
Abstract
Object We analyzed MMP-9 expression using mRNA and protein level determinations and explored the possibility that Matrix metalloproteinase-9 (MMP-9) is a potential biological marker of pituitary adenoma invasiveness and whether MMP-9 could be used to discriminate the extent of invasiveness among different hormonal subtypes, tumor sizes, growth characteristics, and primary versus recurrent tumors. Materials and methods 73 pituitary tumor specimens were snap frozen in liquid nitrogen immediately after surgical resection. RNA and protein were extracted. MMP-9 mRNA transcripts were analyzed by quantitative RT-PCR. MMP-9 protein activity was analyzed by gelatin zymography and validated by western blot analysis. Immunohistochemistry was performed to identify the presence and localization of MMP-9 in pituitary adenomas. Statistical differences between results were determined using Student’s t-test or one way ANOVA. Results Comparing different hormonal subtypes of noninvasive and invasive pituitary tumors, MMP-9 mRNA expression was significantly increased in the majority of invasive adenomas. Considering the protein levels, our data also showed a significant increase in MMP-9 activity in the majority of invasive adenomas and these differences were confirmed by western blot analysis and immunohistochemistry. In addition, consistent differences in MMP-9 expression levels were found according to tumor subtype, tumor size, tumor extension and primary versus redo-surgery. Conclusions MMP-9 expression can consistently distinguish invasive pituitary tumors from noninvasive pituitary tumors and would reflect the extent of invasiveness in pituitary tumors according to tumor subtype, size, tumor extension, primary and redo surgery, even at early stages of invasiveness. MMP-9 may be considered a potential biomarker to determine and predict the invasive nature of pituitary tumors.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Pituitary adenomas are common benign neoplasms and represent 15–20% of primary brain tumors. Although in most cases they do not metastasize, greater than 40% of pituitary tumors demonstrate microscopic evidence of local invasion [1, 2]. They may infiltrate adjacent structures and grow in several directions: superiorly, permeating the diaphragma sellae to reach the suprasellar cistern; inferiorly, eroding the sellar floor and extending into the sphenoid sinus; laterally, disrupting the medial wall of the cavernous sinus, obliterating the venous structures, even encasing the internal carotid artery; posteriorly, destroying the clivus and reaching the brain-stem. From a surgical standpoint, invasive pituitary tumors carry increased risks of cerebrospinal fluid leak, and damage to cranial nerves and the internal carotid artery in the cavernous sinus. Moreover, invasiveness in pituitary tumors makes total resection impossible with standard surgical techniques, and adjunctive therapy is usually necessary for long-term control of disease. Undoubtedly, invasiveness is the major factor that determines therapeutic efficacy and prognosis in pituitary tumors, including the fate of postoperative residual tumor, rate of remission, rate of recurrence and patient survival [3].
At present, the diagnosis of invasive adenomas is made by imaging, histopathology and intraoperative gross observation. Because of the limitations of subjective factors in imaging analysis, during surgery, and with specimens submitted for pathology, an objective biological marker is required to improve the accuracy of diagnosis. It should be sensitive enough to label invasive tumor at an early stage and could become an important complement to the former methods. According to the recognized tumor behavior of invasive lesions, physicians could alter the strategy of operation and postoperative radiation or medical therapy and predict the propensity for recurrence. Furthermore, a biological marker could provide a clue for development of an inhibitor which might block the progression of invasiveness in pituitary tumors.
So far, several biological markers for dural invasiveness have been investigated, but it is not clear which factors are responsible for invasiveness in pituitary adenomas. Isono et al. immunohistochemically examined the expression of leptin and found that leptin expression correlated with the invasive potential of functioning pituitary adenomas [4]. The polysialated neural cell adhesion molecule (NCAM) was found strongly to be related to pituitary tumor invasion [5]. Soluble CD44v6 in peripheral blood was found lower in patients with invasive pituitary adenomas [6]. The p53 tumor suppressor gene did seem to have some usefulness in identifying biologically aggressive pituitary tumor [7] and purine-binding factor (nm23) gene expression was inversely associated with invasive pituitary adenomas [8]. These conclusions have not been accepted by all investigators.
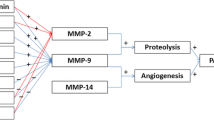
Although tumor cell invasion and metastasis are complex cascades involving multiple host–tumor interactions, the degradation of matrix is a prerequisite to tumor invasion [9]. As for the essential step of extracellular matrix (ECM) and basement membrane (BM) degradation, matrix metalloproteinases (MMPs), particularly MMP-9, are thought to play a central role in this proteolytic process [10]. MMP-9 is a member of the zinc-containing endopeptidases (type IV collagenase, gelatinase B), and is reported to be markedly associated with invasion and metastasis in several human cancers [11–18]. It has been shown in vitro that the secretion of MMP-9 appears at an early stage of tumor cell migration through the ECM [19]. For pituitary tumors, it is well known that, within the sella tucica, the capsule of tumor is enclosed by dura, which is composed of collagen of which the key compartment is type IV collagen [20, 21]. MMP-9 specifically degrades type IV collagen and paves the way for pituitary tumor cells to migrate through the dura and invade into surrounding tissues. In the present study, we determined MMP-9 expression at mRNA and protein levels and explored whether MMP-9 was a potential biomarker for pituitary adenoma invasiveness, in particular whether it is capable of distinguishing invasive from noninvasive tumors and discriminating invasiveness among different tumor sizes, directions of growth, hormonal subtypes and primary versus recurrent tumors. This is a systematic study to correlate MMP-9 expression with the invasive nature of pituitary tumors and the results provide a novel information for the clinician which can be used to recommend appropriate therapeutic strategies.
