
Abstract
Background
There is a need for research to evaluate the feasibility and efficacy of alternative delivery methods to make evidence-based parenting programs more accessible to parents of teenagers.
Objective
This study aimed to test the efficacy of a 2-h parenting discussion group for parents of adolescents experiencing family conflict. It was hypothesised that parents attending the discussion group would report reductions in family conflict and adolescent behavior problems and improvements in the parent–adolescent relationship and parenting in comparison to control parents.
Method
This study was a randomized controlled trial. Ninety parents of teenagers (11–16 years; M = 13.23 years) were randomly allocated to intervention (n = 43) or waitlist conditions (n = 47) and completed questionnaires of parent–adolescent and family conflict, adolescent behavior, the parent–adolescent relationship and parenting at pre- and post-intervention and 6-month follow up.
Results
At post-intervention, intervention parents reported greater declines in adolescent oppositional behavior problems in comparison to controls. No intervention effects were found for parent–adolescent or family conflict, or for the parent–adolescent relationship and parenting practices.
Conclusions
Brief parenting interventions may offer an alternative strategy for supporting parents to deal with challenging adolescent behavior, but further research is required to determine if this type of brief and targeted intervention is effective for family conflict. Such research is important given the need for effective and easily deployable prevention and intervention approaches that address a problem that has significant impact on adolescent wellbeing and family functioning.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Adolescence is often perceived as being characterized by high levels of parent–adolescent conflict (PAC) characterized by reciprocal disagreement, overt behavioral opposition, relationship dissatisfaction and/or mild bickering (Brković et al. 2014; Laursen et al. 1998). While it is true that families experience a peak in conflict around 14 years of age, it is typically minor in nature, and characterized by bickering over everyday issues (Allison and Schultz 2004; Laursen et al. 1998). Most families do not experience significant conflict or disruption to family relationships during adolescence (De Goede et al. 2009; Herrenkohl et al. 2009). When PAC is managed well, using constructive strategies such as problem-solving and compromise, family arguments and disagreements promote a successful transition to adulthood by teaching adolescents to negotiate and resolve conflict effectively (Smetana 2005). In turn, effective management of PAC can enhance family connectedness, facilitate adolescent autonomy and identity development (Smetana 2005; Zhao et al. 2015), and reduce the likelihood of adolescent internalizing and externalizing problems (Tucker et al. 2003).
However, around 5‒15% of families experience intense, long-term issues with PAC, which can have negative implications for adolescent wellbeing in the short- and long-term (Eisenberg et al. 2008). Unresolved, hostile PAC has been found to be a primary risk factor for a range of adverse adolescent outcomes, including externalizing (delinquency, conduct problems, aggression, poor peer relationships; Klahr et al. 2011; Trentacosta et al. 2011) and internalizing issues (depression, anxiety, low self-esteem; Weymouth and Buehler 2016). For families struggling to adapt to the developmental changes of adolescence, the negative impact of PAC on adolescent behavior and adjustment can strengthen over time (Weymouth and Buehler 2016), with the effect for adolescents worse when the parent–adolescent relationship is already problematic (Adams and Laursen 2007). Given this, programs that assist parents to understand and adapt to their child’s transition to adolescence and to effectively manage and reduce the impact of PAC should be key targets for the prevention and treatment of adolescent behavior problems.
The quality of the parent–adolescent relationship has been associated with a range of positive and negative adolescent outcomes, and is influenced by the presence and nature of conflict, with higher levels of conflict demonstrated to have detrimental effects on relationship connectedness (e.g., warmth and closeness; Moed et al. 2015). It is also likely that the association between the quality of the parent–adolescent relationship and parent–adolescent conflict is bidirectional such that when the relationship is characterized by low connectedness and/or higher levels of hostility (e.g., criticism, coercion) then higher levels of conflict are also likely (Kim 2006; Rohner et al. 2005). As such, the parent–adolescent relationship and approaches for dealing with PAC offer a potential target for intervention efforts that may prevent damaging forms of conflict during adolescence and strengthen the quality of the parent–adolescent relationship, thus benefiting the wellbeing of adolescents. Specifically, it is expected that when parents adopt effective communication and positive parenting approaches across the whole relationship, including dealing with conflict, escalation of discussions are less likely, leading to reduced intensity of conflict and fewer oppositional defiant behaviors of adolescents. Further, when parent–adolescent relationships are characterised by higher levels of warmth and connectedness, and lower levels of hostility, it is likely that there will be more willingness to compromise and cooperate in everyday interactions, particularly when problems arise.
There is substantial evidence that prevention and early intervention approaches involving structured parenting programs based on social learning and cognitive–behavior theory are effective for producing sustained reductions in child behavior problems (Dretzke et al. 2009; van Aar et al. 2017). To prevent problems of adolescence, the parenting field has primarily focused on working with parents of preadolescent children (Chu et al. 2012; Webster-Stratton and Taylor 2001). A small number of parenting programs specifically target the adolescent period, including the Teen Triple P-positive parenting program (Teen Triple P; Ralph and Sanders 2003), strengthening families program (Molgaard and Spoth 2001), nonviolent resistance training (Omer and Lebowitz 2016) and the ABCD parenting young adolescents program (Burke et al. 2012), as well as the multi-level, school-based family intervention, the family check-up (Stormshak and Dishion 2009). These programs have been shown to achieve positive outcomes for families and adolescents, including reductions in parent–adolescent conflict (Chu et al. 2015; Kumpfer et al. 2010; Salari et al. 2014) and reductions in adolescent behavior problems (Burke et al. 2012; Chu et al. 2015; Kumpfer et al. 2010; Omer and Lebowitz 2016; Stormshak and Dishion 2009).
Despite the efficacy of multi-session, sequentially-organized parenting programs, researchers and practitioners consistently report difficulties with low levels of engagement and retention of parents of adolescents. Research has reported retention rates as low as 20–35% and attrition rates between 40 and 60% (Baker et al. 2011; Dishion et al. 2002; Weinberger et al. 1990). Enrolment in a conventional parenting program typically involves an 8- to 12-session commitment from parents. Thus, low uptake and poor retention may be due to the time and organizational demands placed on parents related to organizing childcare, transport and managing competing family priorities (Kazdin and Wassell 1999). The investment of time, resources and funding to run conventional parenting programs may also be challenging for practitioners and agencies, especially when you consider the time required for training and supervision (O’Brien and Daley 2011), and may result in an agency declining to offer these programs. These challenges at both the parent- and practitioner-level limit the potential public health impact of evidence-based parenting interventions. Alternative approaches are needed to expand the reach, accessibility and availability of parenting programs (Tully and Hunt 2016).
