there were significant time and group * time effects for the Depression Scale, F (1, 139) = 7.9, p < .001 and F (1, 139) = 7.9, p < .001 respectively; for the Stress Scale, F (1, 144) = 14.8, p < .001 and F (1, 144) = 6.8, p = .01 respectively; and for the Anxiety Scale, F (1, 143) = 1.9, p = .01 and F (1, 143) = 5.5, p = .02 respectively. This suggests that those parents in the intervention group reported less stress, anxiety, and depression than those in the control group at post-intervention, 3 and 6 months.
There were also significant time, F (1, 171) = 40.1, p < .001, and group * time effects, F (1, 171) = 7.3, p < .001 for the PS Total Scale (adjusting for baseline scores, child gender, child age, parent age, and cluster of discussion group) thus suggesting that parental report of dysfunctional parenting practices changed over time and that they were significantly lower in the intervention group than in the control group. The effects of the intervention on parental report of dysfunctional parenting practices were d = .19, 95 % CI (.06, .3) at post-intervention, d = .15, 95 % CI (.01, .3) at 3 months follow-up, and d = .59, 95 % CI (.4, .7) at 6 months follow-up. When analyzing each subscale, there were significant time and group * time effects for the Hostility Scale, F (1, 165) = 11.9, p < .001 and F (1, 164) = 8.8, p < .001 respectively, suggesting that report of hostile parenting practices changed over time and that those in the intervention group reported significantly less use of these practices.
Intention-to-Treat Analysis
Effects of time and group * time (adjusting for baseline scores, child gender, child age, parent age, and cluster of discussion group) were significant for the ECBI Intensity Scale, F (1, 187) = 133.1, p < .001 and F (1, 187) = 23.8, p < .001 respectively; for the ECBI Problem Scale, F (1, 248) = 126, p < .001 and F (1, 248) = 17.7, p < .001 respectively; for the DASS-21 Total Scale, F (1, 148) = 11.3, p < .001 and F (1, 148) = 8.4, p < .001 respectively; and for the PS Total Scale, F (1, 204) = 41.8, p < .001 and F (1, 204) = 4.1, p = .04 respectively.
Discussion
International organizations have highlighted the need to increase access to evidence-based interventions that aim to strengthen families in low-resource settings (World Health Organization [WHO] 2009). Key to success is the identification of programs that are effective in these contexts and that fit cultural, social, and financial realities (Lund et al. 2011). The present study is a pilot RCT of one parenting intervention carried out in low-income communities in Panama and represents one of the few trials to report the use of a very brief, focused preventive parenting strategy in a low-resource setting. Results of this pilot trial indicated that for this sample, the intervention was effective in reducing parental reports of child behavioral difficulties. It is important to clarify that in this pilot study, the assessment of child behavioral difficulties relied solely on parental reports. Parents in the intervention group might have been more positive about their children than those in the control group, rather than their children actually exhibiting a change in behavior. Arguably, however, this is in itself a desirable change.
Changes in parental report of child behavioral difficulties were maintained over time. Strikingly, at 6-month follow-up, the effects were larger. However, effects that are distal from randomization itself should be interpreted with caution, as they are likely to be affected by sources of variance outside the research conditions. We designed a qualitative study to explore the mechanisms operating behind these large effects (Mejia et al. under review). Our qualitative data, collected through interviews with 25 parents, suggested that psychological processes enhanced by the program, such as an increase in parental self-confidence and problem-solving, might have prompted behavioral changes in both the parent and the child. To our knowledge, this is one of the first trials of such a brief parenting intervention, and explanations behind these large effects merit further exploration.
Our results are consistent with a trial of the same intervention from the Triple P system carried out in Australia in which effects on parental reports of child behavior were high at post-intervention (Morawska et al. 2011). The effects in the Australian study were larger than those found in the present trial; socio-demographic characteristics of the samples were however different (i.e., the Australian sample had higher SES level). Existing parenting interventions tend to show higher levels of change in higher income level samples (Lundahl et al. 2006). Future research should explore the kinds of adaptations needed in order to maximize effectiveness of interventions with low-income parents.
In this study, the Triple P parenting intervention also appeared to be effective in reducing parental reports of stress and dysfunctional parenting practices in the longer term. By analyzing subscales, the Parenting Scale allows for a deeper understanding of parenting practices by providing information on laxness, over-reactivity, and hostility. In our analysis, parental reports of hostility in the intervention group decreased significantly more so than in the control group. It is therefore possible to suggest that the effects found in parental reports of child behavior might be explained by a reduction in parental stress and hostile behaviors, which would be supported by the literature (e.g., Martorrel and Bugental 2006).