Materials and methods
Patients
Pituitary tumor specimens were obtained at the University of Virginia Medical Center from November, 2005 to October, 2006, under the approval of the Human Investigation Committee. There were 73 patients, including 50 cases of nonfunctioning adenomas (NFAs) and 23 cases of functioning adenomas (FAs). In the former group, there were 22 women and 28 men, with a mean age of 55 years (range: 19–79 year). In the latter group, there were 14 women and 9 men, with a mean age of 44 years (range: 11–74 year). All of them underwent surgical resection of pituitary adenomas and were classified by histological, immunohistochemical, and ultrastructural analysis. The diagnosis of tumor invasion or noninvasion was made according to the combination of histological evidence of dural invasion and gross observation of invasiveness at surgery. The subtypes and numbers of noninvasive/invasive tumors are: null cell adenomas (7/16), gonadotrophic adenomas (8/9), silent ACTH adenomas (1/7), silent GH adenomas (1/1), Cushing’s disease (ACTH adenoma) (6/3), acromegaly (GH adenoma) (4/7), and prolactinomas (PRL adenoma) (0/3). With regard to tumor size and extension, we classified them into microadenoma (tumor diameter equal to or less than 1 cm), macroadenoma (tumor diameter is more than 1 cm but still restricted to the sella turcica), extending adenoma, in which the tumor extended out of sella turcica to the suprasellar, cavernous sinus and sphenoid sinus regions. The numbers and proportion of NFAs/FAs in different groups are following: microadenoma 8(16%)/13(58%), macroadenoma 4(8%)/3(13%), suprasellar extension 21(42%)/2(8%), cavernous sinus extension 7(14%)/3(13%), sphenoid sinus extension 10(20%)/2(8%). There were 60 primary tumors and 13 recurrent or persistent tumors. The adenomas were obtained at surgery, adherent blood was removed by washing in 1× PBS Buffer, and then samples were snap frozen in liquid nitrogen immediately and stored at −80°C. In 52(71%) tumor specimens, RNA and protein were extracted. For some small surgical specimens, 5 (7%) samples were protein extracted only and 16 (22%) samples RNA were extracted only.
RNA extraction
Total RNA was extracted from human pituitary tumors using Trizol (Invitrogen), according to the manufacturer’s protocol (Invitrogen, Carlsbad, California, USA).
Protein extraction
The tumor specimens were weighed and trimmed by scissors and solublized in 1% Triton X-100 buffer (0.25%TritonX-100, 0.01 M CaCl2, pH 7.5), the tissues were homogenized for 15–20 s in the KIMAX homogenizer and centrifuged at 10,000 rpm at 4°C for 30 min. Supernatant was pooled for assays of MMP-2 and MMP-9 activities in zymography and western blotting. The protein concentration of the supernatant was determined by the BCA protein assay (Bio-Rad).
Gelatin zymography
The activities of MMP-2 and MMP-9 in the pituitary adenoma specimens were detected by gelatin zymography. Aliquots of protein (25 μg) were mixed with four times quantity of sample loading buffer (0.25 M Tris, 40% glycerol, 0.04% bromphenol blue, 8% SDS, pH 6.8) and incubated at 37°C for 30 min. Equal amounts of proteins were loaded for electrophoresis on 10% SDS (Sodium dodecyl sulfate)-polyacrylamide gels containing 1% gelatin under nonreducing conditions. The gels were incubated for 20 h at 37°C and stained with 0.1% Coomassie Blue solution. The gelatinolytic bands of MMP-2 and MMP-9 were identified according to a previous report [22].
Densitometric and semi-quantitation of MMP-9 protein levels
Bands of MMPs were scanned and their activities were quantitated by densitometry and ImageQuant software (Amersham Biosciences). Each gel, under the same condition, was run on five lanes of purified pro-MMP-9 at different concentrations (0.05, 0.25, 0.5, 1, 2 ng/ml). A linear range of a relationship between the concentrations of MMP-9 and integrated optical density (IOD) of the lysis bands was established and a concentration curve was generated. From the standard curve, the MMP-9 activity of each sample was semi-quantitatively analyzed according to its relative concentration (Fig. 1).

Densitometric and semi-quantitation of MMP-9 protein levels. The activities of MMP-2 (72 kDa) and MMP-9 (92 kDa) in the pituitary adenoma specimens were detected by gelatin zymography (Top). Lane 1–3 were noninvasive and lane 4–6 were invasive gonadotrophic adenomas. Under the same conditions, five lanes of purified pro-MMP-9 (lane7–11) at different concentrations (0.05, 0.25, 0.5, 1, 2 ng/ml) were run. A linear range of a relationship between the concentrations of MMP-9 and integrated optical density (IOD) of the lysis bands was established and a concentration curve was generated (Bottom). From the standard curve, the MMP-9 activity of each sample was semi-quantitively analyzed according to its relative concentration. GN: gonadotrophic adenoma, Plus: Invasive adenoma, Minus: Noninvasive adenoma
Immunohistochemistry
Immunohistochemistry for MMP-9 (#3852 polyclonal antibody at 1:50 dilution from Cell Signaling, Beverly, MA) was performed in formalin-fixed, paraffin embedded tissues. All slides were stained using the automated Nexes IHC stainer (Ventana, Tucson, AZ) providing consistency of the experimental conditions. Positive and negative controls were run concomitantly in all cases.
Western blot analysis
Proteins were boiled for 5 min in SDS-PAGE sample buffer. Proteins (200 μg/lane) were separated by SDS-PAGE on 10% polyacrylamide gels and then electroblotted onto nitrocellulose and reacted with monoclonal and polyclonal antibodies. Polyclonal antibodies against MMP-2 and MMP-9 were purchased from Santa Cruz Biotechnology, Inc. (sc-8835) and Cell Signaling (#3852, Beverly, MA) respectively. MMP-2 and MMP-9 antibodies were used at 1:1000 dilutions. The second antibodies were horseradish peroxidase-conjugated secondary antibodies (Sigma, St. Louis, MO). Immunoblotted proteins were detected using ECL reagents (Amersham Biosciences) as described by the manufacturer.