Given these difficulties, parenting programs that adopt a brief or “light-touch” approach have been developed and tested to assess whether such a relatively small dosage of parenting support can be beneficial. In a recent systematic review, Tully and Hunt (2016) identified eight randomized controlled trials that assessed the efficacy of brief parenting interventions (defined as fewer than 8 sessions) targeting behavior problems among children aged 2–8 years. Across all trials, there were significant and sustained reductions in child disruptive behavior at post-intervention compared to the control group, and significant and sustained reductions in effective parenting in all but one of the trials. Most studies reported benefits for parents in terms of their parenting self-efficacy or satisfaction, while there were improvements in parent mental health in three of out of the six trials that assessed this outcome. Overall, the findings from this systematic review support a focus on brief parenting interventions as a possible solution to the challenge of parent engagement and retention.
Within the Triple P tiered system of intervention, there are five levels of intervention that increase in intensity from a universal positive parenting communication strategy (Level 1) to multi-session group and individual programs targeted at managing moderate to severe child behavior and family functioning problems (Levels 4 and 5; Sanders 2012). Level 3 comprises brief parenting interventions, including a series of 2-h discussion groups that target a specific child behavior problem or developmental issues (e.g., disobedience, fighting and aggression, self-esteem). The discussion groups are designed as a preventative or early intervention approach to childhood behavior problems within a tiered or stepped-care model, meaning that they should produce change in their own, but that a more intensive intervention can be offered for those who require more support. Further, like the other programs in the Triple P model, they are based on a social learning and cognitive–behavioral theoretical framework. Several trials have indicated that the discussion groups designed for parents of 2- to 12-year-old children produce sustained improvements at 6-month follow up in the behavior targeted by the group (e.g., disobedience, problems while shopping), as well as broader improvements in child behavior, parenting practices and parenting confidence, with effect sizes ranging from small to large (Dittman et al. 2016b; Joachim et al. 2010; Morawska et al. 2011; Palmer et al. 2019).
Consistent with the wider literature on parenting programs for parents of adolescents, trials assessing the efficacy of brief and light touch approaches to prevent or address problems of adolescence are scarce. One trial of a 2-h group offered universally to interested parents of adolescents produced increases in observed positive family interactions and a marginally significant improvement in parent involvement (Lim et al. 2005), while an uncontrolled evaluation of a three-part seminar series on parenting teenagers (approximately 4 h contact time) found that attendance at the seminars was associated with reductions in ineffective parenting and PAC (Chand et al. 2013). While these findings are promising, further research employing randomized controlled trial methodology is needed to explore the effectiveness of brief parenting support for adolescent-related issues, such as PAC. Such research is important in ensuring the effectiveness of a population-based or stepped-care model of parenting support; low intensity interventions should produce equivalent outcomes to more intensive intervention for at least a proportion of participants (Bower and Gilbody 2005).
A series of discussion groups have also been developed within the parallel Teen Triple P system, which is designed for parents of adolescents aged 12–16 years (Ralph and Sanders 2003). This study was a trial of the ‘Reducing Family Conflict’ discussion group (Ralph and Sanders 2013), which is an existing intervention developed by the authors of the original suite of Teen Triple P programs. The single, 2-h session addresses factors associated with PAC and provides strategies for preventing and managing disagreements and conflict within families. Based on the findings from trials of the discussion groups for younger children, it was predicted that, compared to a waitlist-control condition, parents in the intervention condition would report improvements at post-intervention in (1) family conflict generally and PAC specifically; (2) adolescent oppositional behavior problems; (3) the parent–adolescent relationship (i.e., increased connectedness and decreased hostility); and (4) parenting practices (i.e., increased use of positive parenting and decreased inconsistent discipline). It was hypothesized that (5) intervention gains would be maintained at 6-month follow up.
Method
Participants and Recruitment
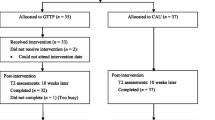
Participants were 90 parents of adolescents (aged 11–16 years) living in the metropolitan city of Brisbane, Australia (population of 2.4 million) who responded to a media-based or online advertisement about a 2-h discussion group on reducing family conflict. Parents were eligible if they had an adolescent in the target age range and indicated concern about the level of conflict with that child. Table 1 provides demographic characteristics broken down by intervention condition and Fig. 1 shows participant flow through the study.

Participant flow through the study
Parent age ranged from 28 to 61 years (M = 46.00; SD = 6.29) and most (81%) were the mothers of the target adolescent. Note that there were two younger female caregivers in the sample; one was a 28-year-old who was the older sister and legal guardian of her identified adolescent, and the other was a 32-year-old stepmother. The age range without these participants was 35–61 years. Most parents were married (74%), born in Australia (70%), and well-educated (64% had completed university studies). Fifty-two percent of parents reported family incomes over $95,000 AUD per annum and 11% below $40,000 AUD per annum.Footnote 1 The mean age of target adolescents was 13.23 years (SD = 1.51) with approximately equal proportions of girls (53%) and boys (47%).
Elevated scores on outcome measures were defined as being more than 1SD above the published mean on that measure, which was interpreted as an early marker for prevention or early intervention efforts. This criterion was adopted based on recommendations from Jacobson and Truax (1991) and Kendall and Sheldrick (2000) that, in the absence of established norms, a “normal” population could be defined as being within 2SD of the mean for that population. Based on parent-report, 38% of adolescents scored 1SD above the published mean on the oppositional defiant behavior subscale of the adolescent functioning scale (see below) at T1 suggesting some elevation in oppositional behavior compared to the normative sample. In comparison, 76% of parents reported elevation of levels of PAC, based on a T1 score 1SD above the mean on the conflict behavior questionnaire (see below).
Measures
Alpha reliabilities reported below are based on the present sample.
Family Background Information
Demographic information collected at pre-intervention included parent and adolescent’s gender and age, parental marital status, employment details and education, and family composition and financial status.