Limitations of the Study
Considering other limitations and as mentioned before, all outcome measures relied on parental report. Even though most published trials of parenting programs rely on parent-reported outcomes (e.g., Hiscock et al. 2008; Kim et al. 2008), future trials would benefit from incorporating different informants appropriate to the research question, for example, independent observations and teacher ratings when children attend school and have reported difficulties at baseline (e.g., Webster-Stratton et al. 2004). Second, it is important to note that while the size of the initial sample was adequate as suggested by power analysis, it remains a pilot trial. Thirdly, video material was not translated, and only subtitles were added. This might have been problematic for parents with low educational levels. This was a pragmatic decision given that this was a pilot trial with limited resources. In future research, it might be preferable to create videos that are ecologically valid if resources are available (e.g., Turner et al. 2007). A fourth limitation was the dropout rate at 6 months (30 %). t tests suggested that there were no significant differences at baseline between those who dropped out at this stage and those who did not, and our ITT analyses suggested that dropouts did not have a significant effect on the results. One of the reported reasons for drop out was parents having too many work commitments. Even though work-family conflict has been described as a worldwide difficulty (Kinnunen and Mauno 2008), it might be a particular challenge for parents living in poverty, and thus, alternatives for accessibility and engagement on interventions need to be explored (e.g., Haslam et al. 2013). Sixth, it is important to discuss the generalizability of findings in light of the exclusion criteria. There was a potential risk that parents might have been excluded due to literacy, although we did not need to do so. Even though most Panamanian adults are literate (94 % according to the WB, 2010), other low-resource settings might have high rates of illiteracy. For example, a study in several LMICs found that low parental educational level is associated with difficulties in children (Schell et al. 2007). This is a barrier that needs to be addressed in those contexts, for example by relying solely on visual material. Seventh, it was not possible to determine whether parents were taking part in any other parenting service. However, to our knowledge, no other parenting program was offered in the schools or communities in this study. Eighth, no assessments to guarantee adherence to the intervention protocol were completed. However, the facilitator was an accredited Triple P facilitator, and frequent supervision by Triple P International was provided. Future studies should include indicators to determine if the process and content of the intervention were followed. A final caveat is that one of the developers of Triple P was involved in this evaluation as a senior consultant thus introducing potential for bias. Nevertheless, two researchers outside the group who developed the intervention led the trial.
Directions for Future Research
An important issue to be raised is the debate between adapting evidence-based interventions versus delivering interventions in their original form with minimal adaptations such as translations (CSAP 2001). The trend forward in cross-cultural dissemination seems to be conducting careful adaptations that recognize cultural values and experiences while maintaining fidelity to the core components (Parra-Cardona et al. 2012). In this study, we aimed to test the efficacy of a minimally adapted protocol (i.e., only language translations), but there is the possibility that unmeasured adaptations, perhaps subtle, occurred in the delivery of the intervention simply based on pure indigenous knowledge of the Panamanian facilitator. Future studies should incorporate procedures for systematically measuring subtle or deep adaptation processes taken place throughout the trial.
Conclusion
A brief intervention from the Triple P system was trialed in Panama. Results suggested that this intervention was effective in reducing parental reports of child behavioral difficulties, parental stress, and ineffective parenting practices. Generalizability of findings to other settings cannot be assumed, given the unique social and cultural characteristics of the Panamanian communities where the trial took place. However, the methodology employed in this study provides an example for future work in other low-resource settings in light of the pressing need for increasing access to mental health services globally.
References
Arnold, D. S., O’Leary, S. G., Wolff, L., & Acker, M. M. (1993). The Parenting Scale: A measure of dysfunctional parenting in discipline situations. Psychological Assessment, 5, 137–144.
Bernal, G. A., & Domenech-Rodriguez, M. M. (2012). Cultural adaptations: Tools for evidence-based practice with diverse populations. APA Press.
Biglan, A., Flay, B. R., Embry, D. D., & Sandler, I. N. (2012). The critical role of nurturing environments for promoting human well-being. American Psychologist, 67, 257–271.
Borkowski, J. G., Landesman, S., & Bristol-Power, M. (Eds.). (2009). Parenting and the child’s world: Influences on academic, intellectual, and socio-emotional development. New Yersey: Taylos& Francis.
Brauner, C. B., & Stephens, C. B. (2006). Estimating the prevalence of early childhood serious emotional/behavioural disorders: Challenges and recommendations. Public Health Reports, 121, 303–310.