Quantitative RT-PCR
Total RNA was extracted as described earlier. Reverse transcription was performed with MultiScribe reverse transcriptase (Applied Biosystems, Forster City, CA) and random hexamers as per the manufacturer’s instructions. Primers were designed from the target sequences by NCBI refseq mRNA database using Primer Express 2.0 software (Applied Biosystems). Quantitative PCRs were carried out in triplicate using equal amounts of each cDNA sample equivalent to approximately 50 ng of starting total RNA. Each reaction contained the fluorescent indicator SYBR® Green I Dye, and 200 nM of each forward and reverse primer (5 μM) in a total volume of 25 μl. Amplifying PCR and monitoring of the fluorescent emission in real time were performed in the ABI Prism 7900HT Sequence Detection System (Applied Biosystems) as described (ABI SYBR Green Protocol). To verify that only a single PCR product was amplified per transcript, dissociation curve data were analyzed with the 7900HT Sequence Detection Software (SDS). To account for differences in starting material, quantitative PCR was also carried out for each cDNA sample using housekeeping, glyceraldehyde-3-phosphate dehydrogenase (GAPDH) and β-actin (ACTB). The data collected from these quantitative PCRs defined a threshold cycle number (Ct) of detection for the target or the housekeeping genes in each cDNA sample.
Relative quantity (RQ) of the perspective target genes was calculated using the relative quantitation method. Briefly, each Ct value was normalized to the correspondent geometric means of the endogenous reference genes (GAPDH and ACTB). For each comparison, the RQ is given by: RQ = 2−ΔΔCt, where ΔΔCt represents the difference in Ct between the transcript and the housekeeping gene for the same RNA sample. The ratio of the RQs for the treated sample and the experimental sample was used to derive the fold change. Analysis of the variance (ANOVA) was then used to determine the mean and standard error for each comparison.
Statistical analysis
Representative experiments with average changes and SEM are shown. Statistical differences between results were determined using Student’s t-test for paired or unpaired data and multiple data from different groups were analyzed by one way ANOVA followed by multiple range tests as appropriate using Prism GraphPad Software. A P value of 0.05 or less was considered significant.
Results
Comparison of MMP-9 mRNA expression among different subtypes of noninvasive and invasive pituitary tumors by Real-Time PCR
Total RNA was extracted from 68 (93%) frozen samples and was analyzed for MMP-9 mRNA transcripts by real-time PCR. Comparing noninvasive and invasive pituitary tumors, MMP-9 mRNA expression was significantly increased in the invasive groups of all pituitary tumors (0.58 ± 0.09 fold vs. 2.32 ± 0.38 fold, P < 0.01), nonfunctioning tumors (0.61 ± 0.13 fold vs. 2.21 ± 0.44 fold, P < 0.01), functioning tumors (0.52 ± 0.12 fold vs. 2.55 ± 0.76 fold, P < 0.01), null cell tumors (0.48 ± 0.17 fold vs. 1.87 ± 0.61 fold, P < 0.05), gonadotrophic tumors (0.70 ± 0.26 fold vs. 2.55 ± 0.48 fold, P < 0.01), and active ACTH tumors (0.36 ± 0.09 fold vs. 2.53 ± 0.48 fold, P < 0.01). There was a slight increase of MMP-9 mRNA in active GH tumors (0.84 ± 0.20 fold vs. 1.38 ± 0.75 fold, P > 0.05). Moreover, MMP-9 mRNA was significantly overexpressed in invasive prolactinomas (6.67 ± 1.82 fold) and positive controls (including three invasive meningiomas and three chordomas) (4.13 ± 2.97 fold) when compared with other subtypes of invasive tumors (P < 0.05) (Fig. 2A).

(A) Comparison of MMP-9 mRNA expression between noninvasive and invasive pituitary tumors of different subtypes by Real-Time PCR. MMP-9 mRNA expression was significantly increased in the invasive groups of PAs, NFAs, FAs, Null, GN, and ACTH. Number of samples in different group (Noninvasive/Invasive): PAs:26/42, NFAs:16/30, Fas:10/12, Null:7/14, GN: 7/9, Silent ACTH:1/6, Silent GH:1/1, Active ACTH:6/3, Active GH:4/6, PRL: 0/3, Positive Control:0/6. (B) Comparison of MMP-9 protein expression between noninvasive and invasive pituitary tumors of different subtypes. (relative concentration (top) and partially corresponding bands (bottom) in zymography). Number of samples in different group (Noninvasive/Invasive): PAs: 23/34, NFAs: 13/22, FAs: 10/12, Null: 6/10, GN: 5/6, Silent ACTH:1/5, Silent GH:1/1, Active ACTH:6/3, Active GH:4/6, PRL: 0/3, Positive Control:0/6. There were no statistically significant differences in noninvasive silent ACTH and silent GH tumors. PAs: all pituitary adenomas (NFAs, FAs), NFAs: nonfunctioning adenomas (Null, GN, Silent ACTH, Silent GH), FAs: functioning adenomas (GH, ACTH, PRL), Null: null cell adenomas, GN: gonadotrophic adenomas, GH: active growth hormone adenomas, PRL: prolactinomas. Star symbol: comparison between noninvasive and invasive tumors in the same group (*P < 0.05, **P < 0.01). Pound symbol: Comparison among invasive tumors or among noninvasive tumors of different subtypes (#P < 0.05, ##P < 0.01). Plus: Invasive adenoma, Minus: Noninvasive adenoma
Comparison of MMP-9 protein expression between different subtypes of noninvasive and invasive pituitary tumors by zymography
Total protein was extracted from 57 (78%) frozen specimens and MMP-9 activity was analyzed by zymography. Two bands corresponding to monomer MMP-9 (92 kDa) and the lipocalin-bound heterodimer of MMP-9 (130 kDa) were detected as described previously [23]. Comparing noninvasive and invasive pituitary tumors, the data showed a significant increase in MMP-9 activity in the invasive groups of all pituitary tumors (1.03 ± 0.20 ng/ml vs. 2.37 ± 0.33 ng/ml, P < 0.01), nonfunctioning tumors (0.77 ± 0.21 ng/ml vs. 1.94 ± 0.34 ng/ml, P < 0.01), functioning tumors (1.41 ± 0.19 ng/ml vs. 3.23 ± 0.65 ng/ml, P < 0.05), active ACTH tumors (1.34 ± 0.13 ng/ml vs. 3.2 ± 0.55 ng/ml, P < 0.01). There was a slight increase in null cell tumors (0.82 ± 0.38 vs. 1.82 ± 0.44 ng/ml, P > 0.05), gonadotrophic tumors (0.70 ± 0.10 ng/ml, P > 0.01), and active GH tumors (1.53 ± 0.53 ng/ml vs. 1.93 ± 0.68 ng/ml, P > 0.05). Additionally, MMP-9 protein expression was significantly elevated in invasive silent ACTH tumors (3.32 ± 0.55 ng/ml), invasive prolactinomas (4.81 ± 1.11 ng/ml) and positive controls (4.03 ± 0.46 ng/ml) when compared with other subtypes of invasive tumors (P < 0.05) (Fig. 2B Top). Notably, in most cases, there was relatively low activity of MMP-2 (72 kDa) and there was no correlation with MMP-9 activity in both invasive and noninvasive pituitary adenomas. (Fig. 2B Bottom)
Validation of MMP-9 protein expression by western blot analysis
To verify the results of zymography, 34 randomized cases (60%) were analyzed for MMP-9 protein expression by western blot. As shown in Fig. 3A, pituitary tumor MMP-9 expressions, analyzed by zymography (panel A), were consistent with counterpart expressions by western blot (panel B). The bands of MMP-2 by western blot were faint and exhibited the same low activity as demonstrated by zymography.