Family Conflict
Two established measures were used to assess family conflict. The 9-item conflict subscale (α = .78) from the family environment scale (FES; Moos and Moos 1994) assessed overall family conflict via items such as “Family members often criticise each other” and “Family members sometimes hit each other”. The 20-item conflict behavior questionnaire (CBQ; Robin and Foster 1989) assessed conflict in the parent–adolescent relationship (α = .93 for the total score) via items such as “We almost never seem to agree” and “My teenager and I compromise during arguments”. Both scales asked parents to rate whether each item was true or false.
Adolescent Behavior Problems
Two scales were used to assess adolescent problem behavior. The 12-item oppositional defiant behavior subscale (α = .91) of the adolescent functioning scale (AFS; Dittman et al. 2016a) assessed general conduct behavior problems (e.g., defiance and rudeness, irritability, temper outbursts, arguing and fighting such as “rudely answers back to me”); and the 10-item interpersonal relations subscale (α = .78) of the youth outcome questionnaire (Y-OQ; Burlingame et al. 2001), which assessed problem behaviors specific to relationships with others (e.g., aggressiveness, arguing, such as “gets into physical fights with peers or family”). Items on the AFS were rated on a scale from 0 (not at all true) to 5 (always true). Y-OQ items were rated from 0 (never or almost never) to 4 (almost always or always), but the subscale has a score range from − 6 to 34 as 3 items on the scale are negatively scored to tap positive behaviors.
Parenting and the Parent–Adolescent Relationship
The 42-item Alabama parenting questionnaire (APQ; Shelton et al. 1996) was used to assess effective and ineffective parenting practices. Three subscales were used in this study based on the factor structure recommended by Zlomke et al. (2013) for use with parents of adolescents. Specifically, the subscales were the 17-item positive and involved parenting subscale (α = .81; e.g., “You compliment your child when he/she does something well”); the 7-item discipline practicesFootnote 2 subscale (α = .60) and the 8-item discipline processes subscale (α = .78). The discipline practices subscale contains items assessing both effective (e.g., “You take away privileges or money as a punishment”) and ineffective (“You slap you child when he/she has done something wrong”) strategies for managing problem behavior, while the discipline process subscale assesses parents’ consistent and predictable application of parenting strategies (e.g., “You threaten to punish your child and then do not actually punish him/her”). The positive and involved parenting subscale was scored so that higher score reflected more adaptive parenting, while the discipline practices and discipline process subscales were scored so that higher score represented more ineffective parenting. Parents indicated how often they typically used each parenting practice from 1 (never) to 5 (always).
Quality of the parent–adolescent relationship was assessed using the 10-item connectedness (α = .91) and 5-item hostility (α = .6) subscales from the 20-item parent–adolescent relationship scale (PARS; Burke et al. 2017). The connectedness subscale assessed positive aspects of the parent–adolescent relationship including warmth, acceptance and emotional support via items such as “I comfort my teenager when he/she is upset”, while the hostility subscale assessed negative aspects, including criticism and complaining via items such as “I think my teenage needs to change his/her attitude”. Parents rated each item on a scale from 0 (not at all true) to 5 (always true).
Design and Procedure
The study was a 2 (condition: intervention vs. waitlist) × 3 [time: pre-intervention (T1), post-intervention (T2), 6-month follow up (T3)], randomized controlled trial. Ethical approval was obtained from the authors’ University Human Research Ethics committee and informed parental consent was obtained.
Eligibility for the study was assessed during an intake call, during which general information about the study and its requirements was also provided. As the discussion group has a preventative focus, parents were not eligible for the study if the target adolescent had a developmental or intellectual disability or chronic illness, if the parent or the adolescent were receiving psychological or psychiatric support for the adolescent’s behavior or adjustment, or if the parent could not read a newspaper without assistance. Parents who were not eligible were provided with contacts of alternative, free or low-cost community support services. Depending on their preference, eligible parents were sent personal log-in details to complete their pre-intervention assessments (T1) assessment and consent process online or were sent hard copies of these materials to be returned in a stamped and addressed envelope.
Randomization to condition occurred following the completion of pre-intervention assessments (T1) by one parent, who self-nominated as the primary caregiver of the target adolescent. Randomisation was conducted by an individual independent of the study using the generation of random integers via an online randomizer tool (www.random.org). Intervention parents were allocated to the next available and most convenient discussion group. Both parents in two-parent families were invited to attend the discussion group, and in single-parent families, parents were invited to bring a support person. Only one person in the family completed the assessments. Intervention parents completed T2 assessments 2–4 weeks following completion of the discussion group, and T3 assessments 6 months after T2. Waitlist participants completed T2 assessments 6 weeks after T1 and prior to attending the discussion group.
Reducing Family Conflict (RFC) Discussion Group (Ralph and Sanders 2013)
The RFC discussion group is a one-off, 2-h preventatively oriented session that encourages active parent participation. The discussion group is manualized and uses principles and strategies from the content of the Teen Triple P program (Sanders and Ralph 2002), which is based on social learning and cognitive–behavioral principles. Video footage that is briefer than the original Teen Triple P programs and targeted at the issue of family conflict is used to introduce parents to possible contributions to conflict in their family, as well as to introduce and demonstrate positive parenting strategies to prevent (e.g., family meetings, problem-solving, reinforcement of cooperation and desirable behavior) and manage family conflict (e.g., supporting adolescent emotional self-regulation, using consistent, assertive discipline). Didactic presentation, interactive exercises and group discussion is used to encourage parents to identify the factors influencing conflict in their family, including their role in the issue, and to facilitate parents’ understanding of the strategies and their implementation. Parents are encouraged to set goals about the strategies they will use at home, and to generalize the strategies to other children and family issues. Parents received a workbook with a summary of program content that could be used to record their responses to activities and to share content with parents and caregivers unable to attend the session.
Groups, ranging in size from 3 to 12 parents, were facilitated by the authors who are all PhD-trained registered psychologists who had completed the training and accreditation requirements to deliver all Teen Triple P discussion groups, including RFC. The second and third authors each have over 20 years’ experience working with parents of adolescents, while the first author has approximately 5 years’ experience. Facilitators recorded their adherence to the manualized program using session checklists, which showed that there was full adherence to the protocol across all groups.