Center for Substance Abuse Prevention (CSAP). (2001). Finding the balance: Program Fidelity and adaptation in substance abuse. Rockville: SAMHSA, U.S. Department of Health and Human Services.
Chaffin, M., Silovsky, J. F., Funderburk, B., Valle, L. A., Brestan, E. V., Balachova, T., et al. (2004). Parent-child interaction therapy with physically abusive parents: Efficacy for reducing future abuse reports. Journal of Consulting and Clinical Psychology, 72, 500–510.
Coard, S. I., Foy-Watson, S., Zimmer, C., & Wallace, A. (2007). Considering culturally relevant parenting practices in intervention development and adaptation: A randomized controlled trial of the black parenting strengths and strategies (BPSS) program. The Counselling Psychologist, 35, 797–820.
Collins, P. Y., et al. (2011). Grand challenges in global mental health. Nature, 475, 27–30.
Dempster, A. P., Laird, N. M., & Rubin, D. B. (1977). Maximum likelihood from incomplete data via the EM algorithm. Journal Royal Statistical Society – Series B, 39, 1–38.
Domenech-Rodriguez, M. M., Baumann, A. A., & Schwartz, A. L. (2011). Cultural adaptation of an evidence based intervention: From theory to practice in a Latino/a community context. American Journal of Community Psychology, 47, 170–186.
Dumas, J. E., Arriaga, X., Moreland, A., & Longoria, Z. (2010). When will your program be available in Spanish? Adapting an early parenting intervention for Latino families. Cognitive and Behavioral Practice, 17, 176–187.
Elliot, D. S., & Mihalic, S. (2004). Issues in disseminating and replicating effective prevention programs. Prevention Science, 5, 47–53.
Ensor, T., & Cooper, S. (2004). Overcoming barriers to health service access: Influencing the demand side. Health Policy and Planning, 19, 69–79.
Eyberg, S. M., & Pincus, D. (1999). Eyberg child behaviour inventory and sutter-eyberg student behaviour inventory-revised: professional manual. Florida: Psychological Assessment Resources.
Faircloth, B., & Cummings, M. (2008). Evaluating a parent education program for preventing the negative effects of marital conflict. Journal of Applied Developmental Psychology, 29, 141–156.
Fergusson, D. M., Horwood, L. J., & Ridder, E. M. (2005). Show me the child at seven: The consequences of conduct problems in childhood for psychosocial functioning in adulthood. Journal of Child Psychology and Psychiatry, 46, 837–849.
Gray, D. O., Jakes, S. S., Emshoff, J., & Blakely, C. (2003). ESID, dissemination, and community psychology: A case of partial implementation? American Journal of Community Psychology, 32, 359–370.
Griner, D., & Smith, T. B. (2006). Culturally adapted mental health interventions: A meta-analytic review. Psychotherapy: Theory, Research, Practice & Training, 43, 531–548.
Haslam, D. M., Sanders, M. R., & Sofronoff, K. (2013). Reducing work and family conflict in teachers: a randomized controlled trial of Workplace Triple P. School Mental Health, 5, 70–82.
Hiscock, H., Bayer, J. K., Price, A., Ukoumunne, O. C., Rogers, S., & Wake, M. (2008). Universal parenting programme to prevent early childhood behavioural problems: Cluster randomized trial. British Medical Journal, 336, 318–321.
Jakobsen, I. S., Fergusson, D., & Horwood, D. (2012). Early conduct problems, school achievement and later crime: Findings from a 30-year longitudinal study. New Zealand Journal of Educational Studies, 47, 123–135.
Joachim, S., Sanders, M. R., & Turner, K. M. T. (2010). Reducing preschoolers’ disruptive behaviour in public with a brief parent discussion group. Child Psychiatry and Human Development, 41, 47–60.
Kaminski, J. W., Valle, L. A., Filene, J. H., & Boyle, C. L. (2008). A meta-analytic review of components associated with parent training program effectiveness. Journal of Abnormal Child Psychology, 36, 567–589.
Kim, E., Cain, K., & Webster-Stratton, C. (2008). The preliminary effect of a parenting program for Korean American mothers: A randomized controlled experimental study. International Journal of Nursing Studies, 9, 1261–1273.
Kinnunen, U., & Mauno, S. (2008). Work-family conflict in individuals’ lives: Prevalence, antecedents, and outcomes. In K. Näswall, J. Hellgren, & M. Sverke (Eds.), The Individual in the Changing Working Life (pp. 126–146). Cambridge: Cambridge University Press.
Knerr, W., Gardner, F., & Cluver, L. (2013). Improving positive parenting skills and reducing harsh and abusive parenting in low and middle income countries: A systematic review. Prevention Science, 14, 352–363.