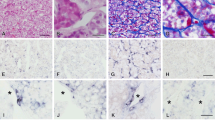
(A) MMP-9 protein activity expression in partial samples were shown by zymography (Panel A) and validated by western blot analysis (Panel B). The MMP-9 protein activity expressions of pituitary tumors by zymography were consistent with their counterparts in western blot analysis. The bands of MMP-2 showed faint, low activities. Null Cell: null cell adenomas, GN: gonadotrophic adenomas, Plus: Invasive adenoma, Minus: Noninvasive adenoma. (B) Validation of MMP-9 protein expression by immunohistochemistry. B–A: Positive control: meningioma intensely stained for MMP-9 in tumor cells, vessels and connective tissues. B–B: Non-invasive adenoma: MMP-9 diffuse and weakly immunoreactive adenoma cells and some faint positive staining of the vascular structures (arrow) were noted. B–C: Invasive pituitary tumor expressing focal but intense cytoplasmic immunoreactivity of adenoma cells for MMP-9. B–D: An adenoma in which bone invasion was present shows intense cytoplasmic immunoreactivity for MMP-9 (arrow)
Validation of MMP-9 protein expression by immunohistochemistry
To identify the source of MMP-9 in the noninvasive and invasive pituitary adenomas, we performed immunohistochemical staining in 23 random cases (40%). As a positive control, we used meningioma sample which was intensely stained by the MMP-9 antibody in tumor cells, vessels and connective tissues (Fig. 3B–A). MMP-9 immunoreactivity was seeing weakly in the cytoplasma of adenoma cells and vascular structures (arrow) in the noninvasive pituitary adenomas (Fig. 3B–B, sample 6 in Fig. 3A). In contrast, the invasive pituitary tumors expressed either focal or diffuse but intense cytoplasmic immunoreactivity of adenoma cells for MMP-9 (Fig. 3B–C, sample 17 in Fig. 3A). Figure 3B–D shows intense cytoplasmic immunoreactivity for MMP-9 (arrow) in a pituitary adenoma with bone invasion.
Comparison of MMP-9 expression among different sizes of pituitary tumors
In the NFAs, with an increase in tumor size, MMP-9 mRNA expression increased correspondingly (0.74 ± 0.28 fold, 1.22 ± 0.21 fold, 1.69 ± 0.35 fold) and the level of MMP-9 mRNA was significantly higher in extending adenomas than in microadenomas (P < 0.05). In the FAs, however, compared to the macroadenomas, microadenmas slightly (0.78 ± 0.17 fold vs. 1.32 ± 0.61 fold, P > 0.05) and extending adenomas significantly (0.78 ± 0.17 fold vs. 2.86 ± 1.23 fold, P < 0.01) demonstrated elevated MMP-9 mRNA expression. Hence, considering all pituitary tumors, there were no significant changes in MMP-9 mRNA transcripts between micro and macroadenomas, but a significant increase was noted in extending adenomas. The general trends of MMP-9 protein activities were consistent (Fig. 4).

(A) Correlation between mRNA expression of MMP-9 and pituitary tumor size. Number of samples in different groups (Micro/Macro/Extension): pituitary tumor: 21/7/40, NFAs: 8/4/33, FAs: 13/3/7. (B) Correlation between protein expression of MMP-9 and pituitary tumor size. Number of samples in different groups (Micro/Macro/Extension): pituitary tumor: 17/7/33, NFAs: 6/4/26, FAs: 11/3/7. NFAs: non-functioning adenoma, FAs: hyperfunctioing adenoma. Micro: microadenoma, Macro: macroadenoma, Extension: extending adenoma. Star symbol: comparison among microadenomas, macroadenomas and extending adenomas in the same group (*P < 0.05, **P < 0.01)
Comparison of MMP-9 expression among different extensions of pituitary tumor
In pituitary adenomas, comparing nonfunctioning and functioning tumors, MMP-9 expression slightly decreased (mRNA level, 1.64 ± 0.29 fold vs. 1.34 ± 0.36 fold) or increased (protein level, 1.52 ± 0.23 vs. 2.18 ± 0.36 ng/ml), and there was no statistically significant difference. In microadenomas only, comparing nonfunctioning and functioning tumors, the latter had slightly increased MMP-9 expression at the mRNA level (0.74 ± 0.28 fold vs. 1.32 ± 0.61 fold, P > 0.05) and it was significantly increased at the protein level (0.61 ± 0.19 vs. 2.25 ± 0.53 fold, P < 0.01). In NFAs, comparing micro-, macro- and suprasellar adenomas, to tumor which extended into the cavernous sinus and sphenoid sinus, there was a significant increase in MMP-9 expression at both mRNA and protein levels. Interestingly, in FAs, there was no significant difference between microadenomas and cavernous sinus/sphenoid sinus extending tumors in terms of MMP-9 expression (Fig. 5).