Statistical Analyses
Expectation–Maximization (EM) was used to estimate missing data (Tabachnick and Fidell 2007). Independent groups t-tests and Chi square analyses on all sociodemographic and baseline variables assessed the effectiveness of randomization and checked for any systematic biases in participant attrition. An intent-to-treat approach was used to assess the short-term effects of the intervention. Multivariate analyses of covariance (MANCOVAs) were conducted on sets of related dependent (T2) variables: family and parent–adolescent conflict (FES conflict, CBQ); adolescent oppositional behavior (AFS oppositional behavior, Y-OQ interpersonal relations); parent–adolescent relationship (PARS hostility and connectedness); and parenting practices (APQ positive and involved parenting, discipline practices and discipline process subscales), controlling for T1 effects of the relevant baseline variable. Where multivariate effects were found, univariate F values were examined to determine which variables contributed to the multivariate effect. The level of clinically-significant change from pre- to post-intervention was evaluated using (a) effect sizes (Cohen’s d; Cohen 1988) and (b) Chi square tests of the extent to which statistically significant improvements were reliable (i.e., change that was statistically significantly greater than a difference that could have occurred due to random measurement error) through calculation of a reliable change index (Jacobson and Truax 1991) for those variables showing significant post-intervention effects. Finally, since the waitlist did not complete follow-up assessments, long-term effects were examined for Intervention only using repeated measures MANOVAs to assess gains from T1 to T3. A per protocol approach (i.e., completers analysis) was used because only 18 (42%) of the original 43 intervention parents completed T3.
Results
Preliminary Analyses
The EM method was used to estimate missing data since there was minimal missing item-level data (i.e., due to missed items within questionnaires) at each time point (< 5% within each questionnaire). Missing values analyses using Little’s criterion (Little 1988) indicated data were missing completely at random. Group comparisons to check adequacy of randomization revealed significant differences between intervention and waitlist on PARS hostility (t(88) = 2.24, p = .028) and YOQ interpersonal relations (t(88) = 2.87, p = .005), with waitlist parents reporting lower levels of hostility and adolescent behavior problems related to others (see Table 2 for T1 means and SDs). These unequal baseline scores were addressed by using MANCOVAs to assess intervention effects, in which T1 levels of all relevant variables were controlled. There were also a greater number of male target adolescents in the Intervention compared to the waitlist, χ2 = 64.35, p = .037.
Participant flow through the intervention is described in Fig. 1. Of the 43 parents assigned to the intervention condition, 34 attended the discussion group (79%), and 29 (67%) completed post-intervention assessments. Eighteen of the original 43 intervention parents (42%) completed T3. In comparisons between those that completed T2 and those that did not, non-completers were more likely to have not completed secondary school (18% vs. 6%) and have a trade or technical college qualification (36% vs. 12%) than completers. There was a trend towards non-completers reporting higher levels of positive and involved parenting practices (M = 66.83, SD = 8.36) than completers (M = 63.35, SD = 7.23; t(88) = 1.89, p = .062). When comparing participants in the Intervention condition who completed T3 to those that did not, non-completers were more likely to have part-time contact with their adolescent (20% vs. 0%), There were no other significant differences in demographic or baseline characteristics between conditions or between completers and non-completers across time points.
Short-Term Intervention Effects
Table 2 presents T1 and T2 means and SDs for each condition, univariate F values and effect sizes. The multivariate condition effect found for adolescent behavior problems was marginally significant, F(2, 85) = 2.92, p = .059. Given this trend toward significance, the univariate effects for AFS oppositional defiant behavior and Y-OQ interpersonal relations scales were interpreted. The condition effect for Y-OQ interpersonal relations was significant (p = .019), and the condition effect for AFS oppositional behavior was close to significant (p = .053), indicating that intervention parents reported significantly greater improvements in adolescent problem behavior than Waitlist parents at post-intervention (medium effect). No multivariate condition effects were found for conflict (F(2, 85) < 1.00, p = .530), the parent–adolescent relationship (F(2, 85) < 1.00, p = .524), or parenting practices, F(2, 83) = < 1.00, p = .496.
With regard to reliable change, more intervention parents (23%) compared to the waitlist (4%) showed reliable improvements on the Y-OQ interpersonal relations scale, χ2 = 7.02, p = .008. The difference in the proportion of parents in the intervention (30%) and waitlist (15%) who showed reliable improvements on the AFS oppositional behavior scale was marginally significant, χ2 = 3.06, p = .080.
Long-Term Intervention Effects
T3 means and SDs for the intervention, univariate time F values and effect sizes are presented in Table 2 for those parents who completed T3 only (n = 18). A multivariate time effect was found for adolescent behavior problems (F(2, 16) = 9.39, p = .002), with a significant univariate time effect found for AFS oppositional behavior. A multivariate effect was also found for the parent–adolescent relationship (F(2, 16) = 3.86, p = .043), with a univariate effect for PARS hostility. No multivariate time effects were found for conflict (F(2, 16) = 1.31, p = .298) or parenting practices (F(3, 15) < 1.00, p = .658).
Discussion
Family connectedness is considered to be one of the primary protective influences on adolescent health and development, with supportive parenting and strong parent–adolescent relationships predicting positive outcomes in adolescents even after controlling for ethnicity, income and family structure (Viner et al. 2012). Evidence-based programs are required that bolster connectedness in families with adolescents, with a particular need for prevention and intervention approaches that can be taken to scale and delivered to a large number of families efficiently and cost-effectively (Catalano et al. 2012). With that in mind, this pilot study tested the effects of a brief, targeted 2-h preventative intervention for parents of adolescents experiencing family conflict, aiming to strengthen parent–adolescent relationships and reduce adolescent behavior problems.
The findings from this study were mixed in terms of their support for the efficacy of the family conflict discussion group. Consistent with hypotheses, intervention parents reported greater reductions than control parents in adolescent problem behavior relevant to relationships with others, and a trend towards greater reductions in adolescent oppositional behavior problems at post-intervention (p = .053). These condition effects were statistically and clinically significant, with medium to large effect sizes. There was also a significant improvement at 6-month follow up among intervention parents in their report of adolescent oppositional behavior. In contrast, there were no significant condition effects on the primary outcomes of PAC specifically, and family conflict generally, although small effect sizes were seen for both measures. Moreover, there were no intervention effects for other constructs hypothesised to be affected by the intervention, namely parenting practices and the parent–adolescent relationship.