Kumpfer, K. L., Pinyuchon, M., Teixeira, A., & Whiteside, H. O. (2008). Cultural adaptation process for international dissemination of the Stregthening Families Program. Evaluation and the Health Professions, 31, 226–239.
Leung, C., Sanders, M. R., Ip, F., & Lau, J. (2006). Implementation of Triple P Positive Parenting Program in Hong Kong: Predictors of program completion and clinical outcomes. Journal of Children’s Services, 1, 4–17.
Lovibond, S. H., & Lovibond, P. F. (1995). Manual for the Depression Anxiety Stress Scale (4th ed.). Sydney: NWS Families International Publishing.
Lund, C., De Silva, M., Plagerson, S., Cooper, S., Chisholm, D., Das, J., Knapp, M., & Patel, V. (2011). Poverty and mental disorders: Breaking the cycle in low-income and middle-income countries. The Lancet, 378, 1502–1514.
Lundahl, B. W., Nimer, J., & Parsons, B. (2006). Preventing child abuse: A meta-analysis of parent training programs. Research on Social Work Practice, 16, 251–262.
Martorrel, G. A., & Bugental, D. B. (2006). Maternal variations in stress reactivity: Implications for harsh parenting practices with very young children. Journal of Family Psychology, 20, 641–647.
Matsumoto, Y., Sofronoff, K., & Sanders, M. R. (2010). Investigation of the effectiveness and social validity of the Triple P Positive Parenting Program in Japanese society. Journal of Family Psychology, 24, 87–91.
Mejia, A., Calam, R., & Sanders, M. R. (2012). A review of parenting programs in developing countries: Opportunities and challenges for preventing emotional and behavioural difficulties in children. Clinical Child and Family Psychology Review, 15, 163–175.
Mejia, A., Calam, R., & Sanders, M. R. (2014a). Examining delivery preferences and cultural relevance of an evidence-based parenting program in a low-resource setting of Central America: Approaching parents as consumers. Journal of Child and Family Psychology. doi:10.1007/s10826-014-9911-x.
Mejia, A., Calam, R., & Sanders, M. R. (2014b). Dissemination of evidence-based parenting programs into low resource settings: Examining the views of practitioners. Journal of Child and Family Studies. doi:10.1007/s10826-014-0028-z.
Mejia, A., Ulph, F., & Calam, R. (under review). Exploration of child and parental changes after participation in a parenting intervention: A qualitative study in a low resource setting.
Morawska, A., Haslam, D., Milne, D., & Sanders, M. R. (2011). Evaluation of a brief parenting discussion group for parents of young children. Journal of Developmental and Behavioral Pediatrics, 32, 136–145.
Nixon, R. D. (2002). Treatment of behavior problems in preschoolers: A review of parent training programs. Clinical Psychology Review, 22, 525–546.
O’Connell, M. E., Boat, T., & Warner, K. (2009). Preventing Mental, Emotional, and Behavioral Disorders among Young People: Progress and Possibilities. Washington, DC: National Academy Press.
Parra-Cardona, J., Holtrop, K., Cordova, D., Escobar-Chew, A., Horsford, S., Tams, L., Villarruel, F. A., et al. (2009). “Queremosaprender”: Latino immigrants’ call to integrate cultural adaptation with best practice knowledge in a parenting intervention. Family Process, 48, 211–231.
Parra-Cardona, J. R., Domenech-Rodriguez, M., Forgatch, M., Sullivan, C., Bybee, D., Holtrop, K., Escobar-Chew, A., et al. (2012). Culturally adapting an evidence-based parenting intervention for Latino immigrants: The need to integrate fidelity and cultural relevance. Family Process, 51, 56–72.
Patel, V., Kieling, C., Maulik, P. K., & Divan, G. (2013). Improving access to care for children with mental disorders: A global perspective. Archives of Disease in Childhood, 98, 323–327.
Peterson, C. (2009). Minimally sufficient research. Perspectives on Psychological Science, 4, 7–9.
Pierantoni, L., & Cabral, I. E. (2009). Criançasemsituação de violência de um ambulatório do Rio de Janeiro: Conhecendoseuperfil. Escola Anna Nery, 13, 699–707.
Prinz, R. J., Sanders, M. R., Shapiro, C. J., Whitaker, D. J., & Lutzker, J. R. (2009). Population-based prevention of child maltreatment: The U.S. Triple P system population trial. Prevention Science, 10, 1–12.
Sanders, M. (2012). Development, evaluation, and multinational dissemination of the Triple P Positive Parenting Program. Annual Review of Clinical Psychology, 8, 345–379.