(A) Comparison of MMP-9 mRNA expression between nonfunctioning and functioning pituitary adenomas with different extension. Number of samples in different group (non-functioning/functioning adenomas): micro: 8/13, macro: 4/3, supra: 17/2, caver.s.: 7/3, sphenoid s.:9/2, all sizes: 45/23. (B) Comparison of MMP-9 protein expression between nonfunctioning and functioning pituitary adenomas with different extension. Number of samples in different group (non-functioning/functioning adenomas): micro:6/11, macro:4/3, supra:12/2, caver.s.:6/3, sphenoid s.:8/2, all sizes: 36/21. There were no statistical significances in functioning adenomas of suprasellar extending and sphenoid sinus extending. Star symbol: comparison between nonfunctioning and functioning tumors in the same group (*P < 0.05, **P < 0.01). Pound symbol: Comparison among different groups in non-functioning adenomas or in functioning adenomas (#P < 0.05, ##P < 0.01) Micro: microadenoma; macro: macroadenoma; supra: suprasellar extension; caver.s.: cavernous sinus extension; sphenoid s.: sphenoid sinus extension
Comparison of MMP-9 expression in pituitary tumor between primary surgery and redo-surgery
In current group, there were 13 samples from redo surgery (NFAs:7, FAs: 6). One case was clearly recurrent, all the others classified as enlargement of persistent tumors. As seen in Fig. 6, all the redo cases expressed more MMP-9 as compared with primary cases at both the mRNA and protein levels. The nonfunctioning tumors from redo surgery had a significantly increased MMP-9 mRNA expression (1.18 ± 0.65 fold vs. 4.84 ± 1.99 fold).

(A) Comparison of MMP-9 mRNA expression in pituitary tumors between primary surgery and redo-surgery. Number of samples in different group (primary surgery/redo-surgery): PAs: 56/12, NFAs: 38/7, FAs: 18/5. (B) Comparison of MMP-9 protein expression in pituitary tumors between primary surgery and redo-surgery. Number of samples in different groups (primary surgery/redo-surgery): PAs: 48/9, NFAs: 31/5, FAs: 17/4. Star symbol: comparison between primary surgery and redo-surgery in the same group (*P < 0.05, **P < 0.01). PAs: pituitary adenomas, NFAs: non-functioning adenomas, FAs: functioning adenomas
Discussion
Invasive pituitary adenomas present a major challenge to physicians because of their local invasive behavior; total surgical resection is not possible with standard surgical techniques [3]. Any residual tumor, even just a few tumor cells, still retains its inherent ability to proliferate and may be the source of tumor recurrence. Accordingly, adjunctive therapy in the form of radiation therapy or medical therapy is often recommended. Recently, however, preventive postoperative treatment in the form of radiation therapy has been frequently withheld [24], because of the risk of significant side-effects [25]. A biological marker of invasiveness in pituitary tumors would be most helpful and should be sensitive enough to identify invasive tumors at an early stage so as to guide clinicians in recommending a reasonable therapeutic strategy, including surgery and adjunctive treatment, with close follow-up and clinical surveillance, seeking to reduce both the risks of side-effects and the recurrence rate as much as possible.
The mechanisms that dictate local invasive behavior of pituitary adenomas remain poorly understood; several biomarkers for dural invasiveness have been investigated but none has been universally accepted. In fact, the degradation of matrix is a prerequisite to tumor invasion and type IV collagen is the key component of dura. As tumor cell invasion involves selective remodeling of the ECM by the secretion of proteases (MMPs and uPA), we confirmed the hypothesis that MMP-9, a type IV collagenase, increases invasion in pituitary tumor cells through collagen IV [26]. In the current study, we tested MMP-9 expression in noninvasive and invasive pituitary adenomas and explored whether MMP-9 might become a potential biomarker to label invasiveness of pituitary tumors.
Criteria for invasive pituitary tumors
In our study, the fundamental issue is to clearly define the concept of the invasive pituitary tumor. Usually, the definition of invasive pituitary tumor depends on pre-operative imaging studies, intraoperative gross observation and post-operative histopathology. Hence, the evidence of invasion varies depending on whether the lesion is examined radiologically, at surgery, or microscopically. As Laws et al. pointed out [3, 27], there was a good deal of confusion about the concept of invasion in pituitary adenomas; this confusion added to the difficulty of diagnosis and had an impact on recommendations for therapy and the risks of surgical management. It is probably incorrect to discuss invasion of pituitary adenomas simply on the basis of MRI appearance. Although high-quality MRI may occasionally show clear evidence of a pituitary tumor breaking through its dural barriers, but this is often inconclusive. Moreover, an adenoma can extend into the cavernous sinus, pushing the dura laterally and on occasion even apparent total encasement of the carotid artery may occur without breaching the dura. Certainly, evidence of dural invasion by histopathology is a golden criterion in the definition of an invasive tumor. However, the dural specimen is usually sampled from a single location at the central inferior portion of the sella turcica, regardless of the location or size of the tumor. This seriously underestimates the actual incidence of dural invasion, especially when the diaphragma sellae and the cavernous sinus dura are invaded [2]. In our present study, there were 21 cases diagnosed as noninvasive or invasive adenomas by pathology which were inconsistent with intraoperative gross observation. Among them, there were five cases in which there was clear evidence of invasion of the medial wall of the cavernous sinus at surgery, but evidence of dural invasion was absent in the pathological analysis. Additionally, some investigators favored the concept that intraoperative demonstration of invasion may be a more important factor affecting therapeutic strategy than the isolated finding of dural infiltration on microscopic studies [28]. Regarding the basis of dural invasion assessed by pathology, if combined with surgical observation, we believe that the diagnosis of invasive pituitary adenomas is accurate and reliable.