It is interesting that intervention effects were found for adolescent problem behavior, but not PAC or family conflict, particularly given there is some overlap in these measures in their assessment of poor interpersonal relations, including disagreements and arguing. Similarly, the finding that there were no significant changes in parenting is inconsistent with the underlying premise of parenting programs that improvements in child and adolescent behavior are achieved through modifying parenting practices. Previous trials of discussion groups and other brief interventions for parents of younger children have had more success, producing improvements on multiple child and parenting outcomes at medium to large effect sizes (Dittman et al. 2016b; Joachim et al. 2010; Tully and Hunt 2016). In comparison, a previous trial with parents of adolescents had similarly modest results and small effects as the current trial (Lim et al. 2005). Thus, one explanation for the current findings is that a 2-h parenting intervention may not be enough for parents of adolescents whose relationship with their adolescent and parenting practices may be more entrenched and less modifiable than those of parents of younger children. However, the small effect size at post-intervention for PAC, family conflict, parent–adolescent hostility and positive parenting, and for PAC, family conflict and discipline practices at 6-month follow-up (intervention group only) suggests that there is a trend for improvements over time and that sample power may have affected the findings. There was also a significant reduction in hostility in the parent–adolescent relationship among intervention families at 6-month follow-up. Because this finding is limited by low retention and an inability to make comparisons with the control group, it is not possible to determine the extent to which this effect is meaningful. However, in combination, these positive trends in the findings provide some preliminary evidence that parenting and the parent–adolescent relationship may be modifiable through a comparatively small dosage of parenting support. Further research is certainly needed with longer-term controlled comparisons and better retention that compare different dosages of parenting support to assess what might be required for parents to achieve meaningful behavior change in their parenting and their relationship with their adolescent.
The findings related to hostility in the parent–adolescent relationship also provide some insight into potential improvements in the nature of PAC among the intervention families. The included measures of conflict (i.e., CBQ and FES-conflict) assessed general reactions and responses to disagreements on a true/false scale, rather than the intensity or impact of the conflict on the relationship or family. The PARS Hostility subscale, on the other hand, targets the level of negativity and rejection in the relationship. Thus, it is possible that the significant reduction in hostility found for the intervention group at follow-up, along with the small effect size from pre- to post-intervention, is an indicator of reductions in the intensity and impact of conflict on the parent–adolescent relationship. As conflict between parents and adolescents is a normative process and the use of constructive strategies for resolving conflict are important for positive adolescent development (Tucker et al. 2003), it could be argued that reducing the intensity and negativity within disagreements is equally if not more important than reducing the amount of conflict. Thus, it is possible that a parenting program may work by effectively defusing negative and relationship-damaging aspects of conflict in the parent–adolescent relationship. This may also be linked to parents’ perceptions of improvements in their adolescent’s behavior in that if there is less hostility during conflict, parents’ perceptions of their adolescent’s behavior as oppositional or defiant may also shift. This model of behavior change requires further exploration with a larger scale RCT and with measures that track frequency, intensity and quality of parent–adolescent interactions. Such research should also delay the intervention for the control condition after the 6-month follow up assessment to allow a more robust test of the long-term effects of the discussion group.
During this study, and consistent with previous research evaluating multi-session parenting interventions, we faced major challenges engaging parents in the intervention, and retaining them over time to complete the post-intervention and follow-up assessments (Baker et al. 2011; Chacko et al. 2016). Of the 43 parents assigned to the intervention condition, only 34 attended the discussion group (79%), and 29 (67%) completed post-intervention assessments. Furthermore, follow-up analyses were based on only 18 (42%) intervention parents. Thus, sample size and power issues are also likely to have influenced the capacity to detect significant intervention effects. Although there were improvements from pre-intervention to 6-month follow up in adolescent oppositional behavior and hostility in the parent–adolescent relationship, any conclusions about what this means for the long-term efficacy of the discussion group need to be drawn cautiously because of the reduced sample size.
One of the main advantages of brief parenting interventions like the discussion group format being tested here, is that parents are only required to commit to 1, 2-h session, which should help address issues of retention in parenting programs that are offered over several weeks. However, we had significant difficulties finding a time that was mutually convenient for multiple parents to attend just one group session, and there were several parents who, despite booking into a session on 2 or more occasions, were not able to make it to a group. These scheduling challenges are consistent with prior research that has found that practical considerations such as competing demands, travel and access are major barriers for engagement and attendance in parenting interventions (Spoth and Redmond 2000). Failure to complete post-intervention and follow-up assessments may reflect these same barriers and perhaps a lack of understanding of the importance of the evaluation component of participating in a research project. Given the challenges with recruitment and retention, future research should look at ways to reduce barriers to engagement and participation as well as retention across assessment time-points. For example, consideration should be given to the setting for the delivery of programs. We delivered the program at a University clinic and in a community venue, but a school setting would be a useful alternative location that might assist with parent engagement. Strategies for boosting participant retention should also be built in, such as using incentives for completing assessments, particularly for parents in part-time contact with their adolescent who were less likely to complete the follow-up assessment, in order to determine the long-term effects of the discussion group.
The addition of adjunctive therapist support is another strategy that may help to address problems with retention and support changes in parenting. In previous trials of the discussion group format with parents of preschool-aged children displaying disruptive behavior problems, the group was tested both with (Morawska et al. 2011) and without (Dittman et al. 2016b) two telephone calls to provide individual support for parents’ strategy implementation. While findings were comparable in terms of the discussion group’s effects on child behavior and parenting (medium to large effect sizes), the trial that included telephone calls had higher parental satisfaction with the intervention and better retention at post-intervention and 6-month follow up than the trial without telephone calls. Further research is required to test whether parents of adolescents would benefit from additional support following participation in the family conflict discussion group, and what impact this would have on program satisfaction, retention and, most importantly, adolescent and family outcomes.