Schell, C. O., Reilly, M., Rosling, H., Peterson, S., & Ekstrom, A. M. (2007). Socioeconomic determinants of infant mortality: A worldwide study of 152 low-, middle-, and high-income countries. Scandinavian Journal of Public Health, 35, 288–297.
Shapiro, C. (2011). Taking a public health approach to parenting: Lessons on minimal sufficiency. Invited Plenary Address, presented at the Excellence in Child Mental Health Conference, December, Istanbul, Turkey.
Shonkoff, J. P., & Phillips, D. A. (2000). From neurons to neighborhoods: The science of early childhood development. Washington, DC: National Academy Press.
Small, S., & Huser, M. (2012). Family-based prevention programs. Encyclopaedia of Adolescence. Retrieved from: http://whatworks.uwex.edu/attachment/FamilyBasedPreventionProgramschapterdraft6-10-10.pdf
Smith, T., Domenech Rodriguez, M. M., & Bernal, G. (2011). Culture. Journal of Clinical Psychology, 67, 166–175.
Turner, K. M. T., Richards, M., & Sanders, M. (2007). Randomised clinical trial of a group parent education programme for Australian indigenous families. Journal of Paediatrics and Child Health, 43, 429–437.
United Nations Development Program [UNDP]. (2014). The future is now: Early childhood, youth and the formation of skills for life. National Human Development Report. Panama, UNDP.
United Nations Office on Drugs and Crime [UNODC]. (2009). Compilation of evidence-based family-skills training programs. Vienna: UNODC.
Vera-Noriega, J. A., Morales, D. K., & Vera-Noriega, C. (2005). Relación del desarrollocognitivo con el clima familiar y el estrés de la crianza. Psico-USF, 10, 161–168.
Walker, S. P., Wachs, T. D., Gardner, J., Lozoff, B., Wasserman, G. A., Pollitt, E., & Carter, J. A. (2007). Child development: Risk factors for adverse outcomes in developing countries. The Lancet, 369, 145–157.
Webster-Stratton, C., Reid, M. J., & Hammond, M. (2004). Treating children with early-onset conduct problems: Intervention outcomes for parent, child, and teacher training. Journal of Clinical Child and Adolescent Psychology, 33, 105–124.
World Bank [WB]. (2010). World Development Indicators Database.The World Bank.
World Bank [WB]. (2012). Panama Poverty Assessment: Priorities and Strategies for Poverty Reduction. Volume I, Main report. Human Development Department, The World Bank.
World Health Organization [WHO]. (2009). Preventing violence through the development of safe, stable and nurturing relationships between children and their parents and caregivers. Series of briefings on violence prevention: The evidence. Geneva: World Health Organization.
Yoshikawa, H., Aber, L., & Beardslee, W. R. (2012). The effects of poverty on the mental, emotional and behavioral health of children and youth. American Psychologist, 67, 272–284.
Zubrick, S. R., Ward, K. A., & Silburn, S. R. (2005). Prevention of child behavior problems through universal implementation of a group behavioral family intervention. Prevention Science, 6, 287–304.
Conflict of Interest
A Mejia is chair of the LMIC Triple P Research Network. She carried out this RCT as part of her PhD project at the University of Manchester. Triple P provided for free training and materials for the conduction of the study. R Calam has long-standing research collaborations with staff at the Parenting and Family Support Centre (PFSC), School of Psychology, University of Queensland (UQ). She has been a board member of the Triple P Research Network and is currently on the Triple P International Scientific Advisory Committee in a research capacity. The Parenting and Family Research Group at The University of Manchester and its members have no share in, ownership of, or formal relationship with Triple P International Pty Ltd and derive no funding or royalty from it. Triple P is owned by UQ. The University through its main technology transfer company, UniQuest Pty Ltd, has licensed Triple P International Pty Ltd to publish and disseminate the program worldwide. Royalties stemming from published Triple P resources are distributed to the PFSC, School of Psychology, Faculty of Health and Behavioral Sciences, and contributory authors. No author has any share or ownership in Triple P International Pty Ltd. MR Sanders is the founder and an author on various Triple P programs and a consultant to Triple P International.
Registration of trial
ClinicalTrials.gov, NCT0177106
Funding
The National Secretariat of Science and Technology in Panama (SENACYT) funded this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Mejia, A., Calam, R. & Sanders, M.R. A Pilot Randomized Controlled Trial of a Brief Parenting Intervention in Low-Resource Settings in Panama. Prev Sci 16, 707–717 (2015). https://doi.org/10.1007/s11121-015-0551-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11121-015-0551-1