Correlation between MMP-9 expression and pituitary tumor invasion
Since the mechanism whereby pituitary tumors become invasive is poorly understood, the correlation between MMP-9 expression and invasiveness of pituitary tumors is controversial. Some authors, using retrospective analysis on the basis of immunohistochemistry [29, 30], suggested that invasive pituitary adenomas were significantly more likely to express MMP-9 than noninvasive tumors. Pereda et al. reported surprisingly high levels of MMP-9 activity indicating a high level of ECM-degrading activity in pituitary adenomas [31], and Kawamoto strongly suggested that MMP-9 secretion, especially the number of MMP-9 secreting cells, may be associated with cavernous sinus invasion by pituitary adenomas. MMP-9 secretion by adenoma cells can be considered an important factor in predicting invasion of pituitary adenomas [32]. Using frozen tumors, Kawamoto believed that type IV collagenase may play a role in the invasion of the cavernous sinus by pituitary adenomas [20], and Beaulieu et al. reported that MMP-9 plays a role in the invasive nature of pituitary tumors studied [33]. Conversely, Knappe found no correlation between MMP-9 expression and tumor invasion [34], and Yokoyama et al. did not find any difference in immunoexpression of MMP-9 in nonsecreting adenomas with or without encasement of the carotid artery within the cavernous sinus [27]. Both of these experiments depended on immunocytochemical analysis.
In the present study, compared with noninvasive tumors, MMP-9 expression, either at the mRNA level or at the protein level, was significantly increased in invasive pituitary tumors of nonfunctioning, functioning and the majority of subtypes. Because our tissues were freshly frozen, they should be more representative of their original status than cell culture or paraffin-embedded specimens; the results should be more reliable and they were validated by multiple analytical approaches. The present report provides evidence that MMP-9 can be used to distinguish invasive pituitary tumors from noninvasive indolent ones and provides the surgeon with complementary information regarding clinical invasiveness of pituitary tumors. Since there are no reliable pathological markers to determine pituitary tumor invasiveness, MMP-9 is proposed as a potential marker to alert the clinician to the possibility of a more biologically aggressive variant of tumor and should prompt careful postoperative clinical surveillance.
Notably, MMP-2 and MMP-9 are both type IV collagenases, which have been shown to be important in tumor invasion because they are able to break down BM, in particular, degrading collagen IV [20]. However, Beaulieu found no correlation could be established between the invasive potential pituitary tumors and the expression levels of MMP-2 [33]. The current study confirmed our previous report [26] that there was very low activity of MMP-2 in both invasive and noninvasive pituitary tumors and that there may be no correlation between MMP-2 and MMP-9 expression [34]. Marbaix et al. have reported that MMP-9 but not MMP-2 could be activated by trypsin [35]. It is likely that MMP-9 or other trypsin-activated type IV collagenases contribute to the high concentration of type IV collagenase activity in pituitary adenomas. So, of all the type IV collagenases, we suggest that MMP-9 rather than MMP-2 plays a key role in the invasiveness of pituitary tumors.
Correlation between MMP-9 expression and pituitary tumors subtypes
There are few studies that report the correlation between invasiveness and different adenoma subtypes. In general, poorly differentiated sparsely granulated, and hormonally inactive pituitary adenomas are more often invasive than well-differentiated, densely granulated, and hormonally active adenomas [28, 36, 37].
From our results, MMP-9 expression in invasive silent-ACTH adenomas, active ACTH adenomas and prolactinomas was slightly higher at the mRNA level and significantly higher at the protein level than that of other invasive subtypes. It has been demonstrated that the frequency of recurrence and aggressiveness of silent corticotroph adenomas is higher than average and this underscores the need for long-term follow-up [38–40]. In ACTH-secreting adenomas, overexpression of MMP-9 contributes to the relatively high proportions of ACTH-secreting adenomas that are invasive [41, 42].
Comparing nonfunctioning and functioning pituitary tumors, Meij et al. reported that dural invasion was present in more than 50% of NFAs and in 30–35% of patients with endocrinologically active adenomas [2]. Regarding MMP-9 expression, Kawamoto proposed that there was no obvious difference between nonfunctioning and functioning tumors [32]. Our data showed the same results as Kawamoto and it may reflect that there is no different invasiveness between nonfunctioning and functioning pituitary tumors.
Correlation between MMP-9 expression and tumor size, and extension
Many investigators found a positive correlation between tumor size and the frequency of microscopic or radiological invasion in pituitary tumors [1–3, 28]. Using the correlation between MMP-9 expression and tumor size, Turner stated that there was no difference among various sizes of prolactinomas [29] and Liu suggested that there was no correlation between MMP-9 expression and tumor size [43]. In contrast, Beaulieu, reported MMP-9 activity detected by zymography showed some correlation between MMP activity and tumor grade [33]. Our study showed, in nonfunctioning tumors, that MMP-9 expression was positively correlated with increase of tumor size, consistent with the relationship between frequency of dural invasion and tumor size. However, in FAs, MMP-9 expression in microadenomas was higher than in macroadenomas and was not statistically significantly different from extending tumors. This may reflect the high level of invasiveness in certain microadenomas such as ACTH adenomas characterized by frequent invasiveness [42]; these microadenomas often infiltrate the medial wall of cavernous sinus [44, 45]. Accordingly, MMP-9 demonstrated its ability to discriminate invasive tumors even at an early stage, depending on the principle that the secretion of MMP allowing migration of tumor cells is an important early aspect of the invasive process [19]. As for tumor extension, MMP-9 expression significantly increased when tumor invaded into the cavernous sinus or the sphenoid sinus.
Correlation between MMP-9 expression and primary/redo surgery
Dural invasion was present more frequently in the repeat surgery group than in the primary transsphenoidal surgery group [2]. We demonstrated that MMP-9 expression increased in the redo surgery group. This change was particularly significant in NFAs and confirms the progression of invasiveness between primary and repeat surgery. It remains debatable whether tumor invasiveness significantly impacts the recurrence rate. Theoretically, the ability of pituitary adenomas to invade may be reflected in their tendency to persist or recur after transsphenoidal excision. This may influence the rate of cure for endocrinologically active tumors and the rate of recurrence for clinically NFAs [28]. Comtois reported a higher incidence of recurrence in invasive tumours (33%) than in enclosed adenomas (15%) [46]. Nevertheless, Meij showed that the recurrence rate was not related to dural invasion in a consistent or significant fashion on the basis of histopathological evidence [2]. As for MMP-9 expression, Turner suggested that recurrent tumors were more likely to express MMPs [29] and Knappe insisted that there was no difference in expression of MMP-9 in recurrent adenomas [41]. Because of the small numbers in the current study, further research is ongoing to explore whether there is a positive correlation between MMP-9 expression and the recurrence rate and whether levels are higher at the tumor’s second presentation.