The current study had several limitations that potentially affected outcomes. First was the relatively small sample size and high attrition across time, both of which potentially affected the likelihood of finding differences across time and between groups. Further, there may be potential biases because of unmeasured differences in the participants who completed post-intervention and follow-up assessments and those who did not. Second, the measures used to assess conflict were limited to general levels of conflict in families and in the parent–adolescent relationship. Thus, a critical aspect of conflict, and one that has been shown to be damaging to family relationships and adolescent wellbeing, was not specifically assessed beyond a global measure of hostility within the relationship. Further, the study relied on parent-report only, meaning that the findings in this study reflect parent perceptions of change in their adolescent’s behavior. Future research into the potential of brief parenting programs to support parents of adolescents should involve larger, more diverse samples including a larger proportion of fathers, should obtain collateral information from teenagers and teachers, use objective outcome measures (e.g., parent–adolescent observations) and assess important related outcomes (e.g., internalizing problems). Additionally, assessment should involve a multi-dimensional assessment of PAC. Longer-term follow-up that includes both intervention and control conditions is also required to determine whether light touch parenting programs help to prevent negative long-term outcomes for adolescents and promote positive youth development.
Overall, the current study provides some preliminary evidence that a brief, single-session program targeting PAC may have benefits for families of adolescents, particularly in relation to parental perceptions of reduced oppositional and defiant behavior. Such behavior is an important precursor and outcome of conflict, that left unchecked, can have a significant impact on family relationships over time. However, given the high attrition and the lack of substantive reduction in PAC or in parenting practices, further research is needed to determine if the program format is effective. Such an endeavor is worthwhile given the potential for this format, if effective, to offer parents and agencies a low-cost, low-resource alternative to a problem that has significant impact on adolescent wellbeing and family functioning.
Notes
The median family income in Australian in 2016 was $90,168 (Australian Bureau of Statistics 2017).
Zlomke et al. (2013) reported that 9 items loaded on this factor in their analyses. However, we removed two items from this subscale as they loaded higher on other factors and had factor loadings less than the conventional .3 for inclusion in a factor. Specifically, item 5 loaded .36 on the positive parenting subscale, but only .26 on discipline practices, while item 39 loaded − .41 on discipline processes but only .29 on discipline practices. Removing these items made no difference to the results of the MANCOVA analyses on the APQ.
References
Adams, R. E., & Laursen, B. (2007). The correlates of conflict: Disagreement is not necessarily detrimental. Journal of Family Psychology, 21(3), 445. https://doi.org/10.1037/0893-3200.21.3.445.
Allison, B. N., & Schultz, J. B. (2004). Parent–adolescent conflict in early adolescence. Adolescence, 39, 101+.
Australian Bureau of Statistics. (2017). 2016 census quickstats: Australia. (4261.3). Canberra: Australian Bureau of Statistics. https://quickstats.censusdata.abs.gov.au/census_services/getproduct/census/2016/quickstat/036?opendocument.
Baker, C., Arnold, D., & Meagher, S. (2011). Enrollment and attendance in a parent training prevention program for conduct problems. Prevention Science, 12(2), 126–138. https://doi.org/10.1007/s11121-010-0187-0.
Bower, P., & Gilbody, S. (2005). Stepped care in psychological therapies: Access, effectiveness and efficiency: Narrative literature review. British Journal of Psychiatry, 186(1), 11–17. https://doi.org/10.1192/bjp.186.1.11.
Brković, I., Keresteš, G., & Puklek Levpušcˇek, M. (2014). Trajectories of change and relationship between parent–adolescent school-related conflict and academic achievement in early adolescence. Journal of Early Adolescence, 34(6), 792–815. https://doi.org/10.1177/0272431613503213.
Burke, K., Brennan, L., & Cann, W. (2012). Promoting protective factors for young adolescents: ABCD parenting young adolescents program randomized controlled trial. Journal of Adolescence, 35(5), 1315–1328. https://doi.org/10.1016/j.adolescence.2012.05.002.
Burke, K., Dittman, C. K., Ralph, A., & Haslam, D. (2020). Assessing critical dimensions of the parent-adolescent relationship from multiple perspectives: Development and validation of the Parent-Adolescent Relationship Scale (PARS). Manuscript submitted for publication.
Burlingame, G. M., Mosier, J. I., Gawain Wells, M., Atkin, Q. G., Lambert, M. J., Whoolery, M., et al. (2001). Tracking the influence of mental health treatment: The development of the youth outcome questionnaire. Clinical Psychology & Psychotherapy, 8(5), 361–379. https://doi.org/10.1002/cpp.315.
Catalano, R. F., Fagan, A. A., Gavin, L. E., Greenberg, M. T., Irwin, C. E., Jr., Ross, D. A., et al. (2012). Worldwide application of prevention science in adolescent health. The Lancet, 379(9826), 1653–1664. https://doi.org/10.1016/S0140-6736(12)60238-4.
Chacko, A., Jensen, S. A., Lowry, L. S., Cornwell, M., Chimklis, A., Chan, E., et al. (2016). Engagement in behavioral parent training: review of the literature and implications for practice. Clinical Child and Family Psychology Review, 19(3), 204–215. https://doi.org/10.1007/s10567-016-0205-2.
Chand, N. L., Farruggia, S. P., Dittman, C. K., & Sanders, M. R. (2013). Positive youth development and Teen Triple P: Promoting positive youth development through a brief parenting intervention program. Youth Studies Australia, 23(1), 29–36.
Chu, J. T. W., Bullen, P., Farruggia, S. P., Dittman, C. K., & Sanders, M. R. (2015). Parent and adolescent effects of a universal group program for the parenting of adolescents. Prevention Science, 16(4), 609–620. https://doi.org/10.1007/s11121-014-0516-9.
Chu, J. T. W., Farruggia, S. P., Sanders, M. R., & Ralph, A. (2012). Towards a public health approach to parenting programmes for parents of adolescents. Journal of Public Health, 34(suppl_1), I41–I47. https://doi.org/10.1093/pubmed/fdr123.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.). Hillsdale, NJ: Lawrence Earlbaum Associates.
De Goede, I. H., Branje, S. J., Delsing, M. J., & Meeus, W. H. (2009). Linkages over time between adolescents’ relationships with parents and friends. Journal of Youth and Adolescence, 38(10), 1304–1315. https://doi.org/10.1007/s10964-009-9403-2.
Dishion, T. J., Kavanagh, K., Schneiger, A., Nelson, S., & Kaufman, N. K. (2002). Preventing early adolescent substance use: A family-centered strategy for the public middle school. Prevention Science, 3(3), 191–201. https://doi.org/10.1023/a:1019994500301.
Dittman, C. K., Burke, K., Filus, A., Haslam, D., & Ralph, A. (2016a). Measuring positive and negative aspects of youth behavior: Development and validation of the adolescent functioning scale. Journal of Adolescence, 52, 135–145. https://doi.org/10.1016/j.adolescence.2016.08.002.
Dittman, C. K., Farruggia, S. P., Keown, L. J., & Sanders, M. R. (2016b). Dealing with disobedience: An evaluation of a brief parenting intervention for young children showing noncompliant behavior problems. Child Psychiatry and Human Development, 47(1), 102–112. https://doi.org/10.1007/s10578-015-0548-9.
Dretzke, J., Davenport, C., Frew, E., Barlow, J., Stewart-Brown, S., Bayliss, S., et al. (2009). The clinical effectiveness of different parenting programmes for children with conduct problems: A systematic review of randomised controlled trials. Child and Adolescent Psychiatry and Mental Health, 3(1), 7. https://doi.org/10.1186/1753-2000-3-7.
Eisenberg, N., Reiser, M., Maxon, E., Hofer, C., Spinrad, T., & Gershoff, E. (2008). Understanding mother–adolescent discussions: Concurrent and across time prediction from youths’ dispositions and parenting. Monographs of the Society for Research in Child Development, 73(2), 1–30. https://doi.org/10.1111/j.1540-5834.2008.00471.x.
Herrenkohl, T. I., Kosterman, R., Hawkins, J. D., & Mason, W. A. (2009). Effects of growth in family conflict in adolescence on adult depressive symptoms: Mediating and moderating effects of stress and school bonding. Journal of Adolescent Health, 44(2), 146–152. https://doi.org/10.1016/j.jadohealth.2008.07.005.
Jacobson, N. S., & Truax, P. (1991). Clinical significance: A statistical approach to defining meaningful change in psychotherapy research. Journal of Consulting and Clinical Psychology, 59(1), 12–19. https://doi.org/10.1037/0022-006X.59.1.12.
Joachim, S., Sanders, M. R., & Turner, K. M. (2010). Reducing preschoolers’ disruptive behavior in public with a brief parent discussion group. Child Psychiatry and Human Development, 41(1), 47–60. https://doi.org/10.1007/s10578-009-0151-z.
Kazdin, A. E., & Wassell, G. (1999). Barriers to treatment participation and therapeutic change among children referred for conduct disorder. Journal of Clinical Child Psychology, 28, 160–172.
Kendall, P. C., & Sheldrick, R. C. (2000). Normative data for normative comparisons. Journal of Consulting and Clinical Psychology, 68(5), 767–773. https://doi.org/10.1037/0022-006X.68.5.767.
Kim, K. J. (2006). Parent–adolescent conflict, negative emotion, and estrangement from the family of origin. Research in Human Development, 3(1), 45–58. https://doi.org/10.1207/s15427617rhd0301_5.
Klahr, A. M., McGue, M., Iacono, W. G., & Burt, S. A. (2011). The association between parent–child conflict and adolescent conduct problems over time: Results from a longitudinal adoption study. Journal of Abnormal Psychology, 120(1), 46–56. https://doi.org/10.1037/a0021350.
Kumpfer, K. L., Whiteside, H. O., Greene, J. A., & Allen, K. C. (2010). Effectiveness outcomes of four age versions of the strengthening families program in statewide field sites. Group Dynamics: Theory, Research, and Practice, 14(3), 211–229. https://doi.org/10.1037/a0020602.
Laursen, B., Coy, K. C., & Collins, W. A. (1998). Reconsidering changes in parent–child conflict across adolescence: A meta-analysis. Child Development, 69(3), 817–832. https://doi.org/10.1111/j.1467-8624.1998.tb06245.x.
Lim, M., Tormshak, E. A. S., & Dishion, T. J. (2005). A one-session intervention for parents of young adolescents: Videotape modeling and motivational group discussion. Journal of Emotional and Behavioral Disorders, 13(4), 194–199. https://doi.org/10.1177/10634266050130040101.
Little, R. J. A. (1988). A test of missing completely at random for multivariate data with missing values. Journal of the American Statistical Association, 83(404), 1198–1202. https://doi.org/10.2307/2290157.
Moed, A., Gershoff, E. T., Eisenberg, N., Hofer, C., Losoya, S., Spinrad, T. L., et al. (2015). Parent–adolescent conflict as sequences of reciprocal negative emotion: Links with conflict resolution and adolescents’ behavior problems. Journal of Youth and Adolescence, 44(8), 1607–1622. https://doi.org/10.1007/s10964-014-0209-5.
Molgaard, V., & Spoth, R. (2001). The Strengthening families program for young adolescents: Overview and outcomes. Residential Treatment for Children & Youth, 18(3), 15–29. https://doi.org/10.1300/J007v18n03_03.
Moos, R. H., & Moos, B. S. (1994). The family environment scale: The manual. Palo Alto, CA: Consulting Psychologists Press.
Morawska, A., Haslam, D., Milne, D., & Sanders, M. R. (2011). Evaluation of a brief parenting discussion group for parents of young children. Journal of Developmental and Behavioral Pediatrics, 32(2), 136–145. https://doi.org/10.1097/DBP.0b013e3181f17a28.
O’Brien, M., & Daley, D. (2011). Self-help parenting interventions for childhood behaviour disorders: A review of the evidence. Child: Care, Health and Development, 37(5), 623–637. https://doi.org/10.1111/j.1365-2214.2011.01231.x.
Omer, H., & Lebowitz, E. R. (2016). Nonviolent resistance: Helping caregivers reduce problematic behaviors in children and adolescents., 42(4), 688–700. https://doi.org/10.1111/jmft.12168.
Palmer, M. L., Keown, L. J., Sanders, M. R., & Henderson, M. (2019). Enhancing outcomes of low-intensity parenting groups through sufficient exemplar training: A randomized control trial. Child Psychiatry and Human Development, 50(3), 384–399. https://doi.org/10.1007/s10578-018-0847-z.
Ralph, A., & Sanders, M. R. (2003). Preliminary evaluation of the Group Teen Triple P program for parents of teenagers making the transition to high school. Australian e-Journal for the Advancement of Mental Health, 2(3), 169–178. https://doi.org/10.5172/jamh.2.3.169.