In conclusion, MMP-9 expression can reliably distinguish invasive pituitary tumors from noninvasive pituitary tumors and may also reflect the different extent of invasiveness in pituitary tumors according to tumor subtype, size, extension, and primary and redo surgery. MMP-9 is a potential candidate for predicting the invasive nature of pituitary tumors. Further study will be required to formulate an invasive index with an absolute value that could become an objective basis for individual cases. With long term follow up, MMP-9 expression from primary tumors and subsequent recurrence in the same patients will be compared and MMP-9 may become a predictor for tumor regrowth if a significant difference is confirmed. Moreover, there are several ongoing trials of synthetic inhibitors of MMP-9 in metastatic tumors of epithelial origin, and, if successful, they may play a role in pituitary tumor management [47].
References
Selman WR, Laws ER, Scheithauer BW, Carpenter SM (1986) The occurrence of dural invasion in pituitary adenomas. J Neurosurg 64:402–407
Meiji BP, Lopes MS, Ellegala DB, Alden T, Laws ER (2002) The long-term significance of microscopic dural invasion in 354 patients with pituitary adenomas treated with transsphenoidal surgery. J Neurosurg 96:195–208
Knosp E, Steiner E, Kitz K, Matula C (1993) Pituitary adenomas with invasion of the cavernous sinus space: a magnetic resonance imaging classification compared with surgical findings. Neurosurgery 33(4):610–618 (Laws ER comment)
Isono M, Inoue R, Kamida T, Kobayashi H, Matsuyama J (2003) Significance of leptin expression in invasive potential of pituitary adenomas. Clin Neurol Neurosurg 105:111–116
Trouillas J, Daniel L, Guigard MP, Tong S, Gouvernet J, Jouanneau E, Jan M, Perrin G, Fischer G, Tabarin A, Rougon G, Figarella-Branger D (2003) Polysialylated neural cell adhesion molecules expressed in human pituitary tumors and related to extrasellar invasion. J Neurosurg 98:1084–1093
Kong YG, Su CB, Ren ZY, Wang RZ, Li GL, Dou WC, Zhang B, Tian SQ (2003) Measurement of soluble CD44v6 in peripheral blood as assistant diagnosis of invasive pituitary adenomas. [Article in Chinese]. Zhongguo Yi Xue Ke Xue Yuan Xue Bao 25:698–701
Thapar K, Scheithauer BW, Kovacs K, Pernicone PJ, Laws ER (1996) p53 expression in pituitary adenomas and carcinomas: correlation with invasiveness and tumor growth fractions. Neurosurgery 38(4):765–771
Takino H, Herman V, Weiss M, Melmed S (1995) Purine-binding factor (nm23) gene expression in pituitary tumors: marker of adenoma invasiveness. J Clin Endocrinol Metab 80:1733–1738
Amar AP, DeArmond SJ, Spencer DR, Coopersmith PF, Ramos DM, Rosenblum ML (1994) Development of an in vitro extracellular matrix assay for studies of brain tumor invasion. J Neuro-onc 20:1–15
Egeblad M, Werb Z (2002) New functions for the matrix metalloproteinases in cancer progression. Nature Rev 2:163–176
Werner JA, Rathcke IO, Mandic R et al (2002) The role of matrix metalloproteinases in squamous cell carcinomas of the head and neck. Clin Exp Metastasis 19:275–282
Horikawa T, Yoshizaki T, Sheen TS et al (2000) Association of latent membrane protein 1 and matrix metalloproteinase 9 with metastasis in nasopharyngeal carcinoma. Cancer 89:715–723
Ballin M, Comez SE, Sinha CC, Thorgeirsson UP (1988) Ras oncogene mediated induction of a 92 kDa metalloproteinase; strong correlation with the malignant phenotype. Biochem Biophys Res Commun 154:823–838
Bernhard ED, Gruber SB, Muschel RJ (1994) Direct evidence linking expression of matrix metalloproteinase 9 (92-kDa gelatinase/collagenase) to the metastatic phenotype in transformed rat embryo cells. Proc Natl Acad Sci USA 91:4293–4297
Hua J, Muschel R (1996) Inhibition of matrix metalloproteinase 9 expression by a ribozyme blocks metastasis in a rat sarcoma model system. Cancer Res 56:5279–5284
Nakajima M, Welch D, Wynn D, Tsuruo Y, Nocolson G (1993) Serum and plasma M(r) 92,000 progelatinase levels correlate with spontaneous metastasis of rat 13762NF mammary adenocarcinoma. Cancer Res 53:5802–5807
Watanabe H, Nakanishi I, Yamashita K, Hayakawa T, Okada Y (1993) Matrix metalloproteinase-9 (92 kDa gelatinase/type IV collagenase) from U937 monoblastoid cells: correlation with cellular invasion. J Cell Sci 104:991–999
Zucker S, Lysik RM, Zarrabi MH, Moll U (1993) M(r) 92,000 type IV collagenase is increased in plasma of patients with colon cancer and breast cancer. CancerRes 53:140–146
Sang QXA (1998) Complex role of matrix metalloproteinases in angiogenesis. Cell Res 8:171–177
Kawamoto H, Uozumi T, Arita K, Yano T, Hirohata T (1996) Type IV collagenase activity and cavernous sinus invasion in human pituitary adenomas. Acta Neurochir (Wien) 138:390–395
Laquerriere A, Yun J, Hemet JTJ, Tadie M (1993) Experimental evaluation of bilayered human collagen as a dural substitute. J Neurosurg 78:487–491
Zhao YG, Cao XM, Xiao AZ, Zhu C (1999) Expression of MMP-2, -9,TIMP-1, -2, -3 mRNA in rat uterus during estrous cycle. Dev Reprod Biol 8:1–10
Zhao YG, Xiao AZ, Newcomer RG, Park HI, Kang T, Chung LW, Swanson MG, Zhau HE, Kurhanewicz J, Sang QX (2003) Activation of pro-gelatinase B by endometase/matrilysin-2 promotes invasion of human prostate cancer cells. J Biol Chem 278:15056–15064