Ralph, A., & Sanders, M. R. (2013). Facilitator’s kit for Teen Triple P discussion group series 1. Brisbane, QLD: Triple P International Pty Ltd.
Robin, A. L., & Foster, S. L. (1989). Negotiating parent–adolescent conflict: A behavioural approach. New York: Guilford Press.
Rohner, R. P., Khaleque, A., & Cournoyer, D. E. (2005). Parental acceptance–rejection: Theory, methods, cross-cultural evidence, and implications. Ethos, 33(3), 299–334. https://doi.org/10.1525/eth.2005.33.3.299.
Salari, R., Ralph, A., & Sanders, M. R. (2014). An efficacy trial: Positive parenting program for parents of teenagers. Behaviour Change, 31(01), 34–52. https://doi.org/10.1017/bec.2013.31.
Sanders, M. R. (2012). Development, evaluation, and multinational dissemination of the Triple P-positive parenting program. Annual Review of Clinical Psychology, 8, 345–379. https://doi.org/10.1146/annurev-clinpsy-032511-143104.
Sanders, M. R., & Ralph, A. (2002). Facilitator’s manual for Group Teen Triple P. Milton, QLD: Triple P International Publishing.
Shelton, K., Frick, P., & Wootton, J. (1996). Assessment of parenting practices in families of elementary school–age children. Journal of Clinical Child Psychology, 25, 317–329. https://doi.org/10.1207/s15374424jccp2503_8.
Smetana, J. G. (2005). Adolescent–parent conflict: Resistance and subversion as developmental process. In L. Nucci (Ed.), Conflict, contradiction, and contrarian elements in moral development and education (pp. 69–91). London: Taylor & Francis.
Spoth, R., & Redmond, C. (2000). Research on family engagement in preventive interventions: Toward improved use of scientific findings in primary prevention practice. Journal of Primary Prevention, 21(2), 267–284. https://doi.org/10.1023/a:1007039421026.
Stormshak, E. A., & Dishion, T. J. (2009). A school-based, family-centered Intervention to prevent substance use: The family check-up. The American Journal of Drug and Alcohol Abuse, 35(4), 227–232. https://doi.org/10.1080/00952990903005908.
Tabachnick, B. G., & Fidell, L. S. (2007). Using multivariate statistics (5th ed.). Boston, MA: Pearson/Allyn & Bacon.
Trentacosta, C. J., Criss, M. M., Shaw, D. S., Lacourse, E., Hyde, L. W., & Dishion, T. J. (2011). Antecedents and outcomes of joint trajectories of mother–son conflict and warmth during middle childhood and adolescence. Child Development, 82(5), 1676–1690. https://doi.org/10.1111/j.1467-8624.2011.01626.x.
Tucker, C. J., Mchale, S. M., & Crouter, A. C. (2003). Conflict resolution: Links with adolescents’ family relationships and individual well-being. Journal of Family Issues, 24(6), 715–736. https://doi.org/10.1177/0192513x03251181.
Tully, L. A., & Hunt, C. (2016). Brief parenting interventions for children at risk of externalizing behavior problems: A systematic review, 25(3), 705–719. https://doi.org/10.1007/s10826-015-0284-6.
van Aar, J., Leijten, P., Orobio de Castro, B., & Overbeek, G. (2017). Sustained, fade-out or sleeper effects? A systematic review and meta-analysis of parenting interventions for disruptive child behavior. Clinical Psychology Review, 51, 153–163. https://doi.org/10.1016/j.cpr.2016.11.006.
Viner, R. M., Ozer, E. M., Denny, S., Marmot, M., Resnick, M., Fatusi, A., et al. (2012). Adolescence and the social determinants of health. The Lancet, 379(9826), 1641–1652. https://doi.org/10.1016/S0140-6736(12)60149-4.
Webster-Stratton, C., & Taylor, T. (2001). Nipping early risk factors in the bud: Preventing substance abuse, delinquency, and violence in adolescence through interventions targeted at young children (0–8 years). Prevention Science, 2, 165–192.
Weinberger, D., Tublin, S., Ford, M., & Feldman, S. (1990). Preadolescents’ social-emotional adjustment and selective attrition in family research. Child Development, 61(5), 1374–1386. https://doi.org/10.2307/1130749.
Weymouth, B. B., & Buehler, C. (2016). Adolescent and parental contributions to parent–adolescent hostility across early adolescence. Journal of Youth and Adolescence, 45(4), 713–729. https://doi.org/10.1007/s10964-015-0348-3.
Zhao, H., Xu, Y., Wang, F., Jiang, J., Zhang, X., & Wang, X. (2015). Chinese adolescents’ coping tactics in a parent–adolescent conflict and their relationships with life satisfaction: The differences between coping with mother and father. Frontiers in Psychology, 6, 1572. https://doi.org/10.3389/fpsyg.2015.01572.
Zlomke, K. R., Lamport, D., Bauman, S., Garland, B., & Talbot, B. (2013). Parenting adolescents: Examining the factor structure of the Alabama parenting questionnaire for adolescents. Journal of Child and Family Studies, 23, 1–7. https://doi.org/10.1007/s10826-013-9803-5.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The Parenting and Family Support Centre is partly funded by royalties stemming from published resources of the Triple P—Positive Parenting Program, which is developed and owned by The University of Queensland (UQ). Royalties are also distributed to the Faculty of Health and Behavioural Sciences at UQ and contributory authors of published Triple P resources. Triple P International (TPI) Pty Ltd is a private company licensed by Uniquest Pty Ltd on behalf of UQ, to publish and disseminate Triple P worldwide. The authors of this report have no share or ownership of TPI. Authors Burke and Hodges are employed by and Dr. Dittman holds an honorary appointment with The University of Queensland. Dr. Dittman is an author on a Triple P Program, but not the program under evaluation in this study. Drs. Dittman, Burke and Hodges may in the future receive royalties and/or consultancy fees from TPI.
Ethics Approval
All procedures performed in this study, which involved human participants, were in accordance with the ethical standards of the authors’ institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all participants in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Dittman, C.K., Burke, K. & Hodges, J. Brief Parenting Support for Parents of Teenagers Dealing with Family Conflict: A Pilot Randomized Controlled Trial. Child Youth Care Forum 49, 799–816 (2020). https://doi.org/10.1007/s10566-020-09557-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10566-020-09557-2