Lillehei KO, Kirschman DL, Kleinschmidt-DeMasters BK, Ridgway EC (1998) Reassessment of the role of radiation therapy in the treatment of endocrine-inactive pituitary macroadenomas. Neurosurgery 43:432–439
Hansen LK, Molitch ME (1998) Postoperative radiotherapy for clinically nonfunctioning pituitary adenomas. Endocrinologist 8:71–78
Hussaini IM, Trotter C, Zhao Y, Abdel-Fattah R, Amos S, Xiao A, Agi CU, Redpath GT, Fang Z, Leung GKK, Lopes MBS, Laws ER (2007) Matrix metalloproteinase-9 is differentially expressed in nonfunctioning invasive and noninvasive pituitary adenomas and increases invasion in human pituitary adenoma cell line. Am J Pathol 170(1):356–365
Yokoyama S, Hirano H, Moroki K, Goto M, Imamura S, Kuratsu J (2001) Are nonfunctioning pituitary adenomas extending into the cavernous sinus aggressive and/or invasive? Neurosurgery 49(4):857–863 (Laws ER Comment)
Scheithauer BW, Kovacs KT, Laws ER Jr et al (1986) Pathology of invasive pituitary tumors with special reference to functional classification. J Neurosurg 65:733–744
Turner HE, Nagy Z, Esiri MM, Harris AL, Wass JAH (2000) Role of matrix metalloproteinase 9 in pituitary tumor. Behav J Clin Endocrinol Metab 85(8):2931–2935
Pan LX, Chen ZP, Liu YS, Zhao JH (2005) Magnetic resonance imaging and biological markers in pituitary adenomas with invasion of the cavernous sinus space. J Neuro-Oncol 74:71–76
Pereda MP, Ledda MF, Goldberg V, Chervi’n A, Carrizo G, Molina H, Muller A, Renner U, Podhajcer O, Gunter EA, Stalla UK (2000) High levels of matrix metalloproteinases regulate proliferation and hormone secretion in pituitary cells. J Clin Endocrinol Metab 85:263–269
Kawamoto H, Kawamoto K, Mizoue T, Uozumi T, Arita K, Kurisu K (1996) Matrix metalloproteinase-9 secretion by human pituitary adenomas detected by cell immunoblot analysis. Acta Neurochir (Wien) 138(12):1442–1448
Beaulieu E, Kachra Z, Mousseau N, Delbecchi L, Hardy J, Béliveau R (1999) Matrix metalloproteinases and their inhibitors in human pituitary tumors. Neurosurgery 45(6):1432–1441
Li Z, Ren Y, Wu Q, Lin S, Liang Y, Liang H (2004) Macrophage migration inhibitory factor enhances neoplastic cell invasion by inducing the expression of matrix metalloproteinase 9 and interleukin-8 in nasopharyngeal carcinoma cell lines. Chin Med J 117(1):107–114
Marbaix E, Donnez J, Courtoy PJ, Eeckhout Y (1992) Progesterone regulates the activity of collagenase and related gelatinases A and B in human endometrial explants. Proc Natl Acad Sci USA 89:11789–11793
Scheithauer BW (1982) Surgical pathology of the pituitary and sellar region. In: Laws ER Jr, Randall RV, Kern EB et al (eds) Management of pituitary adenomas and related lesions with emphasis on transsphenoidal microsurgery. Appleton-Century-Crofts, New York, pp 129–218
Sautner D, Saeger W (1991) Invasiveness of pituitary adenomas. Pathol Res Pract 187:632–636
Kovacs K, Horvath E (1986) Adenomas with ACTH production. In Tumors of the pituitary gland. Armed Forces Institute of Pathology, Washington, pp 134–164
Bradley KJ, Wass JAH, Turner HE (2003) Non-functioning pituitary adenomas with positive immunoreactivity for ACTH behave more aggressively than ACTH immunonegative tumours but do not recur more frequently. Clin Endocrinol 58:59–64
Scheithauer BW, Jaap AJ, Horvath E, Kovacs K, Lloyd RV, Meyer FB, Laws ER, Young WF (2000) Clinically silent corticotroph tumors of the pituitary gland. Neurosurgery 47:723–730
Knappe UJ, Hagel C, Lisboa BW, Wilczak W, Ludecke DK, Saeger W (2003) Expression of serine proteases and metalloproteinases in human pituitary adenomas and anterior pituitary lobe tissue. Acta Neuropathol 106:471–478
Knappe UJ, Ludecke DK (1996) Persistent and recurrent hypercortisolism after transsphenoidal surgery for Cushing’s disease. Acta Neurochir (Wien) 65(Suppl):31–34
Liu W, Matsumoto Y, Okada M, Miyake K, Kunishio K, Kawai N, Tamiya T, Nagao S (2005) Matrix metalloproteinase 2 and 9 expression correlated with cavernous sinus invasion of pituitary adenomas. J Med Invest 52:151–158
Fahlbusch R, Buchfelder M (1988) Transsphenoidal surgery of parasellar pituitary adenoms. Acta Neurochir (Wien) 92:93–99
Scotti G, Yu CY, Dillon WP, Norman D, Colombo N, Newton TH, De Groot J, Wilson CB (1988) MR imaging of cavernous sinus involvement by pituitary adenomas. AJNR 9:657–664
Comtois R, Beauregard H, Somma M, Serri O, Aris JN, Hardy J (1991) The clinical and endocrine outcome to transsphenoidal microsurgery of nonsecreting pituitary adenomas. Cancer 68:860–866
Lozonschi L, Sunamura M, Kobari M, Egawa S, Ding L, Matsuno S (1999) Controlling tumour angiogenesis and metastasis of C26 murine colon adenocarcinomaby a new matrix metalloproteinase inhibitor, KB-R7785, in two tumour models. Cancer Res 59:1252–1258
Acknowledgments
We are grateful to Dr. Yunde Bao (Department of Microbiology, University of Virginia Health System) for excellent technical support.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gong, J., Zhao, Y., Abdel-Fattah, R. et al. Matrix metalloproteinase-9, a potential biological marker in invasive pituitary adenomas. Pituitary 11, 37–48 (2008). https://doi.org/10.1007/s11102-007-0066-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11102-007-0066-2